
Abstract
Introduction:
Telemedicine is a growing segment of the healthcare industry. As telemedicine gains prominence in Japan, the importance of telemedicine patient satisfaction research will also grow. This study examines whether Japanese patients are equally impacted by the same latent dimensions discovered in the multi-dimensional service satisfaction model used by a United States (U.S.) study.
Methods:
The subjects (n = 110) were patients who received telemedicine service between January and December 2023 at Juntendo University Hospital, Tokyo, Japan. Patient satisfaction perceptions were collected using a questionnaire composed of Likert scale items. Overall patient satisfaction served as the dependent variable, and patient perceptions of various aspects of the service were the independent variables. LASSO regression analysis was used to test the impact of the independent variables on overall patient satisfaction along with cluster analysis to examine the satisfaction ratings based upon patient characteristics.
Results:
Japanese patient perceptions of telemedicine health benefits were the most impactful driver of overall satisfaction. Cluster analysis indicated that males were generally more satisfied than females. The least satisfied patients were predominately female and those experiencing telemedicine for the first time. Patients receiving service from a specialist physician were least satisfied with the telemedicine financial costs.
Discussion:
Patient satisfaction levels were found to be highly impacted by perceptions of the health benefits received and the non-financial costs of service. These benefits could be highlighted by Japanese telemedicine providers to increase utilization of telemedicine services. Patient satisfaction was also found to be influenced by patient-centered care (ie, the “soft skills” of providers) to a lesser degree. Therefore, Japanese telemedicine providers may benefit from developing patient-centered communication skills.
Conclusion:
The model used provides nuanced understandings of telemedicine patient satisfaction, which highlights where targeted improvements in Japanese telemedicine patient satisfaction are likely to be most impactful.
Introduction
Telemedicine has become a significant segment of the global healthcare industry.1,2 The COVID-19 pandemic was a major driver for telemedicine’s uptake due to its many benefits, which include reduced patient/provider exposure to infectious diseases,3,4 greater patient access to healthcare services, and increased flexibility of hospital resource utilization.3,5,6 Recognizing its value, the Japanese government has promoted the use of telemedicine by easing telemedicine regulations in the Japanese national health insurance system both during and after the pandemic.
The resultant increase in accessibility to telemedicine may help Japan’s healthcare system tackle other growing challenges facing the nation. For example, approximately one-third of Japan’s population is over the age of 65, and this age category is expected to grow 7 —increasing healthcare demand. 8 In addition, many members of this elderly population live in rural areas, decreasing accessibility to medical facilities. 9 Making matters worse, Japan currently faces a simultaneous shortage of healthcare professionals. 7 The aforementioned factors are likely to pressure the Japanese healthcare system to increase its telemedicine utilization rate. As telemedicine gains prominence in Japan, the importance of telemedicine patient satisfaction research will also grow.4,10-12
Telemedicine patient satisfaction has typically been measured using survey data,10,13,14 with a focus on obtaining a global measure of satisfaction (ie, “how satisfied are you with the telemedicine service received?”). 15 Unfortunately, global measures don’t highlight what aspect(s) of the telemedicine service led to a patient’s overall satisfaction level. 16 However, Mason 17 recently studied United States (U.S.) telemedicine patient satisfaction using a multi-dimensional marketing service satisfaction model known as SERVQUAL to identify latent dimensions of telemedicine patient satisfaction. With a modified version of this model, Mason’s 17 study identified 4 dimensions of telemedicine patient satisfaction: health benefits, patient-centered care, financial costs, and non-financial costs. In short, the dimension of health benefits encompassed patient perceptions of healthcare outcomes (eg, access, safety, achievement of desired health outcomes, etc.). Telemedicine patient-centered care included patient perceptions of the provider’s communication skills (eg, responsiveness, attentiveness, trustworthiness, etc.). Financial costs included the monetary costs (eg, fees, insurance coverage, etc.) incurred to acquire telemedicine service, and non-financial costs included time-saving conveniences and service complexities (eg, technology requirements, equipment problems, etc.). Mason 17 concluded that patient-centered care had the greatest impact on overall U.S. telemedicine patient satisfaction.
Mason’s 17 findings are evidence that a multi-dimensional measurement can provide insights into the primary drivers of telemedicine patient satisfaction. The current study uses the dimensions of telemedicine patient satisfaction identified in Mason’s 17 study to examine Japanese telemedicine patients. Given differences exist between the Japanese and U.S. cultures and healthcare systems, this study examines the research question of whether the primary driver of telemedicine patient satisfaction is the same or differs between Japanese patients and the U.S. patients observed by Mason. 17
Methods
We conducted a single-center, cross-sectional, observation study involving people who had received telemedicine services in Japan. All study subjects met the following inclusion criteria: aged ⩾ 20 years old and the reception of telemedicine services from the study site within the previous year (January 1st, 2023 to December 31st, 2023). The questionnaire created and validated via exploratory factor analysis by Mason 17 for analysis of U.S. telemedicine patient satisfaction was translated into Japanese and sent to Juntendo University Hospital telemedicine patients (See Appendix).
Prior to launching the study, the authors acquired approval to gather human subject data from the Juntendo University Hospital Institutional Review Board. The hospital identified 399 candidate patients (317 females: 82 males) who had received telemedicine services at Juntendo University Hospital (a 1051-bed university-affiliated hospital in Tokyo, Japan) between January and December 2023. Since the hospital does not typically solicit survey responses from patients for research purposes, a letter was mailed to these patients to inform them that they could opt out of receiving an email invitation to participate in the survey. Seventy-seven candidates opted out, leaving a panel of 322 patients (256 females: 66 males). In January of 2024, the panel was sent an email containing a link to participate in the survey via REDCap, a secure web application that can create and manage online surveys and databases. Participation in the study was voluntary and subjects were required to provide consent before starting the survey. Patient responses to the questionnaire were collected during the months of January and February of 2024.
The 4 dimensions of telemedicine patient satisfaction, identified by Mason 17 —health benefits, patient-centered care, financial costs, and non-financial costs—represented the independent variables. The dependent variable was “overall” telemedicine patient satisfaction. Likert scales were used to measure the dependent and independent variables. Patients rated their perceptions of their telemedicine experience by providing their agreement with descriptive statements that were scaled from “1—strongly disagree” to “7—strongly agree.” Higher scores for each item indicated higher satisfaction with the evaluated item. Each independent variable was measured with multiple items. Health benefits was assessed with 5 items. Patient-centered care was measured with 14 items. Patients’ perceptions of telemedicine financial costs and non-financial costs were measured with 4 and 5 items, respectively. Four items were used to calculate the dependent variable. All independent and dependent variables were computed by averaging the items used for each respective variable. The complete set of questionnaire items is provided in the Appendix.
Reliability of the measurement items for the respective independent and dependent variables was assessed with Cronbach’s Alpha coefficients—commonly used in consumer behavior research. 18 A correlation analysis was conducted to examine the significance of independent and dependent variable correlation. A Least Absolute Shrinkage and Selection Operator (LASSO) regression analysis was used to examine the explanatory power of the independent variables for predicting overall patient satisfaction. This technique uses machine learning statistical modeling to examine the predictive power of variables. LASSO is preferred over regression methods for more accurate predictions, especially in data sets with multicollinearity. 19 Finally, cluster analysis was performed to examine the satisfaction ratings based upon patient characteristics.
Results
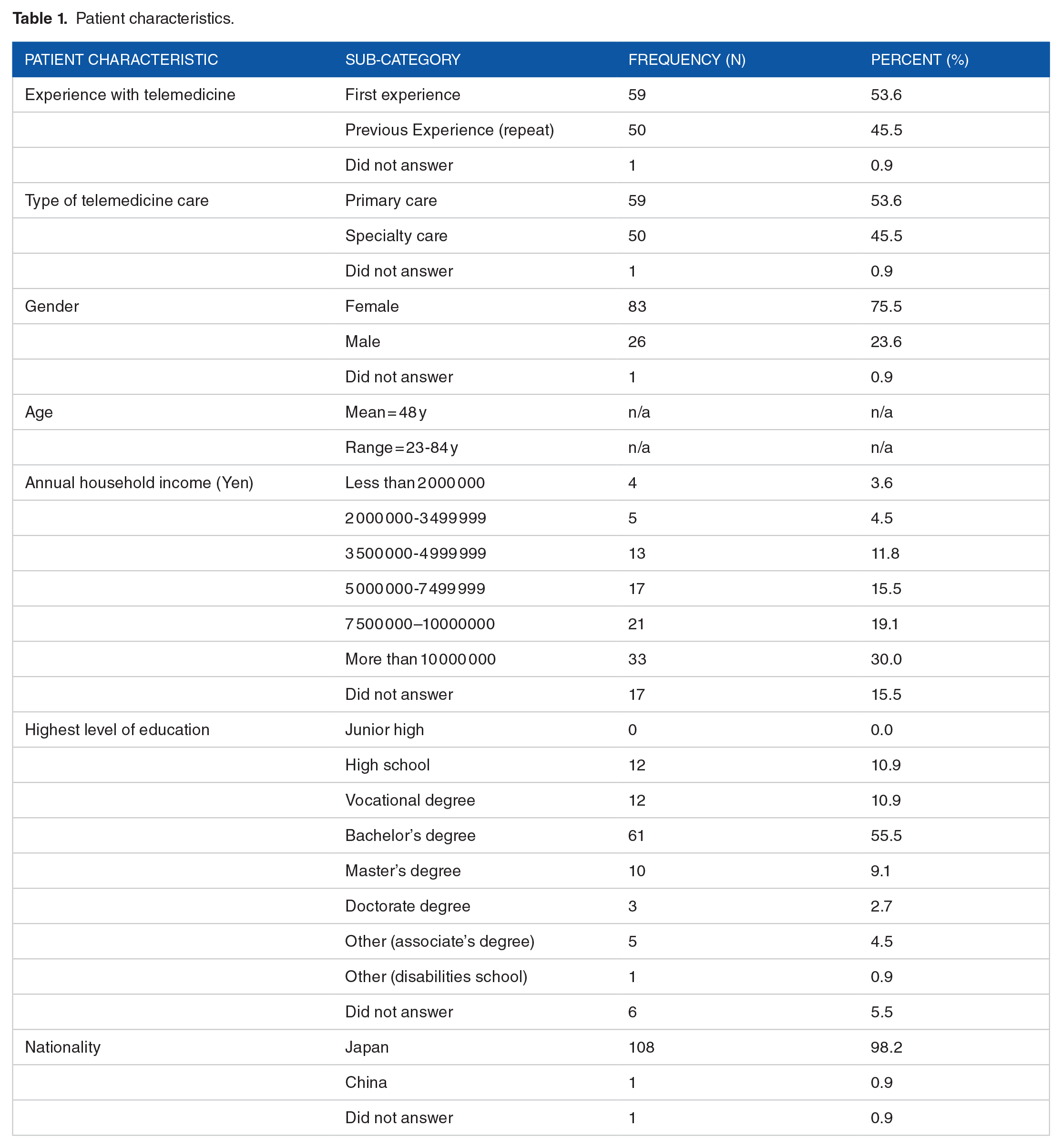
Of the sample pool (322 patients), 110 (34%) responded in full to the questionnaire. The raw data collected is securely stored with the lead author and will not be made public. Table 1 provides a summary of patient characteristics. A little more than half of the patients were first-time telemedicine users, and telemedicine for primary care was the most common type of care received. Due to the subject panel being ~80% female, it was not surprising that the patients’ gender was skewed highly toward females (76%). In addition, respondents were predominately of Japanese nationality. Other than the disproportionate number of females, the sample demographics appeared to be representative of the Japanese telemedicine patient population reported by others. 20
Patient characteristics.
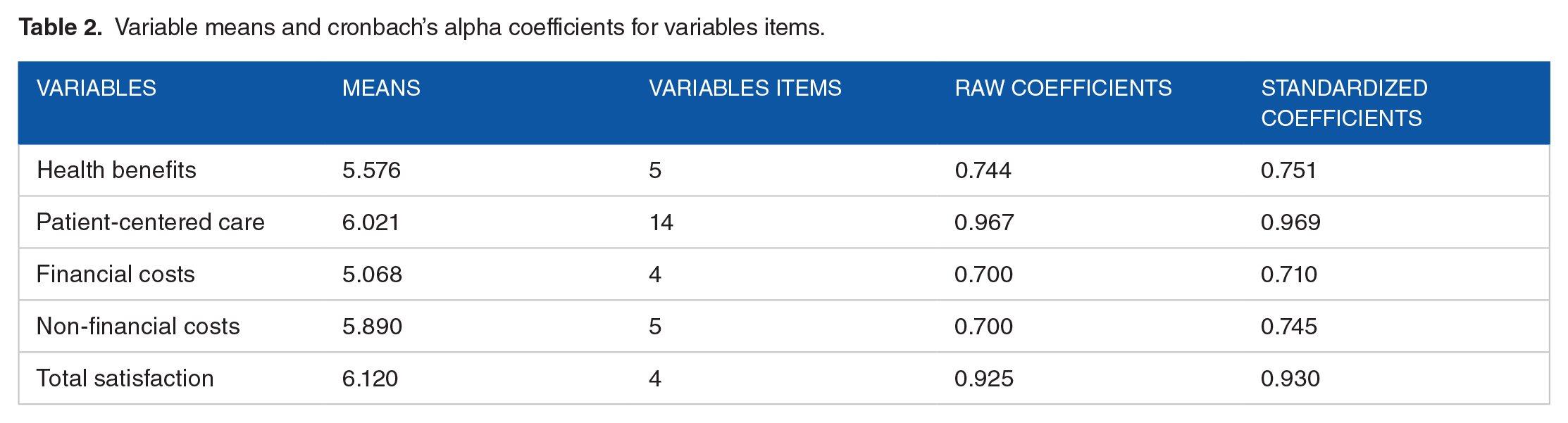
Cronbach’s Alpha coefficients (raw and standardized) were used to validate the reliability of the items used for all independent and dependent variables. The raw coefficients are based upon the correlation of the items to the defined variable. The standardized coefficients are based upon item covariances. Table 2 provides the item reliability coefficients for each of the independent and dependent variables. With all coefficients at 0.70 or higher, the items suggest long held appropriate levels of significance. 18 Thus, the items used to compute the independent and dependent variables were found to be reliable. Table 2 also provides the means for each of the variables. The overall average telemedicine satisfaction score was 6.12 on the 7.0 scale, indicating an even higher overall satisfaction than the U.S. patients (5.6) in Mason’s 17 study. Financial costs, being the lowest mean, appears to be the least favorable aspect of the telemedicine services. Patient-centered care had the highest mean, indicating the patients were most favorable of this dimension of overall satisfaction.
Variable means and cronbach’s alpha coefficients for variables items.
When numerous reliable independent variable items are used to measure a given construct, multicollinearity is likely to occur. Table 3 provides the correlation matrix for all the variables. As expected, high correlations among the independent variables were observed. Correlations among all variables were highly significant. The p-values for the correlation coefficients were less than .0001 except for between patient-centered care and financial costs, with a P-value of .003.
Correlation matrix.

Given the high variable correlations, LASSO regression analysis was performed to isolate which satisfaction dimension has the most powerful ability to predict differences in patients’ total telemedicine satisfaction levels. This technique is important given multicollinearity among independent variables. For example, health benefits clearly exhibit a strong, 69.23%, correlation with patient-centered care and a 59.83% correlation with non-financial costs (see Table 3). This high multicollinearity can cause issues in traditional regression analysis, such as inflated standard errors and unstable coefficient estimates. The results presented in Table 4 demonstrate that two of the variables, health benefits and non-financial costs, had highly significant predictive power for patient total satisfaction (P < .0001). Patient-centered care was marginally significant (P = .0764).
LASSO regression predictive variables model.

As the findings in Table 4 show, among the 4 independent variables, health benefits have the strongest explanatory power impact on total satisfaction (t = 4.21). Non-financial costs and, to a lesser extent, patient-centered care also impact total satisfaction. However, financial costs were not found to have a significant impact on total satisfaction.
As shown in Figure 1, the large, standardized coefficients for health benefits and non-financial costs indicate a parsimonious model of 2 variables would be very strong fit. The corrected Akaike Information Criterion (AICC) was used to adjust for the small sample size to prevent overfitting (see the lower portion of Figure 1). The AICC identifies the number of predictors that strike the best balance between goodness of fit and complexity, as based on the lowest AICC value. As shown in Figure 1, the AICC marginally drops as each variable enters the model and becomes relatively flat and nears 0 after the fourth variable (financial costs). Thus, while patient-centered care and financial cost are insignificant in LASSO regressions, their inclusion still improves model fit.

Visual representation of the LASSO regression results.
For additional insights, cluster analysis was performed to separate the patients into groups, which evaluated the satisfaction dimensions similarly to each other. Several cluster groupings were observed; however, 4 clusters provided the most insights, and the computed Cubic Clustering Criterion was 9.774. Table 5 identifies the 4 clusters. Cluster 1 patients rated all satisfaction dimension at the highest level and had the highest overall satisfaction. Cluster 2 patients rated all but one satisfaction dimension lower than the other groups and had the least overall satisfaction. Cluster 3 provided medium ratings across all satisfaction dimensions and had more moderate overall satisfaction levels. An interesting finding was with patient cluster 4, where ratings varied across the satisfaction dimensions. Compared to the other patient groups, cluster 4 patients had the second highest ratings for health benefits, patient-centered care, and non-financial costs. However, this group had the lowest ratings for telemedicine financial costs. Overall, cluster 4 patients were very satisfied with their telemedicine experience except for the financial costs of the service.
Patient cluster analysis results.

Notable difference compared to other cluster groups.
To better identify the background of patients in each cluster group, demographics associated with each cluster are provided in Table 6. Compared to other patient clusters, the cluster 1 patients (most satisfied) had the highest concentration of males. Cluster 2 patients predominately experienced telemedicine for the first time and had the highest concentration of females. Cluster 3 patients did not show any characteristics that stood out as either the highest or lowest. The notable differences among cluster 4 patients were that this group primarily received specialty care and were more financially affluent.
Patient cluster demographics.

Notable difference compared to other cluster groups.
Discussion
As shown in Table 1, the study’s respondents had an average age of 48 years old with a higher ratio of women to men (76:24). By comparison, Mason’s 17 U.S. respondents had the same average age of 48 years old; however, it had an even gender split (50:50). In both studies, a majority of the respondents held a bachelor’s degree or higher (67% and 60%, respectively). Respondents in both studies also had similar median annual household income ranges after converting yen to dollars at the average 2023 exchange rate (1$ = 141¥). The median U.S. dollar equivalent income of respondents in this study was $53 000–$71 000 whereas it was $50 000–$74 999 in Mason’s 17 study. Finally, all respondents in this study were Asian—mostly Japanese (98%). In contrast, only a small minority of Mason’s 17 respondents were Asian (5%), with the largest majority being Caucasian (83%).
A major finding by Mason 17 was that U.S. patients’ overall satisfaction of telemedicine was impacted most by their perceptions of the patient-centered care received. Thus, Mason 17 concluded that healthcare providers can improve patient satisfaction with telemedicine services by being empathetic, caring, and responsive to the emotional needs of their patients. However, as Table 4 shows, for Japanese patient satisfaction, the variables with the greatest impact were patient perceptions of health benefits and the non-financial costs of the telemedicine service.
Differences in how satisfaction is formed between U.S. and Japanese patients are likely the result of differences that exist between the countries. Americans tend to be more demanding with regards to their individual needs than Japanese nationals. 21 This may explain why U.S. patients’ total satisfaction was most impacted by their perceptions of the patient-centered care received. However, in the more collective-oriented culture of Japan, patients may be more lenient in evaluating patient-centered care, making patient-centered care potentially a less salient determinant of their overall satisfaction. While patient-centered care was found to be a less significant driver of Japanese patients’ overall satisfaction, it does still have an effect. Thus, healthcare providers can differentiate themselves by developing effective patient-centered communication. This would include training telemedicine providers to be responsive to the needs of patients and having an empathetic and caring attitude.
Another potential difference in Japanese and U.S. patients could result from their differing healthcare systems. For example, health care in Japan is nationalized with strict price controls and universal health insurance, whereas health care in the U.S. is primarily a privatized system with high associated costs. This may explain why the financial costs of telemedicine in Japan were found to be insignificant discriminators of overall satisfaction as compared to the U.S. patients in Mason’s 17 study.
A benefit of using a multi-dimensional examination of telemedicine patient satisfaction is that it can uncover nuances in patient perceptions that can lead to improved satisfaction. For example, while the patients observed were generally satisfied with their telemedicine service, as shown in the patient cluster analysis (Table 5), cluster 1 patients were the most satisfied and cluster 2 patients were the least satisfied. Table 6 revealed that cluster 1 patients had the highest concentration of males (38%), which may indicate that the telemedicine service expectations of males were better met or that they are less critical of the services received. Cluster 2 patients were primarily composed of first-time telemedicine users (92%) and females (92%). This may imply that first-time telemedicine users and/or females have higher expectations that cause them to be more critical of the service received. Patients with these characteristics may need to be consulted to clarify their expectations regarding telemedicine services.
The cluster analysis also revealed that telemedicine financial costs can be a source of dissatisfaction for some (Table 5, Cluster 4). Based upon the characteristics associated with cluster 4, financial costs were found to be a less satisfying dimension of telemedicine service. Given that 64% of the patients in cluster 4 received care from a specialist (Table 6), it may be that the financial costs associated with specialty care are less attractive than with primary care. Japan requires patients to pay co-insurance when receiving care, which varies by factors such as income, age, and the type of medical service received. These characteristics can impact patients’ out-of-pocket expenditures for services. To improve patient satisfaction with telemedicine financial costs, telemedicine providers could possibly lobby to improve reimbursement opportunities from health insurance providers for specialty care.
Survey-based research has limitations, and this study is no exception. The sample size was small and, thus, the statistical power of the analysis may have limited the ability to provide adequate statistical significance of the findings. Also, the patients sampled were not selected by a randomized process; rather, the subjects self-selected to participate in the study. Therefore, the subjects may not be representative of the Juntendo University Hospital telemedicine patient population or the Japanese telemedicine population as a whole. Furthermore, the sample data does not control for the environment where subjects responded to the questionnaire. Also, while responses have been kept anonymous, the respondents may have been concerned that their responses might be traced back to them and, therefore, may have provided inflated satisfaction responses to please the healthcare providers or to avoid any consequences related to negative feedback. In addition, it is possible that some respondents may have been distracted or not equally focused when providing their respective response, and the questionnaire’s 7-point scales may have been difficult for patients that may be cognitively impaired.
Future research with a larger sample size is needed to replicate the use of the multi-dimensional measures used in the present study. Studies are also needed across multiple cultures and across various types of telemedicine services. Comparisons of the results of future research across culture and types of service will lead to refinements in the measures, resulting in reliable and valid outcomes, which can highlight specific areas for improvement in telemedicine services. Insights can also be achieved by investigating various potential moderating effects of demographic differences such as gender, education level, ethnicity, and income on patients’ telemedicine satisfaction levels.
Conclusion
Japan has a highly developed technology infrastructure. Therefore, it is well suited to take advantage of emerging technological advancements in the field of telemedicine, such as the advent of virtual spaces for the provision of care (eg, Meta’s metaverse). Technological developments such as these will likely lead to even greater use of telemedicine in Japan and, thus, the need to better understand Japanese telemedicine patient satisfaction. The comprehensive multi-dimensional approach used in this study establishes the most salient factors driving Japanese telemedicine patient overall satisfaction. The results observed also underscore differences in the formation of satisfaction for telemedicine services between Japanese and U.S. patients. Compared to their U.S. counterparts, Japanese patient overall satisfaction was impacted more by the perceived health benefits and non-financial costs of the service than the patient-centered care and financial costs of the service. The findings provide insights into the drivers of overall satisfaction and highlight areas where patients are most critical of telemedicine health care. Strategic effort focused on these key aspects of satisfaction could improve telemedicine services in Japan and lead to better outcomes, especially for those who have difficulties accessing in-person healthcare services.
Footnotes
Appendix: Telemedicine Patient Satisfaction Questionnaire Items
Acknowledgements
The author would like to thank Dr. Matt Brown (Professor, Arkansas Tech University) for data analysis suggestions. Also, the author thanks the editor and anonymous reviewers for their supportive comments and suggestions.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was supported by JSPS KAKENHI (Grant Number 23K09634) from the Japan Society for the Promotion of Science.
Declaration of conflicting interest:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceptualization (AM), Data curation (AM), Formal analysis (AM), Funding acquisition (AM), Investigation (AM, TN, SF, KA, KY, RK), Methodology (AM, TN, SF), Project administration (TN), Resources (AM, TN, SF, KA, KY, RK), Supervision (TN), Writing – original draft (AM), Writing – review & editing (AM, TN, SF, KA, KY, RK).
Ethics Approval and Consent to Participate
This research received approval from Juntendo University Hospital Institutional Review Board (E23-0046-H01). All participants provided written informed consent prior to participating.
Consent for Publication
Not applicable.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.