
Abstract
Background:
Adolescents and youth from socially and culturally underserved communities face a disproportionate burden of depression, exacerbated by systemic barriers to accessing timely and culturally appropriate mental health care. In contexts where health systems are under-resourced, community-based initiatives may offer promising strategies for promoting youth mental well-being.
Objective:
This study explores how adolescents and youth from underserved communities in Mexico perceive and cope with depressive symptoms, with the aim of identifying community-informed strategies that can inform culturally relevant mental health promotion and prevention initiatives.
Methods:
Using an exploratory qualitative design, the study combined participant observation with focus group discussions involving people aged 15 to 25. A thematic analysis guided by resilience and participatory frameworks was conducted to examine youths’ emotional experiences, stressors, and coping mechanisms within their family, school, and social environments.
Results:
Participants reported depressive symptoms such as sadness, social withdrawal, fatigue, and hopelessness. Key stressors included family conflict, exposure to violence, and school-based pressures like bullying and academic demands. Although many youth used positive coping strategies—such as seeking social support and participating in recreational activities—some also exhibited maladaptive responses, including avoidance and silence. Focus groups emerged as empowering spaces for youth to articulate emotions and co-develop potential solutions.
Conclusions:
Findings highlight the urgent need for holistic interventions that integrate family and school-based programs with youth-centered, community-led mental health initiatives. Participatory methods are proposed as culturally sensitive, scalable approaches to address service gaps in under-resourced settings. These community-driven responses not only support individual coping but also contribute to the resilience of local health systems by aligning services with the lived realities of underserved populations.
Keywords
Introduction
Depression is one of the most prevalent mental disorders globally, 1 characterized by persistent sadness, loss of interest or pleasure, feelings of guilt, sleep or appetite disturbances, fatigue, and difficulties in concentration.2,3
A major depressive disorder (MDD), is diagnosed when a depressed mood or loss of interest persists for two or more weeks, accompanied by additional symptoms that significantly impact key areas of life, such as social, occupational, and familial functioning. 4
Depression affects individuals across all ages and social contexts, and in an increasingly globalized world, intensive and problematic internet use emerges as a factor that heightens its prevalence, especially in adolescents. 5
The prevalence of depression in adolescents and young is particularly concerning, having increased by more than 50% in last decades. In Mexico, this age group alone accounts for 426 Disability-Adjusted Life Years (DALYs) per 100 000 people. 6 A recent study in Mexican youth reported a 23% prevalence of major depression, a notably high figure given that adolescence represents a critical period for the development and progression of depressive symptoms, which are often accompanied by suicidal behavior. 7 Currently, Mexican adolescents have increased suicide attempts, and suicide has become the second leading cause of death in individuals aged 10 to 24 years. 6 These findings underscore the urgent need to understand how depressive symptoms are perceived and experienced by young people in socially and economically disadvantaged settings, where studies of depression and access to mental health care remains limited.
Health disparities affect ethnic minorities and population in the rural communities, and these inequities often translate into limited access to timely, culturally appropriate, and high-quality mental health services, exacerbating the effects of depression and perpetuating cycles of disadvantage. 8
In underserved communities, adolescents and young people face a dual burden: managing the personal effects of depressive symptoms while navigating systemic barriers to care, such as underinvestment in mental health infrastructure, shortage of trained professionals, and geographic or sociocultural isolation. 9 But there are also community-based initiatives have emerged as promising strategies to promote mental well-being, expand access to support, and build resilience in youth in vulnerable contexts.
The objective of this study is to explore how young people from socially and culturally underserved communities in Mexico perceive and cope with depressive symptoms, within the broader context of limited institutional mental health support. By using a participatory approach through focus groups, the study seeks to identify personal and collective coping strategies that can inform community-based, youth-centered mental health interventions. In doing so, the findings aim to contribute to the development of integrated responses that connect community action with broader health system strategies to prevent the escalation of depressive symptoms into severe disorders.
Methods
Design
This study employed an exploratory qualitative design based on resilience and participatory frameworks and the primary sources of data were three focus group of adolescents aged 15 to 25 years. The research is part of the implementation process of the Primary Care and Psychiatry Model (MAP-PSI), 10 aimed at facilitating early diagnosis and timely treatment of depressive symptoms in young people in underserved populations.
Participatory Framework
This approach aimed to build trust, understand local dynamics, and ensure that the research process was culturally appropriate and contextually grounded. The participatory framework guided both recruitment and fieldwork, as facilitators lived and worked within the community, sharing daily activities and co-organizing the intervention. Community members participated in planning and decision-making, helping to define how the sessions were conducted, organizing focus groups, and coordinating spaces, dates, and schedules. This collaborative process ensured a respectful approach aligned with community dynamics and local cultural practices. 11
Resilience Framework
Understanding depression prevention in adolescence requires recognizing the capacity of young people to adapt to adversity. The resilience framework provides a lens to examine how adolescents activate internal and external resources to maintain well-being under challenging circumstances. This perspective was central to our study, which aimed to identify emotional, cognitive, and behavioral patterns associated with depressive symptomatology. 12
Setting and Sociocultural Context
The State of San Luis Potosí (SLP), located in north-central Mexico, is characterized by significant ethnic diversity, with over 23% of its population identifying as Indigenous, mainly from the Náhuatl, Téenek, and Xi’ui groups. This State has more than 2.8 million inhabitants, with approximately 17% aged 15 to 24 years. The study was conducted in Ciudad Fernández, one of the 59 municipalities of SLP, see (Figure 1), selected for its high proportion of youth. In these underserved communities, 83.9% of the Indigenous population lives in poverty and faces limited access to mental health services, exacerbating existing social and cultural inequalities. 13

Map of Ciudad Fernández, SLP, Mexico.
Participants
Participant recruitment was carried out through community key informants, including healthcare workers, educators, and staff from municipal institutions that provide services and support to young people. These key informants helped extend an open invitation to adolescents and youth of both sexes, aged 15 to 25, residents of marginalized rural or Indigenous communities, and willing to share personal or observed experiences related to depressive symptoms. Participants were not required to have a formal clinical diagnosis; recruitment was based on self-reported emotional experiences, in line with the exploratory qualitative objective of the study. Additionally, as part of the broader MAP-PSI study, mental health promotion and outreach activities were conducted in community spaces commonly attended by youth—such as schools, sports centers, and social development hubs. During these activities, information was shared about depressive symptoms and the purpose of the research, and adolescents and youth were invited to join the focus groups to share their perspectives. Participants were informed that the study aimed to better understand their perceptions of depression to inform mental health strategies. The facilitators, both women—a psychologist and an anthropologist—shared their roles as researchers at the National Institute of Psychiatry with doctoral training in mental health and over 15 years of qualitative research experience, which helped establish trust and rapport during the sessions. A total of 18 youths, 12 females and 6 males from different communities, participated in three focus groups conducted between November 2022 (first group), November 2023 (second group), and August 2024 (third group). The focus groups were not designed for comparative or follow-up purposes but as independent data collection moments at different stages of the MAP-PSI implementation. Each session explored face to face specific aspects of adolescents’ daily stressors, emotions, and coping strategies lasted approximately 50 minutes and followed a format encouraging reflection and the exchange of experiences regarding the daily lives and emotions of young people in the community. The time gaps reflected programmatic phases rather than methodological issues and allowed inclusion of youth from different community clusters, enhancing thematic saturation and credibility. 14 Municipal authorities and local community members facilitated the use of spaces to host these groups.
Procedure
Upon convening the participants, the fieldwork coordinator introduced the study’s objectives, explained the participation dynamics, and clarified any questions. The focus group sessions were conducted in a municipal Mental Health Center located in Ciudad Fernández, a setting chosen to ensure privacy, accessibility, and comfort. In addition to the participants and the two female facilitators—a psychologist and an anthropologist—a third researcher, also a psychologist, was present to take observational field notes on the group dynamics. The sessions were overseen by the study’s lead investigator (LDC). All participants agreed to collaborate voluntarily by signing an informed consent form. For minors, assent was obtained along with the informed consent of a legal guardian or responsible adult. Participants were instructed to replace their names with fictional identifiers, which they adopted and used throughout the interviews. Permission was also requested to audio-record the group discussions, with assurances of confidentiality and anonymity for all information shared. The research protocol was reviewed and approved by the Ethics Committee of the National Institute of Psychiatry Ramón de la Fuente Muñiz.
An interview guide was developed ad hoc, adapting elements from the BETLS Observation Tool (Early Childhood Australia, ECA). 15 The semi-structured interview guide itself was developed collaboratively by the research team, composed of professionals with extensive experience in clinical interviews in child and adolescent psychology and psychiatry in consultation with municipal health personnel, ensuring cultural relevance. The BETLS was used only as a conceptual reference to identify key domains of exploration—emotions, thoughts, and behaviors—relevant to the study objectives. This approach enabled the integration of contextual factors into five key dimensions: (1) daily life, (2) sources of stress or conflict, (3) emotions, (4) thoughts and actions (behaviors) against emotional discomfort for identifying coping strategies, and (5) sources of support. A new category emerged during the focus groups regarding mental health care needs and access to available services, enriching the understanding of perceptions, coping strategies, and service gaps in these underserver communities. A graphical representation of the research methodology is provided in Figure 2.

Research methodology of focus group study.
The interview guide and the researchers’ credentials and roles are described in detail within the Consolidated Criteria for Reporting Qualitative Research (COREQ) report are available online at Figshare [DOI 10.6084/m9.figshare.29365460].
Analysis
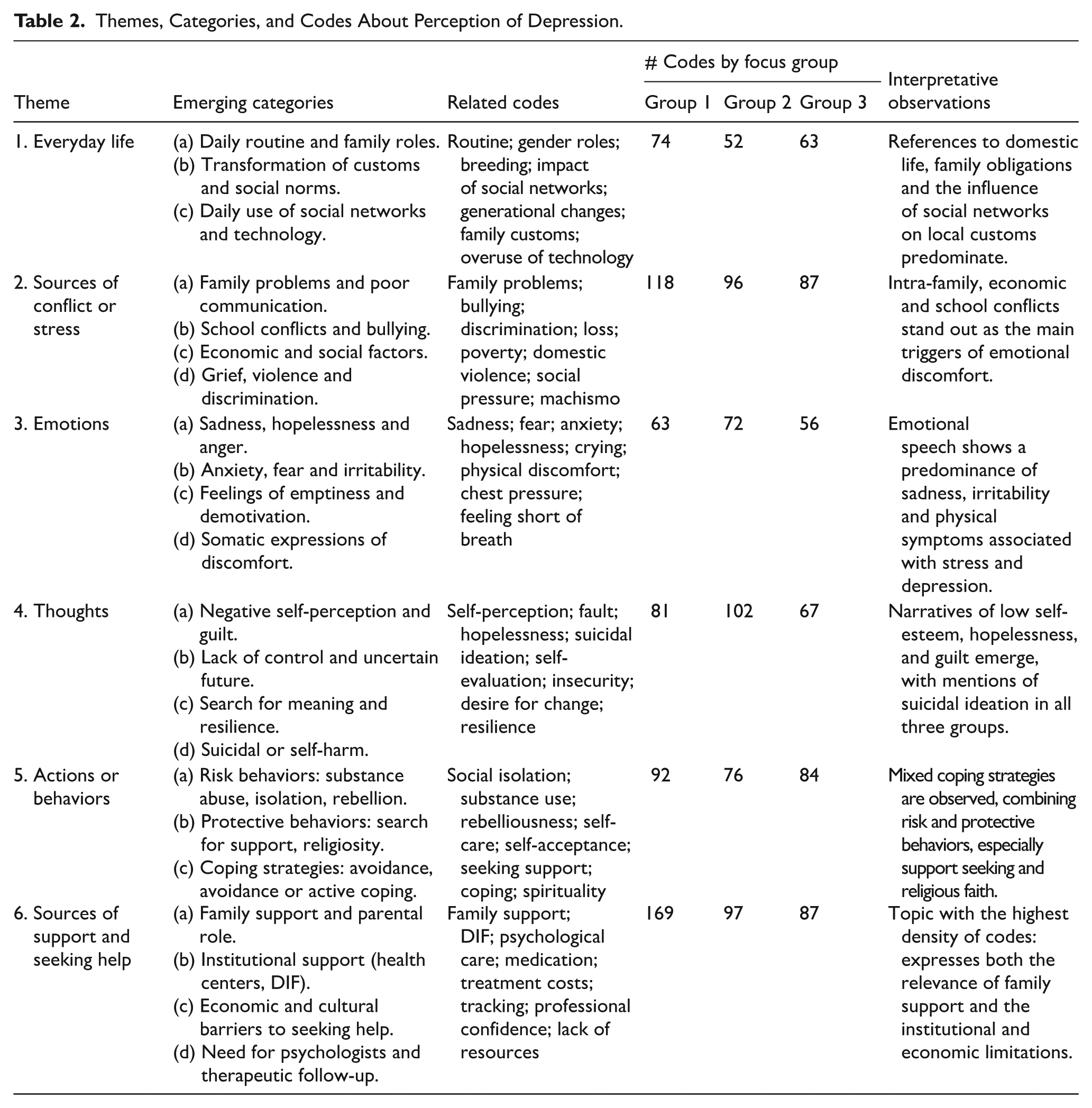
The focus groups were transcribed in Word and imported into ATLAS.ti.V.24, a qualitative analysis software package used to organize the information and conduct content analysis through a three-step process 16 : (1) identification of general meaning units and thematic dimensions reflected in the experiences and textual expressions shared by the adolescents and youths, (2) identification of specific categories within each thematic dimension established in the interview guide, including the definition of criteria and application of coding, and (3) review and discussion of the data considering the context and observations recorded by the research team during fieldwork. Field notes were taken during the sessions by a third researcher, which allowed for the clarification of emerging themes with participants before concluding each focus group. These notes also captured information beyond the original interview guide, such as the emergent topic of access to mental health services, which was later integrated into the thematic framework. A total of 1606 codes were generated, organized into analytical categories and overarching themes (Table 1). Two researchers (NBA and LDC) independently coded all transcripts and discussed discrepancies until reaching consensus, ensuring credibility, dependability, and confirmability as per Lincoln and Guba’s 17 framework. The full transcripts were not returned to participants for comment, but a description of each theme was presented and clarified during the sessions to ensure accuracy and shared understanding. Data saturation was monitored across groups as part of the iterative analytical process, as no new categories or themes emerged after the third focus group.
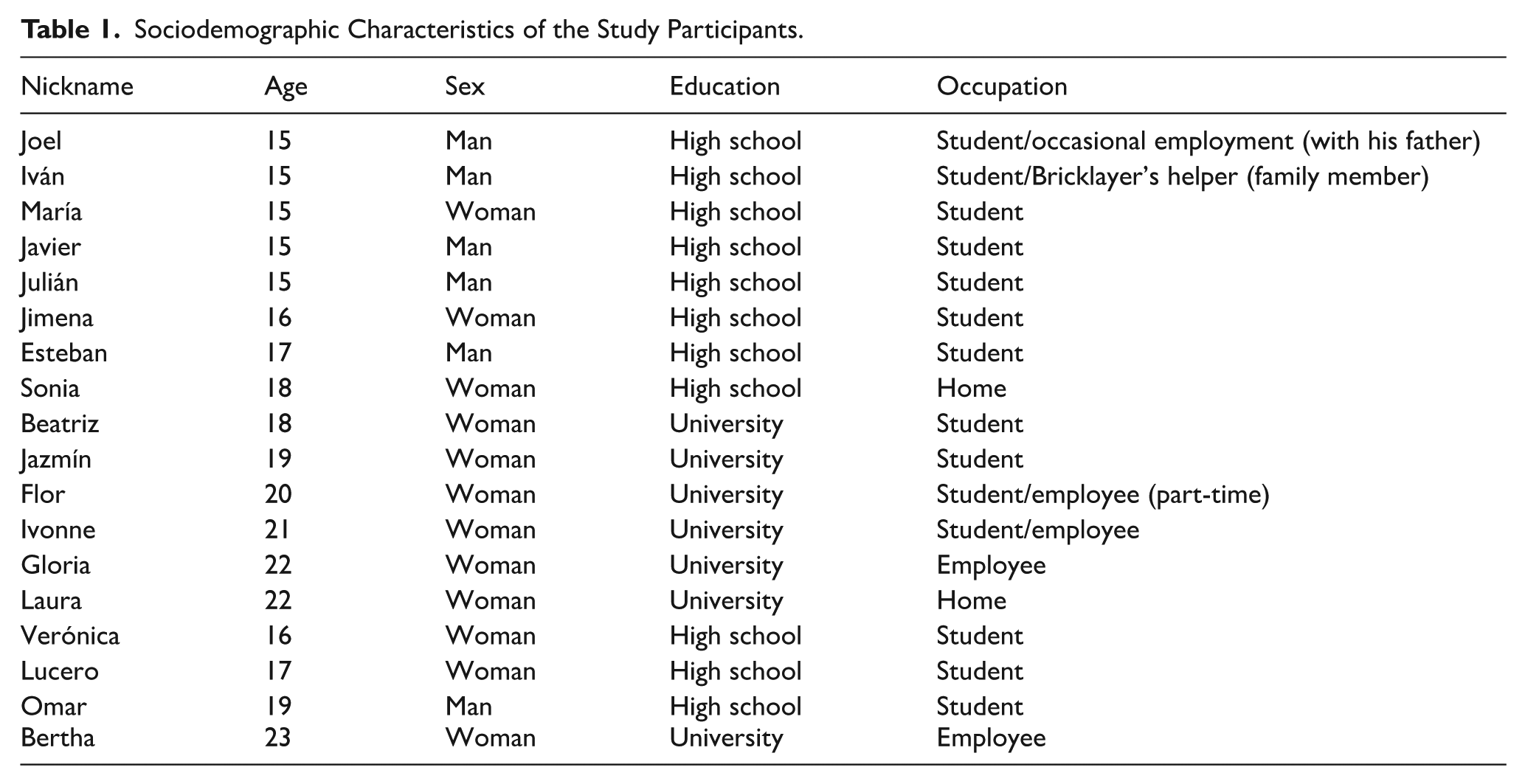
Sociodemographic Characteristics of the Study Participants.
Results
The sociodemographic characteristics of the participants are summarized in Table 2. The results obtained through the categorization and analysis of their testimonies are presented below. The dimensions were identified around experience and emotional health from the perspective of young people.
Themes, Categories, and Codes About Perception of Depression.
Daily Life
This dimension describes the daily routine of young people including their activities, social interactions, and use of free time. Knowing how they configure their daily routine and the options available to them around them favours the understanding of the system of values, beliefs and social norms in which they develop and from which they configure their identity, life project, and self-perception within their group and society. Their daily life revolves mainly around home and school. Some also engage in work activities: minors usually assist their parents or guardians, mainly fathers, while older youth add work as a third sphere of development and interaction.
Well, in the morning I go to school, and in the afternoons sometimes I go with my dad to work or if not, to play baseball. (Joel, 15 years old). He [dad] works as a bricklayer, I help him there with what I can, like making the mixture and all that (Iván, 15 years old).
Although some have jobs, they perceive few entertainment or employment options, which they recognize could help relieve emotional distress through distraction.
Some people like to do one thing, and for example, one can’t do that here, mmm, there could be more places to see what they like to do [. . .] then you get bored following the same routine, it’s kind of boring and for some, it’s good (Flor, 20 years old). Most want to work and it’s not allowed and sometimes [it’s] kind of desperate for them because they want to make money or something, they have the craving for money. Sometimes work would also be something for them to be distracted by (Sonia, 18 years old).
Regarding free time, the activities in most cases are delimited by those that can take place, preferably, within the home. This places them in greater exposure to the use of digital devices and the impact of social networks, the latter, although they represent spaces that favor interaction and communication between adolescents, especially in environments where national and international migration is a constant that modifies ties and community dynamics. However, social networks can also constitute a source of unreliable, false and inappropriate information, stereotypes, value judgments and various stimuli capable of negatively impacting the emotional health of young people, generating feelings of dissatisfaction, lack, anxiety and depression.
The digital media too, there is a lot of information there, many campaigns for depression, anxiety and all, all these problems. Social media has a very, very important influence because they can pay more attention to a video than even to their parents, you could say so. Most of us are out there on social media a lot and think that everything we see there is true. If they see that a person is happy doing something, for example, if someone buys drugs there and is happy like that, doing that, then they are going to believe it, they are going to say: “Ah, this is very good.” They are very influential on young people lately and it is important to regulate them as well. The algorithm is very addictive, it teaches you things about what you like. For example, if I like bicycles, I always start to get shown things about bicycles and all that. (Esteban, 17 years old).
Sources of Stress and Emotional Distress
School and family were referred to as the two main sources of stress and conflict. A common expression reported in all focus groups was that they did not feel understood or heard by adults, mainly by their parents and teaching staff, which translates into a deep need for attention and to be heard.
Problems come from not understanding each other, rather, but I don’t like to talk to them because I feel that sometimes they don’t understand it, somehow, they don’t understand me enough, or I don’t know if we don’t understand each other when we talk (Esteban, 17 years old). In my school no one pays attention to me, no one listens to me, and the teacher does not listen to me about what happens to me. I have suffered since kindergarten bullying, cyberbullying and many other things (Javier, 15 years old).
The family is described as an environment where rejection, criticism, expressions of violence, discredit, and undervaluation are experienced, constituting in many cases a source of insecurity. However, they report the need for communication and closeness, for greater coexistence, mainly with their parents.
Well, I think it’s happened to all of us back there, right? There are problems or you go through situations or many times they don’t understand, they don’t understand how you feel, they start to tell you things, that is, you prefer to avoid all that and better get out, avoid it because they don’t understand. (Jazmín, 19 years old).
The configuration of the domestic group as a source of stress is mediated by the presence of various family problems, communication and, in many cases, expressions of violence (verbal, psychological, physical and sexual) that can be minimized or normalized.
I also don’t want to be like my dad because he drinks, he’s a policeman, but he drinks and he can be fired from his job if he keeps doing that. . . Yes, he does behave badly and get in a bad mood. Bad words, so to speak, words that hurt me, like those times when I made an effort to do something and he didn’t value it when he was like that like he didn’t think things through when he says them, he doesn’t think about them and on one of those times that he drank, he told my mom to leave the house and my mom said: “Well, I’m leaving,” and so it was. She took all the things and so, that was, just what happened. (Esteban, 17 years old). All my life I have wanted to know my father’s name. I don’t have a father, I was born because of sexual abuse, a brother of my mother raped my mother and my mother became pregnant. (Javier, 15 years old).
In addition to alcohol consumption, young people report the presence of mental health problems present in various family members (sister, mother, father, etc.), which are not always diagnosed or under medical treatment of any kind.
My sister about two weeks ago, had a problem, she had a lot of anxiety and she called me, she said: “I have a lot of anxiety”, something like that she told me and she was crying. I was at a friend’s house at that time and I told her: “I can’t pick you up”, but she called my dad and my dad went to her. She said that she was crying and that she was already hospitalized in the IMSS [healthcare services], they put her there and sedated her, I don’t know how much they did to her, but they said they were going to take her to the next day to San Luis. And now, it seems that about two days later they went to San Luis with the psychiatrist and the psychiatrist gave her the medicines. And she’s better now. I think that he [dad] also has anxiety, he is always very anxious if he is not drinking. And I tell him: “No, calm down” And then he tells me: “Let’s run”. And I tell him: “I don’t like to run, but if you want I’ll accompany you or something.” And that’s it, that would be his solution, you could say (Esteban, 17 years old).
School, on the other hand, also represents a source of stress from the difficulties and problems experienced in peer relationships and bullying to a greater extent, followed by difficulties associated with academic performance.
For example, yesterday I went to school with a problem, my classmates did not accept me, they humiliated me, they have always humiliated me. They insult me, they tell me that I am worthless, that I have no value for anything, that is, they humiliate me. They even beat me, I feel so lonely without friends, without anyone to listen to me. I told her everything that happened to me [teacher], about my classmates, I didn’t do anything to them, I didn’t say anything to them. I have always been a child without friends, without classmates who respect me and I have never had friends or anything (Javier, 15 years old).
At the base of this dimension of analysis, we can observe how interpersonal relationships and social interaction constitute a source of stress that is having a significant impact on the emotional health of young people.
In this same sense, working on them, on their improvement, as well as on the development of resources and personal skills and more appropriate parenting and education practices would favor their transformation into a source of well-being and support.
[My mom] tells me: “Well, you are very important to me in my life” That is what she tells me and makes me feel good, very good (Jimena, 16 years old).
Emotions
As part of this dimension of analysis, the main manifestations of emotional distress and depressive symptomatology that adolescents recognize concerning three different areas are reported: affective or emotional, physical and behavioral. It is important to note that although they all recognize expressions of sadness, feelings of loneliness, pain, suffering, frustration, dissatisfaction, fear, contempt, insecurity, anger, rejection, and humiliation, in this study sample, these are manifested differently between male and female adolescents, accounting for how the variation in the expression of emotional distress is crossed by sociocultural factors and gender models.
Some immerse themselves in their evil. . . I think that everyone has their way of expressing what they feel. Some are very aggressive, and others go on drugs so as not to feel everything they feel, to let it out, so to speak. Also, others who drink, but more than drinking I think they go more to drugs, I have not seen many who go to drink (Esteban, 17 years old). Because of school problems that I couldn’t, I couldn’t concentrate or that kind of thing. Yes, because I was also sad before, but I said: “Well, no, I have to solve it.” No, it’s not, it’s not so much that I say: “I can’t, I can’t”, I just blocked myself, but no, in the end, I said “No, I can, it’s not that much, it’s not difficult, it’s easy to think that everything is difficult” (Joel, 15 years old).
A difference between sexes was observed, in women, emotional distress and depressive symptomatology linked more frequently to a more internal, emotional sphere more prone to the experience of deep sadness, crying, compared to men in whom the manifestations are characterized by adopting a more behavioral dimension, such as the consumption of substances and risky practices, as well as emotional expressions linked to irritability and aggressiveness that are projected outside the person. On the other hand, physical exhaustion and isolation are reported as manifestations of emotional distress and depressive symptomatology in both men and women in the area.
I have seen that those people who are doing well and little by little are falling into their emotional state, who are sometimes happy and sometimes they are very sad, but little by little they are more depressed, you can tell in their eyes and sometimes in the actions they perform, that nothing comes out anymore, I don’t know, all that kind of thing (Esteban, 17 years old).
Thoughts and Actions (Identifying Coping Strategies)
During this stage of life, young people face different processes of change related not only to their biological development but also to social, and cultural processes and life expectations linked to the definition of their own identity, a life project, school and work responsibilities in many cases, as well as the construction of affective bonds that include dating relationships and friendships with their peers. The way they cope with these stressful situations and other difficulties involves the deployment of a series of efforts at a cognitive and behavioral level that shape coping styles according to the meaning they give to their experience and the personal resources they have.
The most common coping strategies for emotional distress are positive ones, mainly seeking support and engaging in enjoyable or distracting activities outside the home.
Having a hobby [. . .] something you love to do to keep your mind distracted and not be thinking bad things or anything like that. It’s a way of keeping yourself okay, so to speak (Esteban, 17 years old).
Thirdly, they report talking about the problem with people close to or trusting, as well as exploring the resolution of the problem.
The search for information and working on the emotion they experience are other strategies to which they resort and to a lesser extent report physical activity or exercise, as well as a negative or refusal to consume substances in the face of the offer by friends. The availability of substances is a reality present in the spaces where young people develop, making the difference between developing a substance use problem, and the resources and skills they may have to deal with it.
At my school, many people use drugs, which I think is very wrong. I’ve been offered, but I always say no. While it doesn’t happen much inside, it does outside, involving the same classmates. For me, biking is my main escape—I’m a mountain biker and often go on tours, usually with my dad or sometimes alone. (Esteban, 17 years old).
While some participants reported the refusal to experiment with substance use as part of positive strategies, others recognized that is common in some classmates at school and even in adults, as is the case of their parents with excessive alcohol consumption. As part of the negative coping strategies, the main strategy reported is not talking about the problem, followed by avoidance, self-harm (cutting) and expressions of aggressiveness.
Well, my mom brought me [psychology service] because I started cutting myself, because when I felt bad instead of talking about it I cut myself, I think I felt more liberated (Jimena, 16 years old). I don’t know, I’m not one to tell you anything about my problems, until now that I know that I can go to the psychologist, to the psychiatrist, that I’ve already started to let go more (Gloria, 22 years old). In my case, before if I was the same, I preferred to make other commitments than to be at home and think about things and so I feel like being alone, like my mind cooks more. . ., (Jazmín, 19 years old).
Although both positive and negative dimensions were reported in the coping strategies, it is important to mention that there was a greater reference and diversity in the case of positive strategies that allow accounting for the personal resources and strengths that young people already have, which would need to be reinforced and accompanied through care services.
I aim to finish what I’m studying and also high school I don’t want to get anyone pregnant, I don’t want to get high or anything like that, I want to finish everything well. In the grades, I have always excelled, so it is not so much that, I always make sure that I am at the level and do not drop, do not drop from what I already am. (Esteban, 17 years old).
Support Resources
The first thing that is worth highlighting as part of this dimension of analysis is the fact that young people recognize the need to approach, talk and receive support from their closest circle, which includes their father, mother, siblings, teaching staff, as well as other adolescents and young people, such as peers, and friends. In this sense, the three main support resources available to them would be the family member, father, mother or siblings according to the circumstances in each of their lives. Secondly, friendships, peers and finally, the medical services available in the area. In such a way, young people are placed not only as passive subjects, in a situation of vulnerability that makes them require support but as beings capable of providing support to others who are going through similar situations by adopting a more active role as part of the support network of others, including their parents.
I hardly feel sad, but if I did, then in that case [I would go with] my sister. When I know that my friends have a problem or something like that, I try to give them a solution, I try to help them, but sometimes it’s just a matter of them having the initiative to do, to help themselves because, so to speak, you can’t do it alone, you need help from someone else too. To be happy they need to talk to others (Esteban, 17 years old). With my mom, she’s the only one who listens to me. I told her: “Mom, I want to go to a psychologist, I want to value myself and have courage and have my health” And then she said: “Well, let’s go, mijo.” My partner knows very well, he knows everyone there from the DIF [National System for Family Development] and I have his number and he helps me a lot (Javier, 15 years old).
Mental Health Care Needs and Access to Available Services
The population expresses a clear need for psychological and psychiatric care, reflected in a growing demand for available services. However, access is limited by the absence of public services, long distances to care centers, and related expenses such as private consultations, medications, and transportation, since no local public transport exists in the area.
He charged me eight hundred [for the consultation], the pills were one thousand two hundred, I think, more or less, but anyway, every time you go he charges you for the consultation (Beatriz, 18 years old). My apartment is here at CDFDZ, [it takes] like half an hour, not that much, like twenty minutes. Well, if it were in a taxi, I think I would jump for about thirty, to forty minutes (Gloria, 22 years old). From my house, I walk from school, about half an hour to here, if I take a taxi about ten (Ivonne, 21 years old).
The search for care despite these obstacles is reinforced by the positive outcome and the changes experienced as a sense of well-being and liberation that young people recognize and attribute to receiving psychological care. This goes hand in hand with having satisfied the need to be heard and understood previously mentioned, to give value to their voice and what they are experiencing.
I already feel more liberated, talking to him about everything. More than anything, as in my case, he helped me to let off steam, to bring out what I couldn’t tell any people. (Julián, 15 years old). Well, it helped me a lot at the beginning of the service to ask for change because I didn’t know, I felt very confused, and in the sessions, I kind of felt calmer, that is, it helped me solve some problems and think a little more and not stay with the first thing. I changed many decisions with what I wanted to do and that affected me and other people. (Gloria, 22 years old).
Likewise, in the psychoeducation care sessions, they find a space to leave or move from the place that is generating stress and emotional discomfort, in addition to finding the opportunity to develop resources and skills for managing their emotions, solving problems and coping with their life experiences in general.
I participated on one occasion and that’s how it guided me to be able to solve my problems and to this day I try and I still do it sometimes [laughs] But I do remember the strategies and I do apply them (Beatriz, 18 years old).
Regarding pharmacological treatment, the testimonies touch on issues surrounding medication use, with one focused on practical barriers (adherence) and the other on concerns about medication intensity. There is a notable perception of public psychiatric care as more moderate and less reliant on intense medication, contrasting with the assumed practices of private care.
For me, well, I’m a little out of control because of the times, because I’m going here, there. I forget the medicine, or I miss the hour, but it does help me a lot. On the one hand, as they say, fifty per cent, to help me, then it does help me a lot, doing it right with myself (Gloria, 22 years old). I say it’s fine because a private psychiatrist gives you very strong medication, I’m telling you because I’ve seen it, I’ve never been to one, but I’ve seen it. So, depending on the medication, it is already a little very difficult, so here you come, they give you anything, but it’s not strong, you don’t depend on it (Ivonne, 21 years old).
A key contribution of this work is the use of focus groups to create a space where young people feel heard and actively participate in identifying the challenges they face, constructing potential solutions, and recognizing available support options, such as primary care services and remote psychiatry. One participant reflected, It’s good to have this type of meeting. You can share what’s happening and feel like you’re being taken care of. Sharing is very good (Laura, 22 years old).
Discussion
The results of this study provide a deeper understanding of the emotional experiences and needs of young people from socially and culturally vulnerable communities. Young people’s daily lives are deeply influenced by their family and school environments, with interactions reflecting both support and tension. These findings are consistent with prior literature on the importance of family and school as critical contexts for adolescent emotional development.18,19 In this study, however, the family is not only described as a space for affective interaction, but also as a significant source of stress due to violence, neglect, and poor communication—factors that demand intervention to promote positive parenting and healthier family dynamics.
Participants reported a range of depressive symptoms, such as sadness, loneliness, fatigue, and social withdrawal. These findings are consistent with previous studies on emotional distress in vulnerable adolescents20,21 and show how these symptoms are determined by sociocultural gender expectations. 22 Early adverse experiences, such as neglect or emotional abuse, were associated with emotional dysregulation and maladaptive coping, also consistent with prior findings.23,24
Despite these challenges, adolescents and youths also demonstrated resilience through positive coping strategies such as seeking social support and engaging in recreational activities. However, the simultaneous use of negative coping—such as emotional suppression (silence and avoidance)—emphasizes the need to develop safe, trusting environments that encourage help-seeking and emotional expression. 25
The school environment, often a source of bullying and academic pressure, was also identified as a critical site of stress, highlights those seemingly maladaptive strategies play a long-term regulatory role in coping with intense emotions and stressful events that could lead to hopelessness and suicidal behavior. 26 The coexistence of anxiety, depression, and a bleak future are associated with hopelessness, which is why this factor should be considered a key element in interventions aimed at preventing suicidal behavior. 27 These findings reinforce the importance of mental health promotion within educational settings, moving beyond academic performance to prioritize emotional well-being. In this context, community-based mental health strategies—such as school-based support services and peer-led initiatives—represent promising practices that integrate health promotion into adolescents’ daily environments. 28
Notably, the idea of implementing telehealth services emerged as a innovative, community-informed solutions to address access gaps, especially in under-resourced or rural settings. 29 Whereas that challenges to implementation remain, 30 patient-centered, culturally adapted models co-designed with young people offer viable pathways to improve service delivery. 31 These approaches not only facilitate early care access but also represent a means to strengthen the overall resilience of the health system by decentralizing care and making it responsive to community-specific needs. Crucially, for youth who reported feeling perpetually unheard in their primary social contexts (family and school), these services offer a structured, confidential, and non-judgmental professional space. This validation, as evidenced by participants’ attribution of “liberation” and “sense of well-being” to professional psychological care (eg, “talking to him about everything”), directly addresses the core unmet need to be understood.
The use of participatory methods—such as focus groups—was itself a key element of community engagement in this study. These spaces enabled youth to voice concerns, build solidarity, and co-identify problems and strategies. These community-led initiatives function as crucial, non-familial listening spaces that actively counter the daily experience of feeling neglected by adults. By facilitating the sharing of concerns and the collective construction of solutions, community-led programs inherently valorize the youth voice. Rather than passive subjects of intervention, participants became agents of change, illustrating the power of community-based participatory research to inform inclusive mental health responses. This reinforces the importance of designing community-led or co-developed mental health initiatives, aligning with WHO recommendations for people-centered, context-specific interventions. 32
A central finding of this study is the interplay between structural stressors (eg, poverty, violence) and interpersonal vulnerabilities (eg, family conflict), which together constitute a double layer of adversity. 33 These intersecting challenges demand comprehensive, multisectoral responses. Integrating mental health with family-based programs, school initiatives, and digital health solutions offers a multi-level community-based strategy that could meaningfully support adolescents’ emotional well-being.
When comparing our findings to research involving other socially and culturally vulnerable youth communities, both similarities and crucial differences emerge. Similarities primarily revolve around the universal experience of stressors: family dysfunction and the perception of not being heard are consistently reported across low-resource settings, including studies in African and Asian contexts.34,35 Furthermore, the presence of gendered expressions of distress (internalization in females, externalization/risk behavior in males) is a well-documented phenomenon globally. 36 However, the context of the middle zone of San Luis Potosí reveals distinctive nuances. Unlike the high-density urban vulnerability often studied, our cohort navigates a semi-rural setting characterized by a critical lack of structured recreational and job opportunities. This structural deficit forces an intensified reliance on the immediate family and, increasingly, on digital media for social connection and identity formation.
This finding contrasts with studies where youth may have greater access to alternative social spaces, shifting the locus of both risk and resilience disproportionately back to the domestic sphere. Moreover, the bimodal coping profile—strong positive strategies (eg, support from mothers/siblings, hobbies like biking) coexisting with high exposure to negative practices (substance use, self-harm)—underscores a community-mediated resilience that requires specific cultural adaptation in intervention design. This specific blend of high interpersonal stress, limited external resources, and family-driven coping differentiates the profile of these Mexican youth from more general findings on poverty or marginalization alone.
Limitations
One limitation of this study is the small sample size (n = 18), reflecting the broader challenge of limited youth engagement in research contexts. A second limitation of the focus group is the risk of social desirability bias, where participants may be reluctant to disclose highly sensitive or stigmatizing experiences in a collective setting. However, we mitigated this risk through trained facilitators, confidentiality, and a supportive environment encouraged open discussion. Despite these limitations, the data provided valuable insights that supported the study’s objectives and conclusions.
Conclusions
This study highlights the emotional challenges faced by adolescents and youth in socially and culturally vulnerable communities, emphasizing the importance of holistic and participatory approaches that promote resilience, emotional expression, and co-created, contextually relevant solutions. Such initiatives can strengthen local capacities and complement formal health systems.
Footnotes
Acknowledgements
The authors would like to thank the young participants for their enthusiastic involvement and for generously sharing their life experiences with us. Their openness made this research both meaningful and memorable. The authors acknowledge the use of ChatGPT (OpenAI) for English language and grammar editing support during the preparation of this manuscript.
ORCID iDs
Ethical Considerations
The research protocol underpinning this article was approved by the Research Ethics Committee of the National Institute of Psychiatry Ramón de la Fuente Muñiz (Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz—INPRFM) under registration number CEI/C/034/2022, dated July 18, 2022.
Consent to Participate
All participants provided written informed consent prior to enrollment in the study.
Author Contributions
NBA: Contributed substantially to the design of the study, as well as in the analysis, interpretation, and presentation of the data. LDC: Played a significant role in the design and acquisition of the study, as well as in the analysis, interpretation, and presentation of the data. Drafted the manuscript and conducted critical revisions for significant intellectual content. CDC: Contributed substantially to the analysis and interpretation of the data. HCR: Provided significant input into the analysis and interpretation of the data. BEPV: Made important contributions to the interpretation of the data and critically revised the manuscript to enhance its intellectual content. JCSH: Offered valuable insights into the interpretation of the data and conducted critical revisions of the manuscript to ensure its intellectual rigor. All authors reviewed and approved the final version of the manuscript for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research and the subsequent publication of this article were supported by the Gonzalo Río Arronte Foundation I.A.P. Grant Number S.736.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.