
Abstract
Aim:
To provide a comprehensive scientometrics analysis of Six Sigma research in healthcare, a field gaining momentum due to its capacity to address missed improvement opportunities and inefficient cost-control strategies across global health systems.
Design:
A cross-sectional mixed-methods study combining quantitative research and health metrics with thematic content analysis to explore trends and research patterns.
Methods:
The study analyzed publications indexed in PubMed, Scopus, Web of Science, SciELO, and KCI, using thematic mapping techniques through term co-occurrence networks and cluster analysis. Also, correlation analysis with healthcare quality indicators and global health metrics were executed.
Results:
A total of 883 publications were analyzed. (1) Geographical analysis showed 70.8% from high-income countries and 0.7% from low-income countries. (2) Thematic clusters were centered on hospital applications and patient safety. (3) Temporal trends revealed an increasing focus on “big data” and “health innovation.” (4) Strong correlations were found between publication output and health/research expenditure (P < .01 for all cases); negative associations emerged with out-of-pocket expenditures and researcher density in low-income settings.
Conclusions:
Findings provide a roadmap for aligning global research priorities and highlight the need for inclusive strategies that build research capacity and foster context-sensitive applications of Six Sigma in healthcare.
Introduction
Continuous quality improvement in healthcare services is essential for ensuring patient safety, optimizing resource utilization, and enhancing trust in health systems. 1 The Agency for Healthcare Research and Quality (AHRQ) identifies six domains of healthcare quality, routinely assessed through quality indicators, encompassing safety, efficiency, timeliness, effectiveness, equity, and patient-centered care. 2 Institutions with a thorough understanding and implementation of their healthcare quality systems tend to achieve superior service indicators and improved population health outcomes. 3 Therefore, the establishment of continuous improvement systems in healthcare services is indispensable.
The Six Sigma model has emerged as a pivotal strategy for quality management. 4 Initially developed within industrial settings, it was subsequently adapted to the healthcare sector. 5 This approach emphasizes the reduction of variability and the elimination of defects in processes, contributing significantly to enhanced clinical and operational outcomes.6-8 Six Sigma has been effectively implemented across diverse healthcare settings, leading to measurable improvements in patient outcomes, operational efficiency, and data-driven management. For example, in emergency departments, it has improved patient flow, 9 in clinical laboratories it enhanced diagnostic accuracy, 10 and in surgical care, it streamlined perioperative pathways. 11 It has also contributed to reducing infections, 12 optimizing pharmacy operations, 13 and minimizing insurance claim rejections. 14
Despite its recognized utility, the evolution, patterns, and characteristics of research on Six Sigma in healthcare, including its primary data, have not been robustly explored. This underscores significant knowledge gaps that necessitate resolution.
In alignment with standards of relevance and pertinence in biomedical research,15,16 the unequal geographical distribution of studies, the limited exploration of specific implementation areas, and the variability in methodological quality hinder the generalization of findings and the systematic adoption of strategies and outcomes in global contexts.15,16 The application of scientometrics and meta-scientific methods enables the identification of patterns, gaps, and priority research areas 17 while providing a critical evaluation of the quality within specific domains of biomedical evidence. 18 Scientometrics refers to the quantitative study of scientific literature to assess trends, productivity, and impact, while bibliometric approaches are specific tools within scientometrics that use citation-based metrics. Meta-scientific methods aim to evaluate the quality and structure of research systems. Based on this framework, the present study aimed to examine, for the first time, the evolution and characteristics of global research on Six Sigma in the healthcare sector from a scientometrics, and health and research indicators perspective.
This study was conducted and reported following the recommendations of the BIBLIO guideline (Guideline for Reporting Bibliometric Reviews of the Biomedical Literature) for preparing scientometrics/bibliometric studies. 19
Methods
Study Design
A cross-sectional mixed-methods study combining quantitative research and health metrics was conducted.
Data Sources
A systematic literature search was performed using Scopus, PubMed/MEDLINE, Web of Science Core Collection, SciELO Citation Index, and the KCI-Korean Journal Database. These databases were selected due to their high indexing standards and their coverage of health systems, biomedical sciences, and operations management, ensuring both breadth and rigor in capturing relevant Six Sigma research. The use of these resources has been previously validated and reproduced for similar studies.20-23
Search Strategy
A search strategy was developed using MeSH terms and synonyms to identify any document that followed the regular peer-review process and aimed to analyze, discuss, study, summarize, or explore the application or implementation of Six Sigma in healthcare. The search targeted literature within the thematic areas of life and health sciences systematically used by the bibliographic and citation databases, including medicine, nursing, dentistry, health professions, biochemistry, genetics, molecular biology, immunology, microbiology, neuroscience, pharmacology, toxicology, and pharmaceutics.
Initial pilot tests were performed with combinations of terms and tags across the different databases and search engines. Ultimately, the following example strategy yielded the most precise results: SUBJAREA (heal) OR SUBJAREA (dent) OR SUBJAREA (nurs) OR SUBJAREA (medi) OR SUBJAREA (bioc) OR SUBJAREA (immu) OR SUBJAREA (neur) OR SUBJAREA (phar) AND TITLE-ABS (“Six Sigma”) OR TITLE-ABS (“Total Quality Management”) OR TITLE-ABS (“Continuous Quality Management”) OR TITLE-ABS (“Sigma Metric”) OR TITLE-ABS (“Lean Six Sigma”). This example was the strategy used in Scopus and was adapted to the remaining databases and search engines.
Time Period
The search was conducted on July 27, 2024, in both English and Spanish. The initial title and abstract screening occurred between July 28, 2024, and September 30, 2024. A subsequent review was conducted from October 1, 2024, to November 10, 2024, to complete the collection of essential scientometrics domains and specific health metrics.
Eligibility Criteria
Publications were included in the synthesis and analysis if they met the following criteria: (A) Scientific articles published in peer-reviewed journals as part of a serial publication process; (B) Full-text availability; and (C) A clearly stated objective focused on examining, discussing, investigating, synthesizing, or exploring the application or implementation of Six Sigma in healthcare.
Exclusion criteria encompassed: (A) Conference proceedings, book chapters, books, errata, and retracted publications; (B) Documents lacking essential bibliographic details, such as author information, journal name, or correspondence details; and (C) Articles categorized as “in press.”
Publications originally released in languages other than English or Spanish were considered eligible if their abstracts were available in either of these languages and they fulfilled all inclusion criteria while avoiding any exclusion conditions. English and Spanish were selected due to their dominance in scientific publishing within healthcare disciplines, ensuring broad but manageable linguistic coverage for data extraction. Given the historical nature of the study, no restrictions were imposed on the publication year of the included documents.
Data Refinement
Following data retrieval from multiple databases, the records were exported in .CSV format, incorporating all available metadata, including document titles, author names and institutional affiliations, keywords, publication year, citation count, publication type, and other relevant bibliographic details. A preliminary manual review was conducted by two researchers to remove duplicate entries and assess the titles and abstracts for adherence to the inclusion and exclusion criteria. This initial screening was performed using Microsoft Office Excel 2016.
A subsequent evaluation was carried out by two researchers to complete the extraction of key scientometrics variables, healthcare quality indicators, and global health metrics. Any discrepancies identified during this phase were resolved by a third reviewer. Additionally, data standardization procedures were applied to enhance uniformity across the dataset. For instance, all review articles, regardless of methodological design (eg, narrative reviews, systematic reviews with or without meta-analysis), were classified under the category “reviews.” Similarly, letters to the editor, correspondences, notes, and commentaries were consolidated into the “letters” category. For the “country” variable, the corresponding author’s country of affiliation was used as the primary reference.
Data Synthesis and Analysis
To evaluate scientometrics domains, the quartile and h-index of each publication were obtained and adjusted by year. This information was recovered from the historical database of Scimago Journal & Country Rank (available since 1999) and the Journal Citation Reports (available since 1997), selecting the most favorable metric for the journal in which the document was published.
Countries were by income group, which includes low-income, lower-middle income, upper-middle income, and high-income. This classification is based on the 2024 World Bank open-access criteria. 24
For the domains related to healthcare quality indicators and global health metrics, quantitative indicators directly associated with health expenditure, disease burden, and health research and development were used. These indicators were recorded in their original measurements and classified by country or geographic region as appropriate. Data were extracted from open-access databases, including the World Bank, 25 the World Health Organization’s (WHO) Global Health Observatory, 26 and the WHO Global Observatory on Health Research and Development. 27 All indicators were analyzed in their original expressions and magnitudes.
Thematic, collaboration, and co-occurrence networks were constructed to assess the evolution, collaboration, and research patterns over time. Thematic analysis and cluster identification were performed using automated co-occurrence. To refine the visual analysis, a thesaurus file containing word names and variants was created to normalize terms of interest or exclude general terms. This bibliometric analysis was performed using the Bibliometrix package in R (version 4.3.1), the Matplotlib library in Python (version 3.9), and the VosViewer tool (version 1.6.18). Clusters were generated using VosViewer’s modularity-based clustering algorithm, which groups keywords based on frequency and co-occurrence strength.
A descriptive analysis was conducted to explore the baseline characteristics of scientific production. The Kolmogorov–Smirnov was used to assess the normality of quantitative variables. Quantitative data were presented as mean ± standard deviation or median and interquartile range, depending on the data distribution. Qualitative variables were summarized as frequencies and percentages. Correlation analyses used Spearman or Pearson coefficients to assess exploratory associations and correlations. Correlation analyses modeled publication frequency and the distribution of articles across journal quartiles (Q1-Q4) as dependent outcomes, using health expenditure, research and development (R&D) investment, and researcher density as independent predictors. A P-value of <.05 was considered statistically significant. All analyses were conducted using the R statistical package (version 4.3.1) (https://www.r-project.org/).
Ethical Statements
This study received approval from the Scientific Committee of the Universidad de la Costa (code GRA.2021-07-001-19). However, no humans, animals, or medical records were utilized as units of analysis.
Results
Scientific Production and Growth Trends
A total of 883 publications were included in the analysis after applying inclusion and exclusion criteria (Figure 1). Temporal analysis revealed a consistent increase in the frequency of publications related to Six Sigma in healthcare since 1999, the first publication, with projections indicating sustained growth over the next 5 years, primarily in Q1-Q2 journals (Figures 2A and B). The average annual growth rate was 11.25%. Articles constituted 81.4% of the total publications, followed by reviews (12.6%). Most documents (94.7%) were published in English, with an average document age of 8.55 years (Table 1). Each publication had an average of 4.01 coauthors, while the percentage of international collaboration was 10.18%. According to Lotka’s Law, a bibliometric principle suggesting that most authors contribute only once to a given field, we found that 91.4% of authors had only a single publication in this domain. This finding suggests a maturing yet still relatively fragmented field with many occasional contributors and limited core authorship continuity.
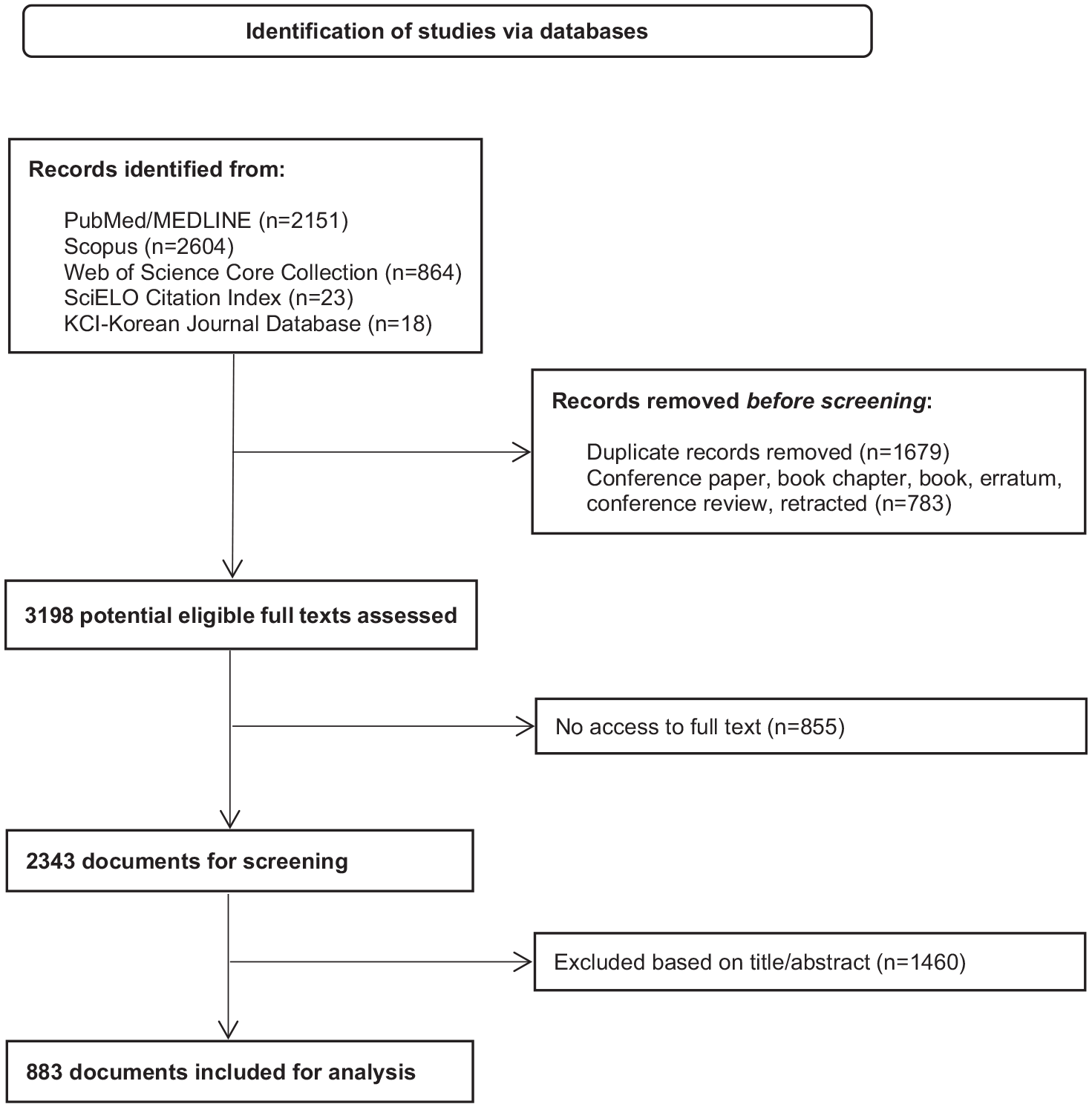
Documents selection flow diagram.

(A) Annual scientific growth of global research on Six Sigma applied to healthcare, and projection of future publications in the next 5 years, (B) frequency of publications over time, distributed according to the quartile of the journal, and projection of future publications in the next 10 years, and (C) distribution of publication frequency by country.
General characteristics of the included publications (N = 883).

Corresponding author’s country.
Category according to most recent World Bank update (2024).
Year-adjusted value of the journal metrics.
Geographical and Economic Distribution
High-income countries accounted for 70.8% of the publications, whereas low-income countries contributed only 0.7% (Table 1). By region, North America emerged as the leading producer (47.3%), followed by Europe and Central Asia (30%) and East Asia and the Pacific (8.7%; Figure 2C). Among the publications, 35.1% appeared in first-quartile journals, with an average h-index of 67 (±58.9). However, only 35% of the documents were published as open access.
When production was analyzed by quartile as a proxy for publication quality, the United States demonstrated the highest volume of Q1 publications (16.6%), followed by China (2.2%) and Italy (0.76%). Q1 publications also showed the highest representation of authors from high-income countries (25.3%). For Q2 publications, Europe and Central Asia, led by Italy and Turkey, increased their share. Open access was more prevalent in Q2 journals, with 15.2% of publications available. In lower quartiles (Q3-Q4), low- and lower-middle-income countries slightly increased their representation, although they remained a minority (Table 2).
Scientometrics characteristics of publications by journal quartile.

Corresponding author’s country.
Category according to most recent World Bank update (2024).
Thematic Evolution and Keyword Analysis
Figure 3 provides a detailed overview of thematic areas and research trends related to Six Sigma in healthcare. The most frequently used keywords included “quality management,” “continuous improvement,” “operational efficiency,” and “patient safety” (Figure 3A). Correspondence analysis revealed strong associations between key terms such as “laboratory processes,” “patient safety,” and “hospital management,” indicating a thematic concentration in hospital services and clinical laboratories (Figure 3B).

(A) Word cloud with the most frequently used keywords in research on Six Sigma applied to healthcare, (B) correspondence analysis of thematic relationships (shaded region indicates higher term density or thematic concentration), (C) heat map with the most frequently used thematic terms related to Six Sigma over time, and (D) temporal evolution of hot topics over time.
Thematic evolution analysis over time demonstrated an initial focus on “quality control” and “manufacturing processes,” which progressively shifted toward terms such as “information technology” and “data analysis.” This shift reflects the growing integration of technological tools in implementing Six Sigma (Figure 3C). Regarding hot topics, recent terms such as “health innovation” and “big data” emerged, signaling a transition to more modern, data-driven approaches (Figure 3D).
The co-occurrence analysis of terms identified various clusters with significant central nodes. Two primary clusters were observed. The first cluster, centered on “patient safety” and “major clinical studies,” with a frequency of 8 to 12, highlights a focus on care safety (Figure 4A). The second cluster, associated with “laboratory” and “health services,” reflects practical applications in hospital and laboratory settings (Figure 4B).

Cluster connection map between core terms and thematic areas in research on Six Sigma applied to healthcare: (A) cluster connection map (central terms: “patient safety” and “mayor clinical study”; frequency 8 to 12), (B) cluster connection map (central terms: “laboratory” and “health service”; frequency 6 to 12), and (C) international collaboration between countries.
Collaboration Networks
International collaboration analysis indicated that high-income countries dominate global partnerships, with the United States, the United Kingdom, and Canada serving as key players (Figure 4C). However, interactions between middle- and low-income countries were minimal, underscoring a significant gap in global collaboration.
Correlation Between Six Sigma Research and Global Health Metrics
The analysis of correlations among scientometrics variables, healthcare quality indicators, and global health metrics revealed that research and development expenditure (as a percentage of GDP) demonstrated a consistent positive correlation with publication frequency (r2 = .65; P < .01) and with articles published across all journal quartiles, showing the strongest correlation in Q4 journals (r2 = .75; P < .01). Additionally, current health expenditure as a percentage of GDP demonstrated a strong positive correlation with publication frequency, regardless of the journal quartile (P-value < .01 for all cases). Payments for the use of intellectual property exhibited moderate positive correlations with Q3 (r2 = .73) and Q4 (r2 = .72) articles. In contrast, weaker correlations were observed for Q1 (r2 = .30) and Q2 (r2 = .35) articles (P-value < .01 for all cases).
Interestingly, weaker correlations were found between indicators such as disability-adjusted life years (DALYs) or crude mortality rates by country. Unexpectedly, negative correlations were identified between publication frequency and journal quartiles with variables such as official development assistance by individual countries and income groups, out-of-pocket health expenditures, and the number of health researchers across WHO regions (Table 3).
Correlations between scientometrics variables and indicators of health care quality and global health metrics by countries. ǂ

Abbreviations: DALYs: disability adjusted life years; GDP: gross domestic product; ODA: official development assistance; WHO: World Health Organization.
Corresponding author’s country.
P-value < .05. **P-value < .01.
Discussion
The scientometrics analysis presented reveals valuable insights into the global landscape of Six Sigma research in healthcare. The consistent growth of publications since 1999, particularly in high-income countries, underscores the recognition of Six Sigma as a vital tool for improving healthcare quality. However, the geographical disparity in publication frequency is striking. High-income countries contributed 70.8% of the research, while low-income countries accounted for only 0.7%. This imbalance reflects systemic inequities in research capacity and access to resources, potentially perpetuated by economic constraints and limited infrastructure for health research in resource-limited settings. 28
The thematic analysis highlights a concentration of studies in hospital services and clinical laboratories, with keywords like “patient safety” and “quality management” dominating. This thematic focus aligns with the urgent need to enhance operational efficiency and safety in complex healthcare environments (eg, community health).28,29 The evolution of research themes from “quality control” and “manufacturing processes” to “big data” and “health innovation” illustrates a shift toward integrating advanced technologies into quality improvement efforts. Nevertheless, the limited representation of lower-income regions in these advancements indicates that such innovations may not be globally accessible or equally prioritized.
The correlation findings emphasize the critical role of economic factors in research productivity. The positive association between research and development expenditure and publication frequency, particularly in lower-quartile journals, suggests that robust funding environments enable greater research output. Conversely, negative correlations with out-of-pocket health expenditures and health researchers per million inhabitants in low-resource regions highlight systemic barriers to engaging in and benefiting from Six Sigma research. 30
These disparities have profound implications for global healthcare systems. The underrepresentation of low-income countries and the scarcity of collaboration across income groups limit the generalizability and applicability of Six Sigma strategies in diverse contexts. Addressing these gaps through targeted funding, capacity-building initiatives, and international partnerships is imperative for equitable improvements in healthcare quality.30,31 Such efforts could also foster the adoption of evidence-based practices tailored to the unique needs of underserved populations. 31
Previous systematic reviews have documented a growing interest in adopting Six Sigma within healthcare settings, focusing on hospital-wide implementations rather than specific departments or functions.30,31 This aligns with our findings, which indicate a thematic concentration on hospital services and clinical laboratories, emphasizing areas such as patient safety and quality management. However, our study provides a more granular examination of thematic evolution over time, highlighting a shift from traditional quality control and manufacturing processes to contemporary themes like big data and health innovation. This progression underscores the increasing integration of advanced technological tools in Six Sigma methodologies within healthcare—a nuance less explored in earlier reviews. 32
Some prior studies suggest Six Sigma has shown limited sustainability or scalability in public hospitals due to workforce resistance or contextual misalignment.30-32 However, our findings of growing global adoption may reflect increased training, institutional commitment, or external incentives (eg, accreditation demands), which warrant further investigation.30-32
Previous studies have explored factors influencing the academic and societal impact of Six Sigma publications in terms of research impact, noting that content relevance plays a more significant role than bibliometric characteristics.30-32 Our analysis complements this by demonstrating that economic factors, including research and development, are strong predictors of research output, particularly in lower-quartile journals. This suggests that while content is crucial, the capacity to produce and disseminate research is heavily influenced by economic resources.
Then, our study not only corroborates existing findings regarding the adoption and thematic focus of Six Sigma in healthcare but also introduces novel insights into the temporal evolution of research themes, the economic determinants of research output, and the global collaboration landscape. These contributions are pertinent for informing future research directions and policy decisions to foster equitable advancements in healthcare quality improvement.33,34
Our findings suggest that low research productivity in low-income countries correlates with limited investment in health R&D and infrastructure. Aligning investment priorities with outcome-driven frameworks—such as Six Sigma—could help resource-limited systems identify high-impact inefficiencies, design context-adapted protocols, and optimize cost-effectiveness, particularly in hospital logistics, infection control, and claims management.
The dominance of one-time contributors observed through Lotka’s Law analysis indicates that Six Sigma in healthcare may still be an emerging field, with limited consolidation of expert authorship and institutional leadership. This fragmented authorship pattern may hinder the continuity of research lines and long-term innovation strategies.
Future research should focus on inclusive international partnerships, investment in local research capacity—especially in low- and middle-income countries—and context-specific adaptations of Six Sigma tools. Areas such as community health, public hospitals, and outpatient services require models tailored to limited-resource environments. Emphasis should be placed on knowledge transfer, digital integration, and fostering regional research networks.
Healthcare institutions in low- and middle-income countries can prioritize context-sensitive Six Sigma interventions targeting specific areas like inventory management, patient triage, or infection control, supported by regional technical partnerships and simplified training modules. By reducing variability and error in processes like diagnostics or medication management, Six Sigma can significantly improve care outcomes for underserved populations, where system inefficiencies often result in disproportionate harm. Practical barriers to adoption—such as the cost of Six Sigma certification, limited institutional incentives, and resistance to change—must be addressed through subsidized training, integration with accreditation processes, and leadership-driven cultural change.
This study is subject to limitations. First, as a scientometrics analysis, it focuses on publication-based metrics and does not account for the quality or implementation outcomes of Six Sigma initiatives. Second, grey literature, including reports, theses, and unpublished quality improvement projects, was not included, which may omit relevant data from non-indexed local initiatives, especially in low- and middle-income countries. The analytical tools used, such as Bibliometrix and VosViewer, are limited by the structure of indexed metadata, potential citation biases, and uneven database coverage. Moreover, they may amplify visibility of highly cited articles regardless of methodological quality. While our correlation analysis provides an initial overview, multivariate modelling—adjusting for confounding variables such as population size, education level, or GDP per capita—would further refine these associations and is recommended for future studies. Citation-based metrics may be influenced by self-citation practices, regional journal visibility, and editorial policies that inflate impact factors without reflecting research quality.
Conclusions
This study provides the first comprehensive scientometrics analysis of Six Sigma research in healthcare. Key findings include a significant growth in publications over the past two decades, predominantly driven by high-income countries, and a thematic focus on patient safety and hospital-based applications. The evolution of research themes toward data-driven innovations highlights the dynamic nature of this field, although disparities in geographical and economic representation remain evident. Economic factors, such as research and development expenditure, emerged as strong predictors of research output, while barriers in low-resource settings continue to hinder contributions from lower-income countries. These results emphasize the requirement for strategies to bridge global disparities, including enhanced funding mechanisms, international collaboration, and capacity-building initiatives in low- and middle-income regions.
To encourage contributions from low-income countries, stakeholders should implement targeted engagement strategies such as micro-grant schemes, simplified ethics approval frameworks, and regional quality improvement hubs that promote practical Six Sigma training and publication mentorship.
Footnotes
Author Contributions
YGP, MHP, DAHP, DNR, KSN, AMRO, TBV, IDLM, and PD conceived and designed the review. YGP, MHP, DAHP, DNR, KSN, AMRO, TBV, IDLM, and PD carried out the draft of the manuscript. IDLM, and PD developed the search strings. The reviewers YGP, MHP, DAHP, and AMRO screened and selected the studies. YGP, MHP, DAHP, and IDLM extracted the data and evaluated the quality of the studies. DNR, KSN, AMRO, TBV, and IDLM carried out the analysis and interpretation. All authors rigorously reviewed, read, and approved the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All related data has been presented within the manuscript. The dataset supporting the conclusions of this article is available from the corresponding author upon request.