
Abstract
First responders (police, firefighters, and paramedics) are routinely exposed to potentially psychologically traumatic events (PPTE). While the prevalence of mental disorders is difficult to estimate, research has demonstrated that first responders report higher rates of mental health disorders than the general population. They also report significant barriers to accessing mental healthcare, including concerns about the confidentiality of mental health services and stigma by co-workers and organizational leadership. One way to address these barriers to seeking care is through the establishment of a first responder specific mental health clinic. The objective of this qualitative study was to assess how to best implement such a service for first responders in Ottawa, Canada. We conducted 14 in-depth semi-structured qualitative interviews with key interest holders from first responder services, unions/associations, and the Workplace Safety and Insurance Board (WSIB) which explored elements of service delivery and organizational barriers and facilitators to implementing the clinic. Interviews were analyzed and coded using thematic analysis by two independent coders. Four main themes were identified: implementation context (perceived need, workplace culture), design of the clinic (service delivery, confidentiality, cost, and communication about the clinic), the implementation process (barriers and facilitators to implementation), and the broader impact of the implementation of the clinic. Findings show that it is the right time to implement first responder specific clinical services as services begin to prioritize the mental health needs of their members. To increase uptake by first responders, confidentiality and cultural competency of care providers is paramount.
Keywords
Introduction
First responders (police, firefighters, and paramedics) work in unique environments where they are routinely exposed to potentially psychologically traumatic events (PPTE).1-3 While 50%-90% of the general population reports exposure to a PPTE in their lifetime,4,5 first responders report being repeatedly exposed to multiple types of events over the course of their career. 1 The repeated exposure to PPTE puts first responders at higher risk of developing mental illnesses, including post-traumatic stress disorder (PTSD), depression, alcohol and substance misuse,6-9 the development of suicidal thoughts or behaviors, 10 as well as difficulties with sleep. 11 However, first responders also have a strong sense of purpose, a sense of belonging to a team, and pride in having unique skills and training.
Mental Health Disorders Among First Responders
The prevalence of mental disorders in this population is difficult to assess as most studies use small, unrepresentative, self-selected samples. For example, a national survey in Canada was sent to an estimated 250,000 public safety personnel (PSP), which included first responders, of whom 5,813 replied. 6 In Canada, the lifetime prevalence of PTSD in the general population is 9.2%, while prevalence in first responders varies among police (8%-32%), paramedics (26%), and firefighters (17%). 12 An increased prevalence has also been recorded for other mental disorders, including depression (5.4%-11.7% compared to 26.4%) and past-year prevalence of alcohol use disorder (3.2% compared to 5.9%).6,13,14 Suicidal thoughts and behaviors also occur at increased rates compared to the general population with 10.1% of PSP reporting suicidal ideation, 4.1% reporting a plan, and 0.3% reporting a suicide attempt in the past year. 10
Barriers and Facilitators to Accessing Mental Healthcare
Given these rates, many first responder services have identified the mental health of their members as a strategic priority. However, many barriers still exist for first responders accessing mental health care. In a 2017 systematic review and meta-analysis, the most commonly reported factors influencing non-service use included concerns about confidentiality, worries that seeking mental health services would negatively impact one’s career, fear of judgment by co-workers and organizational leadership. 15 Ricciardelli et al16,17 also found that system-level processes, which are underpinned by stigma towards mental health, may be influencing help-seeking among Canadian first responders. Members may be concerned with how they will be viewed by their colleagues, which in turn, may impact their awareness of their own mental health needs. 17 Interestingly, stigma was not directed towards mental health itself, as it was generally accepted that stress encountered as a function of first responder occupations can lead to PTSD, but instead, towards the legitimacy of the perceived cause of injury. 17 Some stressors are seen as legitimate causes of mental distress while other events are seen as spurious and result in individuals being seen as “abusing the system” or “taking advantage” of accommodations. 17 Other studies have found that pervasive beliefs that those with mental illness are “weak,” “inferior,” or possibly “dangerous” in their role, continue to act as barriers to treatment. 18 There is also the cultural aspect of duty being placed before self-care.19,20 Lower tolerance for extended absences related to mental illness was also highlighted as a potential factor discouraging help seeking. 18 First responders have also reported structural barriers to seeking mental health support, including difficulty in scheduling appointments, not knowing where to get help, difficulty in getting the time off work needed to attend appointments, a fear of traumatizing clinicians, lack of adequate transportation, and a lack of support from their organization.15,21,22
While a substantial portion of the literature has focused on barriers to seeking care among first responder populations, important facilitators of treatment have also been identified. For instance, a scoping review by Smith et al 23 found that organizational interventions focusing on broad culture change, such as resiliency building, or mental health awareness programs have been shown to support overcoming barriers to help seeking. Jones et al 19 found help-seeking among firefighters and emergency medical technicians/paramedics was facilitated by members knowing that they were not alone in their mental health struggles; buy-in from peers, administrators, and their union; positive experiences with therapists who often had experience working with first responders or military personnel; and having mental health problems become so severe that other people began noticing.
The Current Study
One possible solution to the barriers to care experienced by first responders is to develop an Operational Stress Injury (OSI) clinic for this population based on the model currently used by the Canadian military. 24 In this care delivery model, a multi-disciplinary team is assembled that includes psychiatrists, psychologists, social workers, mental health nurses, and other clinicians with specialized training in the needs of the population they serve. This team provides ongoing mental health support based on current best practices with links to services in the community, such as family physicians and substance abuse treatment as needed. 24
To determine the best way to develop a first responder specific OSI clinic, we conducted qualitative interviews with key interest holders from the first responder community in Ottawa, Canada, including individuals in management position at first responder services, associations, unions, and workplace safety organizations. These interviews aimed to describe the mental healthcare needs of first responders, identify key components in the delivery of mental healthcare to this population, and assess potential barriers and facilitators to accessing care to inform best practices for the development and implementation of a first-responder specific OSI clinic.
Method
Study Design
This qualitative study describes a series of interviews with key interest holders from the first responder community in Ottawa, Canada. Individual qualitative interviews were used because they allow participants to articulate their experiences, thoughts, beliefs and feelings about how to best address the mental health needs of first responders in their community. 25 Specifically, this study sought to answer the question “What is the best way to implement an Operational Stress Injury Clinic among first responders?”
Recruitment
Participants were members of the first responder community, specifically those in a management position with the Ottawa Police Service, Ottawa Fire Services, the Ottawa Paramedic Service, the Workplace Safety and Insurance Board (WSIB) and the services’ respective Unions and/or Professional Associations. Interviews were also completed with first responders with a history of mental health disorders, frontline staff, and members of the respective peer support groups, the results of which are reported in another article. 22 Study eligibility criteria are outlined in Table 1.
Study eligibility criteria.
We aimed to recruit a total of 10 participants, which is aligned with smaller sample sizes used in exploratory qualitative research studies focused on sensitive topics. 26 Participants were recruited using a combination of purposive sampling and snowball sampling techniques that ensure the sample contained an abundance of “information power,” a concept used to guide sample size for qualitative research using criteria like the aim of the study, the specificity of the sample, and the availability of established theory to ensure information power. 27 First, individuals known to the research team through other research collaborations were approached to refer potential participants to the study. Second, organization-wide emails about the study and recruitment posters were distributed through the research team’s professional networks, including via service Peer Support Groups and first-responder specific committees in Ottawa. Finally, we also asked each participant who was interviewed whether there was anyone else they felt had an important perspective to share on the implementation of the clinic. Interviews continued until data saturation was reached, which was defined as the point at which additional interviews would not yield any new ideas or details. 28
Participants
A total of 14 participants completed qualitative interviews between July 2019 and October 2019. Interviews ranged from 48 minutes to 2 hours and 56 minutes, with an average of 1 hour and 46 minutes per interview. The ages of participants varied from 38 to 61 years of age (M = 46.1, SD = 9.2) and 85.7% (12/14) of participants were male. Participants were members of key interest holder groups including: the police (1), paramedic (5), and fire (4) services as well as first responder unions/associations (3) and WSIB (1). To protect participant confidentiality, participants will only be identified using their participant ID number.
Data Collection
Semi-structured interviews were completed by two research staff members using a comprehensive interview guide (Supplemental Material 1) focusing on elements of service delivery (e.g., clinic hours, available services, and communication) as well as organizational barriers and facilitators to implementing the clinic. Participants were able to complete the interview in the official language of their choice (English or French). We used a consensus qualitative research (CQR) approach 29 which involves: (1) open-ended semi-structured interviews to allow for the consistent collection of in-depth perspectives and experiences from participants; (2) several judges or coders [CA, NEE, SEM] throughout the analysis process to encourage multiple perspectives; (3) consensus as the driving force in determining the meaning of the data collected; (4) at least one auditor [SH] to check the work of the coders and minimize the impact of groupthink; and, (5) domains, constructs, or core ideas in the data analysis. Interviews were conducted at a neutral location, chosen by the participant, away from areas first responders typically associate with their profession (e.g., hospital emergency departments, clinics, etc.) at a time of their choosing. All interviews were transcribed by a professional transcription service.
Data Analysis
To understand participant perspectives on how to best implement a first responder OSI clinic, we employed an applied interpretivist lens, with a recognition that to understand the social world, we must begin with human experience and/or perspectives. 30 Similarly, in taking an applied approach, we highlight that objective and subjective truth are not mutually exclusive and both have a role to play in knowledge development. Specifically, we acknowledge that our disciplinary commitments influence what we observe in the field. 31
Thematic analysis was used to identify, analyze, and report themes observed in the qualitative data. The analysis was guided by the six steps of thematic analysis outlined by Braun and Clarke. 32 First, during the familiarization phase, all coders [SEM, NEE, CA] immersed themselves in the interview data by reading each transcript at least twice. Second, the coders completed a round of pilot coding using an open coding technique to identify data extracts that might potentially form the basis of patterns or themes. At the end of this phase, the coders developed a preliminary codebook to guide data analysis; however, remained open to the possibility that new themes might be discovered in subsequent phases of the analysis. Third, independent focused coding of each transcript was completed, with each transcript coded by two coders. Following the coding, conflicts were discussed and reconciled. In cases where coders could not agree, the auditor [SH] was consulted. Fourth, once coding was complete, the three coders met to identify overarching themes and sub-themes using a thematic map. During this phase, coders also ensured that themes were both internally homogeneous (i.e., each theme was coherent) and externally heterogeneous (i.e., distinctions between themes were clear and identifiable). Fifth, each theme to be included in the final analysis was then named and defined. Lastly, the final analysis was written up based on the prompts identified by Braun and Clarke, 32 including: What does this theme mean? What are its implications? What does the overall story of the different themes reveal about this topic? All data analysis was completed using NVivo 12 or NVivo 12 Pro.
Ethics
Research ethics approval was obtained from the Ottawa Health Sciences Network Research Ethics Board (OHSN-REB ID: 20180903-01H). Written informed consent was obtained from all participants prior to study procedures and all participants consented to the audio-recording of their interview. During the informed consent visits, a study staff member explained the details of the study, including aims, participants rights, potential risks to participation, and the voluntary nature of the study.
Findings/Results
An overview of the themes discovered through the qualitative interviews in this study is outlined in Figure 1 and is further described in Supplemental Material 2. Unsurprisingly, the implementation of a novel clinical service, like a first responder OSI clinic, is complex, requiring close attention to many interrelated concepts and factors. Four main themes were identified as relevant to the implementation of a first responder OSI clinic: the implementation context (perceived need, workplace culture), design of the clinic (service delivery, confidentiality, cost, and communication about the clinic), the implementation process (barriers and facilitators to implementation), and the broader impact of the implementation of the clinic.
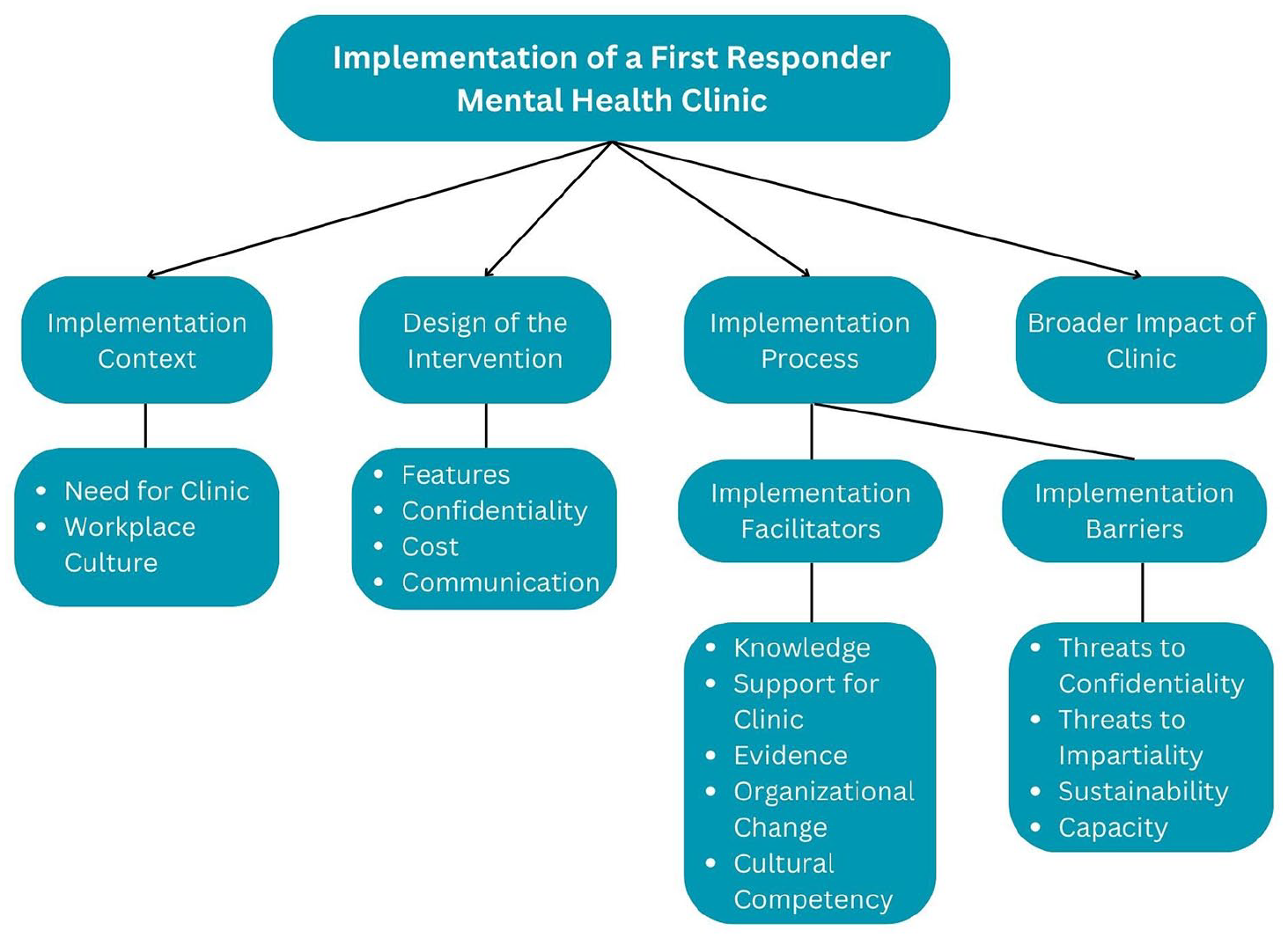
Thematic map.
Implementation Context
Need for Clinic
All participants interviewed saw a need for a first responder OSI clinic. Many highlighted that existing services, such as the Employee Assistance Plan (EAP) and Peer Support Groups, while helpful, are not enough to address the unique and increasing demands for mental health support for first responders: “We need help. Some of our members need help, and we need to send them to people who actually understand our industry” (P020).
Participants expressed that we are currently at an important juncture for first responder mental health, with the introduction of presumptive legislation in many jurisdictions in Canada for a diagnosis of PTSD, whereby first responders no longer have to “prove” their PTSD is a result of their profession, and that the time is right for implementation of a clinical service: “The organization, the culture there, I think it’s ripe for it, and those older management, those people in authority that aren’t onboard, we’ll drown them out” (P019).
Some participants also explained as the mental health of service members has become a priority among first responder organizations, there has been an increased need for care and existing universal healthcare resources have been unable to meet this increased demand. A first responder OSI clinic could be instrumental in filling this gap in care: [I]t’s nice that people recognize that they need help and they’re asking for help, but they ask, and the resources aren’t there. My understanding is that there’s a shortage of mental health professionals in the province and so from that perspective, any additional resources that we can put to this issue is positive. (P016)
Participants also voiced that a specialized clinic has the potential to address some of the challenges with accessing care. Participant 018, for example, spoke of the perceived risk of accessing emergency services during a mental health crisis: The cops responding to a cop, depending on who the cops are, they might get a very good response and supportive and all that, but for the individual making the call, that’s going to be tough. If there’s some sort of a safer way for them to get somebody that’s truly going to be supportive, rather than rolling the dice and calling 911, and you get whoever you get. . . (P018).
This was echoed by Participant 038 who spoke of the challenges of seeking mental healthcare in the same setting as the general population: . . . [H]aving a place where only first responders go, I really think that it would make it easier for them to do it, right? Because. . . a police officer doesn’t want to walk into a doctor’s office and the person they arrested last week is sitting there. That would not be a good thing, right? (P038).
Finally, nearly all participants mentioned the inconsistencies in private insurance coverage for first responders in Ottawa. This also speaks to obvious tensions between the services, who each negotiate their collective agreements separately, with the police service securing unlimited mental health benefits for their members whereas the paramedic and fire services have a very limited budget. While this issue is beyond the control of the clinic itself, it speaks not only to the high mental health needs of this population, but also the difficulties they experience in trying to seek services in the community.
Workplace Culture
Interviewees highlighted that workplace culture within each of the services is a key consideration when designing and implementing a first responder OSI clinic as this has impacts at both the individual and organization level. At the individual level, a workplace culture that is not supportive or accepting of the mental health impacts of a first responder career may inhibit service members from seeking care. At the organizational level, it can hinder the success of top-down mental health initiatives. Many participants spoke to the positive changes that prioritizing mental health within their service has made to the culture: . . .[I]t’s a pillar of the administration, whenever we do something or whenever we consider something or whenever we make a decision, we try and tie it back to one of these pillars. And you can do that with lots of things for mental health. Every good thing you do is part of mental health support. (P016)
A similar perspective was shared by Participant 020: I consider the wellness of our employees, not only their work wellness, but their family wellness, is extremely important, and mental health is one of those major pillars within in that, whether it’s physical health, mental health, and preventative measures. We have preventative measures for cancers and heart, well, we need preventative measures for mental health as well, and how we can actually provide that (P020).
Participants who spoke to these positive changes in workplace culture also often acknowledged that further culture change is still needed: I think the change is coming, and I think that - I think we’re getting better at it, but I think internally, we still struggle, and which affects our external ability to serve our community. . . I think there’s definite change, because I think people are realizing that . . .the way we treat each other is huge, right? (P037)
This change is badly needed, especially as it concerns members of equity-seeking groups: When I say it’s getting better, the stigma. . . as a white male, yes, it is. As a female. . . no, and that’s why we have very, very few minorities. . . For them to access care, they feel that it will confirm these pre-assumptions that people have anyways (P023).
Other participants, however, voiced that first responder culture continues to be detrimental to the mental health of service members. When asked what this looks like in their respective workplace, interviewees spoke to generational issues, dark humor, and gossip as key mechanisms: Firefighters have a long history of horseplay, and being funny, and changing our culture to get people to understand that not everything is funny. It depends on how the receiver actually takes it. . . I’ll give you an example of that. . . Water pailing, right? That’s when somebody’s standing by a truck and somebody’s on a truck with a pail of water and dumps it on them. That’s viewed as a joke for a lot of people, because it’s funny, and they get wet, right? Well, some people who actually get pailed view that as a strength of their character, and it’s how they react, and sometimes they get very, very angry, and then they’re not happy with themselves, because they got angry over something that should be funny. (P020)
Others still explained that while service leadership claims to prioritize mental health of its members, they felt this was mostly “lip service” to protect the organization’s reputation: I’m going to be quite honest with you, the employer has—so since mental health and wellness has become a topic in the last five years, [the service] has pretended it knows what it’s doing—I’m not trying to be mean—they don’t know what they’re doing. No, it’s been a lot of talk, little action. (P019)
This was echoed by Participant 023: I think we all have a part to play in improving [stigma related to accessing mental healthcare]. I don’t think we’ve done a great job as [an organization], I’ll say that. I think management pays lip service, and I think people see that, that they’re a little bit transparent. They’ll pay lip service, especially to the public. On certain days, mental health day. . . we don’t forget. We take that seriously, but in practice, they don’t (P023)
Design of the Clinic
Discussion of the potential features of the first responder OSI clinic was a central component of each interview. These included components of service delivery, measures to ensure confidentiality, associated costs, and communication about the clinic.
Service Delivery
Interviewees identified service delivery components that they viewed as essential to the clinic’s successful implementation, including the integration of specialists to deliver care to both first responders and their families; the importance of low barriers to entry into the clinic; the role of local peer support groups in the clinic’s functioning; the role of the clinic in critical incident debriefing; and logistical considerations, such as the clinic’s location, hours, and whether uniforms should be permitted on site. Participants spoke of a need to centralize the delivery of mental health services, providing “one stop shopping” (P032) for members. Central to this is the development of a multi-disciplinary team to provide a suite of mental health services, as described by Participant 017: It’s best to have a multitude of types of caregivers involved. I go to a family health clinic - I have for decades and decades, and the best part is they’ve got psychologists. They’ve got doctors. They’ve got nurse practitioners. They have tie into all kinds of different therapists and work with the program, and it’s much easier to manage if you need different kinds of supports, because it’s all in one house (P017).
As intimated by this quote, many participants spoke of the need for the clinic to provide multiple kinds of services, both in-person and virtually. However, interviewees repeatedly spoke to the need for first responder crisis services: . . .[Y]ou could implement a 1-800 line or something of that nature where they could actually contact and get access to 24/7 type service, at least the triage type service where they’re being assessed when they need help. Immediate - if it was possible to have them somehow attached to our peer support team where you could have some crisis intervention, emergency crisis intervention or assistance. (P020)
Some participants also envisioned the first responder OSI clinic being involved in debriefing after critical incidents, such as city-wide emergencies involving mass casualties as well as service member deaths, especially suicides, rather than relying solely on local peer support groups. Interviewees disagreed about the integration of local peer support groups in the first responder OSI clinic, with some showing strong support for peer supporters as “the best ambassadors when somebody’s hurting” (P024). Others, however, spoke to the complexities of embedding peer support groups in this clinic. Participant 023, for example, explained that while it would be beneficial for peer support workers to be affiliated with the clinic to obtain proper supervision and training, that including them in care delivery would be problematic: I wouldn’t recommend it. These are healthcare issues. . . In my opinion, they’re healthcare issues. . . I think the role of peer support - the intention is great, but it doesn’t need to be over expanded. Peer support is to assist in crisis, post-crisis, and some of these matters may be related to personal issues. Again, I think it’s overly exposed in our membership that aren’t properly trained to manage those things. They’re really supposed to be a point of contact or refer people to specialized services (P023).
In terms of the logistics involved in accessing the clinic, participants routinely spoke of the need for low barrier entry. Participant 017 suggested that one way to reduce barriers to accessing the clinic would be to accept referrals from sources including family doctors and service EAPs. Others highlighted the need for the clinic to be connected with in-patient treatment programs as a means of providing appropriate aftercare. Numerous participants also spoke of the need to minimize waitlists as much as possible: Sometimes you get that sweet spot where the person just says I want to get help. Okay, let’s wait two weeks. Let’s wait a week. Do we still have the momentum in a week? Sometimes yes, sometimes no. (P009)
There was also significant discussion of where exactly the clinic should be located. Interviewees agreed that the clinic be in the community, separate from any mental health facilities or hospitals which participants often viewed as an extension of their workplace. However, there was little agreement with where the first responder OSI clinic should be located.
Confidentiality
Participants repeatedly spoke of needing to be reassured that all services provided in the context of the clinic would be kept confidential from their employer. As Participant 020 explains: The employees will need to know that the access to their information is not possible through their employer, or else there will be no buy in. There will be the belief that this is the employer’s way of getting information they can’t get through other legal means, and, therefore, absolute anonymity is important (P020).
This participant also went on to explain that because the clinic is “attach[ed] to the current medical system in the province” (P020), it should help mitigate some of the hesitancy related to privacy as all clinic staff would be bound by provincial legislation related to the disclosure of health information. Other participants also highlighted the need to prevent the inadvertent identification of clinic patients by staggering appointments to ensure that patients do not recognize each other in the waiting room.
Communication
Interviewees provided insights on what they viewed as the best ways to communicate with first responders about the availability of the clinic. Chief among these recommendations was the development of a media and marketing toolkit that includes multiple different communication products, such as a clinic website, information pamphlets, posters, social media, and videos. Multiple participants also recommended presentations about the clinic at each of the services through, for example, their daily briefings or continuing education sessions. However, they also spoke to the need to balance this with remaining distinct from the employer. For instance, Participant 024 suggested: Maybe an initial roll out of here’s the clinic, this is what we do and offer, but then back right out. Don’t be seen as part of the WSIB [Workplace Safety and Insurance Board] process. . . If the employer is sending them there, you don’t want to be the one the employer is sending them to (P024).
Several interviewees also spoke about the use of testimonials as a way of increasing the credibility of the clinic. Participant 009, for instance, explained that having first responders tell their own stories would be much more impactful than any data or statistics about mental health issues among this population. Speaking about facilitating a previous mental health session: . . . we had two [members] who shared their stories. . . told everybody that he made a suicide attempt. They were popular, like they were well liked by everybody. . . people were shocked because some didn’t know. Most didn’t know. They were able to keep a straight face at work, so these are way more powerful than statistics. And if again, people give their testimony on how much this clinic helps, it’s going to be way better than any stats (P009).
Participant 037 also explained that for testimonials to be impactful, they should be delivered by frontline first responders and not those who are in management positions who are “already drinking the Kool-Aid” (P037).
Implementation Process
Implementation Facilitators
Interviewees identified five key facilitators to the implementation of a first responder OSI clinic, including: knowledge about the clinic; buy in from leadership; evidence of the effectiveness of the clinic; organizational change; and the cultural competency of providers.
First, interviewees explained that the more knowledge they had about the clinic, the better positioned they would be to assist in implementing it. Much of the information they identified as essential was logistical in nature, including who the clinic serves (who “counts” as a first responder), hours of operation, catchment area, services, capacity, wait times, the clinic’s mandate, who the clinic is affiliated with (e.g., the City of Ottawa, The Ottawa Hospital, the provincial WSIB, or a third-party), and how members can access the clinic.
Second, participants were asked what indicators or evidence they would need to know that the clinic was successful. Interviewees explained that improvements in return-to-work rates among service members over the long-term would be essential to obtaining support or buy-in for the clinic. Others spoke of the role of positive recommendations from other service members: That’s a difficult decision we find ourselves in, and how do we recommend some place that has worked for A, B, and C, but not X, Y, and Z? What evidence I would need. You know what? I’d just need one good experience from somebody, and hearing that, and getting that feedback. . .to let people know, but that is the difficulty that we have is how do we properly recommend a place. (P023).
Third would be organizational level changes to internal priorities, policies, and procedures. While participants highlighted that member mental health has been a priority for their organization, others have explained that this has not necessarily resulted in the creation of specific mental health initiatives. For example, Participant 016 explains: I don’t think that there’s anything specific. . . We have a communications pathway for mental health issues. There’s a number of them. It’s not necessarily completely sufficient, but they’re there, and the resources and the supports that are in the service now, people are aware of them. They are supported by everyone in the organization (P016).
While this participant has highlighted that many changes have been made at the organizational level, the discussion with most participants centered on the changes still left to be made to facilitate member access to the clinic. For instance, others highlighted the need for more training at the organizational level so that disclosures are sought in a meaningful way and so that members feel supported: I think it’s so systemic, right? I remember sitting on the [highway] with a body in the back of the truck, and our sup. walked over and said, “You guys okay?” My partner said, “Yep, we’re good,” and rolled up the window. It was like, I was, but what if I wasn’t. . .Even the sup., he was - he wasn’t doing it because he really wanted to know. It was kind of process. I better ask them, because they have a dead body, right? (P018)
Other participants spoke of a need for internal procedures about how to provide support when a member has a rough call and needs immediate assistance; accessing the clinic on shift; to ensure that when a member is off on leave that they receive appropriate follow-up from the organization; and reassignment procedures.
Finally, almost all participants spoke to the importance of having service providers who were trained in first responder culture. These participants spoke of the frustration they experience when having to explain basic components of their job to their care providers. These feelings were amplified when multiple carers were involved, where participants felt they would have to explain these things over and over. Participant 020, for example, highlighted how a lack of cultural competency acted as a significant barrier to accessing their organization’s EAP, where the number of free sessions they can access is limited: . . .our members tend to spend the first six sessions just explaining the work that we do. The therapists often haven’t dealt with the first responder community, and, therefore, it seems like you’re wasting all of your benefits on just explaining - before you get to the crux of the matter (P020).
This was echoed by Participant 023 who explains that they spend a lot of time educating care providers on the language of first responder professions: I’ve spent a lot of time explaining what some of the words and the jargon means, and how we function day-to-day, and that type of thing. Those are the only things that I can recommend is educating people on what it is we do, and the culture that work in (P023).
Implementation Barriers
Interviews identified numerous potential barriers to implementation of a first responder OSI clinic, including threats to confidentiality, concerns about impartiality, sustainability, capacity, and questions about provider exclusivity. First, numerous participants voiced concerns over the confidentiality of care provided at the clinic. For example, Participant 022 highlighted that some members might be concerned that mental health issues discussed in the context of the clinic would be shared with their employer: . . .that would be one of the processes that would have to have to be established to say how does someone who doesn’t want to be identified, access this facility without management ever knowing? It’s kind of that way of thinking, and unless they have that surety, they’re going to be reluctant to use it (P022).
Other participants clarified that, in their observations, concerns about confidentiality were less related to clinic staff or the employer, but more about wanting to remain distinct from the general public.
Confidentiality was especially important to police officers, who may feel hesitant to seek mental health treatment if it might threaten their identity. For example, they may have concerns that if they are deemed mentally unwell, their use of force could be taken away. Participant 037, for instance, highlighted the extent to which a police officer’s identity is tied to their badge and gun: They’re going to take away my gun. That’s another huge barrier for police. If I come forward and say, “You know, I just want to smash my car into that wall’ . . .‘Well, you have your gun, so we’re going to take it away.” Do you know what I mean?. . . if somebody identifies so strongly as a police officer, that’s the only thing that’s keeping them going, because we all know that work is probably the last thing that people lose. Then, I’m going to suffer in silence (P037).
Second, many participants also spoke of the need for the first responder OSI clinic to remain distinct from their employer, with many stating that endorsement from service management would be detrimental to the success of the clinic: And I think work should also keep an arm’s length from the clinic to avoid the fear that the chief will get an audio and video transcript of any conversation that happens in this building, because the number of times the employer tried to do the right thing—like one day we had free chiropractor assessments. Nobody went, because they were afraid that the employer would get the result: this guy has a bad back, like it will harm their career. So, I think that’s why the organization needs to keep an arm’s length from the clinic so if, even if it would never happen, there’s ethics, there’s colleges, there’s like so many things that would make it impossible for this to happen. People still are paranoid about this (P009)
This was echoed by Participant 023, who explained: If there’s a perception that. . . management has a close relationship with a clinic, that might be a perceived barrier as far as members thinking maybe there’s issues with confidentiality. There’s issues with the clinic being objective in nature or biased for whatever reason. . . It’s very - I know it’s cynical, but a lot of our members that have had difficulty accessing services are cynical, and especially those that have had resistance and difficulty with management (P023).
First responder services, as employers, were often perceived as self-interested, only looking out for the success or reputation of the organization, rather than the overall wellness of their members: I think impartiality is important, because . . . there sometimes can be a lot of suspicion that either management or WSIB or the employer, per se the city, is only looking out for themselves, and not really the employee, and they just want to write them off as quickly as possible. (P017)
Third, participants voiced concerns about the funding associated with the clinic. At the time of the interviews, the first responder OSI care delivery model was funded by a research grant. Participants, consequently, expressed concerns about the sustainability of services. For example, as Participant 022 describes: “I don’t want to put all my eggs in one basket, if it’s a temporary or unfunded thing” (P022).
Second, participants spoke to issues of capacity considering how many first responders in their organization currently need mental health care. Participant 017 explains: As with anything, when it’s new, there could be a whole lot of people - we know we have a fair number of people now with various forms of operational exposure and injury, and how many more out there that you don’t know about, and will the clinic have the resources to - is there a plan for the clinic to have resources to scale it up if the initial demand is greater than expected? (P017).
This was echoed by Participant 009 who spoke to the tension that exists between wanting the clinic to be successful and what that might mean in terms of access to the clinic: Okay, at one point you’ll have to say no. Yes, at one point—I don’t want to say I hope you’re going to have to say no—but I hope you can be the victim of your success. And eventually if you are, you’re going to have to turn people away, or send somebody somewhere else (P009).
Finally, Participant 017 expressed concerns about the OSI clinic becoming the exclusive provider of mental health services for first responders in the city and how this might also impact capacity: You need many pathways to care, because not all paths - one pathway is not going to suit everybody. . . I wouldn’t want the OSI clinic to just become that’s the only way people can get into the system, because they probably can’t deal with the volume (P017).
Cost
While the services available through the first responder OSI clinic would be covered by Ontario Health Insurance Plan (OHIP), interviewees routinely brought up concerns about costs. First, there were concerns about members who do not fall within OHIP’s scope: “. . . it’s about 20 per cent, maybe 15, 20 per cent of our staff live in Quebec, if I remember correctly. . . what do you do with people who live in Quebec?” (P009)
This is an important concern as patients from out of province will typically have to pay for services up front and seek reimbursement from their provincial healthcare plan. This could place undue financial burden on service members and prevent them from accessing the clinic.
Broader Impact of the Clinic
Participants spoke positively about the impact that a specialized OSI care delivery model could have on first responder mental health and wellness in the province as well as nationally. Specifically, participants voiced direct benefits or impacts for first responder services and leadership as well as for society. First, some interviewees highlighted that access to the first responder OSI clinic could offer them a competitive advantage compared to other services in the region: “I think if we’re trying to portray the service as an employer of choice, it definitely offers a competitive advantage that way, because we’re offering - we’re tied into more supports for people” (P017). Other participants, however, resisted this language: I don’t want to see it as competitive. We’re talking about people’s lives, so I don’t want to go into competition. It’s something to brag about. . . I don’t want to brag that like our employees are taken care of, yours are not. Because first responders, I’ve been to places around the world with their medics, with their first responders and we’re all the same world. We’ve got the same struggles, the same problems. It’s all the same around the world. I don’t want to brag that we are better than you are because if you are suffering, it gets me as much as my colleagues, because we’re all the same. (P009)
Second, participants spoke of the clinic, and the research embedded within it, as a powerful tool for service leadership: What feedback - I think it could be an extremely important reflective tool for the management and organization to be able to have that feedback on all the aspects of what leads to operational stress in the workplace, whether it’s burnout, whether it’s critical incident stress, whether it’s moral injury. How are we contributing to that? How can we prevent it? Are there things we’re putting in place for a bureaucratic reason or policy reason, actually subverting the employee resilience and creating the conditions where other kinds of injuries are more prevalent. (P017)
Finally, one participant explained that investment in the first responder OSI clinic could result in substantial return on investment: Every dollar you invest in proactive treatment saves three dollars on society. You save three dollars in the hospital system, three dollars in billings and medical systems or benefits. . . That to me should be where the real buy in should be is that proactive treatment of first responders saves - you save litigation expenses. You save liabilities. You save countless hours of investigations from somebody who’s suffering from being untreated acting inappropriately or just not producing or functioning, right? It has a tremendous impact on society. (P024)
Discussion
This study explored the perspectives of senior leaders in first responder organizations on how to best design and implement a first responder OSI clinic to meet the needs of their members. They reported four broad focus areas to consider: implementation context, design of the clinic, implementation process, and the wider impact of the clinic.
Respondents indicated a clear need for a first responder mental health clinic. Many first responder services have prioritized the mental health of their members as a strategic priority. The study findings were mixed in terms of the impact of this shift towards prioritizing mental wellness. Consistent with previous work, most participants acknowledged the negative impact that organizational stigma has on both members’ mental health6-11 and their willingness to access mental healthcare.15-18,22 While some interviewees explained that they have seen shifts in workplace culture as services have begun to center the mental wellness of their members, others highlighted that the existence of a first responder OSI clinic could also help to further address the issue of stigma. They explained that the clinic plays a role in normalizing reaching out for help and addressing the feelings of shame or embarrassment often described by first responders seeking mental healthcare.16-18,22
A large body of scholarship has highlighted that concerns about confidentiality act as one of the main barriers to seeking mental healthcare among first responders.8,19,22 For instance, in their systematic review and meta-analysis on barriers to care and mental health stigma among first responders, Haugen et al 15 found fear of service not being confidential to be one of the chief stigma items endorsed in the studies they identified. This has also been found in more recent studies on first responder mental health. For instance, Testa et al 22 noted the importance of transparent confidentiality processes to member uptake of a first responder mental health clinic. While the current study also found that confidentiality was a chief concern of first responder leaders, participants framed this issue not only as keeping member personal health information separate from their employment, but also as a means of maintaining physical and symbolic separation from the public. A 2020 qualitative study exploring Arkansas, USA first responder perceptions about mental health problems and help-seeking found similar results, highlighting that fear of confidentiality breaches was linked to concerns about showing weaknesses. 19 These participants reported that strength is a central component of first responder culture, and anything less is considered a safety risk. Our study found that this was particularly true for police officers. Participants explained that police officers may be especially difficult to engage in mental health treatment, even at a dedicated clinic, given ongoing fears that doing so may threaten their professional identity. While Workman-Stark acknowledges that, among some police officers, the authority to use force and physical toughness are central to their social identity, further research is needed on the relationship between occupying this identity category and seeking mental health help. 20 Confidentiality in occupational health settings is not just a first responder problem. It is broadly recognized as a difficult ethical and legal issue where the rights of the individual need to be balanced against the safety of the wider workplace and the public. 33 The findings of our study suggest the following avenues of addressing these concerns about confidentiality and, by extension, increasing trust: provision of care in a location that is distinct from both the employer and the public; transparency in terms of when confidentiality can and cannot be guaranteed; and discussion of the provider’s responsibility to provide safe and confidential care as well as providing an overview of which regulatory bodies or legislations are in place to ensure that providers protect patients’ privacy.
Cultural competency of care providers was important in the current study. Nearly all participants spoke of the need for a clinical service that employs providers who are trained in the realities of first responder culture. This is consistent with our interviews with frontline staff who often relayed fears of traumatizing their practitioners who were not familiar with the first responder role or culture. 22 These findings also echo a recent survey study exploring the return-to-work experiences of 145 PSP (128 of which were first responders) who had an approved WSIB claim for a psychological injury, noting the ability of healthcare providers to understand first responder work demands and culture as very important to respondents. 34 While this is an emerging area of research, the emphasis on providers who are trained in first responder culture raises the question as to whether the mental health needs of first responders are best served by a brick-and-mortar clinic staffed by a small number of providers, or whether efforts are better spent training a network of culturally competent providers that can be accessed by first responders nationally.
There were also different views about the scope of any clinic. Some respondents saw it as a routine “outpatient” clinic whereas others saw it as providing 24/7 crisis services, debriefing following critical incidents and a training resource for members. In late 2023, Canada implemented a national suicide hotline and work is ongoing to make these services more accessible and meaningful to PSP.
Strengths and Limitations
This study makes important contributions to the understanding of the mental health needs of first responders in Canada. Specifically, it highlights the importance of care providers trained in the dynamics of first responder occupations and the need for crisis services for this population. It also adds nuance to ongoing conversations on confidentiality as a barrier to mental health help-seeking among first responders.
This study has several limitations. First, interviews were conducted before the COVID-19 pandemic and, as such, it is possible that attitudes towards mental health and help-seeking changed in the intervening years. Second, this study did not systematically collect health equity indicators (e.g., ethnicity, race, sexual orientation) and, as such, it is not possible to speak to the experiences of potentially marginalized service members. Third, the perspectives represented are limited in that they do not include retired members or those on long-term disability leave which may have excluded leaders with lived experience of mental health disorders. Finally, it is possible that participant involvement in service-level mental health initiatives may have resulted in social desirability bias.
Conclusions
This study assessed the perspectives of senior leaders in first responder organizations on how to best implement a first responder specific mental health clinic. The issue of first responder mental health has been a high priority over the last 10 years. Specialized mental health services for this population have been highlighted as one potential avenue to address the high need of this population. 35 While findings from the current study speak to the needs for culturally competent, specialized care for this population, we urge practitioners and other decision-makers to consider whether the services are best delivered through a brick-and-mortar clinic. Given differences in first responder sectors and geographic challenges (especially for rural or remote services), a network of providers who are knowledgeable of first responder culture and aware of their unique mental health needs and preferences may be a better approach to providing care for this population. To facilitate this, more research is needed on what cultural competency means to first responders, how to best manage confidentiality, and what the scope of a first responder mental health clinic should be.
Supplemental Material
sj-docx-1-his-10.1177_11786329251333019 – Supplemental material for A Qualitative Study on the Design and Implementation of a First Responder Operational Stress Injury Clinic
Supplemental material, sj-docx-1-his-10.1177_11786329251333019 for A Qualitative Study on the Design and Implementation of a First Responder Operational Stress Injury Clinic by Sarah E. MacLean, Nicole E. Edgar, Chloe Ahluwalia, Valerie Testa and Simon Hatcher in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329251333019 – Supplemental material for A Qualitative Study on the Design and Implementation of a First Responder Operational Stress Injury Clinic
Supplemental material, sj-docx-2-his-10.1177_11786329251333019 for A Qualitative Study on the Design and Implementation of a First Responder Operational Stress Injury Clinic by Sarah E. MacLean, Nicole E. Edgar, Chloe Ahluwalia, Valerie Testa and Simon Hatcher in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329251333019 – Supplemental material for A Qualitative Study on the Design and Implementation of a First Responder Operational Stress Injury Clinic
Supplemental material, sj-docx-3-his-10.1177_11786329251333019 for A Qualitative Study on the Design and Implementation of a First Responder Operational Stress Injury Clinic by Sarah E. MacLean, Nicole E. Edgar, Chloe Ahluwalia, Valerie Testa and Simon Hatcher in Health Services Insights
Footnotes
Acknowledgements
The study team would like to thank all of the participants who provided their time and expertise during this study. The study team would also like to recognize and thank the following individuals for their contributions to this project: Alexandria Bennett, Zachary Cantor, R. Nicholas Carleton, Ian Colman, Daniel J. Corsi, Deniz Fikretoglu, Alexandra Heber, Marnin J. Heisel, Jeffrey Jutai, Shannon Leduc, and Kednapa Thavorn.
Statements and Declarations
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.