
Abstract
Background:
This qualitative systematic review aims to identify, analyse and discuss barriers and facilitators to formal dementia services for South Asians in the UK with dementia. South Asian individuals in the UK are more likely to face a dementia diagnosis than the White British demographic; a trend which is expected to grow over the following decades. Despite this greater need for support, the UK South Asian demographic is less likely to access formal dementia services.
Methods:
MODEM, Web of Science, PubMed, CINAHL via EBSCO, The Cochrane Library, and Scopus were searched (22nd July 2025) using a SPIDER search strategy and included studies’ bibliographies were checked, in addition to existing review literature. Data on included studies was extracted using an adapted Cochrane Library data collection form and quality assessed using the JBI critical appraisal instrument for qualitative research. Themes were extracted and analysed using reflexive thematic analysis. Ten articles were found to meet the inclusion criteria and therefore included in this systematic review. While this review is framed as considering UK South Asians, data was only available from Bangladeshi, Indian and Pakistani individuals. However, much literature which claims ‘South Asian’ only defines South Asia as consisting of these three countries. Therefore, calling this paper a review of the ‘South Asian’ demographic allows us to critique this homogenisation.
Results:
Five main themes were identified: Lack of Knowledge, Racism/Culturally Inappropriate Care, Stigma, a Familial Duty of Care and Service Delivery. There was disagreement in the literature regarding the existence of stigma. Previously unrecognised interrelations between these themes were identified, as a lack of knowledge had a potentially causal effect on both stigma and a familial duty of care.
Conclusion:
The results indicate a need for review of current policy and practice, however further research is needed, particularly with regard to facilitators, which lacked data in comparison to barriers.
Introduction
Dementia, a progressive neurodegenerative condition, is characterised by cognitive decline and behavioural changes. Symptoms of dementia include negative emotional outcomes (eg, depression, anxiety, apathy, irritability), sleep and appetite disturbances, and atypical motor behaviour.1-3 The condition can significantly impact an individual’s daily life, making it difficult to perform routine tasks.1-3
Dementia diagnosis in the UK typically involves an initial assessment by a medical practitioner, after which the individual is referred to a memory clinic. 4 At a memory clinic, a dementia specialist will conduct a comprehensive physical and psychological examination to confirm the diagnosis and recommend appropriate care. 4 A formal dementia care plan considers how an individual with dementia can best maintain normalcy, and provides information about services and financial support, and how to access them. 5
Definition of South Asian
UK South Asians are 1st, 2nd, or 3rd generation individuals living in the UK, from the countries of Afghanistan, Bangladesh, Bhutan, India, the Maldives, Nepal, Pakistan, and/or Sri Lanka 6 and those who have migrated from the Indian subcontinent (comprising all South Asian countries apart from Afghanistan) to East Africa, and then to the UK (East African Asians). 7
According to 2021 census data, individuals of Indian, Pakistani, and/or Bangladeshi descent make up 6.9% of the UK population, 8 increasing 9 from 5.3% in 2011 and 3.9% in 2001. Data for other South Asian countries are not available.
This systematic review only includes individuals from Bangladeshi, Indian and/or Pakistani heritage. However, we maintain the use of South Asian as readers looking for research regarding dementia and UK South Asians may not, without this paper, be met with any discussion on the generalisability of results across all South Asian demographics. Further, our search strategy, regardless of which countries it returned, would still be inclusive of ‘South Asian’.
Epidemiology of Dementia of South Asians in the UK
Literature indicates a higher prevalence of dementia among the UK South Asian population compared to the white British population.10,11 There is a significantly increased 12 risk of dementia in South Asians relative to those of White European ancestry.
In 2011, the number of dementia cases across the South Asian and black ethnic groups in the UK was 25 000. 11 This number is predicted to increase exponentially. By 2026, there are expected to be 50 000 individuals living with dementia in these groups, with a sevenfold increase to 172 000 cases anticipated by 2051. 11 The South Asian community is expected to experience the most rapid growth in dementia cases during this period. 13
Minority ethnic (ME) communities experience delays in diagnosis and treatment of dementia14-17 being symptomatically affected at a younger age and dying earlier than White populations with the condition. 18 Further, ME populations have higher rates of dementia risk factors, including vascular risks (and therefore vascular dementia), marginalisation, and deprivation.19,20
Definitions of Barriers and Facilitators to Formal Dementia Services
We define a barrier as something participants report as hindering the likelihood of South Asians in the UK with dementia from accessing formal dementia healthcare services, and a facilitator as an either implemented or potential solution to overcoming these barriers.
Existing Systematic Reviews
Previous reviews21-24 have explored barriers to dementia service access among South Asians in the UK. These studies identified several common themes, including reduced knowledge about dementia symptoms and services, cultural beliefs about the condition, and familial responsibilities.
Three of these reviews21-23 identified a limited knowledge of dementia in UK South Asians. This lack of knowledge included being unaware of symptomologies of dementias,21-23 not knowing about formal services,21,23 and a belief that the condition is God-given.21,23 This lack of knowledge was identified as a direct barrier to service access in all three articles,21-23 with some individuals reporting their beliefs that dementia is a curable condition. 21
One review 22 stated that the belief of dementia being God-given causes stigma, while another 21 reported an individual with dementia will receive blame from their family, while also reporting that care is preferred to be kept informal and within the family unit.
Three of these previous reviews21,23,24 do not provide a formal definition of South Asian, while one 22 only included India, Bangladesh and Pakistan. In this review, we have provided a clear and appropriate definition of UK South Asian. This allows us to discuss gaps in existing literature and the risk of homogenisation of results across countries/groups.
None of the previous reviews21-24 formally discuss interrelations of themes, with the closest being the aforementioned reporting of a lack of knowledge (dementia being God-given) leading to stigma. 22 Our methodology of Braun and Clarke’s reflexive thematic analysis 25 allowed for a more intricate story to unfold by entering the data analysis stage without a preset list themes.
Research Question
What are the barriers and facilitators to accessing formal dementia services for South Asians in the UK?
Methodology
A systematic review was conducted to address the research question outlined above, adhering to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) standards.
Search Methodology and Terms
A SPIDER (Sample, Phenomenon of Interest (POI), Design, Evaluation, Research Type) search strategy was employed across MODEM, Web of Science, PubMed, CINAHL via EBSCO, The Cochrane Library, PsychINFO, and Scopus. This search was conducted on the 22nd July 2025. The PubMed database search is given as an example in Supplemental Appendix 1. Search terms are given in Table 1 below.
Search Strategy.

MeSH terms were used when searching PubMed, PsychINFO, and The Cochrane Library. Equivalent CINAHL headings were used when searching CINAHL via EBSCO. Keyword searches were done in Scopus, Web of Science and MODEM. MODEM does not allow truncation so all terms were entered explicitly. Where possible, keyword searches included abstract and title searches.
In addition to database searches, the reference lists of included studies were examined, along with the aforementioned review literature.21-24 Furthermore, other literature which cited the included papers was assessed for eligibility. Originally, grey literature in the form of Google Scholar was searched, however this returned results of the order of hundreds of thousands, and was therefore not pragmatic to continue. Theses were actively excluded as they are not peer reviewed literature.
Inclusion Criteria
Literature was considered for inclusion if it concerned South Asians of first, second, or third generation descent with dementia, or carers for first, second or third generation UK South Asians with dementia, whether formal (professional) or informal (familial). Further, literature needed to focus on barriers and/or facilitators of accessing dementia services in the UK, be qualitative in nature, and be primary data studies published in 2000 or later. Additionally, only English language studies were considered for inclusion.
Exclusion Criteria
Literature was not considered for inclusion if it was concerned with regions outside of the UK, or if it did not include South Asian individuals with dementia or carers for those with dementia.
Further, literature was excluded if it was not focused on access to formal dementia care services, used quantitative or mixed methods methodologies, or used secondary data. Finally, papers published prior to 2000 or not written in English were also excluded.
Quality Assessment
The JBI (Johanna Briggs Institute) critical appraisal instrument for qualitative research 26 was utilised to assess the quality of studies. Quality assessment was conducted by all three researchers, where each study was reviewed by two authors. The first author reviewed all 11 studies, while the second author reviewed six and the third author the remaining five. Where disagreements occurred, these were discussed, with the lead author making the final decision. A template of the JBI critical appraisal instrument for qualitative research in Supplemental Appendix 2, and study characteristics in Supplemental Appendix 3.
Data Extraction
The Cochrane Data Collection Form (Supplemental Appendix 4) was used to extract relevant information from the included studies. Extracted data included: First author, Year of publication, Title, Study design, Participants, Aim(s), Definition of South Asian used, Data collection method, Data analysis method, and Data source(s). Data extraction was conducted by the first and second authors.
Data Synthesis
Reflexive thematic analysis was used to analyse the data from the included studies, to avoid constraining the voices of participants with a preset list of themes and concepts. 25 This approach allowed for the identification of both directly discussed themes and novel themes not explicitly addressed in the included studies. 27
Results
Search Results
Figure 1 provides a PRISMA diagram of the selection of studies. In total, the search identified 868 papers from the MODEM (565), Web of Science (172), PubMed (65), CINAHL via EBSCO (52), The Cochrane Library (10), PsychINFO (7), and Scopus (0) databases. Of these, 142 were removed due to duplication, leaving 730 studies to be screened. A further 704 papers were excluded during the abstract screening phase. One full text could not be retrieved, and 16 studies were excluded for criteria including inappropriate/no definitions of South Asian (n = 9) and the document being a PhD thesis (n = 7). Hence, a total of eight papers were identified for inclusion from database searching. Citation searching of these eight studies, and previous reviews21-24, identified three further papers as appropriate for inclusion, providing a total of 11 papers which met the inclusion criteria. Quality assessment excluded one of these 11 papers, and so this systematic review includes ten studies.
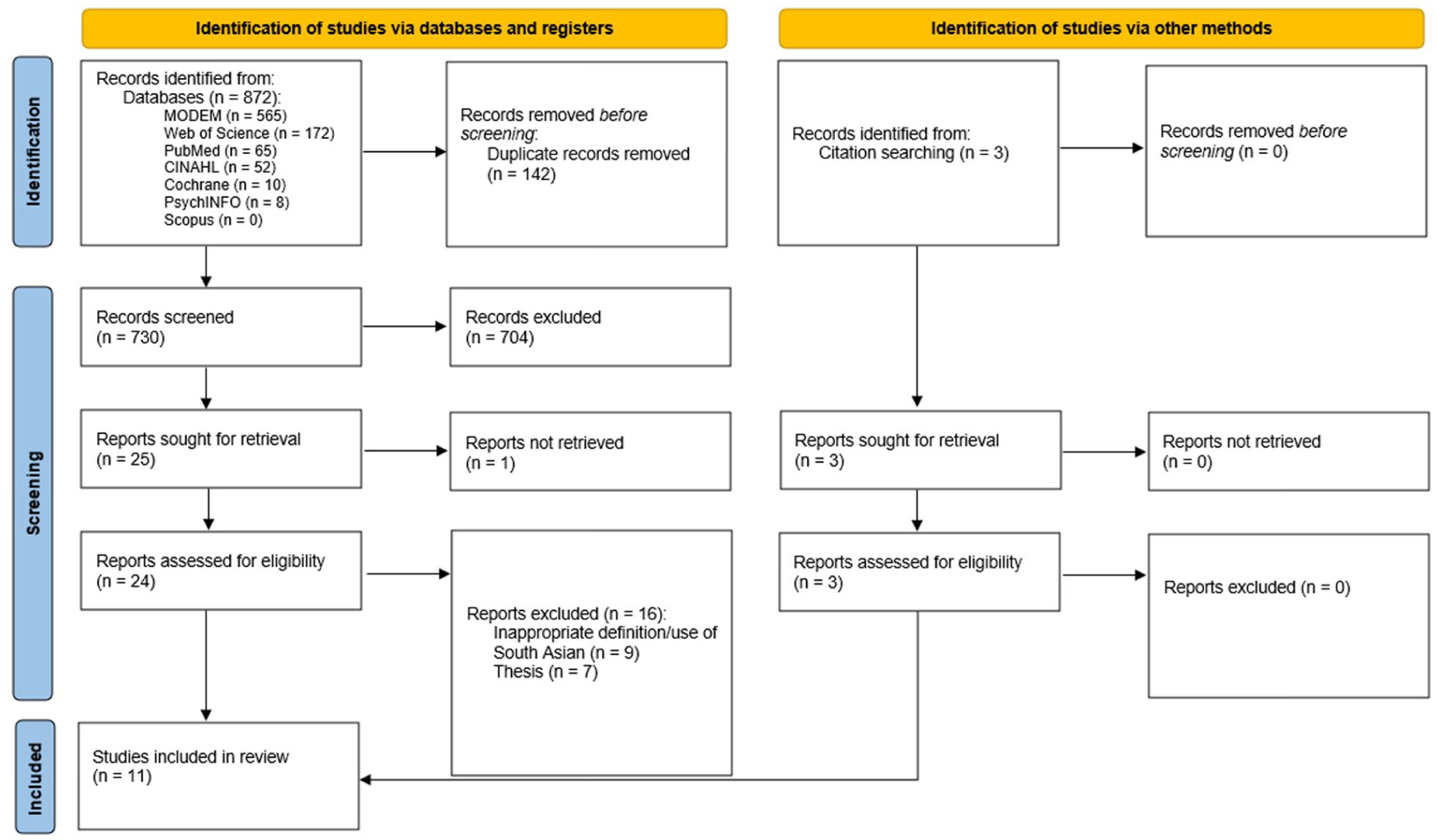
PRISMA diagram.
Quality Assessment
Ten of the 11 included papers were assessed to be of high quality. The paper 28 assessed to be of low quality was excluded from the review. Full quality assessment results are presented in Supplemental Appendix 5.
Characteristics of Included Studies
A total of 265 participants were included across the 10 studies,29-38 of which 208 were South Asian. The remaining participants were from other ethnicities, as four studies29,31,32,34 focused on multiple ethnic groups.
Participants in six studies29,31,32,36,37 were exclusively carers of individuals with dementia. One study 33 focused solely on individuals with a dementia diagnosis, two studies30,38 included both carers and individuals with a diagnosis of dementia, and one study 33 specified participants had a ‘range of backgrounds’.
Pooling age and sex data from the included studies,29-38 ages ranged from 18 to 83, with 70 males and 95 females (additionally one participant’s sex was ‘unknown’). Three studies30-32 did not provide information on age range, and two studies31,32 did not provide information on sex. Additionally, one study 30 only provided sex information for participants with a dementia diagnosis, not professionals within dementia care.
Two studies29,31 specified that participants include South Asians who immigrated via East Africa. Eight studies30,32-38 do not specify East African South Asian participants in their definitions. One study 31 specified that participants were first, second and third-generation South Asian immigrants in the UK.
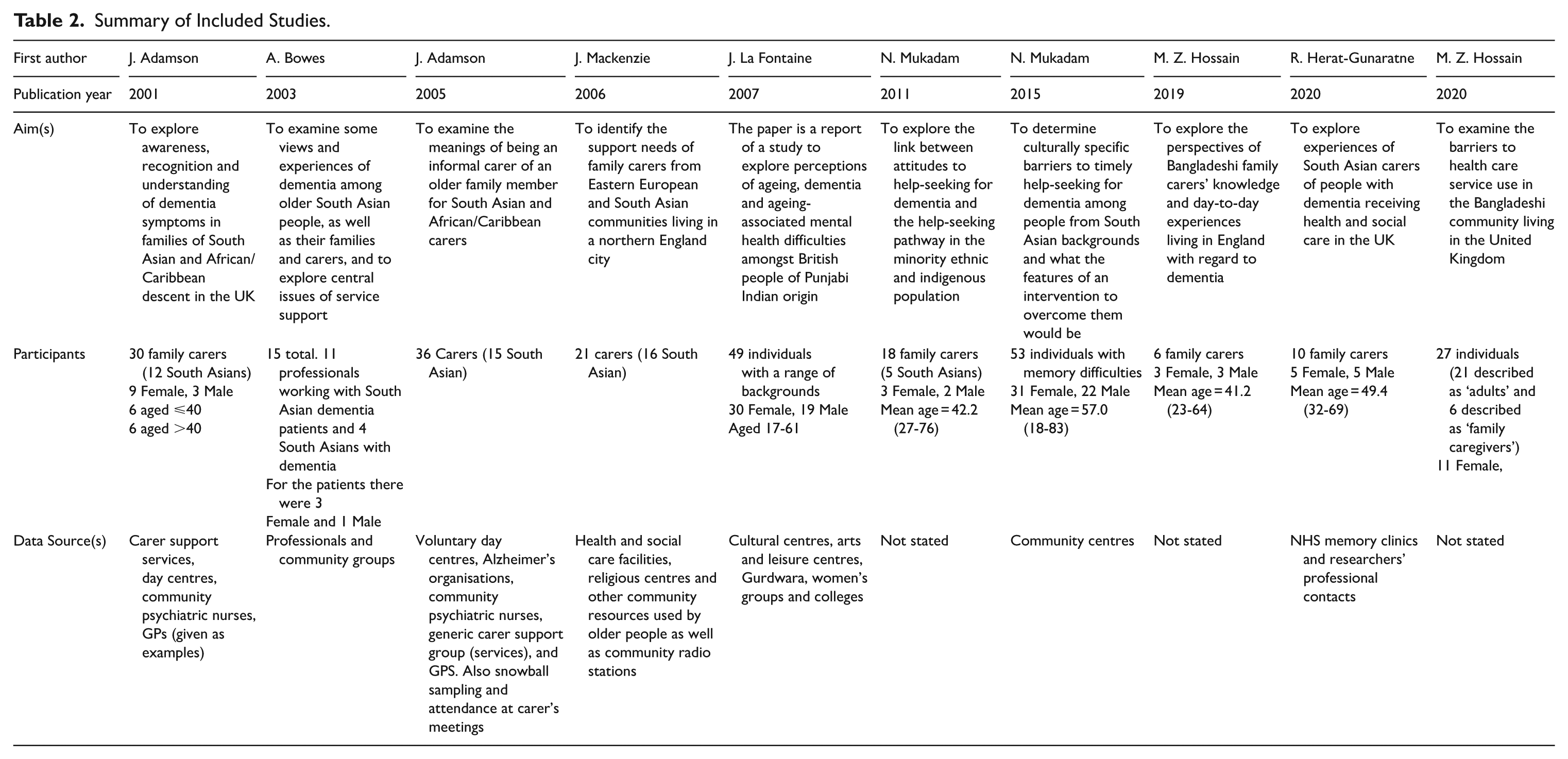
Table 2 shows the first author, publication year, aim(s), participant information, and recruitment settings of each study. Full study information is given in Supplemental Appendix 3.
Summary of Included Studies.
Themes
Lack of Knowledge
Barriers
Eight studies29,30,32-36,38 identified a lack of knowledge as a barrier to timely access to dementia services. Six of these papers29,30,33,34,36,38 reported a lack of knowledge about dementia itself, while two studies35,36 presented a lack of knowledge where dementia was seen as a normal part of the ageing process, and three studies30,32,36 reported a belief of some UK South Asians that dementia was a result of God.
This lack of knowledge about dementia led to delays accessing care, with some not seeking help until there was a specific risk. 35 Some participants described delays in accessing care due to not knowing the symptoms of dementia, thinking the symptoms were related to other conditions, or the symptoms not impacting on the patients’ activity due to their care being taken over by the family. 34
Two papers33,36 discussed how help-seeking for dementia by UK South Asians is often in response to other medical conditions, for example, eczema treatment. Three studies33,35,38 reported a lack of knowledge among individuals with dementia and their family/community networks regarding how to access dementia care services. One of these three studies 38 stated that service providers can demonstrate a lack of knowledge about effective methods to recruit UK South Asians to dementia services.
Facilitators
One study 36 believed that dementia support services should discuss dementia with South Asian communities. Another 35 emphasised the importance of communicating that dementia has a physical cause, and the value of information coming from a trusted source.
Racism/Culturally Inappropriate Care
Barriers
Racism or culturally inappropriate care was identified in five studies.29,30,33,37,38 Three papers30,37,38 discussed the perception among UK South Asians that care homes were culturally inappropriate. There were concerns regarding the ability of healthcare professionals to provide appropriate care, particularly in relation to religious needs and potential racial discrimination. 38
Two studies33,37 highlighted language barriers as a factor contributing to the breakdown of dementia support. Concerns regarded the ability of families to communicate their worries due to language differences. 33 Some individuals faced difficulties in finding home care workers who spoke the same language as their relative with dementia. 37
Facilitators
One study 35 suggested that information presented in leaflets, DVDs, TV adverts, and videos in GP waiting rooms could be beneficial. Another study 33 reported that a more conversational approach would help; taking time to build rapport with patients in a friendly environment.
Stigma
Barriers
Five studies30,32,33,35,37 discussed stigma as a barrier for UK South Asians to access dementia services. Individuals associated the stigma of a mental disorder with being much worse than the stigma of a chronic medical disorder, for example: Most illnesses, . . . you can be distanced from them and you can deal with them on a practical level. You get diagnosed. You’re treated, you do something to make it go away, or live with it, . . . but with dementia it’s more devastating, I think, because it completely takes over the person. . .it actually takes you away from who you are as a human being, with all these connections that we have. (Individual with memory difficulties)
35
However, one study 36 reported that there was no stigma associated with dementia. Four studies30,32,33,37 wrote that isolation of those with dementia could result from the stigma they faced. One article 30 raised concerns that individuals with dementia might isolate themselves due to guilt and associated stigma. Additionally, stigma could lead to families of those with dementia wanting to conceal their ill relative(s) from their wider community. 32
Facilitators
Normalising help-seeking was thought to promote others to seek support earlier, 35 emphasising that it is nothing to be ashamed about and it is experienced by many people. No more specific facilitators were identified.
Familial Duty of Care
Barriers
Six papers31-33,35,37,38 reported strong cultural beliefs that the family of an individual with dementia should provide care for them. It was discussed 32 how family carers had limited acceptance of dementia services due to feelings of shame in accepting outside help and pride in their ability to provide care. There was also a belief that an individual’s perceived duty of care may be intrinsically linked to their ethnicity and religion.31,32
Facilitators
Family carers indicated reluctance to accept formal care due to the pressures of these cultural expectations. One study 37 suggested that early implementation of support services could facilitate acceptance of dementia services by allowing UK South Asians to see the benefits early.
Service Delivery
Barriers
In addition to services not being culturally appropriate, service delivery in the UK was identified as a barrier to seeking care, and four papers highlighted issues with the process of getting a diagnosis of dementia.33-35,38 Two papers30,33 highlighted the lack of dementia services as a problem in getting help, and a participant in one study 37 reported an issue with service provision being reduced when they had moved in with their relative to care for them.
Facilitators
Some participants 36 described having a positive experience with dementia diagnosis and other participants 35 expressed the view that health and social care support was very good in the UK. Three papers30,34,35 reported that participants said they would go to their GP in the first instance when symptoms were an issue, though as mentioned previously, some participants 34 said they only received a diagnosis when seeking help for other physical health conditions.
Interrelations Between Themes
There is evidence that a lack of knowledge is causally related to both stigma and a familial duty of care. One study 33 found that stigma could be associated with a lack of knowledge of dementia. A second study 35 discussed the belief that the individual with dementia or their family could improve the illness.
Discussion
Key Findings
To aid interpretation, we structured the discussion around cross-cutting mechanisms linking the five core themes, emphasising how individual beliefs, family expectations and service design interact to influence help-seeking.
A lack of knowledge emerged as the most prominent theme, reported in eight papers.29,30,32-36,38 Supporting review literature 24 has similarly found that dementia was often viewed as a normal part of ageing, as one study 38 reported that only 21% of South Asian participants were aware of dementia and its impact on cognitive function. In addition to a lack of knowledge about service availability, wider research 24 has identified transportation as a potential barrier to access, with many individuals relying on family in order to access services. However, clinicians also reported difficulty in knowing how to best to engage those with dementia from a South Asian background in formal services. 38 It has been argued 39 that clinicians face challenges overcoming cultural and language barriers and may lack knowledge about best practices for community engagement and multilingual service provision. To our knowledge, this review is the first to explicitly model the interrelations between these determinants using the Health Belief Model, illustrating how knowledge deficits may precipitate stigma and reinforce familial duty norms that deter service use. This conceptual linkage advances the field significantly, offering a theoretical foundation for developing multifactorial interventions.
Racism or culturally inappropriate care was identified as a barrier in five studies.29,30,33,37,38 Existing literature has also found that language barriers were a major concern for clinicians when considering the inclusion of South Asians in clinical trials.39,40 Research 41 suggests that hiring healthcare professional from a wider range of backgrounds or offering language courses could help bridge the communication gap.
Stigma was identified as a barrier to accessing dementia services in five studies.30,32,33,35,37 Other literature 41 has predicted that 77% of the variance of help-seeking can be explained by attitudes towards dementia, highlighting the significant influence of perceived social pressure. There is discourse in existing literature42,43 that there is great value in understanding religious communities as a method to reduce stigma.
A familial duty of care was discussed as a barrier to accessing dementia services in six studies.31-33,35,37,38 Cultural expectations regarding family care influenced reluctance to seek professional help. One article 37 suggested that early implementation of formal support could facilitate acceptance of dementia services by allowing UK South Asians to see the benefits early.
Service delivery was also identified as a barrier to accessing care in four studies,33-35,38 though this is not necessarily an issue specific to UK South Asians. Participants reported difficulty with diagnoses and issues with service provision, which can be exacerbated by the lack of knowledge around dementia symptoms and services.
A lack of knowledge was found to have a potentially causal effect on stigma and a familial duty of care; a novel finding from this research not mentioned in existing literature. We have modelled this in Figure 2 using the Health Belief Model, a model which allows for ones personal beliefs to be included in assessing why a particular behaviour may be reached, and to therefore better assess interventions. 44

Health belief model applied to formal dementia care access.
Further literature39,40 also highlighted a lack of knowledge of professionals with regard to providing culturally appropriate care, especially language barriers. Therefore, addressing a lack of knowledge from both the professional and patient sides could result in greater trust and help overcome the barriers of stigma, culturally appropriate care, and a familial duty of care.
Strengths of Review
Within the existing literature, as is apparent in the results and discussion of this article, there is far more data regarding barriers to formal dementia care access, than there is regarding facilitators to overcoming these barriers. However, in synthesising facilitator evidence, we identified several promising mechanisms through which access could be improved. Educational outreach and multilingual information campaigns can directly address the widespread lack of knowledge; community dementia champions and peer-led workshops may reduce stigma and normalise help-seeking; and embedding cultural-competence training within primary care pathways can improve service delivery. Positioning facilitators alongside the corresponding barriers provides a more applied framework for future intervention design.
Additionally, we believe this to be the first review of this subject debating the homogenisation of results across South Asian countries. We believe that this should be the starting point of any such research, and therefore encourage researchers to have this discussion with themselves and others when conducting such work and thinking about the implications of any results they report. We also believe this is a more respectful way to conduct this research, as it acknowledges that there are both similarities and differences in cultures, religions and values between countries in South Asia and individuals from those countries, and therefore the need to promote the individual representation of these demographics.
Limitations of Review
This review only included articles published in English, and further, the included papers only reported the views of 208 individuals, with no participants of Afghani, Bhutanese, Maldivian, Nepalese or Sri Lankan nationality or descent. The included papers lacked information on specific needs in relation to specific countries or religions within South Asia.
During the quality assessment stage, two included studies29,31 did not have clear ethical approval statements, nine included papers29-34,36-38 did not have a clearly stated philosophical perspective, nine did not have a clear statement locating the researcher culturally or theoretically,29-32,34-37 and all ten studies29-38 did not entirely state how the researcher(s) influenced the research or vice-versa. The absence of reflexive accounts within most included studies limits our ability to evaluate how researcher positionality or cultural assumptions may have shaped data interpretation; this introduces uncertainty around the transferability of insights about stigma and culturally defined care expectations. The decision to include these studies, and conduct this research, was partly based on the immediate need for such an article, given the growing rates of dementia in the UK South Asian demographic.10-18 Fundamentally, despite the aforementioned quality limitations of the included studies, the overall quality of research was assessed to be high enough for their inclusion, and conducting this research now helps push for conversation around this pressing topic.
Ideally, the theme of ‘Racism/Culturally Inappropriate Care’ would be separated clearly into ‘Racism’ and ‘Culturally Inappropriate Care’. This would of course allow for a more nuanced discussion of the barriers and facilitators relating to these themes. However, given the data available in the included studies, it would be too difficult to disentangle this neatly into these two categories without it feeling like guess work.
Potential publication and language biases are present due to the omission of non-English language publications. However, as this systematic review addresses UK research, we felt it was appropriate to exclude non-English language publications. This was also justified by the lack of ability of authors to translate all potential languages, adding potential time and other resources to this research which we did not have. Nevertheless, the consistency of findings across diverse qualitative contexts and convergence with wider minority-ethnic dementia literature lend confidence to the robustness and relevance of these conclusions.
Implications for Research and Policy
Country-specific research is needed for UK South Asians with Afghani, Bhutanese, Maldivian, Nepalese or Sri Lankan heritage to identify potential differences and inform the development of more specific facilitators. In addition, research discussing the needs of each South Asian country and major religion is required.
Further research is also needed with specific regard to facilitators of access to formal dementia services of the UK South Asian populace, as current research primarily focuses on barriers. Additional research is required regarding the interrelation of themes as barriers to formal dementia care access. A more complex analysis of these relationships could inform the development of effective facilitators to access dementia support for UK South Asians.
Additionally, while this article focuses on South Asians, research also indicates the potential vulnerabilities of other minority ethnic groups. 11 Therefore, important, similar research is strongly suggested for other groups. Further research focusing on the gendered effects of stigma, generational differences, socioeconomic groups, and a comparison of South Asian countries to other minority ethnic groups would add great detail to this growing body of work.
The difficulty in separating what is considered ‘Racism’ and what is considered ‘Culturally Inappropriate Care’ with existing data leaves space for this to be pursued in future research. The impacts of separating these themes are, of course, very important, and affect how policy and practice (hiring, carer practice, review procedures, working conditions, etc.) should be updated.
We would recommend systems to appoint ‘dementia champions’ within South Asian communities, building knowledge, reducing stigma and normalising help-seeking. This process involves recruitment of respected individuals from a community, who work to normalise help-seeking behaviours in their community, acting as a mediator between those around them, and formal services. 45 We therefore recommend the contacting of religious leaders and community group leaders as potential starting points for these roles. As a note, the role of a community member as a dementia champion, is not to be confused with a formal, healthcare professional working as a ‘Dementia Champion’. 46 Comparable initiatives such as the Alzheimer’s Society’s ‘Dementia Friends’ programme and NHS England’s community health ambassador schemes demonstrate the feasibility of community-embedded advocacy roles. Integration of these approaches through Integrated Care Boards (ICBs) and local voluntary-sector partnerships could provide sustainable mechanisms for culturally sensitive dementia engagement. While this too could be helpful, there are existing barriers in the unpaid time of these professionals to perform such roles, which we do not have time to discuss here. 46
Further, we believe mandatory cultural competence training for dementia specialists would reduce cultural divides and allow for practitioners to apply evidenced competencies when communicating with those from South Asian backgrounds. Collaboration with community organisations would facilitate co-designed services with South Asian patients central to their own framework.
Conclusion
Multiple, nuanced barriers and facilitators exist for South Asians accessing formal dementia services in the UK. These barriers and facilitators were categorised into five themes: a lack of knowledge, racism/culturally inappropriate care, stigma, a familial duty of care and service delivery. We found a lack of knowledge regarding dementia as have a potentially causal effect on both stigma and a familial duty of care. Given the lack of careful definition of ‘South Asian’ in existing literature, and that this systematic review only includes evidence regarding the Bangladeshi, Indian and Pakistani demographics, we advise great care in generalising results, including between these three groups.
The combination of projected dementia prevalence and underutilisation of formal dementia services by UK South Asians creates an unavoidably pressing need for investment in tailored and thoughtful strategies. The longer the wait until such strategies are implemented, the more individuals will suffer unnecessarily from the effects of dementia.
Supplemental Material
sj-docx-1-his-10.1177_11786329251408964 – Supplemental material for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review
Supplemental material, sj-docx-1-his-10.1177_11786329251408964 for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review by Dan Chaib, Katie Biggs and Hina Khan in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329251408964 – Supplemental material for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review
Supplemental material, sj-docx-2-his-10.1177_11786329251408964 for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review by Dan Chaib, Katie Biggs and Hina Khan in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329251408964 – Supplemental material for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review
Supplemental material, sj-docx-3-his-10.1177_11786329251408964 for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review by Dan Chaib, Katie Biggs and Hina Khan in Health Services Insights
Supplemental Material
sj-docx-4-his-10.1177_11786329251408964 – Supplemental material for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review
Supplemental material, sj-docx-4-his-10.1177_11786329251408964 for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review by Dan Chaib, Katie Biggs and Hina Khan in Health Services Insights
Supplemental Material
sj-docx-5-his-10.1177_11786329251408964 – Supplemental material for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review
Supplemental material, sj-docx-5-his-10.1177_11786329251408964 for Barriers and Facilitators to Formal Dementia Care Use Among UK South Asians: A Systematic Review by Dan Chaib, Katie Biggs and Hina Khan in Health Services Insights
Footnotes
Acknowledgements
Dan Chaib would like to thank Dan Green, for his supervision with this research in its original form of a Masters dissertation.
Ethical Considerations
Ethical approval for research conducted and information public in this article was not obtained as it was not necessary.
Consent to Participate
Informed consent for information published in this article was not obtained as data used was all secondary.
Author Contributions
DC undertook the systematic review as part of a master’s dissertation under the supervision of KB and wrote the first draft of the paper. Both DC and KB extracted data from the included papers, synthesised and interpreted the results. DC, KB and HK all quality assessed studies. HK added valuable background information.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Sheffield Institutional Open Access Fund was accessed for the open access publication fees. No other financial support was accessed for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is this systematic review is available from the included studies. All data used is secondary and qualitative.
Rights Retention Statement
For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.