
Abstract
Objectives:
This study aims to investigate patients’ privacy experience when receiving care in emergency departments (EDs) in Newfoundland and Labrador, Canada. We aim to assess the level of satisfaction with privacy and to assess for factors that improve or worsen the privacy experience, not limited to patient demographics, length of stay, and hospital location.
Methods:
This study used a mixed-methods design, gathering quantitative and qualitative data using a telephone survey and semi-structured interviews. Our primary outcome measure was patients’ privacy experience in the ED. The independent variables in our study were age, gender, ED location, patient-reported wait times, reason for ED visit, and healthcare provider involved in care.
Results:
Among the 821 patients who participated in the interviews, 1 in 4 patients (24%) did not have satisfactory ED privacy experiences. Multinominal logistic regression showed patients who waited 4+ hours before being examined by a provider [aOR = 0.34, 95% CI: 0.17-0.69] and those who visited the urban EDs [aOR = 0.17, 95% CI: 0.09-0.35] reported low levels of privacy. Furthermore, those whose overall length of stay was 4 to 8 hours [aOR = 0.44, 95% CI: 0.23-0.84] and 8+ hours [aOR = 0.36, 95% CI: 0.17-0.78] also reported dissatisfaction with ED privacy experience. Our qualitative analysis found privacy concerns in waiting rooms, triage areas, and curtain rooms, with females voicing more concerns than males.
Conclusion:
Patients with longer wait times and who have been seen in urban EDs experience less privacy. Our qualitative data shows that women also raised more privacy concerns than men and that waiting rooms and triage areas are the locations with the most reported privacy concerns. Patient experience and outcomes would benefit from improving patient privacy when receiving care in EDs.
Keywords
Introduction
Patient privacy is a long-established cornerstone of healthcare. 1 A physician’s responsibility to provide patients with adequate privacy is described ubiquitously in medical literature, ranging from the initial Hippocratic Oath written in the 10th century to the modern Health Insurance Portability and Accountability Act (HIPAA).1,2 With the growing emphasis on patient-centered care, healthcare systems are increasingly prioritizing patients’ needs, preferences, and values.3,4 This approach emphasizes delivering care that deeply respects individual patient preferences and ensures that their values guide every clinical decision.3,4 Central to this model is the protection of patient privacy, which is fundamental to trust, dignity, and ethical care. Safeguarding privacy strengthens the patient-provider relationship and upholds the integrity of care delivery in diverse healthcare settings.1-4
Studies have shown that patients are less likely to seek medical care, more likely to withhold health information, refuse physical examination, and less likely to follow management plans set out by their providers when their privacy is compromised.1,5 Diagnoses and management plans become less accurate and effective without complete information from patient histories and physical exams, leading to poorer patient outcomes.1,6,7 Therefore, to maximize the likelihood of patients being accurately diagnosed and properly treated, patients must first have a positive experience regarding their privacy.
A patient’s overall privacy experience, however, is subjective. 8 It depends on patient-specific factors (sex, age, culture, religion, and presenting medical complaint) and institutional-specific factors (healthcare setting, geographic location, occupancy, and staff). 8 For example, a middle-aged man presenting with a cough to an urban hospital in a large city where no one recognizes him will likely have a very different privacy experience compared to a young woman presenting with urinary symptoms to a small community hospital where other patients and staff recognize her.
In hospital settings where patients have minimal ability to influence their surroundings, they often encounter diminished privacy and heightened stress. 9 Being away from their personal space and comfort zone makes patients uneasy. 9 This makes them less likely to ask questions or express disagreement with their treatment plan. 9 Similarly, patients’ social privacy can be compromised in situations where patients must change their clothes in the presence of hospital staff, remove clothing from areas not related to their medical condition, or answer personal questions about their social lives or sexual health. 9 Finally, informational privacy may be compromised during patient-provider interactions, such as when a private screening area is unavailable, patient information is shared without consent, or when nearby patients can overhear sensitive medical details. 9 As such, emergency departments (EDs) provide a good example of a healthcare setting where a lot of personal health information is gathered and exchanged, allowing privacy breaches.
In the already hectic and high-pressure environment of EDs, the constant exchange of information between patients and providers increases the risk of privacy breaches, highlighting the critical importance of safeguarding patient privacy. 10 However, factors present within EDs, such as triage, waiting rooms, open floor designs, curtain-divided rooms, and high occupancy, make ensuring constant patient privacy difficult. 1 Additionally, Canadian EDs are experiencing many challenges, including long wait times, crowding, and boarding, which may add additional challenges to ensuring patient privacy. 11 Overcrowded EDs not only compromise physical space but also create environments where private conversations and examinations are more likely to be overheard, intensifying patient discomfort and fear of stigma. 12 This is especially critical for individuals seeking care for sensitive conditions, who may delay or avoid visits altogether.12,13 In rural areas, where anonymity is even harder to maintain, privacy concerns become an even greater barrier. As previously discussed, since EDs can predispose to lower levels of privacy, patients may thus be at a higher risk of poor outcomes and have a decreased trust in the medical system. 7
Studies have consistently found positive privacy experiences correlated with increased overall satisfaction with ED care.7,8,14 Baghaei et al 7 found that patients reported a better privacy experience when cared for by nurses than by physicians. Many studies have shown that patients receiving care in walled ED rooms compared to curtained rooms experienced more privacy, allowing for more sensitive discussions and physical exams to be completed and resulting in a better overall privacy experience.14-16 Longer wait times and length of stay in EDs are related to decreased privacy satisfaction.8,14,15 Older patients have also been found to have poorer privacy.8,14 Nayeri and Aghajani 14 showed that the relationship between gender and privacy experience was insignificant, while another study found that women had poorer satisfaction with privacy and experienced more privacy breaches than men. 15 Thus, there remains conflicting data on how patient gender impacts ED privacy experiences, while no studies have explored how hospital location (rural vs urban) impacts privacy. There are also no prior studies addressing the ED patient privacy experience in Newfoundland and Labrador (NL), a predominantly rural and remote province in Canada.
With this study, we aim to understand further how patients are experiencing privacy while receiving care in EDs, specifically in Eastern Newfoundland. The goals of this study are twofold. First, to assess the degree of patient satisfaction concerning privacy upon receiving care in an ED; second, to determine how patient privacy experience is impacted by age, gender, ED location (rural vs urban), wait times, reason for ED visit, and healthcare providers involved in care.
Methods
Study design and setting
This mixed-methods study gathered quantitative and qualitative data using telephone surveys and semi-structured interviews. Survey questions were developed based on validated patient-reported experience surveys such as the Canadian Institute of Health Information Patient-Reported Experiences Survey, the Ontario Emergency Department Patient Experience of Care Survey, the Press Ganey Emergency Department Survey, and the NHS Accident and Emergency Department Questionnaire.17,18 A semi-Delphi approach was used with the SurgeCon team members and the patient research partner (PRPs) to finalize the questions.17,18 The survey was pilot-tested with 10 volunteers.17,18 More details on question selections and pilot testing are available via our published papers.17,18 The semi-structured interview guide was also created with PRPs and centered on respect, communication, information sharing, and the ED environment. We used a convergent design 19 where the survey and semi-structured interviews were complementary and used together to validate and strengthen the study findings.
The data presented in this paper has been extracted from an extensive multi-faceted project entitled “SurgeCon,” which aims to improve ED patient flow and patient experience.17,18 SurgeCon has been implemented at 2 rural and 2 urban EDs in NL through a Stepped-Wedge Cluster Trial.17,18 Details about this study are available via other publications (Trial registration number: NCT04789902).17,18 Ethics approval was obtained from the Health Research Ethics Authority (HREA) of Newfoundland & Labrador (HREB #2019.264). Table 1 presents a description of the study settings.
Description of the NL EDs Included in this study (data from 2021).

Data derived from The Town of Clarenville – Health Care. 20
Data derived from Eastern Health. 21
Sample size
The SurgeCon project was designed to detect a 30% change in patient-reported experience measures (5% Type I error rate and 80% power, with an intracluster correlation (ICC) of 0.1). 18 Therefore, a sample size of 1320 was calculated to be adequate. 18 Assuming a 50% response rate, we aimed to conduct 25 surveys per month at each ED. 18
Data collection
Data collected through the SurgeCon project during its control period in the 4 EDs are used in this study. Quantitative data using the telephone survey was collected from March 1, 2021, to July 27, 2023, and qualitative data using semi-structured interviews was collected from May 1, 2024, to July 29, 2024. All the patients who visited the 4 EDs during the study period were included in the study.17,18 Patients were randomly selected to complete the survey using a program that generates random date and time selections.17,18 This method ensured that participants were randomly chosen after ED discharge. For each month of the study, we randomly generated 25 date and time combinations that covered the morning, afternoon, evening, and night hours. There was a ±2-hour window where if no one visited the ED at the chosen time (eg, 1:30 AM), the next patient closest to it (eg, 1:41 AM) was selected.
After obtaining the selected participants’ contact details through medical records, a research assistant (RA) contacted them via telephone within 48 hours of their visit to provide an overview of the study and obtain informed consent.17,18 They were given the option to request the informed consent documentation via e-mail or post mail.17,18 Each participant’s verbal consent was recorded in a patient log form and whether they requested a digital/physical copy of the consent form. In the case of minors or patients who could not participate in the study, guardians/parents or caretakers were asked to provide consent and complete the survey on their behalf. The interviewer also had to check a box next to the following question: “The consent form was read and explained to the participant before receiving the participant’s consent, and the participant had knowledge of the research project and appeared to understand it” before administering the survey. During the survey, patients were asked to provide details on their demographics and experience with their ED visits.17,18
Finally, interested patients were also invited to participate in a follow-up semi-structured interview at a later date. Informed consent was also obtained to collect audio recordings of these interviews. Data collection was completed by male and female RAs with undergraduate degrees who completed ethics training and SurgeCon’s training for conducting quantitative and qualitative interviews. The telephone surveys and semi-structured interviews had an average duration of approximately 30 minutes. Survey participants were entered to win a random prize draw for gifts worth $200-$500, and all semi-structured interview participants were given a $25 gift card.
Quantitative analysis
Descriptive analysis was completed by deriving variables’ frequencies. The chi-square and Fisher’s exact tests were used for bivariate analysis of the independent variables with privacy. 25 Finally, due to collinearity between PIA and LOS [ρ (rho) = 0.56, P-value < 0.001], two multinomial logistic regressions models with PIA and LOS variables (Model I and Model II, respectively) were run separately with all other variables. R Studio for Windows (version 4.3.2) was used for analysis, and a P-value of <0.05 was considered statistically significant.
Our outcome measure was patients’ ED privacy experience, collected with the question: “Were you given enough privacy when talking to staff or while being examined or treated?” Patients could choose from 4 options, “Yes,” “Somewhat,” “No,” and “N/A.” Patients who answered “N/A” (n = 4, 0.5%) or did not respond to the question (n = 7, 0.8%) were not included in the analysis.
Independent variables in our study were age, gender, ED location, patient-reported wait times, reason for ED visits, and healthcare providers involved in care. We evaluated 2 types of wait times: PIA (Physician Initial Assessment) and LOS (Length of Stay). PIA was the time patients waited before being examined by a physician or their delegate. LOS was the total amount of time patients spent at the ED. The main reason for the ED visit was collected, and finally, patients confirmed the type of healthcare providers involved in their care. They had the option to select from “doctor,” “nurse,” or “resident,” and if they chose multiple providers, we included it as “more than 1 healthcare provider.”
Qualitative analysis
Thematic analysis 26 was employed to analyze the 10 open-ended survey questions and semi-structured interviews, focusing on extracting codes and themes related to patients’ ED privacy experiences. Five researchers reviewed the transcripts in the initial step and independently conducted open coding. This was followed by weekly meetings to compare and discuss the codes, explore emerging themes, and review and refine the themes. The researchers then defined the main themes and sub-themes from the analysis and described the content within each theme to provide a comprehensive understanding of the data. Open-ended questions in the survey were analyzed first, followed by semi-structured interviews to achieve cross-validation. Finally, findings were presented to PRPs for feedback. Qualtrics 27 and Microsoft Teams were used for data storage and analysis.
Patient research partnership
This patient-oriented research engaged patients as active partners throughout all stages, from conceptualization to knowledge dissemination.17,18 Our PRP committee comprises six individuals of diverse ages, genders, and ethnicities. These are community members, including patients, family members, or caregivers who have been part of the SurgeCon team since its inception, and we meet with them monthly to discuss our research progress.17,18 They played a key role in developing the survey questionnaire17,18 and the semi-structured interview guide used in this study, enabling us to include questions aligned with patient priorities. Following data analysis, we worked closely with them to gather feedback and integrate their lived experiences into the dissemination process, ensuring our study findings accurately reflected their perspectives.
Results
Quantitative results
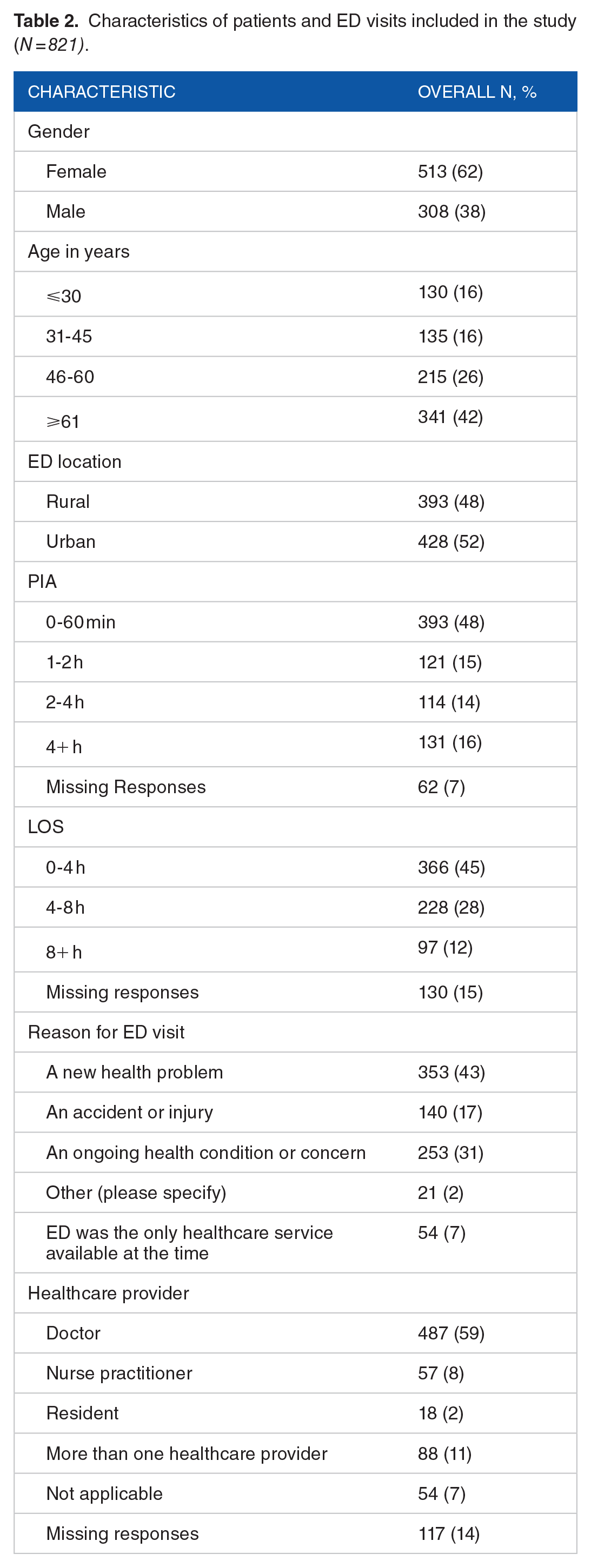
Among the 821 participants, 101 (12%), 101 (12%) and 619 (75%) responded with “No,” “Somewhat,” and “Yes,” respectively to their privacy experience. Participants were predominantly females (62%) and ⩾61 years old (42%). Missing responses were the highest in LOS (15%) and healthcare provider (14%) variables; Table 2.
Characteristics of patients and ED visits included in the study (N = 821).
The chi-square test showed that age, ED location, PIA, and LOS were significantly associated with privacy (P < 0.05), and Fisher’s exact test showed that the variable healthcare provider was also associated with privacy (P < 0.001); Table 3.
Factors associated with patient privacy experience in 4 EDs of NL from 1 March 2021 to 27 July 2023 (N = 821).
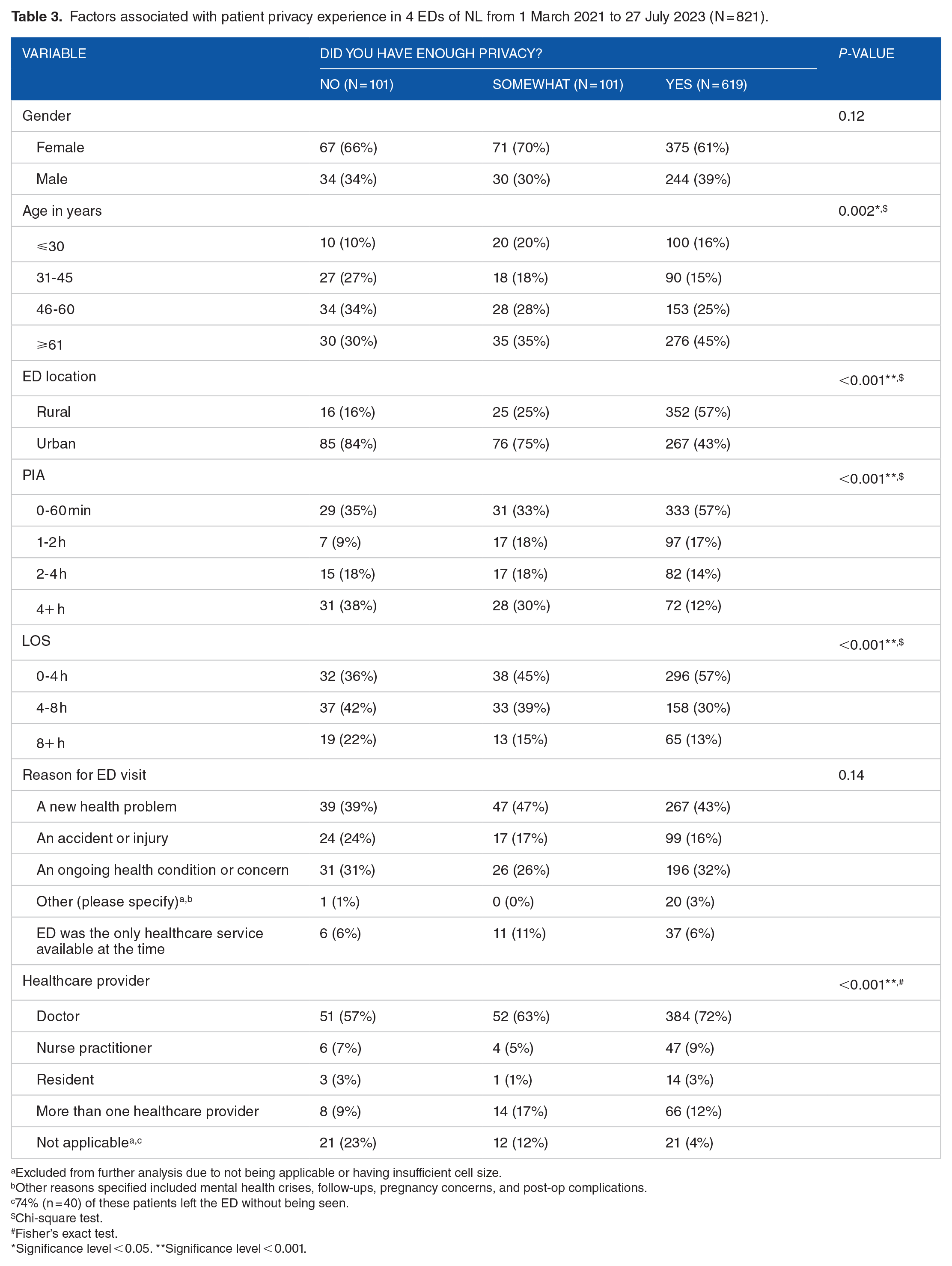
Excluded from further analysis due to not being applicable or having insufficient cell size.
Other reasons specified included mental health crises, follow-ups, pregnancy concerns, and post-op complications.
74% (n = 40) of these patients left the ED without being seen.
Chi-square test.
Fisher’s exact test.
Significance level < 0.05. **Significance level < 0.001.
As shown in Table 4, in the multinomial regression model of privacy with PIA (Model I), no significant variables were found for “Somewhat” versus “No” privacy levels. However, in “Yes” versus “No,” hospital location and PIA were significant. Visiting urban hospitals [adjusted Odds ratio (aOR) = 0.17, 95% Confidence Interval (CI): 0.09-0.35] and waiting 4+ hours before being examined by a provider [aOR = 0.34, 95% CI: 0.17-0.69] were associated with not experiencing enough privacy.
Multinomial logistic regression analysis of factors that affect patient privacy experience in 4 EDs of NL.

Significance level < 0.05. **Significance level < 0.001.
Similarly, in the multinomial regression model of privacy with LOS (Model II), no variables were significant for “Somewhat” versus “No” privacy levels; Table 4. Visiting urban hospitals was again found to be associated with insufficient privacy [aOR = 0.18, 95% CI: 0.09-0.36] in the “Yes” versus “No” privacy levels. Furthermore, patients whose overall length of stay was 4 to 8 hours [aOR = 0.44, 95% CI: 0.23-0.84] and 8+ hours [aOR = 0.36, 95% CI: 0.17-0.78] were more likely to choose “No” compared to “Yes” when asked if they experienced enough privacy.
Qualitative results
Of the 821 participants, 57 (7%) provided additional comments about privacy, and 5 patients participated in the in-depth semi-structured interviews, at which point we reached thematic saturation. Two key themes emerged from the analysis of open-ended questions and semi-structured interviews: (1) Challenges of ED Environment and Structure and (2) Confidentiality Concerns.
(1) Challenges of ED environment and structure
ED environment and structure were a predominant theme. Overcrowded waiting rooms and insufficient wait areas led to a lack of space in the ED. Due to overcrowding and limited space, patients often received treatment in areas that were not private or were relocated to different rooms outside of the waiting area in an effort to gain some privacy.
“People were sitting on the floor in the waiting room. . .which also led to having no privacy. . .when asked for a more private space, the nurse rolled her eyes, which was uncomfortable. The ED was overcrowded. . .was treated via IV in the hallway, and the hallways were so full that someone tripped on the IV lines.” - Survey response from a female patient, ⩽30 years old, who visited an urban ED. “[Patient] talked about waiting to be seen for over 8 hours. . .was in so much pain and crying and the other patients waiting kept staring. . . ended up being moved to the waiting room for CT scans so she could have some privacy.” – Survey response from a female patient, 31-45 years old who visited a rural ED
Curtained cubicles in the ED contributed to privacy issues. Unlike solid walls, curtains provide minimal separation between patients and compromise personal space. These curtains are sometimes absent altogether, further exposing patients to others in the room and adding to the negative patient experience.
“The privacy was not great because [patient] was only separated by curtains from other patients.” – Survey response from a male patient, ⩾61 years old, who visited an urban ED. “No privacy whatsoever, no curtains in the room, not comfortable talking about anything.” – Survey response from a female patient, ⩾61 years old, who visited a rural ED. “Only curtains between patients, not a lot of privacy.” – Survey response from a male patient, 46-60 years old, who visited an urban ED “[Patient’s mother] also mentioned being put in a room with another patient with only a curtain between them, which she didn’t love for privacy reasons.” – Survey response from the mother of a female patient aged ⩽30 years old, who visited a rural ED
(2) Confidentiality concerns
Several patients raised confidentiality concerns due to the structure of check-in, triage, and waiting areas. EDs with check-in and triage close to the waiting area made patients uncomfortable with sharing and overhearing medical history and other confidential information due to proximity to other patients and staff.
“There is a total lack of privacy in the ED; it is ridiculous. I don’t understand why triage can be private, but you have to give the front desk all your details in front of everyone. I can’t imagine being the victim of sexual assault and having to explain to the entire waiting room why you’re there.” – Survey response from a male patient, 46-60 years old, who visited an urban ED. “Little to no privacy when checking in” – Survey response from a male patient, 31-45 years old, who visited an urban ED. “[Patient] was incredibly bothered by the lack of space and privacy in the ED. . .felt very uncomfortable. . .could hear many other patients' health concerns. . .there was no separation between triage and the waiting room. . .patients had to yell through the plexiglass. . .a good portion of the waiting room could hear all of the personal information.” – Survey response from a female patient, ⩾61 years old, who visited an urban ED.
PRP feedback
This study was reported to our PRP team. One of the PRPs commented on prolonged wait times affecting privacy: “The longer we [patients] wait, the more we go to check if it is time to be seen – hence making us feel we don’t have enough privacy.” The PRPs also agreed that urban EDs provide less privacy than rural EDs. They said: “The urban EDs here are overcrowded; we often see patients on stretchers in the hallways. In rural EDs, staff are more cautious of putting patients in the same room.” Overall, the PRPs agreed with our findings and confirmed that they align with their experiences.
Discussion
Interpretation of findings
Our study shows that 1 in 4 patients reported insufficient privacy in the ED. The longer patients waited or stayed in the ED, the more they reported issues with privacy. Patients who visited the urban EDs also reported less privacy. Privacy concerns were generally due to overcrowded waiting rooms, proximity to other patients in the reception and triage areas, and curtained cubicles, leading to discomfort in sharing and overhearing health concerns and an overall negative ED experience.
Comparison to previous studies
Most studies on patient privacy experience found that only 50% to 64% of patients had satisfactory privacy levels.14,16,28,29 However, we found that more patients (ie, 75%) reported sufficient privacy. Previous literature associates increased age with poorer privacy.8,14 However, age was not significant in our multivariate analysis. Our thematic analysis also did not show any patterns in privacy among patients of different ages. Our findings that patients with PIA and LOS of 4+ hours had less privacy are consistent with previous literature associating prolonged wait times with poorer privacy.8,14 Patients visiting urban EDs were also at least 81% less likely to experience enough privacy than those who visited rural EDs. To our knowledge, no prior studies have compared privacy experiences between rural and urban EDs. In our quantitative analysis, gender was not significantly associated with privacy. Nayeri and Aghajani 14 found no association between privacy and gender, while another study found that women reported worse privacy than men.14,15 Our qualitative analysis did not show that patient-provider gender concordance impacted privacy experience. Our literature search also found no prior studies directly addressing patient-provider gender concordance with privacy experience. However, there is evidence that gender concordance does impact overall patient experience. 30 The reason for ED visits and the type of healthcare provider was not associated with privacy experience in this study. One study found that nurses provided more privacy than physicians, 7 while another study found that physicians were more cognizant of patient privacy than nurses. 31 There exists little data assessing the reason for ED visits and privacy. Although our qualitative results did not show any major theme related to reasons for ED visits and privacy, there were certain instances where patients raised confidentiality concerns when overhearing sensitive ED visit reasons or having to share rooms with multiple other patients. One study showed that patients seeking care for sensitive conditions, such as a female patient presenting with hemorrhoids, report heightened privacy concerns. 13 This highlights the need for further studies to explore the relationship between the acuity of medical issues and patients’ privacy experiences.
Our qualitative analysis revealed privacy concerns around the ED environment due to insufficient space at reception, triage areas, and waiting rooms. This caused discomfort in sharing personal information and health concerns and overhearing other patients’ confidential information. A systematic review identified privacy and security as key themes in the ED environment, showing that privacy was affected by several factors, including “personal information overheard by others” and “overhearing others’ personal information.” 32 Curtained cubicles also led to a lack of privacy, consistent with previous literature.14,15,29,33 However, privacy concerns related to structural layouts are not confined to ED environments. Research on Primary Health Centers (PHCs) in Indonesia revealed that privacy is compromised when consultation room doors are left fully or partially open or when overcrowding forces multiple patients to share the same consultation space. 13 Similarly, redesigning the layout of an ED obstetric unit by replacing curtained cubicles with walled cubicles significantly enhanced perceptions of privacy and confidentiality, with satisfaction rates rising from 21% to 89%. 34 Private rooms in acute care settings have been proven to enhance patient privacy, allowing individuals to control their personal information and offering a quiet space for rest and private conversations with family and friends. 35 In cancer care centers, patients have strongly preferred privacy, favoring single treatment rooms and waiting areas designed to avoid the traditional “rows of chairs” layout often seen in healthcare settings. 36 This further supports our suggestions to focus on the ED environment and layout to improve privacy.
Finally, our study showed the importance of wait times in determining the ED privacy experience. While wait times are an established factor affecting patient satisfaction with ED services, our analysis shows that they affect other aspects of care, including privacy. This is the first study in NL to show the relationship between wait times and privacy. Our mixed-method approach strengthens our results and supports the importance of decreasing wait times to improve ED patient privacy.
Strengths and limitations
In our study, three out of four participants (75%) responded to the survey and semi-structured interviews. Nonresponse was attributed to factors such as unavailability, lack of interest, and concerns about the call being perceived as spam. Some of the survey responses to LOS (15%) and type of health care providers (14%) were lost due to an error in the data collection software, Qualtrics. 27 However, a sensitivity analysis showed that the lost data did not impact results (results not shown). Given the nature of data collection using a survey, there is potential for response bias, with more females responding to the survey than males. However, patients were contacted randomly, thus reducing response bias. Given the duration of the study and the time elapsed between the telephone survey and the semi-structured interviews, there is a possibility of recall bias, as patients may have forgotten details of the specific ED visit for which they were recruited, potentially conflating it with similar visits. However, the mixed-methods approach employed in this study helps mitigate these concerns. The RA collecting survey data paraphrased some responses to open-ended questions, which may have introduced potential interviewer bias. Additionally, while patients themselves completed most surveys, a small number (approximately 10%) may have involved input from guardians, parents, or caregivers. This could limit the accuracy of reported patient satisfaction with privacy, as proxies may be less able to capture the patient’s perspective fully.
Using the convergent mixed-method design, 19 data were collected through the survey and semi-structured interviews separately, with survey data providing a quantitative perspective and semi-structured interviews offering qualitative insights. Collecting and analyzing the quantitative and qualitative data independently and then integrating the results proved valuable in enhancing the comprehension and understanding of privacy concerns. This integration was particularly beneficial in studying the complex phenomenon of privacy in the dynamic environment of the ED.
Evidence suggests that ethnicity and gender identity may contribute to increased privacy breaches, with one study showing immigrant, HIV-positive, and Black trans-feminine patients reporting more privacy concerns than their white counterparts. 37 Our study could not find evidence of this, and further research is necessary to explore the privacy experiences of ethnically and gender-diverse populations more comprehensively. Furthermore, our quantitative section did not specify between privacy concerns, such as auditory versus visual or personal privacy breaches versus overhearing others’ information. However, we collected this information via semi-structured interviews and open-ended questions. The follow-up semi-structured interviews also allowed us to gather in-depth information on privacy without limiting us to survey data. This mixed-method approach allowed us to elaborate on quantitative results and examine the complexities of ensuring privacy in EDs. Finally, as patient partnership was one of the prominent components of this study, it allowed us to gain a deeper understanding of patient perspectives and experiences.
Clinical and research implications
Given that our results identified triage areas causing less privacy, future interventions to improve privacy at ED triage could be beneficial. 12 Bigger waiting rooms to avoid overcrowding, walled cubicles, not having multiple patients in the same room, and a more private triage area are some solutions for improving the ED privacy experience. Patients generally prefer not to be triaged in the same area as the waiting room. Separating triage and waiting rooms could be the first step toward enhancing patient privacy experience. Understanding how specific patient groups perceive and experience privacy is also necessary to meet patient needs and expectations concerning privacy. Interviewing patients who leave the ED without being seen might also help to identify if privacy is one of the reasons for leaving the ED. Finally, our survey was administered as part of a more extensive study. However, regularly assessing patient feedback and implementing it for continuous improvement in the ED can ultimately lead to higher-quality care.
Lengthy waiting times and overcrowding are two other important aspects of the privacy experience that need to be improved, especially in Canada.8,11 ED overcrowding is a well-documented global challenge affecting patient experiences and clinicians’ capacity to deliver effective care. 12 This issue is often exacerbated when patients endure prolonged waits in ED hallways until inpatient beds become available. 12 Such patients usually lack physical privacy and have limited opportunities to share sensitive information with healthcare providers discreetly. 12 Additionally, this can also leave patients feeling disrespected. 12 Together, these factors violate patients’ physical, social, and informational privacy.9,12 Our qualitative findings revealed that patients often avoid ED visits due to overcrowding (results not shown). While this does not directly indicate avoidance due to privacy concerns, it underscores the need for improved policies to manage patient volumes effectively, reduce wait times, and enhance patients’ privacy experience.
Conclusion
Patient privacy has implications for patient experience and outcomes in EDs. This study demonstrates that patients in urban EDs with longer wait times are likelier to have worse privacy experiences. We also identified triage areas and waiting rooms as a frequent source of privacy complaints. Addressing these issues will ensure that all patients feel safe, respected, and valued when interacting with healthcare providers and the broader healthcare system. Therefore, improving privacy measures will enhance the patient care experience and foster trust and confidence in the healthcare system.
Footnotes
Acknowledgements
We sincerely thank our patient partners for their invaluable contributions to the development and successful completion of this manuscript. We also appreciate all team members’ advice and support: Dr. James Rourke, Dr. Kris Aubrey-Bassler, Dr. Jennifer Jewer, and Dr. John Knight. We also thank all the interviewers for assisting in data collection.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors (SA, CP, DS, PW, HE, HM) are currently receiving financial support from the Canadian Institutes of Health Research (Grant No. SR4-165123), the Government of Newfoundland and Labrador (Grant No. 5404-2312-101), Newfoundland and Labrador Health Services, Memorial University of Newfoundland, and the Trinity Conception Placentia Health Foundation for the continued development of the SurgeCon platform to improve emergency department wait times and patient satisfaction.
Declaration of conflicting interest:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CP and PN are the co-founders of SurgeCon Innovations. Our team received funding for a project entitled “SurgeCon: An Emergency Department Surge Management Platform” from the Canadian Institutes of Health Research, Newfoundland and Labrador Provincial Government, Newfoundland and Labrador Health Services, and the Trinity Conception Placentia Health Foundation. PN has a royalty-sharing agreement with MOBIA Technology Innovations and the Newfoundland and Labrador Health Services.
Author Contributions
All authors actively contributed to the research and manuscript development and were consulted for their expertise at every stage of the process.
Detailed of their contributions are as follows:
• Conceptualization: All authors.
• Formal analysis and methodology: Aswathy Geetha Manukumar, Matthew Miller, Hensley Mariathas, Nahid Rahimipour Anaraki, Anna Walsh, Oliver Hurley, Peter Wang, Shabnam Asghari.
• Results interpretation: All authors.
• Writing – original draft preparation: Aswathy Geetha Manukumar, Matthew Miller.
• Writing – review and editing: All authors.
Ethical Considerations
Ethics approval for this study was obtained from the Health Research Ethics Authority (HREA) of Newfoundland & Labrador (HREB #2019.264)
Consent to Participate
Participants provided informed verbal consent and could request to receive a copy of their consent documentation via electronic or post mail before participating in the study.
Data Availability
Data cannot be made available due to restrictions on data-sharing agreements. For more information, please contact