
Abstract
Objective:
Evaluating user satisfaction and its associated factors in two primary healthcare centers in Ucayali, Peru.
Methods:
The study was cross-sectional analytical study conducted in April 2025 among patients who received care at two primary healthcare centers located in Ucayali, Peru. To assess their satisfaction with the care received, we used the Ambulatory Medical Consultation Satisfaction Scale (ESCOMA). To identify the factors associated with the ESCOMA satisfaction score, we used linear regression models.
Results:
A total of 465 patients were included; 66.5% of those surveyed were women, and the median age was 40 years (IQR 31-52). Of these, 74.8% lived in the same city as the healthcare center. The median ESCOMA score was 7 points (range 6.17-8.28). Medical care received the highest dimensional score (mean: 7.94 ± 1.5), while facility infrastructure recorded the lowest (mean: 6.37 ± 1.9). The questions with the highest and lowest scores were “How would you rate this facility regarding the treatment by medical staff?” (mean: 8.33, SD ± 1.7) and “How would you rate this facility regarding the equipment?” (mean: 5.71, SD ± 2.7), respectively. Age ⩾ 47 years (β = .34; 95% CI: 0.02-0.67) was the main factor associated with a higher ESCOMA satisfaction score; on the other hand, patients who lived 2 hours from the health center had lower satisfaction (β = −.68; 95% CI: −1.09 to −0.28).
Conclusion:
User satisfaction with primary healthcare centers in Ucayali is favorable regarding medical care and staff treatment. However, perception is significantly lower concerning infrastructure and equipment availability. As the distance from homes to the health centers increases, satisfaction with medical care decreases. These findings highlight the need to improve physical conditions and equipment to optimize the quality of care in these institutions.
Introduction
Patient satisfaction, understood as the subjective evaluation of one’s experience with medical care, constitutes one of the three pillars of quality of care, along with clinical effectiveness and safety. 1 As such, it is a crucial performance indicator used to evaluate health systems, identify areas for improvement, and predict user adherence to services.2,3
In Peru, the primary level of care represents the fundamental access point to the healthcare system, comprising over 95% of the country’s infrastructure and theoretically responsible for serving 80% of the population. 4 However, a profound discrepancy exists between its strategic role and its material reality. A 2022 national assessment revealed that 94% of these facilities operate with inadequate installed capacity.5,6 This precariousness is especially severe in the Amazon region, the country’s largest, where the infrastructure gap reaches a critical 98%.5,6
The Peruvian Amazon, home to over 2500 native communities, 6 not only faces an infrastructure deficit but also exhibits the consequences of marked health inequality. Its maternal and infant mortality rates (28 per 1000 live births) 7 are significantly higher than those in other regions, such as the coast (17 per 1000 live births). 8 Although this objective data reveals systemic failures, the perspective of the main stakeholder—the patient—remains completely unknown. The user’s voice, which could precisely identify the most deficient dimensions of care, remains unexplored.
This lack of information represents a blind spot for decision-making and the formulation of cost-effective public policies. In this context, the present study aims to evaluate the degree of patient satisfaction at the primary level of care in the Peruvian Amazon. It seeks to understand their satisfaction with the care provided in the health centers they attend and, furthermore, to identify specific local needs to improve these facilities, which often represent the only available access to healthcare for the population of this region.
Methods
Study Design and Setting
An observational, cross-sectional, and analytical study was conducted. on patients affiliated with the EsSalud Aguaytia Medical Post located in the province of Padre Abad and the EsSalud Contamana Medical Post located in the province of Contamana, both in the Ucayali region. The EsSalud Ucayali Health Social Security network serves over 166 700 insured individuals through five primary care establishments and a category II-2 hospital, the latter located in Pucallpa, the regional capital. 9 The Peruvian Amazon is the region with the lowest coverage of insured individuals, which evidences a gap in healthcare access. 9 The manuscript was drafted following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 10 guidelines for reporting observational studies (Supplementary Material 1).
Population
We included adult patients (18 years and older) affiliated with one of the two EsSalud Ucayali network healthcare centers. Healthcare personnel and administrative staff were excluded, as the study aimed to measure the degree of satisfaction from the patient’s perspective. Patients who did not wish to participate in the research were also excluded from the study.
The study employed a convenience sampling method, surveying all eligible users who agreed to participate during the data collection period. A post hoc statistical power calculation was subsequently performed to assess the adequacy of the sample size. The analysis was based on a one-sample mean test, using the final sample size (n = 465), a standard deviation (SD) of 15.5 derived from a similar population, 11 and a two-sided significance level (alpha) of .05. Based on these parameters, a statistical power of 99.9% was obtained, indicating that the sample was sufficiently large to reliably detect a meaningful deviation in the mean satisfaction score.
Procedures and Techniques
After obtaining ethics committee approval and authorization from the EsSalud Ucayali network, data collection proceeded between April and May 2025. First, two investigators trained for correct survey completion invited patients to participate after they had finished their medical care and/or completed their activities within the healthcare center. After the invitation, they were informed about the anonymity of the surveys, the risks and benefits of participating in the study, and also about informed consent. If the patient agreed to participate in the study, they signed the consent form and proceeded to complete the survey. If the patient had any questions during the survey, the interviewers resolved them. The surveys were transcribed into a Microsoft Excel database where the first quality control was performed. This consisted of verifying the physical surveys twice and checking that the information in the database was the same. Surveys with more than 10 missing items (n = 15) were excluded from the final analysis. For the remaining surveys with sporadic missing data, a complete-case analysis (listwise deletion) was performed, meaning that calculations involving a variable with a missing value for a specific patient excluded that patient only for that specific analysis.
Instrument and Variables
Outcome Variable
The survey consisted of three sections, ordered as follows: (1) sociodemographic characteristics (nine questions); (2) perception of the healthcare facility and services they frequented most continuously (seven questions); (3) ESCOMA satisfaction scale (17 questions).
To evaluate the degree of satisfaction, we used the ESCOMA Questionnaire, an adaptation of the Outpatient Consultation User Satisfaction Scale (SUCE) developed in Spain. The ESCOMA scale was adapted and validated to improve its understanding among the Peruvian population. The validation study was conducted on 13 814 adult patients, cared for in outpatient medical consultations at healthcare service provider institutions (IPRESS) in Peru. The Confirmatory Factor Analysis showed acceptable goodness-of-fit indices (CFI = 0.945; TLI = 0.937; SRMR = 0.036), supporting its use as a standard instrument to evaluate satisfaction in the quality of health services. 11 The ESCOMA satisfaction scale is composed of 18 items grouped into three dimensions: dimension one (Satisfaction with administrative processes dimension) has six questions, dimension two (Satisfaction with the facility’s infrastructure dimension) has eight questions and dimension three (Satisfaction with medical care dimension) has four questions, each item is rated on a 1 to 10 Likert scale, where 1 indicates a very low level of satisfaction and 10 represents a very high level of satisfaction. Due to the heterogeneity in the number of items per ESCOMA dimension, the total scores for each dimension are not directly comparable. To allow for a valid comparison and clearer interpretation, the mean item score was calculated for each dimension (sum of its item scores divided by the number of items in that dimension) and for the total ESCOMA score. In this way, all dimensions and the total score were expressed on the same original scale (from 1 to 10), facilitating the identification of the areas with the highest and lowest satisfaction. For the purpose of interpretation, scores were subsequently categorized into three levels: “low satisfaction” (<6 points), “satisfied” (6-8 points), and “very satisfied” (>8 points) (Supplementary Material 2).
Statistical Analysis
The analysis was performed using the statistical software Stata v17. Categorical variables were described in absolute frequencies and percentages; numerical variables were described with measures of central tendency and dispersion. The mean ESCOMA score (range 1-10 points) was distributed with its median and interquartile range among the categorical variables.
The ESCOMA dimensions were described using their mean and standard deviation. The mean score of each dimension was calculated to compare the scores across dimensions. To identify associated factors, crude and adjusted linear regression models were employed. Variables that were significant (P < .05) in the crude model were included in the adjusted model, calculating the adjusted beta coefficients and their respective 95% confidence intervals (95% CI). Finally, a box plot was generated to display the ESCOMA scores and its dimensions, and the Wilcoxon signed-rank test was used to evaluate statistically significant differences between the median scores.
Ethical Considerations
We followed the research ethics guidelines of the Declaration of Helsinki. The research protocol was evaluated and approved by the ethics committee of Hospital II EsSalud, Pucallpa (Authorization Code: Nota N° 000282-DRAU-ESSALUD-2025) in April 2025. All patients signed the informed consent to participate in the research. To ensure confidentiality, all surveys were anonymous, and no personal identifiers were collected. The digital database was encrypted, password-protected, and stored on a secure server accessible only to the principal investigators.
Results
We surveyed 480 patients, of whom 15 patient records were removed due to incomplete filling (more than 10 missing data points), so we analyzed data from 465 patients (Figure 1). The majority were women (66.7%), and the median age was 40 years (interquartile range 31-52). The predominant marital status was married or cohabiting (64.3%). A total of 74.8% lived in the same city as the healthcare center (Table 1).

Participant flow diagram.
Characteristics of the Population and Distribution According to the ESCOMA Satisfaction Score.

Median and interquartile range.
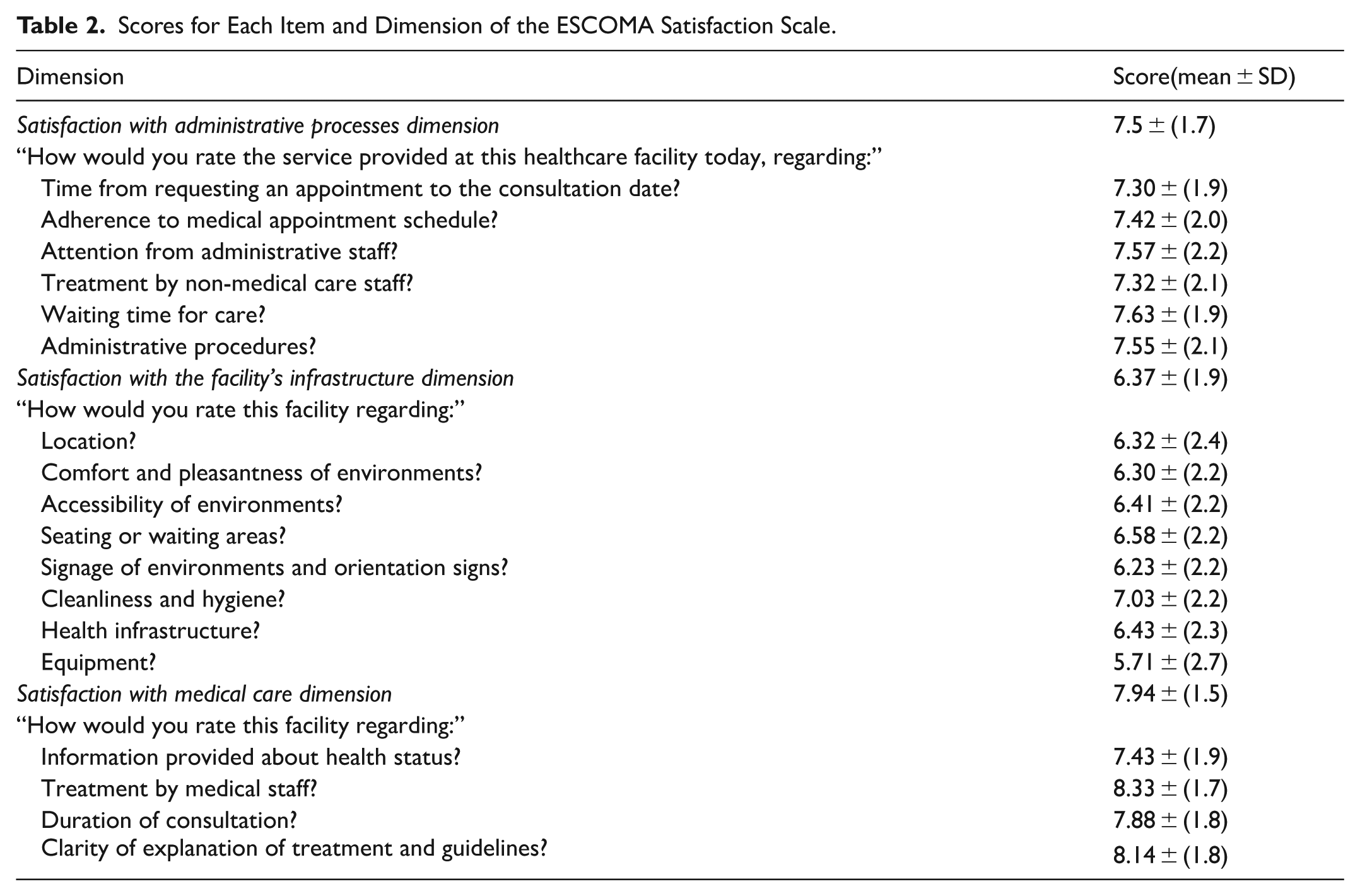
Regarding the ESCOMA score, the median total score was 7 points (range 6.17-8.28). The categorized ESCOMA scale indicated that 50.4% of patients were “satisfied” and 29.7% were “very satisfied” with the care received. The dimensions with the highest and lowest scores were satisfaction with medical care (7.94, SD ± 1.5) and satisfaction with the health facility’s infrastructure (6.37 SD ± 1.9), respectively; this difference was statistically significant. The questions with the highest and lowest scores were “How would you rate this facility regarding the treatment by medical staff?” (8.33, SD ± 1.7) and “How would you rate this facility regarding the equipment?” (5.71, SD ± 2.7), respectively (Table 2). Regarding the ESCOMA score by healthcare center, the median was 6.67 (IQR: 6-7.72) at Posta Médica Aguaytía and 8.11 (6.61-8.67) at Posta Médica Contamana; this difference in scores was also statistically significant (Figure 2).
Scores for Each Item and Dimension of the ESCOMA Satisfaction Scale.
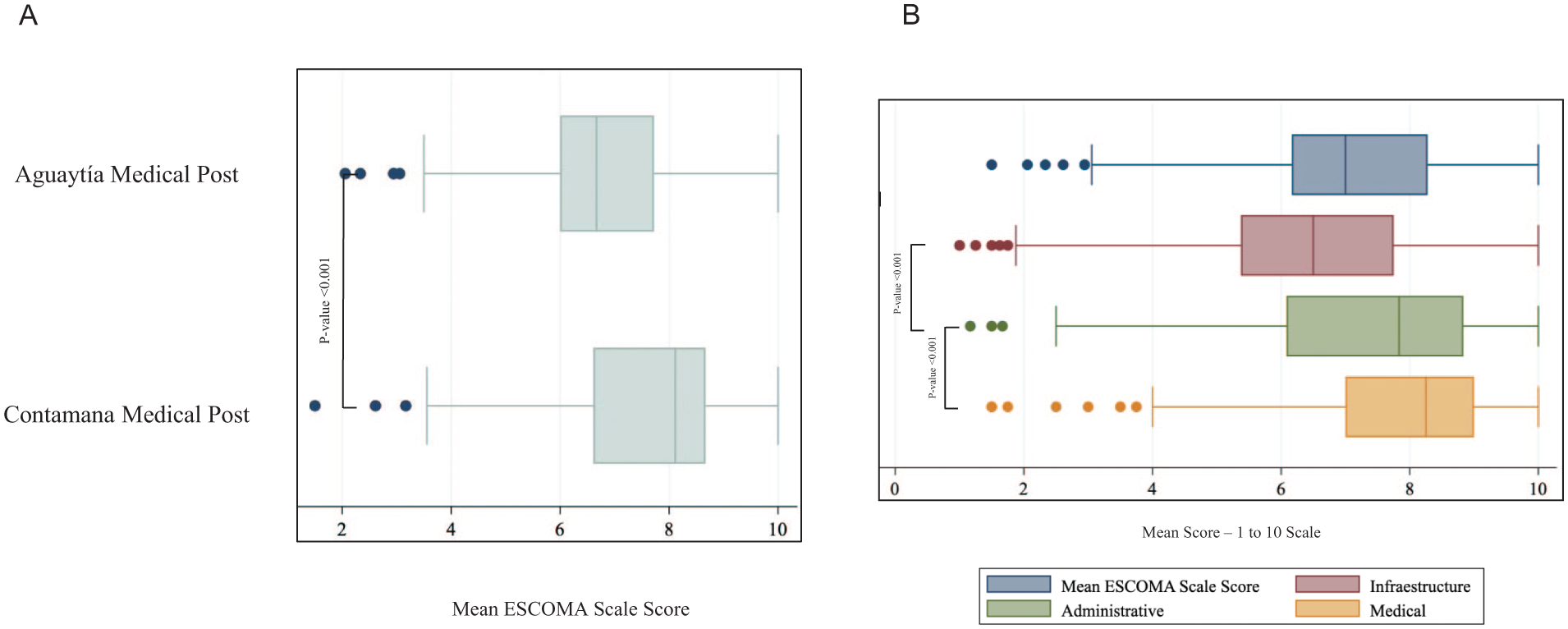
Distribution of the mean ESCOMA scale score and its dimensions by health center.
The multivariate linear regression analysis identified two factors independently associated with the ESCOMA satisfaction score. An age of 47 years or older was associated with a higher satisfaction score (β = .34; 95% CI: 0.02-0.67) compared to the reference group (those under 35 years old). Likewise, residing 2 hours from the healthcare center was significantly associated with lower satisfaction (β = −.68; 95% CI: −1.09 to −0.28) compared to living in the same city as the facility (Table 3).
Factors Associated with the ESCOMA Satisfaction Score.

Discussion
Main Findings
This study, conducted among 465 users of two primary healthcare centers in the Peruvian Amazon, reveals a picture of stark contrasts. While a vast majority of patients (80.1%) reported high overall satisfaction, this result appears to be driven primarily by the medical care dimension, highlighting the positive perception of staff treatment. In contrast, infrastructure was the lowest-scoring dimension, with critical deficiencies noted in the equipment. Additionally, the multivariate analysis identified longer travel time to the healthcare center as the main factor independently associated with lower satisfaction.
Contrast Between Studies
The low satisfaction with health center infrastructure, a central finding of our study, is consistent with the profound health inequalities documented in Peru, 12 particularly the critical infrastructure gap in the Amazon region.12,13 In fact, our finding that longer travel time is the main factor associated with lower satisfaction provides empirical validation, from the patient’s perspective, of these geographical barriers already described in the literature. 12 This approach aligns with Bambra et al, 14 who emphasize how social structure shapes the distribution of health, disease burden, and even mortality. Their arguments invite us to question how political and public factors might be associated with the formation of these inequalities. In the same vein, the study by Carrasco-Escobar et al 15 highlights marked differences in health access between the coastal and rural areas of Peru, emphasizing the prolonged travel times to healthcare facilities in the Peruvian Amazon compared to coastal areas.
Despite the low rating in the infrastructure dimension, the majority of patients expressed satisfaction with the medical care received, notably highlighting the good treatment from healthcare personnel. This finding is consistent with what was reported by Hernández-Vásquez et al, 16 who indicate that residents of the Amazon tend to perceive greater satisfaction with health services compared to those on the coast. This apparent paradox could be explained by the effort of healthcare personnel in the Amazon, who, despite the limitations and inherent difficulties in these environments, strive to provide the best possible care—a commitment that is clearly valued and perceived by patients. Additionally, an interesting finding from our multivariate analysis is that older patients (⩾47 years) reported significantly higher satisfaction. This could be due to multiple factors not explored in this study, such as lower prior expectations or a different cultural valuation of the care received, which represents an interesting area for future qualitative research.
Placing our findings in a broader international context, comparisons with health systems in other low- and middle-income countries reveal important parallels. For instance, a study in the Kurdistan region of Iraq reported an overall satisfaction rate with primary care of only 31.4%, a figure markedly lower than the 80.1% found in our Amazonian cohort. 17 Crucially, the main barriers identified in that setting—inadequate services, lack of specialists, and poor availability of equipment and medicines—directly align with the deficiencies our patients reported in the infrastructure dimension. This dissatisfaction with the public sector often translates into a preference for private providers, as shown in another study from the same region where a majority of patients sought care in private clinics (46.3%) and hospitals (18.6%) despite the significantly higher costs. 18 Taken together, these studies suggest that while satisfaction in our Peruvian sample is comparatively high—likely sustained by the quality of the healthcare staff—the weaknesses in infrastructure place it in a vulnerable position. If left unaddressed, these deficiencies could erode trust and encourage a migration toward the private sector, similar to what has been observed in other contexts.
Implications
The findings of our study have direct implications for health policy management in the Peruvian Amazon. The marked user dissatisfaction with infrastructure and, specifically, with equipment, underscores the urgent need for health authorities to prioritize investment in these areas. While the warmth of staff treatment is a fundamental pillar, it cannot indefinitely compensate for material shortages that limit the quality and resolution capacity of care. Therefore, we recommend that improvement plans and budgets focus on providing modern medical equipment and maintaining physical facilities, as these are the deficiencies most critically perceived by the users themselves. Additionally, the fact that distance is a key factor in dissatisfaction reinforces the need to strengthen the problem-solving capacity of primary care centers to minimize the need for referrals to more complex facilities. Future research could adopt a multidisciplinary approach, combining patient perception with technical engineering and architectural assessments, to develop models of health facilities truly adapted to the Amazonian context. To contribute to this future direction, and based on our team’s multidisciplinary experience, we have developed a conceptual framework with architectural proposals for health facilities in Amazonian contexts, which is available as Supplementary Material 3.
Strengths and Limitations
To our knowledge, this is the first study in Peru that evaluates satisfaction with healthcare in an Amazonian region. The following limitations were encountered: first, given the observational nature of the study, we could not find a causal association between variables. Second, since it was not a multicenter study, our results may not be generalizable to all regions of the Peruvian Amazon. To reduce this limitation, we calculated a statistical power of 99.9%. Finally, being based on self-administered questionnaires, biases such as social desirability bias and recall bias might have been present; however, participants were informed that the survey would be anonymous, which could decrease this risk.
Conclusion
The results of this study show a satisfactory perception of users regarding the medical care received in two primary healthcare centers in Ucayali, highlighting the good treatment provided by medical personnel. However, significant deficiencies were identified in satisfaction related to the infrastructure and equipment of the establishments. These findings underscore the urgent need to prioritize investments in infrastructure improvement, acquisition of medical equipment, and strengthening the physical conditions of health services, with special emphasis on the Peruvian Amazon.
Supplemental Material
sj-doc-3-his-10.1177_11786329251405984 – Supplemental material for Patient Satisfaction in Primary Healthcare Centers: A Cross-Sectional Study in the Peruvian Amazon
Supplemental material, sj-doc-3-his-10.1177_11786329251405984 for Patient Satisfaction in Primary Healthcare Centers: A Cross-Sectional Study in the Peruvian Amazon by Wendy Ramos-Huanca, Cesar Copaja-Corzo, Guimel Palomino-Guerra, Rodrigo Vargas-Joaquin, Tomás N. Santana-Téllez, Edgar Parihuana-Travezaño, Orietta M. Barriga-Soto and Renza L. Gambetta-Quelopana in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329251405984 – Supplemental material for Patient Satisfaction in Primary Healthcare Centers: A Cross-Sectional Study in the Peruvian Amazon
Supplemental material, sj-docx-2-his-10.1177_11786329251405984 for Patient Satisfaction in Primary Healthcare Centers: A Cross-Sectional Study in the Peruvian Amazon by Wendy Ramos-Huanca, Cesar Copaja-Corzo, Guimel Palomino-Guerra, Rodrigo Vargas-Joaquin, Tomás N. Santana-Téllez, Edgar Parihuana-Travezaño, Orietta M. Barriga-Soto and Renza L. Gambetta-Quelopana in Health Services Insights
Supplemental Material
sj-pptx-1-his-10.1177_11786329251405984 – Supplemental material for Patient Satisfaction in Primary Healthcare Centers: A Cross-Sectional Study in the Peruvian Amazon
Supplemental material, sj-pptx-1-his-10.1177_11786329251405984 for Patient Satisfaction in Primary Healthcare Centers: A Cross-Sectional Study in the Peruvian Amazon by Wendy Ramos-Huanca, Cesar Copaja-Corzo, Guimel Palomino-Guerra, Rodrigo Vargas-Joaquin, Tomás N. Santana-Téllez, Edgar Parihuana-Travezaño, Orietta M. Barriga-Soto and Renza L. Gambetta-Quelopana in Health Services Insights
Footnotes
Ethical Considerations
The protocol was reviewed by the Research Ethics Committee of the Hospital II EsSalud, Pucallpa (Authorization Code: Nota N° 000282-DRAU-ESSALUD-2025) on April, 2025.
Consent to Participate
All patients signed the informed consent to participate in the research.
Author Contributions
Conceptualization: WRH; Data collection: GPG and RVJ; Statistical analysis: CCC; Manuscript draft writing: All authors; Critical review of the manuscript: TNST, EPT, OBS, CCC, and RGQ; Final version writing: All authors; Final version approval: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.