
Abstract
Background:
Affiliations between community and academic hospitals are increasing. However, their impact on transfer practices remains under-characterized.
Objectives:
To understand the impacts of hospital affiliation on transfer practices and hospital resource utilization.
Design:
Retrospective cohort study.
Methods:
We included patients ⩾18 years who were transferred from a 178-bed community hospital to a tertiary academic hospital between January 2015 to December 2019. Interrupted time series analysis was used to evaluate changes in outcomes after the affiliation in January 2017. Our primary outcome was the change in quarterly rate of early discharge (discharge within 48 hours post-transfer). Secondary outcomes included change in quarterly proportions of low-income patients, patients residing at a far distance from the hospital, and ICU admissions. We performed a sub-analysis in patients transferred to a surgical specialty that evaluated the tri-annual rate of operative management (surgical or interventional radiology procedure performed <72 hours after admission).
Results:
Among 144 included patients, 93 (64.6%) were transferred post-affiliation and 63 (43.1%) were transferred to a surgical specialty. No significant trends were seen across outcomes in the pre-affiliation period. Relative to the former period, there was a quarterly decrease in early discharge rates (P = .027) and a quarterly increase in the percentage of patients residing at a long distance from the transferring hospital (P = .027) after affiliation. There was also a relative tri-annual decrease in the rate of operative management (P = .039).
Conclusion:
Post-affiliation, the volume of transfers and utilization of resources at the receiving hospital increased. The percentage of transfer patients residing farther from the transferring hospital also increased.
Introduction
Over the past decade, there has been a rapid increase in hospital affiliations between rural or community hospitals and major academic centers.1-3 Affiliations can lead to important consequences for clinical operations, such as through enhanced access to specialist consults and shared electronic health records, but the impact of this trend on the quality of care itself remains debated.4-6 Following the affiliation, it is common for the affiliated hospital to use the name brand of the academic center. 7 This can increase patients’ confidence in the standard of care at the smaller hospital and may lead to an increased preference for such hospitals in patients seeking care.8,9
Transfer practices between hospitals have the potential to significantly impact patient outcomes. Appropriate transfer of complex cases allows these patients to benefit from the advanced interventions, resources, and experienced personnel present at high-volume academic centers.1,10-14 Conversely, an unnecessary transfer can contribute to worse patient outcomes, higher costs of care and resource utilization, and delays in care and an increase in fragmentation of care.15-17 Previous studies that evaluate the impact of hospital affiliation on transfer practices remain limited to a single specialty or disease, as such their results may not be generalizable across other disciplines.18,19
Several studies have investigated the impact of hospital affiliation on the quality and cost of care at participating centers.20-22 However, the impact of affiliation on patient transfer practices remains under-characterized. This study aimed to understand the impact of hospital affiliation on transfer practices and transfer patients’ utilization of hospital resources at the receiving hospital.
Methods
Ethical Approval
This study was carried out in compliance with the ethical principles for medical research involving human subjects outlined in the Declaration of Helsinki. Our institutional review board exempted our study from ethical review and the need to obtain informed consent from participants since it was a retrospective chart review study that was not expected to cause any harm to patients and where all information was de-identified (IRB Approval/Waiver No. 2022P002475).
Patient Population
We performed a retrospective cohort study. We included patients ⩾18 years of age who were transferred from the affiliated hospital (Wentworth Douglas Hospital; WDH) to the sponsoring hospital (Massachusetts General Hospital; MGH) between January 2015 and December 2018. We performed chart review for data regarding the patient’s demographics, transfer, and hospital course at the receiving hospital. Patients were excluded if data regarding the primary outcome (whether or not the patient experienced early discharge, ie, <48 hours after transfer) were absent. No sample size calculation was performed, and all eligible patients were included to maximize the available data.
Affiliation
An affiliation was formed between an academic, tertiary, Level I trauma center (MGH) and a 178-bed community hospital (WDH) in January 2017. Following the affiliation, an acute care surgery program was established, and the process for registering WDH as a trauma center was initiated. Monthly education sessions were arranged, which were open to all staff at WDH, including acute care surgeons, operating theater technicians, nurses, and emergency medical service staff. A multidisciplinary quality assessment committee was also established, comprising members from both institutions, and regular quality assessment sessions were held. A joint rotation system was established whereby the Trauma Medical Director at WDH rotated at MGH. Finally, a collaborative approach was used to delineate patients eligible for transfer; preference was provided to transfer patients from WDH, and efforts for repatriation of transfer patients to WDH were initiated.
Clinical Variables
We included the following patient characteristics: age, sex, race, ethnicity, insurance status, BMI, and comorbid conditions (Charlson Comorbidity Score at the time of admission to the receiving hospital after transfer), median family income, patient location type, and distance from the affiliated and receiving hospital. We also assessed the specialty that the patient was transferred to, the length of stay of the patient surgical or interventional radiology procedures that they underwent during their hospitalization. To assess the patient’s median family income, we merged the US Census Bureaus’ publicly available database that provides median family income according to the zip code. 23 We evaluated the patient’s location type, using the rural-urban commuting area database. 24 Finally, for the patient’s distance from either hospital, we used the National Bureau of Economic Research Zip Code distance database which provides the great-circle distance between two zip code regions. 25
Primary Outcome
We compared the rate of early discharge among transfer patients before and after the affiliation. We defined early discharge as discharge within 48 hours of the patient’s transfer.
Secondary Outcomes
We compared the rate of intensive care unit admission before and after the affiliation. We categorized the distance at which patients lived from WDH and MGH into quartiles. Patients in the third and fourth quartile were considered to reside at a long distance. We compared the proportion of transfer patients residing at a long distance from WDH and MGH before and after the affiliation. Similarly, we categorized patient income into 4 categories based on previously established quartiles of annual income (in line with the United States Nationwide Readmissions Database reporting practices). 26 Patients belonging to the first and second quartile were considered to have below median income. We compared the proportion of transfer patients with lower income before and after the affiliation. These analyses were considered secondary and hypothesis generating.
Sub-Group Analysis
We performed a sub-group analysis among patients who were transferred to a surgical specialty. We evaluated whether these patients underwent a surgical or interventional radiology procedure within 72 hours of their arrival.
Statistical Analysis
For demographic characteristics, we reported continuous variables as median (interquartile range) and categorical variables as frequencies (percentage). To compare demographic characteristics between patients transferred before and after the affiliation, we used a t-test or Wilcoxon rank-sum test for continuous variables and Pearson’s χ2 test or Fisher’s exact test for categorical variables where applicable.
We performed an interrupted time series analysis with the affiliation in January 2017 as the intervention to evaluate the change in trends of each outcome before and after the affiliation. We calculated a quarterly percentage of patients with early discharge and ICU admission. Similarly, we calculated the proportion of patients who resided at a far distance and had lower income each quarter. For the sub-group analysis, we calculated a tri-annual rate of patients who underwent a surgical procedure or interventional radiology procedure.
Details on the implementation and interpretation of ITSA in Stata are detailed in the literature. 27 Briefly, a regression model was fit to the data with the time of hospital affiliation landmarked as the ‘intervention’. The model estimates the slope and statistical significance of the linear trend of the outcome of interest over time, such as the percentage of patients undergoing early discharge, in the pre-affiliation period. The change in this slope relative to the pre-affiliation baseline, and its statistical significance, is then determined in the post-affiliation period to gauge the durable change in the trend attributed to the affiliation. The difference in the outcome in the interval immediately after the change in affiliation status is also compared with that expected by extrapolating the pre-affiliation trend. If statistically significant, this is taken to represent the immediate effects of the affiliation.
All analyses were performed using Stata version 17.0 (Stata Corp, College Station, TX). A P-value of <.05 was considered statistically significant. Our institutional review board considered this study exempt from review since it was a retrospective chart review study that was not expected to pose significant harm to patients.
Results
Demographics
We included 144 patients who were transferred from WD to MGH during the study period. The number of patients in each quarter is reported in Appendix Table A1. Among these 51 (35%) were transferred pre-affiliation and 93 (65%) post-affiliation. The majority of patients were White (96.5%), and non-Hispanic (95.8%). Most patients had private insurance (56.9%) followed by Medicare insurance (34.7%). The pre- and post-affiliation subgroups did not significantly differ across demographic characteristics including age, sex, Charlson comorbidity score (calculated at the time of admission to MGH after transfer), and insurance status. A summary of participant demographic information is reported in Table 1.
Characteristics of transferred patients pre- and post-affiliation.
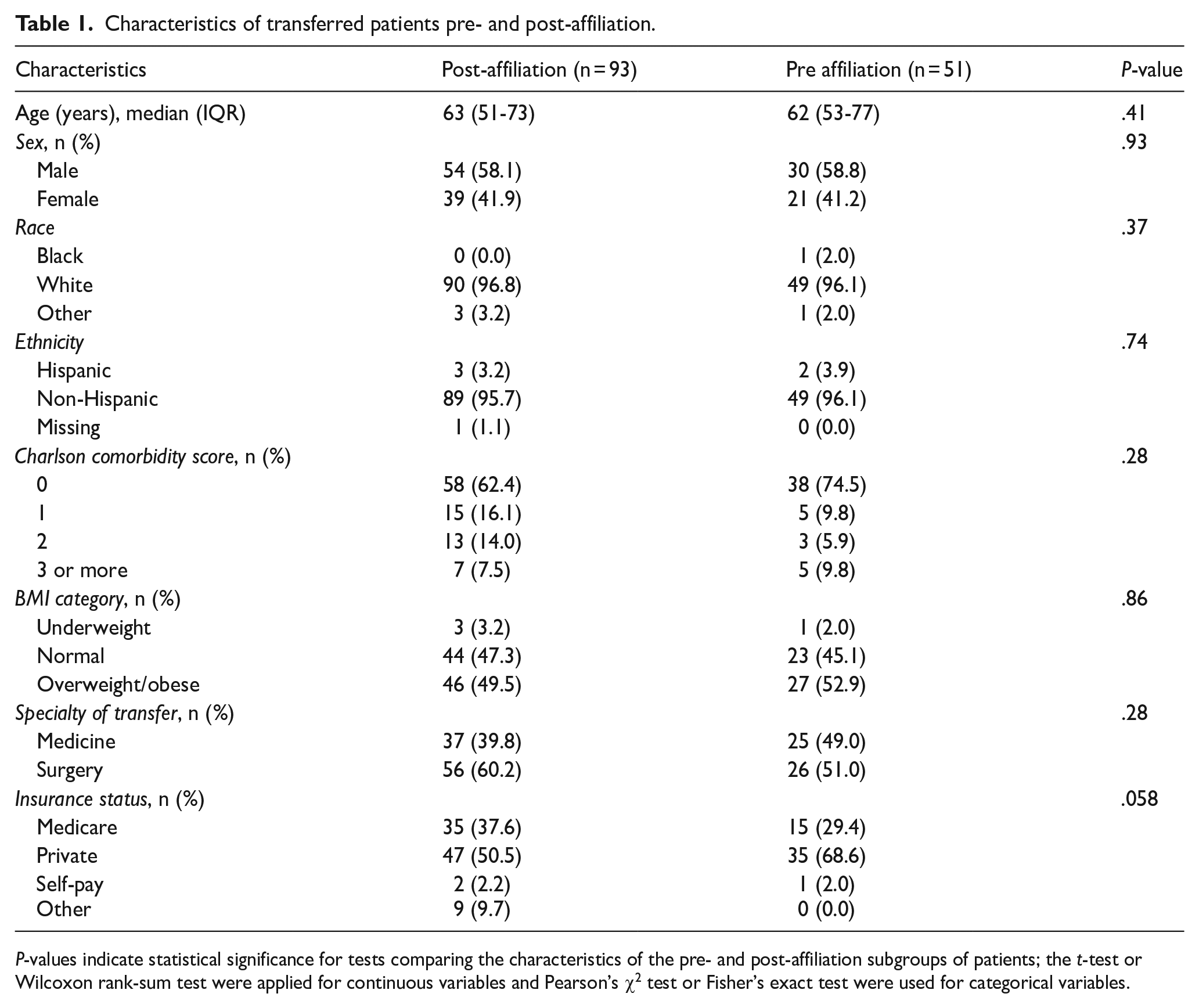
P-values indicate statistical significance for tests comparing the characteristics of the pre- and post-affiliation subgroups of patients; the t-test or Wilcoxon rank-sum test were applied for continuous variables and Pearson’s χ2 test or Fisher’s exact test were used for categorical variables.
Early Discharge
The quarterly percentage of patients discharged early did not demonstrate a significant trend during the pre-affiliation period (P = .091) and no significant change occurred in the first quarter post-affiliation between January 2017 to March 2017 (P = .272). However, a significant downtrend relative to the pre-affiliation period was seen thereafter and early discharge rates decreased by 5.4% each quarter (Coefficient: −5.40; 95% CI: −9.83, −0.98; P = .034; Figure 1 and Table 2).

Interrupted time series analysis of quarterly trends of the percentage of early discharge relative to the affiliation.
Interrupted time series analysis of trends relative to the affiliation in transfer patients.

Abbreviations: MGH, Massachusetts General Hospital; WDH, Wentworth Douglas Hospital.
Refers to the difference between the pre-affiliation and post-affiliation slopes, which is taken to indicate the effect of the affiliation over time.
Distance from the Hospital
The proportion of transfer patients residing at a long-distance away from WDH did not vary significantly pre-affiliation between January 2015 to December 2016 (P = .242) and did not shift in the first quarter post-affiliation (P = .272). However, a significant quarterly increase of 8.57% relative to the pre-affiliation period was seen over the subsequent study period (Coefficient: 8.57; 95% CI: 1.88, 15.25; P = .027; Figure 2 and Table 2).

Interrupted time series analysis of quarterly trends of the proportion of patients residing at a far distance from the transferring hospital relative to the affiliation.
Similarly, the percentage of patients residing at a long-distance from MGH was stable in the pre-affiliation period (P = .101) and in the first quarter after affiliation (P = .30). This percentage began to increase quarterly by 8.43% post-affiliation (Coefficient: 8.43; 95% CI: 1.88, 14.98; P = .027; Figure 3 and Table 2).

Interrupted time series analysis of quarterly trends of the proportion of patients residing at a far distance from the receiving hospital relative to the affiliation.
ICU Admission
The rate of ICU admission did not change significantly pre-affiliation (P = .481). There was no significant change in the rate of ICU admissions during the first quarter after the affiliation (P = .858). Finally, the change in ICU admission post-affiliation relative to pre-affiliation was not significant (Coefficient: −1.77; 95% CI: −6.55, 3.01; P = .482; Appendix Figure A1 and Table 2).
Patient Income
The proportion of patients with low-income did not vary significantly pre-affiliation (P = .82), in the first quarter post-affiliation (P = .881), or during the post-affiliation period (P = .682; Appendix Figure A2 and Table 2).
Subgroup Analysis
We included 63 patients in our sub-group analysis of patient transferred to a surgical specialty. The tri-annual rate of patients who underwent a procedure within 72 hours of transfer did not vary significantly during the pre-affiliation period (P = .24). Although a significant change was not seen during the first 4-month post-affiliation interval (P = .151), the percentage of patients undergoing surgical procedures declined by 5.78% (P = .039) per tri-annual period over the remainder of the study period (Appendix Figure A3 and Table 2).
Discussion
Changes in reimbursement policies, financial challenges, and a competitive market have led to historic increases in hospital affiliations.28-30 A critical aspect of the collaboration between affiliated hospitals is their transfer practices as part of patient triage or escalation of care. In this study, we analyzed the impact of hospital affiliation status on patient transfer practices. Our results demonstrate a significant downtrend in early discharge rates and a rising volume of patients who travelled greater distances to the hospital in the post-affiliation period. These findings suggest an increase in the utilization of recipient hospital resources after affiliation.
The increase in the number of transfers that MGH received may have been due to a preference for it as a transfer site after the affiliation. In a previous study Zachrison et al 19 showed that hospital affiliation was the most important hospital characteristics determining transfer destination after accounting for distance and structural network characteristics. The declining early discharge rates may indicate improved communication between the hospitals regarding transfer protocols that delineated patients needing transfer from those best managed locally. 8 A previous study examining transfer practices after a partnership between a Level II community trauma center and Level I academic trauma center also found a rise in transfer volume, especially for patients requiring advanced workup. 19 Additional factors such as age and comorbidities that may influence the timing of discharge after transfer did not differ significantly in the populations before and after affiliation. 31
Our findings also showed that there was an uptrend in the proportion of transfer patients who resided at a far distance from WDH post-affiliation. This may be reflective of an increase in the geographical catchment area and higher patient volume there. Previous studies have shown that forming an affiliation may improve public perception of the smaller community hospital. Chiu et al 9 showed that there are public expectations that physicians working at larger hospitals participate in care at the smaller affiliated hospital. The improved confidence in the care provided at the community hospital after affiliation has been shown to influence patient decisions to seek care there and may have contributed to patients traveling from farther away. However, these findings should be interpreted with caution since only a subset of the patients presenting to WDH is being considered.
Similarly, no significant results were seen in our analysis of the proportion of transfer patients with low-income status. However, it is unclear how informative this result is, given that nearly all included patients had private or Medicare insurance. Future studies on patients, particularly those who are not transferred, may investigate whether hospital affiliation status has differential effects on patients across levels of income or tiers of insurance.
Our subgroup analysis among patients transferred to a surgical specialty showed a significant down-trend in the proportion of patients who underwent operative management in the post-affiliation era. This could indicate the selection of more critically ill patients who may not have been fit for surgical intervention. In addition, the implementation of the acute care surgery at WDH may have improved its technical capacity to perform common emergent procedures and patients with surgical diseases may have been transferred for advanced medical work up or stabilization instead of the surgery itself. Previous studies have shown that smaller centers are able acquire the resources and expertise to manage surgical cases after an affiliation while transferring only patients requiring specific complex interventions to the larger hospital.3,32 Ultimately, this result should be interpreted with caution due to its limited sample size in the sub-analysis population and the unavailability of data pertaining to patients who were not transferred from WDH. Moreover, no significant results pertaining to rates of ICU admission were seen. Given these considerations, future studies that are adequately granular and powered to stratify results by disease subtypes and severity are needed.
This study has several limitations. Firstly, we only included patients transferred to MGH during the study period. The impact of the affiliation on non-transfer patients at both hospitals was not characterized. Importantly, post-affiliation changes in the volume and characteristics of patients presenting WDH were not captured. Reasons for transfer were also not consistently noted in patient’s charts and could not be incorporated into the analysis. In addition, due to the wide spectrum of diseases included, it was not possible to use a criterion to assess disease severity at the time of transfer. Thus, we cannot rule out differences in the characteristics of patients presenting to WDH before and after the affiliation status as having confounded our results. Secondly, we did not include a comparator hospital that did not enter an affiliation. Future studies should seek to include control series from hospitals that did not experience a change in affiliation status to obtain more robust results. It may be argued that the education and training sessions provided as part of the affiliation between the hospitals may have driven our findings and not the affiliation itself. However, we would assert that technical partnerships and cross-trainingw between teams is a natural part of agreements between affiliated hospitals and that it is valid for these effects to be impounded in the results observed. However, our findings may not generalize to scenarios where affiliations are not accompanied by preparation of hospital systems and staff to leverage their institutional partnerships effectively. Finally, we did not perform a sample size calculation for this study and instead included all patients who met the inclusion criteria in order to maximize the available data. However, while suggestive, our subgroup analysis of patients transferred to surgical specialties suffered from a particularly small sample size. We were able to derive a more meaningful result despite the small number of patients in this subgroup by using larger time-intervals for this prespecified subgroup analysis, but this result remains underpowered and hypothesis generating at best, in addition to our other secondary analyses, and larger studies are needed to characterize these trends across specialties and disease categories.
Despite its limitations, this study provides valuable insight regarding the impact of the affiliation on patient transfer practices. These results are of particular interest to surgeons, as there has been an increased emphasis on hospital and surgeon volume in the contemporary era with a corresponding shift towards inter-hospital transfers, referrals, and centralization particularly seen in fields such as trauma and emergency surgery and surgical oncology. As the healthcare system moves towards centralization and affiliations increase at a historic rate, it is important to understand the impact of the hospital affiliation on patient’s management practices and outcomes at the affiliated hospitals. It is also important to note that the terms and nature of the agreement and the consequent effects of the affiliation may vary between hospitals. This variation is important to consider and account for when assessing the impact of the agreement on patient care.
Conclusion
This study showed that the volume of patient transfers increased while the rate of early discharge decreased post-affiliation. In addition, the distance travelled by patients to both the transferring and receiving hospital increased. Among surgical transfers, there was a decreasing trend in of operative management. These findings suggest that hospital affiliation may lead to a more judicious selection of patients for hospital transfer.
Footnotes
Appendix
The number of patients included in each quarter.

| Quarter | Total patients |
|---|---|
| January-March 2015 | 2 |
| April-June 2015 | 4 |
| July-September 2015 | 7 |
| October-December 2015 | 4 |
| January-March 2016 | 3 |
| April-June 2016 | 9 |
| July-September 2016 | 10 |
| October-December 2016 | 13 |
| January-March 2017 | 11 |
| April-June 2017 | 5 |
| July-September 2017 | 12 |
| October-December 2017 | 10 |
| January-March 2018 | 10 |
| April-June 2018 | 14 |
| July-September 2018 | 21 |
| October-December 2018 | 9 |
Ethical Considerations
Our institutional review board considered this study exempt from review since it was a retrospective chart review study that was not expected to pose significant harm to patients.
Author Contributions
The study was conceptualized by W.R, D.A., J.O.H., G.C.V., J.J.P., and M.P.D. The study design and methodology was devised by W.R. and M.P.D. Data curation was performed by W.R., C.A., and E.L. Statistical analysis, tabulation, and visualization was performed by W.R. and O.M. The initial manuscript draft was written by W.R. and O.M., with subsequent review and editing by all authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Use of Artificial Intelligence
All authors affirm that no artificial intelligence tools were used in the preparation of this manuscript.