
Abstract
Background:
Calibration of medical devices is vital for diagnostic reliability, quality healthcare delivery and patient safety. While awareness is critical, the confidence of healthcare professionals (HCPs) in calibration-related knowledge significantly influences adherence to best practices in calibration-related tasks. However, this area is underexplored in sub-Saharan Africa.
Objectives:
This study aimed to assess the confidence levels of HCPs in Ghana regarding their calibration-related knowledge and competencies. It examined how these vary by professional role, training status, and years of experience.
Methods:
A cross-sectional survey was conducted among 461 HCPs in Ghana, including doctors, nurses, midwives and technicians/clinical engineers, using a structured questionnaire covering five thematic areas: general understanding of calibration knowledge, knowledge of calibration procedures, device-specific knowledge, training and institutional support, and the perceived impact on patient care.
Results:
Statistical analyses revealed variations in sentiment scores across profession, experience levels and training status. Technicians/clinical engineers consistently reported higher confidence, while doctors, nurses and midwives scored significantly lower. Additionally, respondents with prior calibration training, regardless of experience level, showed substantially greater confidence than their untrained counterparts.
Conclusion:
These findings demonstrate the need for targeted, hands-on calibration training and continuous professional development to improve confidence and competencies in calibration practices. Such initiatives are essential for effective device management and overall healthcare system performance. This study offers evidence to guide policy improvements and capacity-building efforts to strengthen calibration knowledge and practices in Ghana’s healthcare sector.
Keywords
Introduction
Medical devices are indispensable in modern healthcare diagnosis, treatment, and monitoring of diseases. They perform highly sensitive functions that directly influence clinical decision-making and patient outcomes.1-3 For instance, infusion pumps deliver medications with accuracies that exceed manual methods, substantially minimising administration errors.4-6 Similarly, advanced imaging systems like PET scanners have revolutionised early detection of diseases like cancer and facilitate early interventions for improved survival rates. 7 However, the performance of medical devices is not static. With use, environmental stressors, mechanical wear and tear, lapses in maintenance, and frequent movements degrade their accuracy.8-10 Performance deviations can compromise the effectiveness of diagnosis and therapy. To safeguard against such deviations, medical devices are calibrated routinely or on demand.10-12
Typically, technical personnel are tasked with performing calibrations, but given that healthcare professionals (HCPs) are the primary users of medical devices, their role in recognising calibration needs and initiating timely action is important.13-15 As such, HCPs should have sufficient knowledge and awareness of medical device calibration. Also, they must be confident in their ability to detect and respond to calibration issues correctly.3,8,16 Confidence is equally as crucial as the know-how. Confidence reflects not only their technical competence but also their willingness to act, especially in high-stakes clinical settings.
Studies have shown that HCPs with low confidence are less likely to initiate or complete clinical tasks, even when they have the requisite knowledge.17-21 By extension, low confidence could lead to hesitation and errors in calibration or even avoidance of calibration tasks. Conversely, HCPs confident in their calibration skills are more likely to incorporate medical device calibration into check-ups and routine maintenance and are, therefore, more likely to detect and address calibration issues before they impact patient care.13,22 This confidence enables them to advocate for best calibration practices, participate in decision-making for calibration training programs, and influence policies for best practices to ensure medical devices remain accurate and reliable.3,13 While increased confidence in calibration knowledge can improve patient outcomes, overconfidence may lead to diagnostic errors, and so an optimal balance of confidence is essential. A study by Yang et al 23 found that long-serving nurses often exhibit overconfidence in their clinical judgments, resulting in poor patient-care decision-making.
Despite the importance of confidence in medical device calibration, very few studies have explored this concept, particularly in resource-constrained settings like Ghana, where infrastructural and training deficits often challenge medical device maintenance and oversight. This study addressed this gap by systematically evaluating the confidence levels of Ghana HCPs in their calibration knowledge and skills. Since confidence directly impacts calibration effectiveness, this assessment helps identify knowledge gaps and the factors that affect confidence. It also sheds light on the effectiveness of current training methods and highlights areas for improvement. This assessment ensures that interventions enhance competence and prevent misplaced confidence to foster a sense of responsibility and caution in handling medical device calibration. The study advances the understanding of the behaviour of HCPs around calibration. It provides actionable insights to inform tailored capacity-building initiatives to improve calibration practices and reduce calibration-related risks for enhanced patient outcomes.
Methodology
Study Design
This study employed a cross-sectional survey design to assess healthcare professionals’ confidence in medical device calibration knowledge and practices in Ghana.
Study Setting
Apart from the University of Ghana Medical Centre, which is a quaternary facility and located in the capital, Ghana’s healthcare system is organised into three main levels: primary (eg, district hospitals), secondary (eg, regional hospitals), and tertiary (eg, teaching hospitals like Korle-Bu and Komfo Anokye). Most facilities are publicly owned and managed by the Ghana Health Service under the Ministry of Health, though private providers operate across all levels.
Sampling Strategy
A stratified purposive sampling strategy was employed to ensure broad representation across regions, facility types, and professional categories. Within each stratum, convenience sampling was used to recruit eligible participants based on availability and willingness to participate. While this method facilitated efficient data collection from a geographically diverse population, it may limit generalisability due to the potential for selection bias.
To mitigate this, we sought representation across:
all 16 administrative regions of Ghana,
public and private healthcare facilities,
all levels of care (primary to quaternary), and
multiple professional roles (doctors, nurses, midwives, and technicians/clinical engineers).
Eligible participants included clinical engineers/technicians, doctors, nurses, and midwives in active employment in a healthcare facility in Ghana, involved in routine handling of medical devices and patient care, and willing to consent to participation in the study. Healthcare professionals not engaged in direct patient care, such as administrative staff and medical interns, and who had not used any medical devices in their clinical roles within 6 months, were excluded to ensure relevance to current calibration practices.
Sample Size and Response Rate
Using Cochran’s formula at a 95% confidence level, 5% margin of error, and an estimated 50% response proportion, the minimum sample size was calculated as 384. To account for potential incomplete responses and improve robustness, we targeted 450 participants. The online questionnaire link was sent to 500 people, and we received 369 responses, yielding a response rate of 74%. For the in-person distribution, 133 questionnaires were given out, and 122 were returned, resulting in a 92% response rate. We followed up proactively with the questionnaires we sent to improve response rates and reduce non-response bias. In total, 491 questionnaires were returned, of which 30 in-person responses were incomplete and excluded from the final analysis. This left 461 fully completed questionnaires: 369 received online and 92 in-person.
Instrument Development
A 29-item structured questionnaire was developed specifically for this study, guided by:
The questionnaire was organised into six sections, with Sections 2 to 6 employing a 5-point Likert scale from Strongly Disagree (1) to Strongly Agree (5). The structure of the questionnaire is as follows:
(1) Sociodemographic information (11 items): Gathered background details of participants, including gender, age range, profession, and calibration training status.
(2) Understanding the importance of calibration (5 items): Assessed general understanding of calibration, its significance in healthcare settings, and its importance.
(3) Knowledge of calibration procedures (4 items): Evaluated knowledge of the practical aspects of calibration, familiarity with calibration schedules, and ability to distinguish calibration from general maintenance.
(4) Device-specific calibration knowledge (3 items): Examined confidence in abilities to recognise when devices require calibration, perform basic calibration checks, and follow device-specific manufacturer guidelines.
(5) Impact on patient care (3 items): Explored perceptions of the influence of calibration on patient outcomes, views on calibration training for healthcare workers, and confidence in current calibration practices.
(6) Training and support (3 items): Evaluated views on the calibration training sufficiency, resource availability, and the perceived need for continuous calibration education.
Item domains were established through consultation with biomedical engineers, clinicians, and health services researchers. The tool was developed from multiple validated sources rather than adapted from a single existing instrument to suit the local context. A pilot test with 10 HCPs showed good internal consistency (Cronbach’s alpha = .82) and informed wording adjustments for clarity.
Statistical Power
A post hoc power analysis was conducted, using G*Power version 3.1, for a two-tailed independent samples t-test comparing trained and untrained respondents. Using an effect size of .5 (Cohen’s d), a significance level of .05, and a total sample size of 461, the calculated power was >.95. This indicates a high likelihood of detecting statistically significant differences in calibration confidence scores between the two groups.
Bias Consideration
Several potential biases were acknowledged and mitigated:
Selection bias: Certain geographic or institutional clusters may be overrepresented due to convenience sampling.
Social desirability bias: Participants may have overstated confidence in calibration practices. To reduce this, the survey was anonymous and emphasised non-evaluative use.
Response bias: While the high response rate helps reduce concern, non-responders may differ systematically from responders.
Data Collection Process
Data was collected over 10 weeks from December 2024 to February 2025. Two modes of distribution were employed: online (via an anonymous Google Form) and in person (via printed questionnaires). For in-person administration, the researchers visited healthcare facilities to distribute questionnaires, which were returned within 1 to 2 weeks. The dual approach was adopted to maximise response rates and ensure inclusion of professionals in urban and rural areas, particularly those in facilities with limited internet access (Supplemental Material).
Data Analysis
The analysis of the data collected involved multiple steps to identify patterns and trends.
Data Cleaning and Preparation
The dataset was inspected to identify any inconsistencies. To facilitate quantitative analysis, responses to the Likert-scale questions (Strongly Disagree to Strongly Agree) were converted into numerical values using a predefined mapping (−2 to 2). However, demographic variables (calibration training status, occupation, age categories, education level, and years of experience) were retained in their original format to facilitate comparative analysis.
Descriptive Statistical Analysis
Descriptive statistics were used to summarise the demographic characteristics of participants and visualised using pie charts and bar charts. The average scores and standard deviations for each thematic section were computed to provide an overall sentiment score and understand the variation of responses per section. Additionally, for each question, the means and standard deviations of the sentiment scores were calculated.
Comparative Analysis
Comparative analysis was conducted to identify differences in sentiment and knowledge across various demographic attributes. The average sentiment for Likert-scale questions was calculated and compared among participants by calibration training status (Trained vs Untrained), years of experience (less than 1 year, 1-3 years, 4-6 years, 7-10 years, more than 10 years), and occupation (Nurse, Technician/Clinical Engineer, Doctor, Midwife).
Ethical Considerations
Participant anonymity and confidentiality were maintained throughout the study, which received ethical approval from the Komfo Anokye Teaching Hospital Institutional Review Board, Ghana (Approval Number KATH IRB/AP/183/24).
Results
Sociodemographic Characteristics of Participants
Of the 461 respondents, 56% were male, with the largest group (42.7%) aged 20 to 30 years. Most respondents (59.7%) held a bachelor’s degree. Nurses formed the largest professional group (42.3%), and nearly 40% reported having 1 to 3 years of experience in their fields. Regional representation was highest among healthcare workers in the Ashanti Region (22.9%). Most respondents were employed in public facilities (83.3%), and 38.4% worked in secondary-level hospitals. About 46% of respondents used 3 to 4 medical devices daily, and a majority were stationed in outpatient departments (31.7%) and intensive care units (24.1%). Additionally, over half (58.8%) reported receiving prior calibration training. Further details on respondent demographics are provided in Table 1 for context.
Demographic Profiles of Respondents.

Sentiment Analysis Across Sections
The analysis of Likert-scale responses across the five thematic sections revealed distinct patterns in sentiments and perceptions of HCPs (Table 2).
Average Sentiment Scores and Standard Deviations Across the Five Thematic Sections.

The Understanding the Importance of Calibration section demonstrated the highest average sentiment score (1.20 ± 0.82), with the statement “I am aware that inaccurate calibration can lead to incorrect patient diagnoses” averaging 1.30 (±0.77). The Impact on Patient Care section also received generally positive sentiment, with an average sentiment score of 1.06 (±0.88). The item “I believe that regular calibration of devices reduces the likelihood of patient harm” recorded one of the highest scores in the section (1.19 ± 0.79).
The average sentiment in the Knowledge of Calibration Procedures section was moderately positive, with a mean sentiment score of 0.83 (±1.02), and the statement “I know the proper steps to take if a medical device fails calibration” scored the lowest in the section (0.64 ± 1.14). The Training and Support section had an average sentiment score of 0.74 (±1.05), with the statement “I have received adequate training on how to calibrate the medical devices I use” yielding the lowest mean sentiment score in the section (0.44 ± 1.25).
The lowest sentiment score was recorded in the Device-Specific Calibration section (0.72 ± 1.06). The statement “I understand the manufacturer’s guidelines for calibrating the medical devices in my department” recorded the lowest average in the section (0.63 ± 1.11). Notably, all sections recorded at least one respondent selecting the maximum sentiment score (+2) for each item.
Analysis by Calibration Training Status
Across all sections, respondents who had received calibration training consistently reported higher sentiment scores (Table 3). The most pronounced difference was observed in the Device-Specific Knowledge section, where trained respondents recorded a mean sentiment score of 1.13 (±0.56), while untrained ones averaged only 0.14 (±1.02). Specifically, trained respondents agreed strongly with statements such as “I can accurately perform a basic calibration check on the devices I use” (1.07 ± 0.74), while untrained professionals scored considerably lower (0.06 ± 1.19).
Mean Sentiment Scores and Standard Deviations Across the Five Thematic Sections According to Calibration Training Status.

Significant gaps were also seen in Knowledge of Calibration Procedures (1.14 ± 0.56 vs 0.39 ± 0.86) and Training and Support (1.03 ± 0.62 vs 0.32 ± 0.89). Notably, trained respondents supported the need for continuous calibration education more, averaging 1.34 (±0.70) for the statement “I feel that continuous education on calibration is necessary for maintaining high standards of care”, compared to 1.16 (±0.83) for their untrained counterparts.
In the Understanding the Importance of Calibration section, trained respondents recorded an average sentiment score of 1.39 (±0.46), while untrained ones scored 0.94 (±0.68). Trained respondents reported particularly high mean sentiment scores for the statement “I understand the importance of regular calibration for medical devices” (1.42 ± 0.67), while untrained respondents scored notably lower (0.94 ± 0.86).
The smallest difference in average sentiment occurred in the Impact on Patient Care section, where trained respondents averaged 1.19 (±0.57), compared to 0.86 (±0.72) for untrained ones. The statement “I believe that regular calibration of devices reduces the likelihood of patient harm” recorded a mean sentiment score of 1.31 (±0.69) for trained respondents and 1.01 (±0.89) for the untrained.
t-Test Results by Calibration Training Status
The t-test analysis showed statistically significant differences between trained and untrained HCPs across all sections (Table 4).
Independent t-Test Results Comparing Confidence Levels in Calibration-Related Knowledge Between Trained and Untrained Respondents Across the Five Thematic Sections.
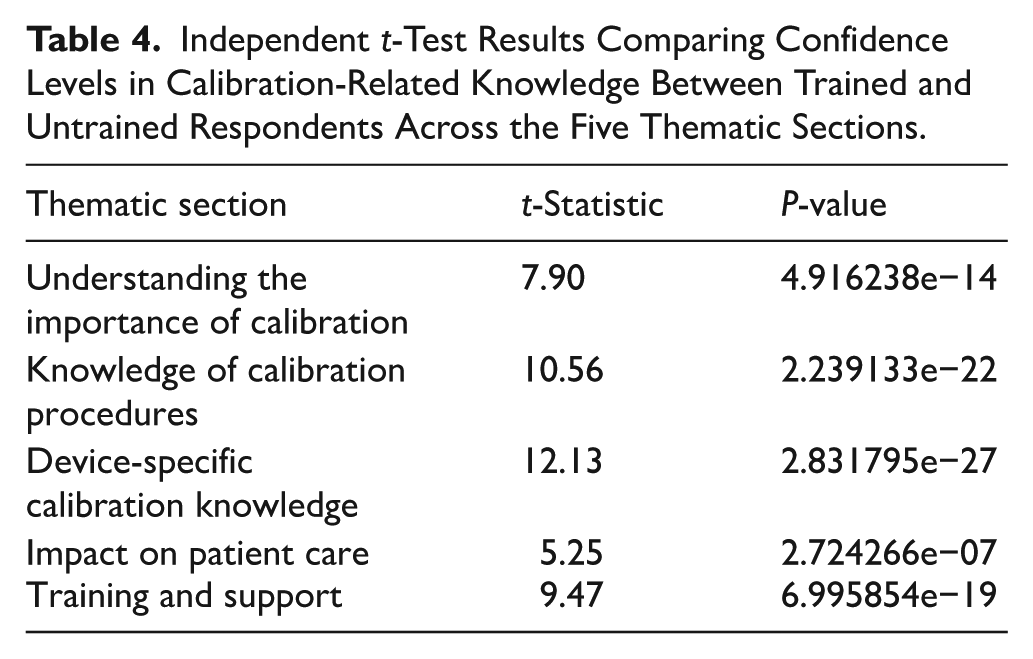
The Understanding the Importance of Calibration section had a t-statistic of 7.90, with a P-value of 4.916238e−14. Similarly, the Knowledge of Calibration Procedures section recorded a t-statistic of 10.56 and a P-value of 2.239133e−22. The most notable difference was observed in the Device-Specific Calibration Knowledge section, where the t-statistic was 12.13 (P = 2.831795e−27). The remaining two sections, that is, Impact on Patient Care and Training and Support, also demonstrated statistically significant differences between the two groups, with t-statistics of 5.25 (P = 2.724266e−07) and 9.47 (P = 6.995854e−19), respectively.
In all cases, the P-values were far below the conventional .05 significance threshold, indicating that the observed differences were not due to chance.
Sentiment Analysis by Occupation
The sentiment analysis across the different occupational groups showed certain trends (Table 5).
Mean Sentiment Scores and Standard Deviations for Each Thematic Section Across Occupations.

Technicians/clinical engineers recorded the highest average sentiment scores for all five sections, scoring highest in Understanding the Importance of Calibration (1.51 ± 0.47), Knowledge of Calibration Procedures (1.02 ± 0.73), and Device-Specific Calibration Knowledge (0.94 ± 0.88). They also demonstrated comparatively high scores in the Impact on Patient Care and Training and Support sections (1.16 ± 0.69 and 0.85 ± 0.84, respectively). Technicians/clinical engineers were followed by doctors, who exhibited relatively high sentiment, particularly in the Understanding the Importance of Calibration and Impact on Patient Care sections (1.29 ± 0.50 and 1.12 ± 0.57, respectively). However, their scores in Knowledge of Calibration Procedures and Device-Specific Calibration Knowledge were notably lower (0.94 ± 0.76 and 0.74 ± 0.92, respectively).
Midwives and nurses recorded relatively low mean sentiment scores across all sections. However, nurses performed slightly better than midwives in most aspects assessed (1.02 ± 0.60 vs 1.01 ± 0.79 for Understanding the Importance of Calibration, 0.71 ± 0.76 vs 0.64 ± 1.00 for Knowledge of Calibration Procedures, 0.63 ± 0.87 vs 0.54 ± 1.13 for Device-Specific Calibration Knowledge, and 0.66 ± 0.79 vs 0.64 ± 0.97 for Training and Support).
Analysis of Variance (ANOVA) by Occupation
An analysis of variance (ANOVA) revealed statistically significant differences across occupations in three sections (Table 6). The most significant was found in the Understanding the Importance of Calibration section, with an F-statistic of 20.25 (P = 2.444446e−12). Significant differences were also observed in the Knowledge of Calibration Procedures section (F = 5.33, P = 1.285102e−03) and the Device-Specific Calibration Knowledge section (F = 3.60, P = 1.361423e−02). However, no notable difference across occupations was observed for Impact on Patient Care (F = 2.46, P = 6.235924e−02) and Training and Support (F = 1.82, P = 1.418232e−01).
One-Way ANOVA Results.

Analysis by Calibration Training Status and Level of Experience
For trained respondents, mean sentiment scores were generally high across all experience groups (Table 7). Notably, those with 10+ years of experience consistently reported the highest scores in most sections (1.62 ± 0.36 in Understanding the Importance of Calibration, 1.29 ± 0.76 in Device-Specific Calibration Knowledge, 1.48 ± 0.59 in Impact on Patient Care, and 1.19 ± 0.75 in Training and Support). Those with 7 to 10 years of experience also had high sentiment scores, recording the highest in Knowledge of Calibration Procedures (1.30 ± 0.58), as did those with 4 to 6 years and 1 to 3 years of experience.
Mean Sentiment Scores and Standard Deviations Across the Five Thematic Sections, According to Calibration Training Status and Years of Professional Experience.
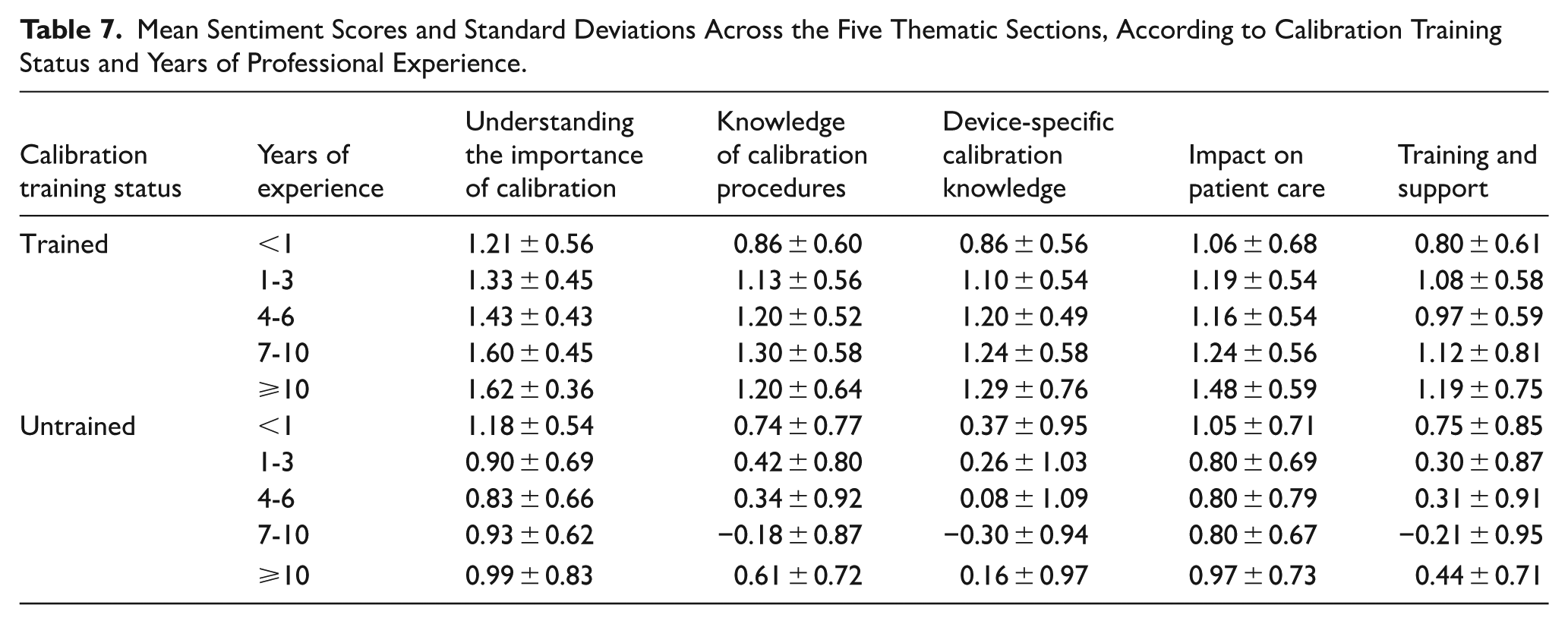
Untrained respondents with 7 to 10 years of experience recorded the lowest scores in most sections (−0.30 ± 0.94 in Device-Specific Calibration Knowledge, −0.18 ± 0.87 in Knowledge of Calibration Procedures, and −0.21 ± 0.95 in Training and Support). Those with 4 to 6 years of experience also reported low sentiments across all sections (0.83 ± 0.66 for Understanding the Importance of Calibration, 0.34 ± 0.92 for Knowledge of Calibration Procedures, 0.08 ± 1.09 for Device-Specific Calibration Knowledge, 0.80 ± 0.79 for Impact on Patient Care, and −0.21 ± 0.95 for Training and Support). Interestingly, untrained respondents with less than 1 year of experience recorded relatively higher scores across all sections, especially in Knowledge of Calibration Procedures (0.74 ± 0.77) and Device-Specific Calibration Knowledge (0.37 ± 0.95).
Discussion
This study provides key insights into the self-reported confidence levels of HCPs in Ghana regarding medical device calibration. The demographic distribution, dominated mainly by early-career professionals, suggests a workforce still developing technical proficiency. Nurses formed the largest group, and directly interacted with medical devices frequently, stressing the importance of strengthening their capacity in this area.
Respondents generally showed a strong understanding of the importance of calibration and its role in patient care. This is consistent with the literature identifying calibration as critical to ensuring diagnostic accuracy and effectiveness of treatment.8,11 The considerable decline in confidence levels, however, particularly in the Knowledge of Calibration Procedures and Device-Specific Calibration Knowledge sections, reflects a gap between knowing why calibration matters and how to engage in it effectively.
The consistently low scores in Training and Support also indicate an institutional shortfall in structured calibration education. This gap may be especially consequential in low-resource settings, where malfunctioning or miscalibrated devices can remain in circulation for extended periods due to limited technical oversight and supervision. 25
The strong association observed between prior calibration training and confidence, with trained professionals recording significantly higher confidence scores than the untrained across all domains, reinforces the critical role of structured training in improving skills and enhancing self-efficacy. Also, the differences in sentiment scores between trained and untrained groups were statistically significant across all sections, supporting findings from previous studies, which suggest that confidence in clinical performance is closely tied to training and practice.26,27
Interestingly, experience alone did not lead to higher confidence. Professionals with more experience but no calibration training often reported lower confidence than their recently trained counterparts. For example, untrained respondents with 7 to 10 years of experience recorded some of the lowest scores across the board. This challenges the common assumption that clinical experience or time in service naturally results in technical competence and confidence, and supports the findings of previous studies with similar findings. For example, in evaluating the effect of clinical experience, task difficulty, and time pressure on nurses’ confidence, Yang et al 23 found no significant difference in accuracy between experienced and student nurses, concluding that experience does not translate into higher confidence. Barsuk et al 28 also found that among clinical residents, greater clinical experience did not equate to greater skill. These studies underscore that, in the absence of targeted, skill-specific training, experience alone may not enhance performance or confidence, particularly in tasks like medical device calibration, which require technical precision.
Differences in confidence by profession were also pronounced. Technicians/clinical engineers reported the highest confidence levels across all sections, and were followed closely by doctors. Nurses and midwives, however, consistently reported the lowest levels of confidence across the board, despite being primary users of medical devices. This is consistent with findings from a similar study by Yayan and Zengin, 9 who observed low calibration knowledge among nurses and midwives in Turkey. This gap signals the need to integrate basic calibration principles into clinical education and ongoing professional development, particularly for frontline staff.
The results of this study suggest that calibration knowledge should not be limited to technical groups. All clinical end-users need a foundational understanding and confidence to identify when calibration may be required, communicate effectively with technical staff, and ensure patient safety.
This study has some limitations. The sample, though broad, may not fully represent HCPs across the entire country, especially in remote areas. Additionally, most participants were from public healthcare facilities, potentially affecting the generalisability of the findings across the Ghanaian healthcare sector. The study also relied on self-reported data, which may have introduced biases, with some respondents possibly overstating or understating their confidence in their knowledge and abilities. Future works could consider incorporating objective skill assessment methods and exploring more interventions to enhance knowledge and confidence across clinical roles.
Conclusion
The study reveals considerable variability in self-reported sentiment across professional roles, experience levels, and training status. Generally, respondents expressed high confidence in their understanding of the importance of calibration. Technicians/clinical engineers reported the highest confidence levels across all sections, reflecting their specialised training and direct involvement in calibration processes. Nurses and midwives, however, consistently reported lower scores, particularly in the more technical sections, pointing to gaps that require attention. Early-career professionals exhibited higher confidence than their mid-career counterparts, suggesting a decline in knowledge over time due to a lack of continuous training. Calibration training was also a strong predictor of higher confidence scores, emphasising the value of structured calibration-related educational programmes.
There is, therefore, the pressing need for continuous professional development, especially for lower-scoring groups. Equipping healthcare professionals with relevant and practical calibration training will significantly improve their confidence in performing calibration tasks, thereby contributing to the safe and effective use of medical devices in clinical care.
Supplemental Material
sj-docx-1-his-10.1177_11786329251378540 – Supplemental material for Confidence in Medical Device Calibration Knowledge and Skills Among Healthcare Professionals in Ghana: A Cross-Sectional Analysis
Supplemental material, sj-docx-1-his-10.1177_11786329251378540 for Confidence in Medical Device Calibration Knowledge and Skills Among Healthcare Professionals in Ghana: A Cross-Sectional Analysis by Benjamin Appiah Yeboah, Isaac Acquah, Mawusi Gbemavor-Assonhe and Emmanuel Agyenim Boateng in Health Services Insights
Footnotes
Acknowledgements
The authors would like to sincerely thank all healthcare professionals who participated in this study. Their cooperation and willingness to provide the necessary information were invaluable to the success of our research, and we deeply appreciate their contributions to our findings.
Ethical Considerations
This study was approved by the Institutional Review Board of the Komfo Anokye Teaching Hospital, Ghana, with approval reference number KATH IRB/AP/183/24. Written consent was given by respondents before participation.
Consent to Participate
Written informed consent was obtained from all participants in the study.
Author Contributions
Benjamin Appiah Yeboah: Methodology, Software, Data Curation, Writing—Original draft preparation, Formal Analysis, Investigation. Isaac Acquah: Conceptualisation, Supervision, Writing, Resources—Review & Editing, Project Administration, Visualisation, Validation. Mawusi Gbemavor-Assonhe: Writing—Original draft preparation, Data Curation, Methodology. Emmanuel Agyenim Boateng: Validation, Data Collection. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.