
Abstract
Objective:
To identify and analyze antibiotics’ prescription patterns and associated factors among terminally ill patients at a hospital in southern Peru.
Methodology:
A cross-sectional analytical study was conducted on adult patients who died in Hospital III Daniel Alcides Carrion in Tacna, Peru, 2023. Data were collected from electronic medical records, focusing on antibiotic use during the last hospitalization. Univariate, bivariate, and multivariate analyses were performed using Poisson regression to adjust for potential confounders.
Results:
The study included 239 patients with an average age of 76. Antibiotics were administered to 93.72% of patients, with 42.46% lacking an identified infectious focus. Ceftriaxone, Meropenem, and Vancomycin were the most used antibiotics. A lower use of antibiotics within 72 hours prior to death was associated with hospitalizations longer than 18 days and having 2 or more comorbidities.
Conclusion:
The high prevalence of antibiotic use at the end of life, often without an infectious focus, suggests a need for better guidelines and education on palliative care to avoid inappropriate antibiotic prescribing. Improved communication between healthcare providers, patients, and families is essential for optimizing end-of-life care.
Introduction
Although the effectiveness of antibiotic therapy at the end of life is often questioned, it continues to be a mainstay practice in hospital care.1-3 This indication aims to alleviate patient’s symptoms derived from infectious diseases. However, terminally ill patients derive little to no benefit from these interventions. 4 Since infections may not be the primary cause of health deterioration in this phase, the focus should be palliative care and pain relief rather than futile treatments.
Moreover, inappropriate antibiotic use at this stage can lead to further complications. 4 Antibiotic resistance is an escalating global concern, and the excessive prescription of antibiotics to patients who derive no benefit from them can exacerbate this issue. 5 Additionally, side effects such as allergic reactions, gastrointestinal issues, and potential interactions with other palliative medications can worsen patients’ conditions, making their final days less comfortable.
Understanding antibiotic prescribing patterns is essential for enhancing medical practices and care for terminally ill patients. Previous studies indicate that antibiotic prescriptions are prevalent among these patients. A systematic review and meta-analysis that included observational studies from 2000 to 2019 found that terminally ill patients who did not receive palliative care were 50% more likely to be prescribed antibiotics. 6 There is a lack of consensus regarding the benefits of antibiotics in this stage of life. While some physicians routinely prescribe antibiotics, others are more selective, resulting in a variability in clinical practice that requires further investigation and standardization. 7 This variability highlights the need for a deeper evaluation to determine when and how antibiotics should be used in palliative care.
Despite the high frequency of antibiotic prescriptions at the end of life, there is a lack of specific data on this practice in hospitals in less-studied regions, such as in low- and middle-income countries. Additionally, the factors associated with these prescriptions are not well-documented in this context. Lacking a clear understanding of the patterns and factors influencing antibiotic prescriptions, it is difficult to establish appropriate guidelines to optimize their use in terminally ill patients. Thus, this study aims to identify and analyze the prescription patterns and associated factors for antibiotics among terminally ill patients at a hospital in southern Peru.
Methods and Materials
Study design and population
A cross-sectional analytical study was conducted by collecting data from adult patients (over 18 years old) who died while hospitalized in Hospital III Daniel Alcides Carrión in Tacna, Peru, during the year 2023. This hospital is a third-level referral center for the three primary care centers that make up the city of Tacna. It also has 110 hospitalization beds and 28 beds in the Intensive Care Unit.
Cases were eligible if: (1) The patient died during the year 2023, (2) They were hospitalized in the services of Internal Medicine, Surgery, Gynecology, Intensive Care Unit, or Emergency. Cases with incomplete medical records were excluded from the analysis.
Procedure
After receiving authorization from the institutional research ethics committee of the Faculty of Health Sciences at the Private University of Tacna, the principal investigator (BMC) requested the death records for the year 2023 from the hospital’s epidemiology section. Once access to the electronic medical record system was obtained through the EsSalud Intelligent Health Service (ESSI), two researchers (BMC and AFY) independently extracted the study variables into a Microsoft Excel file (v.2017). Each extraction was then compared to ensure there were no errors in data transcription. Any discrepancies were resolved with the intervention of a third researcher (MHZ), who specializes in Infectious Medicine and tropical diseases.
Variables
The dependent variable was antibiotic use within 72 hours before death (yes/no). Antibiotic use was considered from the first administration regardless of the duration (one or more days) during the last hospitalization before the patient’s death. This methodology was similar to that of Cruellas et al. 8 The decision to use this cutoff point was made by consensus among the authors.
Independent variables were selected based on the researchers’ experience and after a comprehensive literature review. These were: (1) Age, coded as a continuous variable and then categorized into tertiles. This categorization of age into tertiles was made to reduce variability in the sample; (2) Gender; (3) Duration of the last hospitalization in days; (4) Acute resuscitation plan, which includes maneuvers such as cardiopulmonary resuscitation and the use of vasopressor medications (adrenaline, noradrenaline, dopamine) in response to significant clinical deterioration; (5) Comorbidities, classified as none, one, or two or more, as well as the type of comorbidities: Type 2 Diabetes Mellitus, Hypertension, Chronic Kidney Disease, and Malignancy; (6) If the patient had previously received palliative care, which was categorized as yes/no, information verified in the medical history upon admission, and reviewed during all consultations during their last hospital stay; (7) The variable “infectious focus” was also collected, identifying whether it was urinary, pulmonary, skin and soft tissue, abdominal, or if there was no evidence of an infectious focus. The definition of an infectious focus was determined retrospectively by reviewing the patient’s medical records and followed the following considerations: signs and symptoms suggestive of infection, elevated acute-phase reactants (C-reactive protein, leukocytosis, procalcitonin), and imaging studies suggesting an infectious focus (X-ray, CT scan, or MRI). 9 Additionally, it was evaluated whether there was any microbiological isolation (urine culture, blood culture, secretion culture). This analysis was conducted by a specialist in infectious diseases.
Other variables included were instability upon admission evidenced using vasopressors, the cause of hospitalization, the department of origin, the timing of death (before or after 48 hours from admission), and the number of hospitalizations during the last year before the current admission.
Statistical analysis
In the univariate analysis, categorical variables were presented as absolute numbers and their frequencies. Depending on their distribution, numerical variables were described using measures of central tendency (median) and dispersion (interquartile range). In the multivariate analysis, Poisson regression with robust variance was used to adjust for potential confounders and explore the variables that influenced the dependent variable of interest, “use of antibiotics within 72 hours before death (yes/no).” Variables with a P < .05 in the crude model were included in the adjusted model. All analyses were performed using Stata V17 software.
Ethical considerations
This study aligned with the international standards set forth by the Declaration of Helsinki. It was authorized by the institutional research ethics committee of the Faculty of Health Sciences at the Private University of Tacna on January 15, 2024, under the identification code FACSA-CEI/XXX-2024. The confidentiality of the extracted data was maintained. Due to the observational and retrospective nature of the study, informed consent was not requested.
Results
Table 1 describes the general characteristics of the patients. The median age of the participants was 76 years (IQR [Interquartile Range] from 66 to 84). There were 131 male patients, representing 54.8%. The median hospitalization time was 9 days (IQR from 4 to 17), and 65 patients (27.2%) underwent an acute resuscitation plan. It was observed that 58.2% of the patients had 2 or more comorbidities, with hypertension (34.3%), chronic kidney disease (27.6%), and neoplasms (31.8%) being the most common. Only 5 patients (2.1%) had received palliative care before hospitalization.
Sociodemographic characteristics in the studied population (n = 239).

Median (Interquartile Range).
Table 2 shows the clinical characteristics of the patients. The most common infectious focus was pulmonary (n = 83, 34.7%), followed by gastrointestinal (n = 26, 10.9%) and urinary (n = 18, 7.5%). However, most (n = 101, 42.3%) did not present any infectious focus. Almost all patients (n = 224, 93.7%) received at least one antibiotic. The main cause of hospitalization was the decompensation of a previous illness (n = 113, 47.5%), followed by sepsis (n = 81, 34.0%). As for the history of hospitalizations, most patients (n = 151, 63.2%) had no hospitalizations in the last year.
Clinical variables of the studied population (n = 239).

Table 3 describes the characteristics of the antibiotics administered to the patients. Within the cephalosporin group, the most used antibiotic was Ceftriaxone (61.5%), with significant use across all infectious focus. Cefepime was second and most used in patients with a pulmonary focus. Meropenem was the most prescribed carbapenem used in 62.8% of the patients. Piperacillin/tazobactam was particularly used in patients with a pulmonary focus, representing 46% of its use. Ciprofloxacin was most frequently used in patients with a pulmonary focus, accounting for 39.1% of its total use. Other heavily used antibiotics were vancomycin (55.2%) and metronidazole (13.0%).
Characteristics of antibiotics used in the studied population (n = 239).

Some patients used more than 1 antimicrobial.
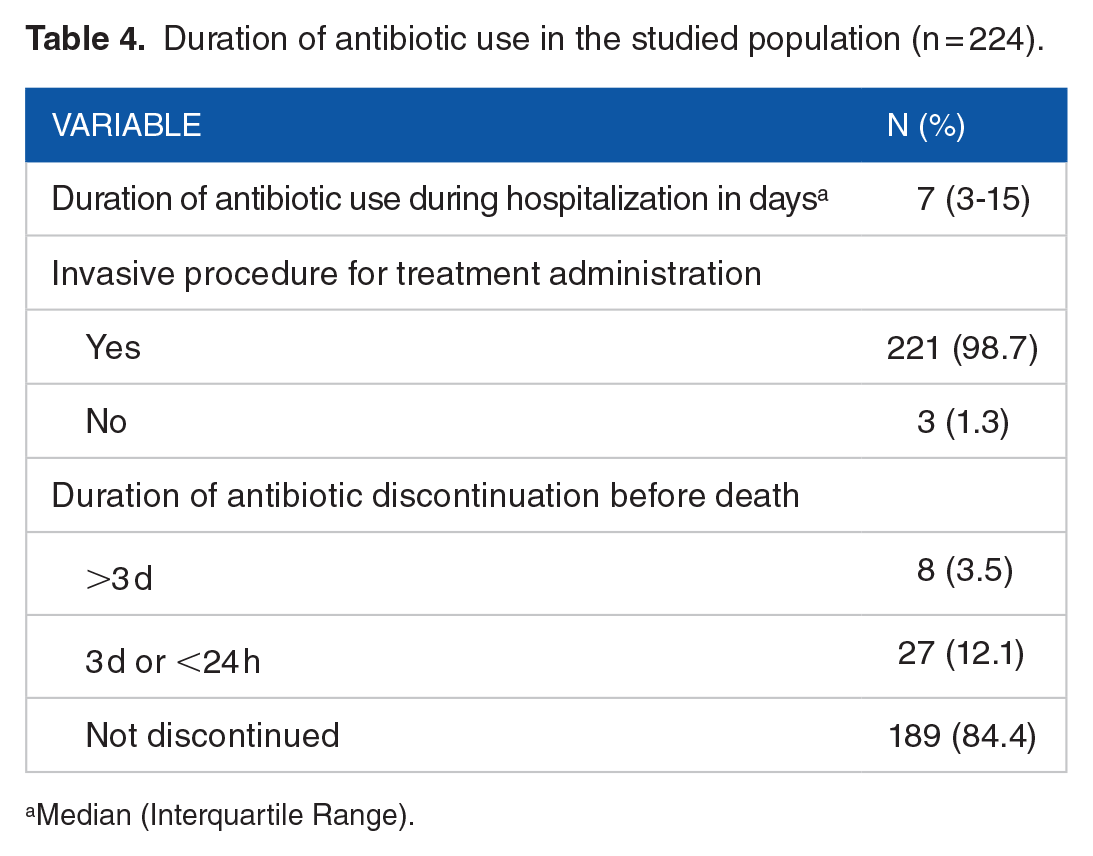
Table 4 describes the duration of antibiotic use in the population. The median duration of antibiotic use was 7 days (IQR from 3 to 15 days). It was observed that 96.5% of patients continued antibiotics until their demise, while only 3.5% discontinued antibiotics 3 days before death.
Duration of antibiotic use in the studied population (n = 224).
Median (Interquartile Range).
Table 5 shows the factors associated with receiving antibiotics within 72 hours before death. Patients with 18 or more days of hospitalization were less likely to receive antibiotics 72 hours before death compared to those with 1 to 7 days (PR: 0.91; 95% CI: 0.85-0.98). Regarding comorbidities, having two or more comorbidities was associated with a lower use of antibiotics 72 hours prior to death compared to having no comorbidities (PR: 0.93; 95% CI: 0.85-0.98).
Factors associated with the use of antibiotics within 72 hours before death (n = 224).

Simple Poisson regression with robust variance.
Multiple Poisson regression with robust variance, a model was generated with the variables hospitalization time in tertiles, number of comorbidities, hypertension, and diabetes mellitus type 2.
Discussion
Summary of findings
We conducted a cross-sectional analytical study on 239 patients who died in 2023 to examine antibiotic use patterns. Our main findings are as follows: (1) 93.7% of the patients received antibiotics during their final hospitalization before dying. (2) No infectious focus was confirmed in 42.5% of these cases. (3) Ceftriaxone, Meropenem, and Vancomycin were the most frequently used antibiotics. (4) Having 18 or more days of hospitalization, having a comorbidity, as well as not having hypertension or type 2 diabetes mellitus, were associated with a lower probability of receiving antibiotics within 72 hours before death.
Interpretation of findings
Our study reveals a significant prevalence of antibiotic use among terminally ill patients, with 93.7% receiving at least one antibiotic during their hospital stay. In 81.5% of the cases, antibiotic treatment continued until the patient’s death. Additionally, it is concerning that in 42.3% of the cases, no infectious focus was identified to justify their use. Similar results have been reported in various studies conducted between 2015 and 2019. The first study, conducted in Australia on 137 deceased patients, showed that 63.0% received antibiotics until their death, and in 37.2% of the cases, no infectious focus was detected. 10 The second study, conducted on 101 oncology patients, found that 6 out of 10 patients received antibiotics upon admission, 92% received them during their last 7 days of life, and no clear infectious focus was identified in 49.0% of cases. 8
Despite differences in healthcare systems and the availability of diagnostic and therapeutic resources in other countries, our findings reveal an alarmingly similar pattern. A study conducted in Brazil in 2016 also reported that a longer time since a physician’s graduation is associated with the inappropriate continuation of antibiotic therapy. 11 This suggests a global trend in inappropriate antibiotic prescribing practices during the final days of patients’ lives. Several factors could influence this trend, including the pressure to “do something” for the patient and their families, the preventive use of antibiotics against opportunistic infections in immunocompromised patients, an aversion to risk to avoid adverse outcomes, and insufficient training in palliative care. 7 These findings indicate that physician experience and ongoing education may also be critical factors.
The most common antibiotics prescribed in our study were ceftriaxone, meropenem, and vancomycin. These findings contrast with those reported in other studies. The first, conducted in Spain in 2019, found higher prescriptions of amoxicillin-clavulanic acid, piperacillin-tazobactam, ceftriaxone, and levofloxacin. 8 Two studies conducted in the United States at different hospitals in 2004 and 2007 highlighted different prescribing patterns. The first study noted a higher use of fluoroquinolones and macrolides, 12 and the other study reported a higher use of vancomycin and piperacillin/tazobactam. 13 Finally, a study conducted in Germany in 2015 identified piperacillin-tazobactam and ceftriaxone as the most commonly used antibiotics. 10 The variability in antibiotic prescribing patterns could be associated with differences in patient’s clinical conditions and the specific practices of each hospital or country. However, it is important to highlight that both ceftriaxone and vancomycin are consistently mentioned as frequently prescribed antibiotics in various studies. This is in accordance with a systematic review conducted in Africa, citing studies from 2010 to 2020, which reported that ceftriaxone was inappropriately indicated in more than 50% of cases. 14 Additionally, the widespread use of vancomycin is especially notable given the significant efforts to restrict its misuse and combat bacterial resistance in pathogens such as Enterococcus and Staphylococcus aureus. 15
Albeit beyond the primary question, one striking and concerning finding was that only 2.1% of the patients who died had previously received palliative care. This low prevalence of palliative care utilization suggests a limited medical culture regarding the early implementation of these specialized care services. 11 It could further explain the high prevalence rate of antibiotic prescriptions. Therefore, it is essential to identify patients who could benefit from palliative care early to avoid prolonging life at the expense of poor quality of life and increased healthcare costs.
Regarding associated factors, our study found that a hospitalization of more than 18 days, as well as having 2 or more comorbidities, were linked to a lower probability of receiving antibiotics within 72 hours before death. Up to the time of conducting this work, we have not found studies that have associated these variables with the use of antibiotics at the end of life. However, we can infer that our results could be due to the fact that a prolonged hospitalization might have completed various cycles of antibiotics, eliminating the need to continue them. Regarding patients with 2 or more comorbidities and their relation to the lower use of antibiotics, this scenario could be due to the limitation of therapeutic efforts because of the complexity of their pathological condition. We believe that a good ethical question to investigate would be at what point the treatment becomes futile and an unnecessary expense, rather than attempting to achieve the medical objective that we might aim to reach in a human being. In contrast to our results, a study in Portugal in 2017, when associating other variables, identified a significant association with the presence of fever and elevated C-reactive protein levels. 16 It is important to note that few studies have investigated how the patient’s functional status affects antibiotic prescribing, generally because it is considered that the patient’s general condition and sociodemographic characteristics do not directly influence these medical decisions. Additionally, a controversial study indicated that withholding antibiotics from patients in poorer general conditions did not affect their survival rates compared to those who received antibiotics. 17
Limitations
The study presents several important limitations. First, the results may not represent other regions because they include only patients from a specific hospital in southern Peru, limiting their generalizability. Secondly, the retrospective nature of the study may introduce selection and information biases, which could limit the analysis performed on the “infectious focus” variable, as it was defined solely based on information recorded in the medical records. Third, the low prevalence of prior palliative care may influence the decision to prescribe antibiotics, and the variability in clinical practice among physicians is not fully explored. Fourth, is the lack of a statistical power analysis. Although a census sample was conducted, which theoretically covers the entire target population and could be considered exhaustive, this analysis was not performed. It is essential to determine if the sample size is adequate to identify statistically significant effects, an omission that could impact the ability to generalize the results.
Conclusions
In conclusion, the use of antibiotics in end-of-life patients presents significant ethical and clinical challenges. Our findings indicate that nearly half of the deceased patients who received antibiotics had no identifiable infection source. Additionally, prolonged hospitalization (more than 18 days), as well as not having type 2 diabetes mellitus or hypertension, was associated with a lower probability of receiving antibiotics within 72 hours before death. It is important to address these issues since the misuse of antibiotics leads to increased healthcare costs and contributes to the broader problem of bacterial resistance.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was self-funded by the authors.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Ethical Considerations
This study aligned with the international standards set forth by the Declaration of Helsinki. It was authorized by the institutional research ethics committee of the Faculty of Health Sciences at the Private University of Tacna on January 15, 2024, under the identification code FACSA-CEI/023-01-2024. The confidentiality of the extracted data was maintained. Due to the observational and retrospective nature of the study, informed consent was not requested.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.