
Abstract
Background:
Low vision care and rehabilitation (LVCR) remains critically underdeveloped in sub-Saharan Africa, despite a high prevalence of moderate to severe visual impairment.
Objective:
This study assessed the current state of LVCR in five sub-Saharan African countries using a modified World Health Organization (WHO) health systems framework.
Method:
A qualitative design was employed, involving semi-structured interviews which were based on a modified WHO health system building blocks: governance and leadership, health service delivery, human resource, low vision aid and technology, and financing. Optometrists providing low vision care in Ghana, Nigeria, Malawi, Kenya, and South Africa were recruited as participants through a combination of stratified random sampling and snowballing. Thematic analysis was conducted to identify the underlying themes.
Results:
Practitioners reported systemic deficiencies across all five blocks investigated. Governance and leadership lacked clear policies, coordination, and data infrastructure. Health service delivery was characterized by poor coverage, the absence of dedicated LVCR centres, and limited integration into public health systems. Human resources were inadequate, with no structured training or recruitment of practitioners, and low recognition of the sub-specialty. Essential assistive technologies were largely inaccessible due to high costs and procurement challenges. Financing was insufficient, with patients primarily paying out-of-pocket and health insurance schemes offering limited support.
Conclusion:
None of the five blocks of the WHO health systems framework were adequate for LVCR in this study. Consequently, strengthening each block particularly governance, workforce development, and financing is essential for advancing equitable and sustainable LVCR systems in sub-Saharan Africa.
Introduction
Visual impairment is an emerging global health priority 1 that affects about 2.2 billion people globally. 2 Out of the six subcategories of quantifiable distance visual impairment (categories 1 to 6) by the World Health Organisation (WHO), 3 the moderate and severe levels of visual impairment (categories 2 and 3), often referred to as partial sight or low vision, present unique challenges among affected individuals. Persons with low vision are more likely to experience mental health challenges, have poorer health related quality of life, restricted mobility, face unemployment and various levels of stigmatization in their environment.4 -8 People with low vision have some useful vision that is usually optimized to reduce the impact of vision loss with the aim of increasing independence and removing barriers to essential activities of daily living. 9 The optimal use of residual vision is achieved through well-structured low vision care and rehabilitation (LVCR) programs.10 -12 However, this type of care faces challenges globally, especially in low and middle income regions despite having the highest burden of visual impairment.13,14 Sub-Saharan Africa has a comparatively lower capacity for providing this form of care with less than 10% coverage rates of low vision services therein. 15 Some of the limiting factors that explain this include inadequate human resources, lack of equipment and assistive devices, cost of care, etc.16 -18 For this reason, several interventions have been implemented in various sub-Saharan African countries to improve LVRC including provision of low cost low vision aids, 19 training of low vision care providers 20 and local production of low vision aids. 21 However, there is a scarcity of evaluations of the impact of these interventions using a systems-oriented approach.
The World Health Organization (WHO) developed a health systems framework comprising six building blocks to strengthen health systems towards universal coverage. The blocks within this framework are service delivery, health workforce, health information systems, access to essential medicines, financing and leadership and governance. 22 This framework has been used for more than two decades and forms the basis for other health systems frameworks. 23 It was developed to measure and evaluate health systems based on specific indicators in low- to middle-income countries. These indicators were designed to be quantitatively measured24,25 and therefore require quality data. A significant proportion of low- to middle-income countries have challenges with access to high quality data. Although some studies have used the framework to measure health systems quantitatively like in the case of prospectively assessing the performance of public health care systems in Ethiopia, 26 others have employed other methods. This includes the use of hybrid qualitative and quantitative methods in the assessment of hypertension in the public primary care system in Guatemala 27 and the use of only qualitative methods in evaluating health interventions in Zambia. 22 Others have adopted a review of literature to assess health systems using the same framework.25,28 Another characteristic of the framework is that it was developed for analysis at the national level. However, it has the advantage of being adaptable to sub-regional levels. Furthermore, it has also been applied to initiatives aimed at strengthening eye care systems in various sub-Saharan countries. For example, in South Africa, it was used to help formulate steps to integrate eye care into existing policy 29 and also to evaluate the integration of eye care into the primary healthcare systems in sub-Saharan Africa.16,30 The flexibility of the application of this framework in various settings and to different data sources makes it suitable for this study which relied on the perspectives of low vision practitioners due to data relating to LVCR being unavailable in most national data sources in sub-Saharan Africa. With this background, this study sought to use a modified WHO health systems framework to assess low vision care within sub-Saharan Africa from the perspective of LVCR practitioners.
Method
Study Design
A framework-guided qualitative study with phenomenological and case study elements using a semi-structured interview was employed in this study to explore the perspectives of optometrists engaged in LVCR across five countries in Sub-Saharan Africa. The adopted approach helped to gain in-depth insights into the experiences, challenges and other factors in the provision of low vision care and rehabilitation services that were essential in evaluating the WHO health systems framework. The Semi-structured interview helped to maintain consistency in the interviews and ensured all components of the health systems building blocks were sufficiently interrogated.
Inclusion and Exclusion Criteria
The population that were targeted for this study were registered optometrists who were providing low vision care within their respective countries. The practitioners were required to provide a range of services including identifying, examining and prescribing vision aids and/or vision rehabilitation to patients with irreversible vision loss. Persons receiving care should have low vision or moderate to severe visual impairment (MSVI) with a visual acuity range from 6/18 to 3/60 in the better seeing eye. Participants who practiced LVCR but where not optometrist were excluded from the study.
Sampling of Countries
Low vision practitioners in five sub-Saharan African countries were recruited for this study. The countries that were included were selected using stratified random sampling. Three out of the four regional blocks; western, eastern and southern Africa, were randomly selected with central Africa being the only region which was not included. Countries that used English as their official language were selected within each regional block. Countries that had more than one optometry program with at least one of them awarding university level undergraduate degrees and had graduated at least three cohorts of students at the time of the study were considered. Based on these criteria, the eligible countries were Ghana, Nigeria, South Africa, Malawi and Kenya. Table 1 shows the countries selected with their respective population and number of optometrist.31,32 It also shows a range of economic states from low income to upper middle income based on world bank data. 33
Characteristics of Countries Included in the Study.

Practitioner Recruitment and Data Collection
A prior relationship was not established between the researcher and the participants before recruitment. The optometry association in each country was contacted to help identify low vision practitioners and optometrists involved in LVCR. The practitioners participated in one-on-one in-depth interviews relating to the state of low vision care in their respective countries. A snowball sampling approach was used to recruit practitioners for the study. Since previous studies have documented few low vision practitioners across sub-Saharan Africa,34,35 a sample of 25 low vision practitioners with five from each country was expected. These practitioners were contacted and interviewed through phone calls, emails and video conferencing platforms based on their preferences. The date, time and medium for the interview were selected by the respondents. All the interviews were conducted by one member of the research team (CHA) to ensure consistency and reliability in the interview process. However, due to inherent differences in each country, some countries did not have enough participants to meet the minimum expected sample and this caused the interviews to end when all available respondents were interviewed. Secondly, based on the core indicators for the health systems framework no new information emerged after the second to third interview in each country. Three practitioners (one from Ghana and two from South Africa) were unable to respond to the request to be interviewed after initially agreeing to partake in the study. None of them gave a reason for declining the interview.
Modified Health Systems Framework
The WHO health systems framework was modified and used to guide data collection in this study. The original framework has six blocks which are: governance and leadership, health service delivery, human resource, health information, essential medicines and financing. The modified framework that was used omitted the health information block as this requires a review of national health information systems. The essential medicine block was modified to read low vision aids and technology as this was more applicable to this study.
The following indicators were used to measure the five blocks:
Governance and leadership: This was measured based on the existing national low vision development plans or its inclusion in national eye care plans.
Health Service delivery: The indicators for health service delivery were restricted to comprehensiveness, accessibility and coverage. The remaining indicators, such as the number and distribution of inpatient beds, outpatient departments per 10 000 population, general service readiness score etc., were not measurable or needed based on the design of this study.
Human resource: Optometrists who were involved in low vision care within the five countries were considered as the human resource. The key indicators for this were perceived adequacy concerning the number of low vision practitioners and an established system for recruiting and developing low vision practitioners (WHO, 2010).
Low vision aids and technology: Low vision care involves vision aids and other assistive devices aimed at optimal use of residual vision. The key indicator for low vision aids and technology revolves around their accessibility that was made up of a composite of availability and affordability.
Financing: The sustainability of LVCR is closely linked to adequate financing. The indicators and measurements that are recommended by WHO (WHO, 2010), which include total expenditure and the ratio of out-of-pocket payment to the total expenditure, were not applicable in this study and therefore indirect measures were used including the ability of facilities to procure low vision aids and the ability of patients seeking LVCR to pay for their care and what mode of payments were used thereof.
The interview guide was generated based on the indicators stated under each block. The guide was pre-tested on about 2% of the expected study sample. The results of the pre-testing was used to modify the guide. The length of the guide was reduced from 48 questions to 22, this helped to shorten the time for the interviews to an average of 45 minutes per participants.
Analysis
All interviews were audio-recorded and transcribed verbatim to ensure accuracy. Thematic analysis was conducted following Braun and Clarke’s six-phase framework 36 with the aid of QDA miner 5.0 software to support organization and coding of the data. The coding was done by CHA who is a male academic with expertise in LVCR and has prior experience with qualitative studies. The six phases involved familiarization with the data, coding, generating initial themes, reviewing themes, defining and naming themes, and producing the report. Coding consistency was maintained through periodic checks by authors DVS and NR to ensure alignment with the research study. The themes and sub-themes were therefore grounded in the data, reflecting both individual perspectives and broader trends relevant to low vision care in the region. Additionally, demographic data for each practitioner, including gender, years of experience, and low vision specific qualifications, were collected and summarized.
Ethical Considerations
Ethical approval for the study was obtained from the Human and Social Sciences Research Ethics Committee of the University of KwaZulu-Natal(HSSREC/00004324/2022). The study adhered strictly to the tenets of the Declaration of Helsinki on studies involving human subjects. Before participation, all individuals were provided with an information sheet outlining the study objectives, procedures, potential risks, and benefits. Sufficient time was allowed for practitioners to ask questions and discuss any concerns. Each practitioner then signed an informed consent form, affirming their voluntary participation and understanding of the research purpose, confidentiality measures, and their right to withdraw at any time without penalty. Furthermore, at the beginning of each interview practitioners were requested to affirm their agreement to participate in the study and provided approval for the interviews to be recorded.
Results
Sixteen low vision care practitioners from five countries participated in this study. The majority were male [11 (65%)]. One third of the respondents [5(31.3%)] were from Nigeria, with Ghana and South Africa having 4 (25%) respondents each. On average, practitioners had worked as optometrists for 15.9 ± 6.1 years, with years of experience ranging from 4 to 28 years. The average period that they had spent in low vision rehabilitation was 5.5 ± 3.2 years, with experience varying from 1 to 11 years as shown in Table 2. In Nigeria, all practitioners had completed a mandatory 4-year fellowship to qualify as low vision practitioners. Additionally, two practitioners from Ghana and one from Kenya had completed fellowship training in low vision care at LV Prasad Eye Institute in India. Other practitioners reported diverse training pathways, including 6-month programs with partner institutions in Europe, others assessed continuous professional development opportunities organized by non-governmental organizations.
Demographic Characteristics of Low Vision Practitioners.
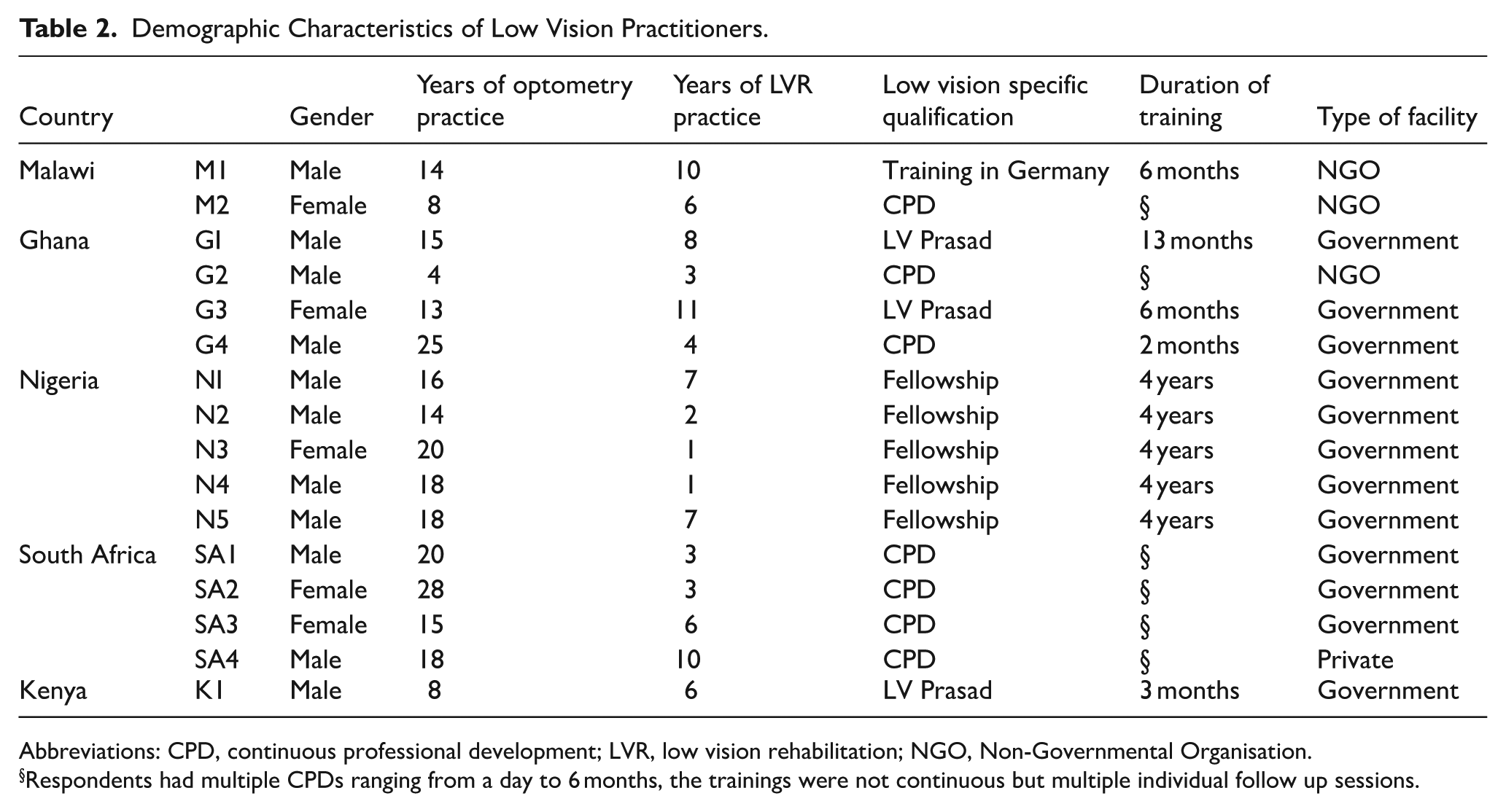
Abbreviations: CPD, continuous professional development; LVR, low vision rehabilitation; NGO, Non-Governmental Organisation.
Respondents had multiple CPDs ranging from a day to 6 months, the trainings were not continuous but multiple individual follow up sessions.
The thematic analysis was guided by the modified WHO health systems framework and comprised five blocks:
Governance and leadership;
Health Service delivery;
Human resource;
Low vision aids and technology;
Financing.
The themes and the portion of respondents that contributed to them are outlined in Table 3.
Distribution of Responses for Identified Themes.

Governance and Leadership
Three themes emerged under the governance and leadership block. These were:
Policies governing LVCR;
Coordination of LVCR activities;
Data availability.
Policies Governing Low Vision Care and Rehabilitation LVCR
The practitioners were not aware of current national policy documents that specifically governed low vision practice and development. However, some practitioners reported being aware of national eye health policies
For now, I don’t know of any such policies. So the only policy I know is a general policy about eye health. But one specific for low vision, I don’t think I’m aware about that for now. Maybe it might be there, but I don’t think I have seen or read something about that. (N2, Male)
A practitioner indicated that the current policy being implemented was from an initiative within the facility in which he practices rather than the government and this has improved detection of children with low vision and aided in proper placement of these children in schools.
There was no policy through the government. However, through a non-governmental organization [name redacted for the ensure anonymity], we have conducted several meetings with the Ministry of Disability, in Malawi. Up to now, the only policy that has come up, is the admission policy to Schools for the Blind. They say any child, before being admitted to the School for the Blind, they have to go through low vision therapist for assessments before going to (the) school. Otherwise, we don’t have any other policy as far as low vision is concerned, in Malawi (M1, Male)
The perceived absence of a policy framework for low vision practice and development had negative consequences for patients as practitioners expressed in the following comment:
We don’t have anything that deals with low vision, partial sightedness, or any vision disability and not having that, has had a ripple effect. We have a Department of Social Development where people with disabilities get care. They get grants, for instance, a social grant to assist them, obviously, especially when they’re not working. But even this Department of Social Development does not have standards for defining vision impairment, low vision, legal blindness. They don’t have it. The reason I’m saying that is, I will have two clients with similar vision function and I will write a recommendation and one will be granted a social development grant and (the other) one will be rejected. . . (SA1, Male)
Coordination of LVCR Activities
Most low vision practitioners were not aware of any coordinating or supervisory body responsible for coordinating low vision care within the country.
In an attempt to identify a possible coordinating body one practitioner indicated that the closest body was the Directorate of Eye Care in the region.
I think it is the director of eye care in the province. But they don’t coordinate as such. The coordination is limited to the compilation of statistics through the monthly reports. Incidentally, we told them (directorate of eye care) that, look, we want to start a low vision clinic. We took it upon ourselves to do that. They did not come to us to say, we want you to start this. No, it’s us who did that. (SA2, Female)
Another practitioner ascribed a coordinating role to the blind union within the country as they were responsible for distributing low vision aids.
Initially, it was left for the Kenya Society for the Blind. They were the ones the government has put as the resource centres where if you need any low vision device, educational materials, you get through them, but it’s really not working (K1, Male)
Data Availability
Data on low vision care seemed to be a major challenge in Sub-Saharan Africa. In some countries, the current prevalence of low vision was not available.
Actually, in terms of statistics, in Malawi, so far, we don’t have statistics of how many people have low vision, apart from the study that we are doing within our organisation. It’s only the number in blind schools that we collect (M1, Male)
This lack of data has an influence on the plan the country would have for the development of LVCR.
Again, I think the last prevalence study of any vision thing that happened in the province was undertaken around 2006, 2007, somewhere there. The question is, do we have a plan? It’s very important. Because we need to have evidence of, you know, prevalence and all those things, the RAAB [Rapid Assessment of Avoidable Blindness] studies and all that. But we don’t have at the moment that deals with the actual numbers. Either looking at those that present in the facility or taking the study out into the communities. At the moment, we don’t have such. (SA1, Male)
One practitioner indicated that the method of reporting information from the country did not provide information specifically on low vision activities. Another described his frustration in trying to modify the reporting format to include data on LVCR.
WHO has decided that in South Africa, there are two [indicators], the number of cataract operations done to prevent blindness, and the number of glasses you have prescribed. So, the information that is sent by us as a country to WHO talks to those two key performance indicators. (SA2, Female) I have tried to smuggle low vision into our strategy. But when it goes to the province, it doesn’t conform with the provincial indicator for our facility. So, it keeps getting kicked out. So, I think the issue now is more on the indicators that we use as a facility because I can do my monthly reporting, but it doesn’t reflect on any strategic platform that low vision is being practiced. (SA1, Male)
Health Service Delivery
Three sub-themes were identified under the health service delivery block. These were:
Coverage and distribution of low vision care centres
Integration of low vision service into the public health care system
Low vision clinic schedule and equipment
Coverage and Distribution of Low Vision Care Centres
The practitioners noted that the coverage of low vision care was low and ascribed this to the low number of practitioners involved in low vision care in relation to the population that needed to be served.
The coverage is still poor when we talk about low vision in Nigeria because Nigeria has a population of over 200 and something million people and the low vision specialists we have, I can tell you, I don’t think we are up to 100. In Edo state alone, which is one of the major states, the low vision specialists here are not up to; let me count, not up to 5. In Lagos too, I don’t think there are up to 10 low vision specialists in Lagos state. In Abuja, same thing. So, in the whole country, I don’t think we have more up to 100 low vision specialists. (N2, Male)
Another practitioner associated the low coverage with the negative experiences of potential low vision practitioners during their first few encounters with patients.
This is because the other optometrist I work with, I ask them, why are you not doing the low vision? Even though you have received training, you know, some time ago a workshop was organized. They even have their certificates. But they don’t do it. So the response I had was, Doc (Doctor), the outcome, most of them, the outcome is no good. It’s time-wasting, time-consuming. The patient will come and they will feel so emotional towards you. Meanwhile, there are other clients you need to attend to. So I think the care in this country is very low, very low because they feel as soon as they identify the condition, they just push the person away. (G2, Male)
Poor remuneration and lack of standardized training were also identified as contributing factors for the poor coverage and distribution of low vision practicing optometrists.
Brien Holden has been having this crash program so by now we should have had every square inch of this country covered by an optometrist who practices low vision but in terms of actualization that’s not yet forthcoming. Like I said they come and do their workshop they go back and they forget about everything they are not interested in practicing because low vision doesn’t fetch money as I said the clients are mainly people from poor backgrounds, so it doesn’t fetch money. In Ghana, there should be a dedicated centre where people can go and have adequate training in low vision and I think that would be the basis of sustainability. (G4, Male)
During the interviews, most practitioners were not able to mention more than three centres that provided low vision care. Distribution was a challenge as some regions in some countries did not have even one centre or low vision practitioner.
So far, I know, Blantyre is the main one, and another one at Queen’s. There’s Nkoma, In Lilongwe we also tried to establish another one, that was at the Central Hospital. Okay. But the challenge is that most of the optometrists are not really interested in low vision. So far, I can say, it’s only, you know, Blantyre, Nkoma and Queens low vision centres so far. (M2, Female)
Integration of Low Vision Service into the Public Health Care System
Most of the practitioners interviewed worked in public health facilities that were funded by the government. However, the low vision clinics were not separate units as they were part of the general services provided in the facility. Therefore, even though low vision services were provided they were not considered low vision centres.
I think in Nigeria, what we have is a general clinic. We don’t have a sub-section that has low vision. So, for now, we don’t have a low vision centre. (N2, Male)
Low Vision Clinic Schedule and Equipment
Practitioners provided general optometric care in their facilities and dedicated specific days that they provided LVCR services. In most cases, one day within the week was dedicated to low vision care and very few patients were booked.
I do general optometry. Then, I also have my low vision clinic in which I see my low vision patients once a week. I don’t book too much patients in the clinic. At least, maximum I book is three. But I prefer to have two because of the time I need to spend with the patients. (N2, Male)
A practitioner indicated that though he has a specific day for providing low vision service, he sometimes needs to compromise and provide care on other days as patients travel very long distances and some do not have the financial resources to return for the specific day dedicated to LVCR services.
So low vision days over here are Wednesdays. However, people come from different parts of the country. Some from Northern region, Volta region with a referral note. They don’t have, they don’t have anyone to contact. I’ve received a number of a good number of low vision cases on the other dates, which I still attend to them. As I mentioned, some are coming from far, far places, Volta Region and the others. So, they will be like, uh, look, I have to go back. Coming back, um, next week or the day you are giving me, won’t be that easy for me. (G2, Male)
The basic equipment needed to examine patients was not a challenge to most practitioners. A practitioner expressed his view on this in the context of the limitations posed by the economic environment.
We are in Africa. Equipment and gadgets we need are wide and varied. I would just say that we have the basics. We don’t have enough. That’s the humble truth. If there’s something like a humble truth or the honest truth. (N3, Female)
In places where equipment was unavailable practitioners used their personal kits even though they worked in a government funded facility.
. . . we do not have the low vision equipment. But by God’s grace, when I was in LV Prasad, because of the interest I had, I managed to buy the low vision kit for myself and that was the primary low vision kit I bought for myself. But post LV Prasad, I have managed to acquire one or two other things. So now, I use my own equipment to assist patients. (G3, Female)
Human Resource
Four major sub-themes emerged from the human resource block. These were:
The Low vision practitioner;
Motivation to practice LVCR;
Recognition of the low vision practitioner;
Training and Recruitment of low vision practitioners.
The Low Vision Practitioner
There were varied responses from practitioners on what they believed should be the definition of a low vision practitioner. One perspective was that an optometrist is equipped with the necessary skills to provide LVCR services.
When you come out of university, you are a low vision practitioner. When you come out into the practice world and actually work, you can choose to use your low vision, or not to use your low vision. You don’t have to do another course to become a low vision practitioner. So, to answer your question, every optometrist is a low vision practitioner; because they’re coming out of university qualified in low vision if they choose to do; that depends on the individual (SA4, Male)
Other practitioners described the need for additional training and certification to provide LVCR services.
a low vision practitioner is someone who’s got an optometry degree and has gone for further training to become a certified low vision practitioner (N3, Female)
In Kenya, optometrists are not officially recognized as low vision practitioners. Ophthalmic clinical officers are trained and certified to become low vision care practitioners.
Officially by the government is the OCO (Ophthalmic clinical officers), it’s all a tricky question because the government does not actually recognise optometrists. But as much as I’m working in a government setting, still an OCO will be in a position to even recommend who is legally blind. (K1, Male)
Motivation to Practice LVCR
The motivation to practice LVCR revolved around two things:
. . . a need for relevance and opportunity to be able to serve the undeserved in the facility where I work. (N3, Female)
The majority of practitioners made their final decisions based on the needs of the facility while others were encouraged by colleagues to pursue a career in the low vision sub-specialty
. . . along the line, I moved to Ocular Health because it was something I had interest in. But, an ophthalmologist, where I work, I told him that I was interested in Ocular Health. And he now said, no, no. He said, why don’t you think about going to low vision? That’s where most people are not really interested in. Go there and try and create a name. Or try and create something for yourself. And distinguish yourself among other professionals. (N2, Male) I think I’m one person whose interests are really stimulated by the need that I see in my workplace. When I start seeing quite a number of people in need of something that I know we have the capability to do, and that I can assist them with, then even if it was never my favourite subject, but I find myself having the responsibility to establish those services so that we can cater for that group of people. (SA3, Female)
Facilities that are equipped and provide low vision care serve as a catalyst for practicing optometrists to develop an interest in low vision.
I was motivated when I worked at one of the federal health institutions here. The ophthalmologists in that part of the country didn’t really have any low vision services. So when I saw the need, I discussed with them and they encouraged me. They’ve got low vision aids that they didn’t know how to use. So, I have something to start with if I actually went for training. So, it was the need that I saw in that special health institution that spurred me to go for a low vision specific qualification. (N5, Male)
Practitioners were divided about the role of undergraduate education in their decisions to practice LVCR. Whilst some believed it made a significant contribution others felt it was woefully inadequate.
I would classify it as just a sketchy training on low vision. That’s what I would describe my undergraduate knowledge of low vision to be [foundational]. Sadly, the emphasis was not really on low vision. We had it as a course, it was not in-depth enough you know. And so I couldn’t really, although I knew what low vision was all about, but it was not deep enough to know about it to be able to see low vision patients. (N4, Male) I think I still refer to all that I studied on campus. Yeah. So the training was very good, I must say. It was really, really very good. It was under the late Prof. Oduntun. So, he really gave us much on that. And yeah, it stuck since then. (SA3, Female)
Recognition of the Low Vision Practitioner
It emerged that in all the countries even in Nigeria where there was a residency program, low vision practitioners were not given any recognition by state agencies and did not get additional benefits in terms of remuneration or promotion. The situation was worse in Kenya where they were still trying to get optometry as a cadre to be recognized and employed by the Ministry of Health even though they have been graduating optometrists since 2012.
There are no such benefits. You become, low vision specialist, you work like a general optometrist, on top of that, as part of your duty, you are also involved in, a low vision assessment without any incentives. (M1, Male) In Kenya, the optometrists started in 2012. That was the first time they graduated. And still up to date, the government is not employing optometrists who are actually supposed to be in charge of low vision (K1, Male)
Training and Recruitment of Low Vision Practitioners
The general view of all the practitioners was that there were insufficient low vision practitioners in their countries. Furthermore, there was no active approach to recruiting future practitioners either. Most of the practitioners had not seen any advertisements for low vision practitioners throughout their careers. In all instances, they were employed as optometrists and largely through their personal initiatives acquired the additional skills to provide LVCR services for their patients.
I haven’t heard any advertisement concerning a low vision practitioner. I haven’t heard any facility looking for a low vision practitioner. (GI, Male) I’m employed as an optometrist in my facility, I have to create the awareness that I have got this exposure and this training and I can offer this (low vision) service. (N3, Female)
The most often adopted approach to increase the number of low vision practitioners has been sporadic short-term training courses. The irregular nature of these training courses failed to provide a continuous supply of low vision practitioners. Therefore, it is seen as a temporary solution and a more sustainable one is needed. However, the practitioners believed that such training courses have their place and are needed to help fill the wide human resource gap in low vision practice.
It’s about eye care. It’s about the people. It’s not about the practitioners. People need to see. People need to read. And then you can count the number of optometrists who are practicing this low vision. We are very few. (G1, Male) These two weeks of training I told you of, they have been having intakes. But sadly, I don’t get to see the products of these training coming up to like practice and see patients. . . But since we need more hands to be on deck, we are not discouraging anyone. Even people that go for the two weeks. You know, we are trying as much as possible to create the awareness. At least even if they are not able to review, they are able to identify and screen. They are able to refer. So, it is all part of the work. (N4, Male)
Low Vision Aids and Technology
Availability and affordability of low vision aids was a recurrent theme that emerged during the interviews as the availability of these aids were limited. This limitation was due to multiple factors including bureaucratic bottlenecks in government institutions, unprofitable for suppliers and difficulty in stocking. Due to the unavailability of these aids in the local market, practitioners often ordered the low vision aids from outside their countries and this led to complications.
So I’ll prescribe it (low vision aids) for them to go and get it if they don’t get it and they came back, then we will look on it online. Amazon and or go to the website of these companies that provide assistive devices. I used to order it in my accounts, you know, and then the patients will pay later and sometimes patients, come and the patient doesn’t have the money and I had already pre-financed it. Sometimes it comes and the patient’s vision or visual demand has changed and we need to change it again. And then it comes up to my cost and all that. So I decided that I won’t get myself involved, but rather I will get them to do the order themselves. (G3, Female)
Discussion related to the availability of these aids was accompanied with the issue of affordability. Practitioners mentioned that the cost of low vision aids were prohibitive, especially for electronic low vision aids. A practitioner summed up the thoughts and drew a link between the cost of these aids, their scarcity on the market and their effect on the practice of low vision care.
There is this perception that, it doesn’t pay. Remember, it’s almost a cost and effect principle here. It is not paying because patients cannot afford it. So, as a ripple effect, distributors find it unprofitable. Because, remember, from the practitioner’s point of view, most of them have a negative attitude in their approach to low vision. It wastes time. These people are almost in a hopeless situation. They don’t accept the aids anyway because they find it maybe cosmetically unappealing and all. (N5, Male)
Financing
The overarching theme for this block related to barriers to accessible financing for LVCR. The practitioners shared their experiences concerning the financing of low vision care and most indicated that one significant barrier was that patients had to pay out-of-pocket to access such care. In some instances, there was a health insurance cover but this provided limited support and often did not cover the cost of the low vision aids.
NHIS is paying for 10,000 Naira. Now, that is what has been enshrined in the National Health Insurance Scheme provision for low vision assessment. A recent inclusion. And that 10,000 Naira, believe me, it goes nowhere. It is just taken as the initial assessment fee to be able to assess the low vision care at all. But when it comes to the devices, that doesn’t cover for it at all. (N1, Male)
Some practitioners believed LVRC services must be considered like any other form of illness or disability and patients should obtain these vision aids at no charge.
Low vision devices like spectacles, like contact lenses are a treatment to our patients, right? They are the treatment plans we have for our patients. For me, it’s the same as a patient who needs some knee repairs, who needs some major surgeries, who needs any other form of treatment that they get for free when they come to the hospital facilities. So, I’m still really waiting for a time wherein our patients in eye care, they will also get everything without paying for them, you know, because it’s like a tablet (medicine) for them. (SA3, Female)
There was also mention of a financing policy that ensures insurance cover for persons with low vision but this was still in the draft stage and is yet to be officially implemented.
NHIS (National Health Insurance Service) scheme is bogus because it’s lumped. It provides an opportunity for a specialty care for the patient with eye needs that is not in primary care. But it’s not detailed if you understand what I mean. The policy is not yet detailed. But there is a policy that is being worked on now that incorporates the low vision needs, the services that we are able to offer. And we are hoping that it gets to the appropriate government offices (N3, Female)
Discussion
This study comprehensively evaluated the state of LVCR in five countries within sub-Saharan Africa using a modified WHO health systems framework. There were noticeable challenges in all the five building blocks which included poor governance structures, inadequate human resources, inaccessible low vision aids and lack of appropriate financing. The integration of existing LVCR into general eye care services and high motivation among practitioners were identified as enablers.
The governance and leadership block showed critical challenges including the absence of identifiable or up-to-date policy frameworks for LVCR, the lack of awareness of available policies among practitioners who were the primary implementors of such policy, lack of effective coordination of LVCR activities and non-existent data collection infrastructure. These are activities that should be the responsibilities of the respective states 37 as without clear governance, coordination is fragmented. The fact that some practitioners attributed policy implementation to NGOs rather than government initiatives implies the state often played a supporting role instead of leading. This lack of effective coordination, alongside inadequate data collection and the absence of reliable indicators, limits the ability to evaluate progress or identify service gaps in the field of LVCR. Even if governments are unable to finance such activities, it is imperative that they establish goals through policy direction, empower the necessary government agencies and play a coordinating role to bring together relevant stakeholders to help achieve the proposed targets.37,38 A good policy framework should provide the necessary structure for standardizing service delivery, guiding resource allocation, and integrating LVCR into broader health and disability services. 38
One positive practice noted in the health service delivery block was the integration of low vision care within general optometric services in most public health facilities. However, these services lack appropriate structure with most practitioners operating without dedicated centres, offering low vision services on specific days and sometimes using personally owned equipment. This severely limits coverage, continuity of care, and referral capacity.39,40 The service delivery approach by the health facilities was often clinic-centred which does not incorporate the broader rehabilitative and social needs of patients with MSVI41 -43 and may limit the possibility of providing holistic and interdisciplinary care required by these individuals. A potential solution could be for governments and relevant state institutions to recognize LVCR as a distinct sub-specialty, support the creation of dedicated service days and centres at all levels of care, and formalize referral pathways to social and educational rehabilitation services.
The study identified a myriad of human resource challenges which included a shortage of trained LVCR practitioners, with no structured recruitment or retention systems and no additional remuneration or promotion benefits for practitioners. There is an over reliance on individual motivation or NGO sponsored training programs which has been known to be unsustainable 39 except in Nigeria where a formalized fellowship program that also trains low vision practitioners have been instituted. Most of the practitioners felt they were not receiving due recognition for their work whilst the facilities they work in benefited from a stream of referrals with the accompanying prestige of providing specialist services. There was also a lack of consensus on who qualifies as a “low vision practitioner,” with some considering all optometrists as qualified by virtue of undergraduate training, while others felt that to be inadequate and insisted on additional formal certifications. In countries like Kenya, systemic barriers prevent even basic recognition of optometrists in public service and therefore they cannot be included in any state programme that aims to train or recruit low vision practitioners. There is a need for consensus on the definition of a low vision practitioner and the required qualifications needed to practice (if any). Such practices will form the foundation needed to advocate for state level recognition of LVCR practitioners.
Practitioners reported significant availability and affordability constraints to accessing low vision aids and technology. Bureaucratic delays, lack of local distributors, and minimal health system procurement policies have left most practitioners dependent on imported devices, often at personal financial risk to practitioners. Moreover, even when these aids are prescribed, their costs are often prohibitive. This aligns with other reports of the low vision aids accessibility barriers in low-income contexts.17,44,45 None of the indicators relating to low vision aids and technology were met in any of the facilities. A reasonable long-term approach to resolve this was to integrate low vision aids into essential medical equipment and medicines lists, support local procurement and distribution chains, and subsidize or cover costs through health insurance schemes.
The finance block showed that across all countries, LVCR is underfunded, with patients paying for services out-of-pocket. Facilities were unable to purchase these aids and patients were unable to purchase them either. Insurance schemes, where present, offer limited or symbolic coverage which does not fully eliminate financial barriers. Practitioners suggested that vision aids should be treated like other essential medical treatments which are supported by disability equity frameworks.46,47
Limitations
The findings of the study may be affected by the number of participants included in the study which was not determined through a standard sample size calculation and consequently may impact it generalizability. However, the numbers reflect the scarcity of optometrist engaged in LVCR in SSA. There was limited focus on country specific challenges in the process of identifying the themes due to the scope of the study. However, where there were contrasting viewpoints or situations in different countries, these were pointed out in the sample quotations and the respondents’ identifiers were linked to their country of origin. Nevertheless, the study does not report on inter-country differences within sub-Saharan Africa and this could be evaluated in future studies.
Conclusion
This study reveals the poorly coordinated and under-resourced nature of LVCR in sub-Saharan Africa. Despite having some committed low vision practitioners barriers relating to systemic gaps in policy, training, financing, and infrastructure hinder the effective delivery of LVCR services. The indicators of each of the five blocks in the modified WHO systems framework could not be met. There was almost non-existent governance and leadership and human service delivery was not comprehensive and suffered from low coverage. Furthermore, human resources were inadequate, low vision aids were not accessible, and financing was a significant challenge with out-of-pocket payments being common. Therefore, to meet the diverse needs of millions of individuals living with visual impairment, strategic investment, stronger governance, and better cross-sector collaboration are urgently needed.
Footnotes
Ethical Considerations
The Humanities and Social Sciences Research and Ethics Committee of University of KwaZulu-Natal (HSSREC/00004324/2022) approved the study.
Consent to Participate
All participants provided written informed consent before the interview and a verbal one during the interview. This was obtained by CHA.
Author Contributions
CHA: Conceptualization, methodology, investigation, formal analysis, writing original Draft, visualization. DVS: Conceptualization, methodology, project administration, review and editing. NR: Conceptualization, methodology, formal analysis, validation, review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data is not publicly available due to ethical restrictions. Anonymized versions can be provided through an email request to the corresponding author.