
Abstract
The COVID-19 pandemic had profound effects on the long-term care (LTC) setting worldwide, including changes in admission practices. We aimed to describe the characteristics and medical complexity of newly admitted LTC residents before (March 1, 2019 to February 29, 2020) and during (March 1, 2020 to March 31, 2021) the COVID-19 pandemic via a population-based serial cross-sectional study in Ontario, Alberta, and British Columbia, Canada. With data from the Minimum Data Set 2.0 we characterize the medical complexity of newly admitted LTC residents via the Geriatric 5Ms framework (mind, mobility, medication, multicomplexity, matters most) through descriptive statistics (counts, percentages), stratified by pandemic wave, month, and province. We included 45 756 residents admitted in the year prior to and 35 744 during the first year of the pandemic. We found an increased proportion of residents with depression, requiring extensive assistance with activities of daily living, hip fractures, antipsychotic use, expected to live <6 months, with pneumonia, low social engagement, and admitted from acute care. Our study confirms an increase in medical complexity of residents admitted to LTC during the pandemic and can be used to plan services and interventions and as a baseline for continued monitoring in changes in population characteristics over time.
Introduction
The COVID-19 pandemic has had profound effects in the long-term care (LTC) settings worldwide, including changes in admission practices. 1 Within Canadian LTC homes, admission rates declined 40% during the first wave of the pandemic. 2 Some LTC homes closed to new admissions, particularly if they experienced an outbreak of the virus. 2 Homes with rooms that housed multiple residents restricted admission to limit the number of residents within a home to minimize the spread of the virus. 2
Fear of COVID-19 infection and negative perceptions of LTC are likely contributing factors to change in admission rates. 3 Frail LTC residents had a higher likelihood of developing severe COVID-19 illness, increasing their risk of death. 4 Indeed, in 12 OECD countries LTC residents were found to have a greater mortality rate from COVID-19 compared to community dwelling older adults. 5 By August 2020, 80% of COVID-19 deaths in Canada occurred in LTC residents. 2 Aside from increased virus-related mortality, the pandemic also highlighted ongoing concerns about staffing levels, quality of care, and proper management of LTC homes. 1 Many community-dwelling older adults shifted their preference to remaining at home out of fear of contracting COVID-19 or because of the concerns in LTC highlighted by the pandemic. 3
The settings from where LTC residents were admitted also changed throughout the pandemic. For example, the largest decrease in admission rates was seen from the community, where 58% fewer residents were admitted during the first wave of the pandemic compared to the same period in 2019. 2 In March 2020, admissions from hospital increased by 21%, likely as hospitals moved to free beds for those infected with COVID-19. 2 However, over the course of the first wave the number of residents admitted from hospital dropped by 18%. 2 Information regarding sources of admissions in subsequent waves and across different provinces of the pandemic is lacking.
Because of the observed changes in admission rates and sources during the pandemic, 2 the characteristics of newly admitted LTC residents likely changed. Older adults entering LTC during the pandemic were likely living with more medical complexity because they were coming from hospital after an acute event or were admitted from home near the end of life or because of caregiver distress. However, the change in characteristics of newly admitted LTC residents in Canada in relation to the pandemic has not been examined to date. Therefore, the purpose of this study is to describe the medical complexity of newly admitted LTC residents in 3 Canadian provinces (Ontario, Alberta, and British Columbia) before and during the COVID-19 pandemic. The results will allow for planning of services and resources and for future pandemics.
Methods
Data sources and variables
This is a population-based serial cross-sectional study using data from the Minimum Data Set (MDS) 2.0 from all LTC homes in Ontario, British Columbia, and Alberta. No data were available from the other provinces and territories at the time of analysis. The MDS 2.0 is a valid and reliable standardized comprehensive assessment completed by trained assessors for every resident within 14 days of admission into a LTC home.6,7 We included newly admitted residents between March 1st, 2019 and March 31st, 2021. We excluded residents who were admitted with an expected stay <90 days, as this population has different characteristics than those admitted with an expected long stay and far fewer residents were admitted with an expected short stay during the pandemic.
While there is no formal definition of medical complexity, 8 we used the Geriatrics 5Ms to guide a biopsychosocial conceptualization. 9 The Geriatrics 5Ms stand for Mind, Mobility, Medications, Multicomplexity, and Matters Most to Me 9 and our conceptualization of each of these constructs with variables available in the MDS 2.0 is described below.
We further identified where residents were admitted from: (1) Inpatient acute care; (2) Community: home care services, ambulatory health services, or private home; or (3) Other inpatient services: inpatient rehabilitation service (general or specialized), inpatient continuing care, inpatient psychiatry, or residential care. The first reported COVID-19 outbreak in Canada was March 5, 2020. 18 In several previous analyses, we have defined the pandemic period as beginning March 1, 2020.19-23Therefore, we defined the waves of the pandemic based on the weekly number of COVID-19 cases reported by the Government of Canada 24 : wave 1 from March 1, 2020 to June 30, 2020 and waves 2 and 3 overlapped from October 1, 2020 to March 31, 2021. July 1, 2020 to September 30, 2020 was defined as off-peak as COVID-19 cases in Canada decreased during this time. Waves 2 and 3 were merged as no true off-peak time could be distinguished between the 2 where cases dropped low enough to be considered no longer a wave.
Analysis strategy
To characterize the medical complexity of newly admitted LTC residents we used descriptive statistics (counts, percentages). We describe characteristics stratified by pre-pandemic (March 1, 2019 to February 29, 2020) and wave 1, off-peak, and wave 2 and 3 timepoints, and by province. To visualize differences across time and geographic location, we graphed select characteristics within the 5Ms model stratified by pandemic wave, month, and province. To further understand the population being admitted from these settings, we examined the proportion of residents with delirium, hip fracture, or end-stage disease or receiving hospice care stratified by practice setting and month. All statistical analyses were completed using SAS version 9.4 (SAS Institute Inc., Cary, NC). Ethical clearance was received from the Research Ethics Board at Dalhousie University (2022-6409).The Research Ethics Board approved that informed consent would not be obtained from participants in this study as it would be both impossible and impracticable to collect consent as described in the Tri-Council Policy Statement Section 5.5A and B. 25 The data are anonymized before researchers access them, and therefore cannot be linked to an individual to provide consent. Further, there are thousands of records collected in the database, many of which belong to LTC residents who would be deceased.
Results
There were 45 756 newly admitted residents in the year prior to the pandemic and 35 744 in the first year of the pandemic. Wave 1, off-peak, and waves 2 and 3 included 10 036, 8970, and 16 738 newly admitted residents, respectively. Table 1 provides the demographic characteristics of residents by pandemic wave.
Demographic characteristics of residents across pre-pandemic, wave 1, off-peak, and waves 2 and 3 by province.
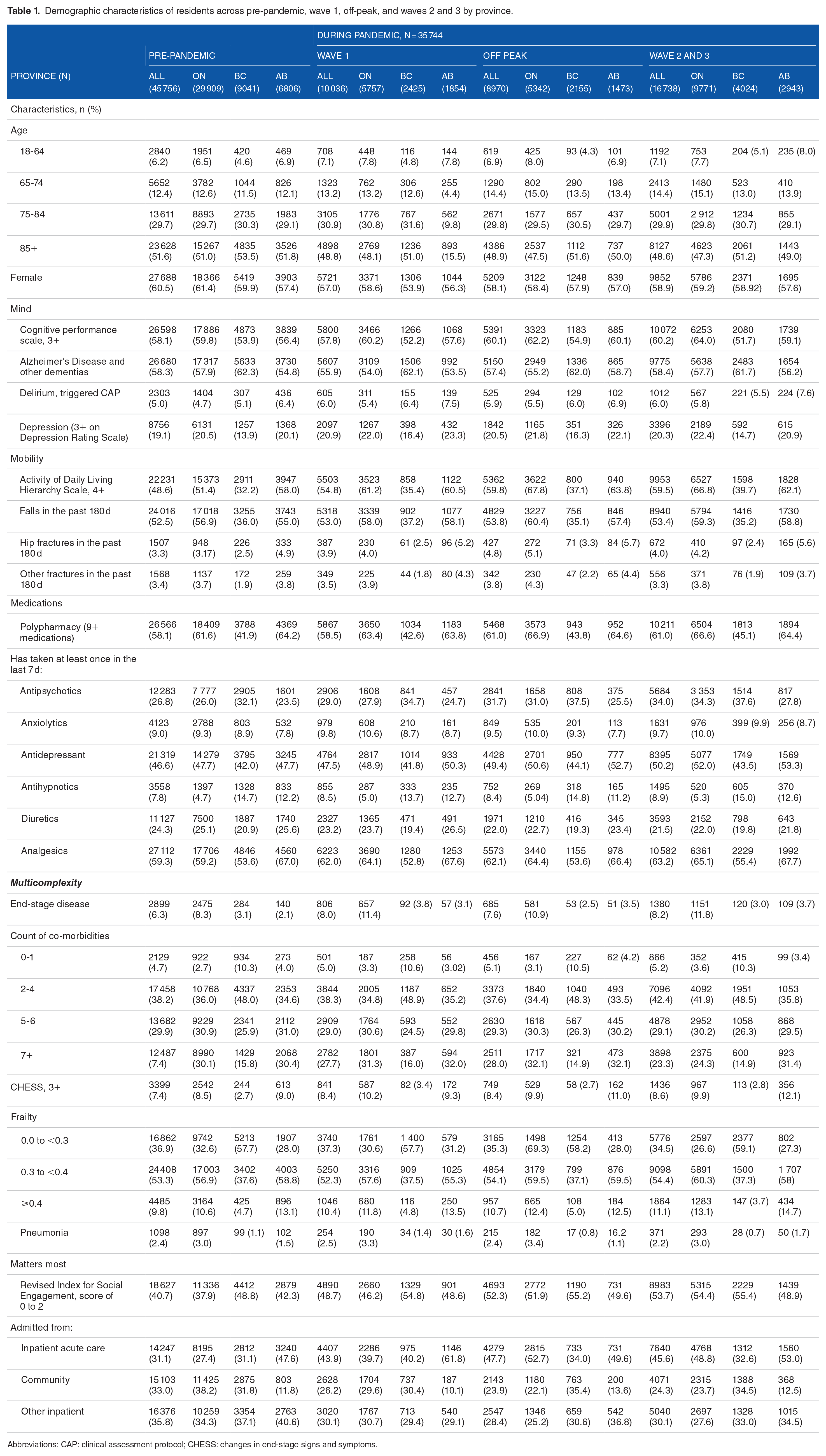
Abbreviations: CAP: clinical assessment protocol; CHESS: changes in end-stage signs and symptoms.
Mind (Figure 1)
Prior to the pandemic, approximately 5% of newly admitted residents in all 3 provinces displayed signs of delirium. During the first wave of the pandemic, all 3 provinces saw decreases in the proportion of new residents with indications of delirium with Ontario (1.8%), Alberta (2.5%), and British Columbia (3.7%) reaching their lowest proportions in May 2020. The proportion of residents with signs of delirium returned near 5% during the second and third waves in January 2021. In the analysis stratified by admission location (Figure 5), delirium rates decreased most in those admitted from the community and inpatient acute care, and remained mostly stable in those admitted from other inpatient settings during wave 1.
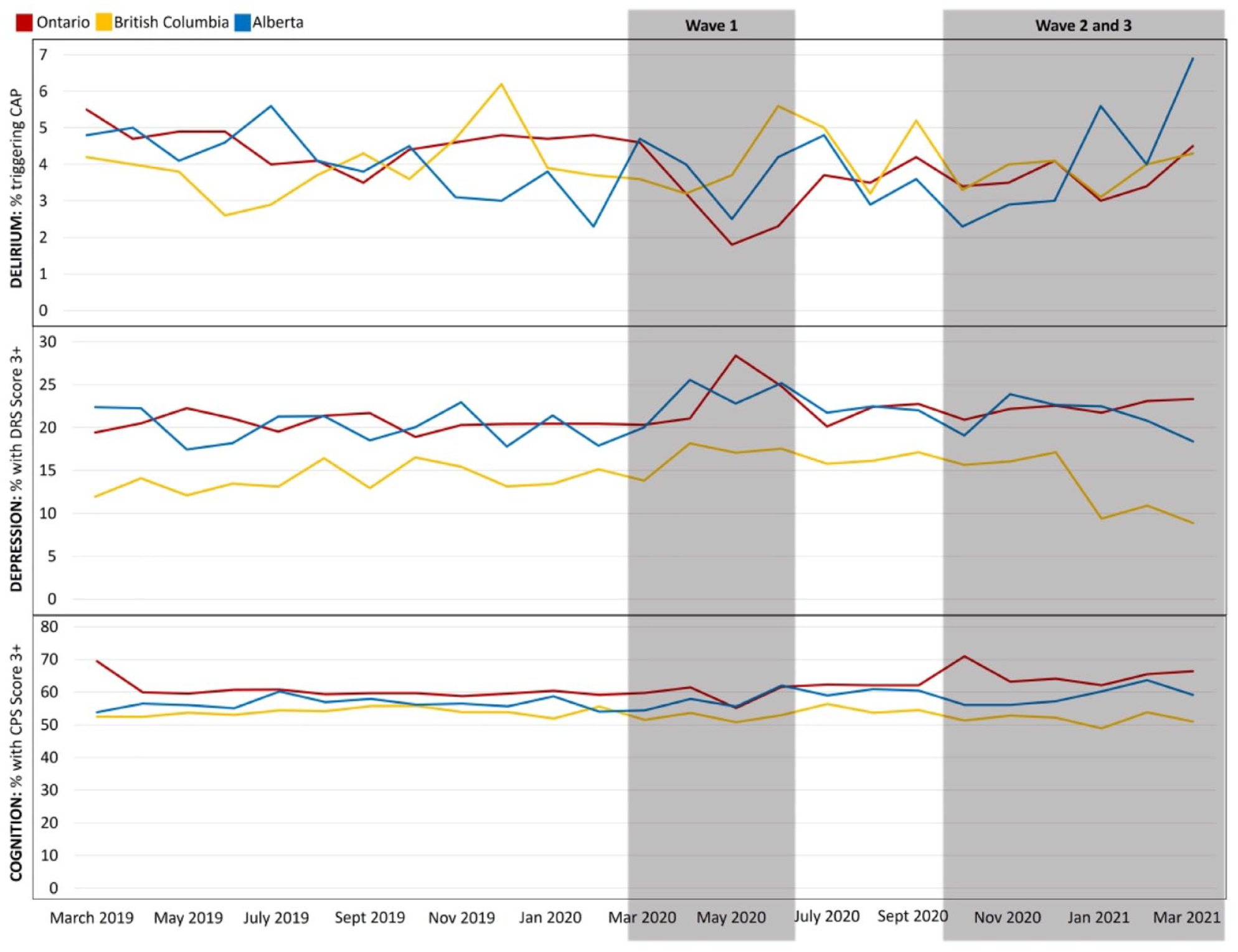
Mind: Delirium, depression, and cognition by province, month, and pandemic wave from March 2019 to March 2021.
The proportion of new residents with indications of depression increased across all 3 provinces during the first wave, with Ontario having the highest proportion of nearly 30% in May 2020, a 10% increase from pre-pandemic values. While the proportion decreased over off-peak and wave 2 and 3 in British Columbia and Alberta, it remained slightly elevated compared to the year prior to the pandemic in Ontario (20.5% pre-pandemic, 22.4% during off-peak and waves 2 and 3).
The proportion of newly admitted residents with moderate to severe cognitive impairment (CPS score 3+) remained stable over the first wave across the 3 provinces (Ontario 60.2%, British Columbia 52.2%, Alberta 57.6%). However, during wave 2 and 3 this proportion increased slightly in both Ontario (64.0%) and Alberta (59.1%) while remaining mostly stable in British Columbia (51.7%). The proportion of newly admitted residents with a diagnosis of Alzheimer’s Disease and other dementias remained largely unchanged across the 3 provinces during the pandemic, with a slight decrease in Ontario during wave 1 which returned to baseline in waves 2 and 3 (pre-pandemic: 57.9%, wave 1: 54.0%, waves 2 and 3: 57.7%).
Mobility (Figure 2)
There was a large increase in the proportion of new residents requiring moderate to extensive assistance with ADLs in Ontario during the first wave that persisted through off-peak and wave 2 and 3, from approximately 50% pre-pandemic to nearly 70% in April 2020. Similar patterns were observed in the other 2 provinces; however, the increases were not as dramatic with British Columbia increasing from approximately 30% to 40% and Alberta from approximately 60% to 65%.

Mobility: Activities of daily living, fractures, and falls by province, month, and pandemic wave from March 2019 to March 2021.
Likewise, there was a large increase in the proportion of new residents who had experienced a hip fracture in the past 180 days in May 2020 in Ontario, increasing from pre-pandemic proportions of 3.2% to 6.9% in May 2020. These proportions remained higher than pre-pandemic proportions in off-peak (5.1%) and wave 2 and 3 (4.2%). Pre-pandemic, Alberta had on average a higher proportion (4.9%) of new residents who had experienced a hip fracture than Ontario and British Columbia. This proportion increased throughout wave 1, peaked in September 2020 (7.2%), and remained elevated compared to pre-pandemic during wave 2 and 3 (5.6%). While the proportion of new residents who had experienced a recent hip fracture in British Columbia (2.5%) was overall lower than Alberta and Ontario, this province also saw its highest peak in September 2020 (4.2%). The proportion of newly admitted residents who had fallen in the past 180 days remained stable across all provinces and waves of the pandemic at approximately 60% in Ontario and Alberta and 35% in British Columbia.
Multicomplexity (Figure 3)
Overall, the proportion of newly admitted residents in Ontario who were complex was much higher than those in British Columbia and Alberta regardless of timepoint. The proportion of new residents who were expected to live <6 months peaked for all 3 provinces during the first wave of the pandemic in May 2020 at 18.4%, 4.4%, and 6.4% in Ontario, British Columbia, and Alberta, respectively. This proportion remained elevated in Ontario and Alberta through off-peak (Ontario 10.9%, Alberta 3.5%) and wave 2 and 3 (Ontario 11.8%, Alberta 3.7%) but returned to pre-pandemic proportions in British Columbia (3.0%).
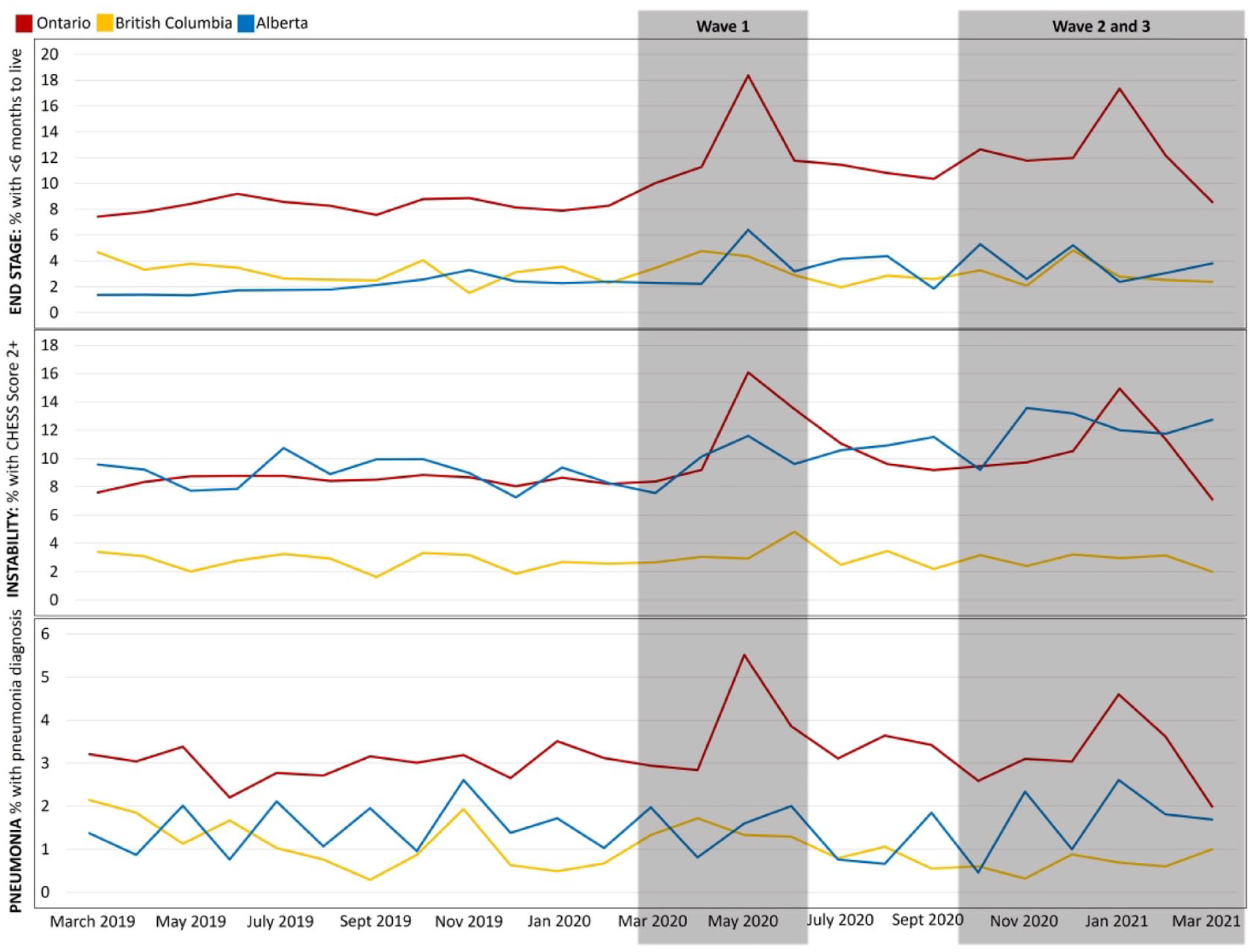
Multicomplexity: End-stage disease, health instability, and pneumonia by province, month, and pandemic wave from March 2019 to March 2021.
Health instability measured through CHESS remained virtually unchanged in Ontario and British Columbia from pre-pandemic to during the pandemic but increased in Alberta from 9.0% to 12.1%. The proportion of residents living with 7+ co-morbidities remained stable across the pandemic in Alberta (approximately 30%) and British Columbia (approximately 15%) and decreased in waves 2 and 3 in Ontario (pre-pandemic: 30.1%, waves 2 and 3: 24.3%). In contrast, the proportion of residents with FI of 0.4 or greater increased in Ontario from 10.6% pre-pandemic to 13.1% in waves 2 and 3, remained mostly unchanged in British Columbia, and increased by 1.6% in Alberta. Finally, the proportion with a diagnosis of pneumonia nearly doubled in Ontario from pre-pandemic proportions of 3.0% to 5.5% in May 2020 and peaked again in January 2021 at 4.5%. Proportions remained on average the same across pre-pandemic, waves 1, 2, and 3 in Alberta and British Columbia.
Medications (Figure 4)
The proportion of residents in Ontario on 9 or more medications increased 5% over pandemic from 61.6% pre-pandemic to 66.6% in waves 1 and 2. Likewise, the proportion increased in British Columbia from 41.9% to 45.1% but remained unchanged in Alberta (64.2% pre-pandemic to 64.4% in waves 2 and 3).

Medications, matters most, and admissions from hospital by province, month, and pandemic wave from March 2019 to March 2021.
The proportion of new residents who had taken an antipsychotic in the last week increased across all provinces through pandemic waves 1, 2, and 3, by approximately 8% in Ontario, 5% in British Columbia, and 4% in Alberta. Antidepressant and analgesic use increased by smaller proportions of 4.3% and 4.9% in Ontario, 1.5% and 1.8% in British Columbia, and 4.5% and 0.7% in Alberta, respectively. The proportion of new residents who had taken an anxiolytic, hypnotic, or diuretic increased <1% across the 3 provinces throughout the pandemic.
Matters most to me (Figure 4)
The proportion of newly admitted residents with low social engagement increased to around 50% in all 3 provinces during the pandemic, regardless of timepoint from pre-pandemic proportions of 37.9%, 48.8%, and 42.3% in Ontario, British Columbia, and Alberta, respectively.
Admission location (Figure 4)
In all 3 provinces admissions from inpatient acute care increased during waves 1, 2, and 3 and peaked in April 2020. Ontario saw the largest increase from 27.4% pre-pandemic to 58.6% in April 2020, while Alberta reached the highest overall proportion of 70% of newly admitted residents coming from inpatient acute care in April and May 2020, in comparison to 47.6% pre-pandemic. By March 2021, these proportions remained higher than pre-pandemic in both Ontario (45.3%) and Alberta (46.5%) but returned to near normal proportions in British Columbia (29.3%). The proportion of new residents admitted from the community decreased across the pandemic in Ontario from 38.2% pre-pandemic to 23.7% in waves 2 and 3. However, in British Columbia and Alberta this proportion remained relatively unchanged. The proportion of new residents admitted from other inpatient settings decreased across all 3 provinces across the pandemic, ranging from a 7% decrease in Ontario to a 4% decrease in British Columbia.
In the analysis stratified by practice setting across all provinces (Figure 5), the proportion of newly admitted residents from the community who had experienced a hip fracture in the past 180 days more than doubled, increasing from approximately 1.5% in 2019 to 3.7% in May 2020, while proportions remained largely unchanged in those admitted from inpatient acute care or other inpatient services. This proportion returned to pre-pandemic levels in the community by March 2021. Likewise, the proportion of newly admitted residents from the community with end-stage disease more than doubled, increasing from approximately 4% in 2019 to 9.4% in May 2020. In contrast, the proportion of newly admitted residents from inpatient acute care with end-stage remained unchanged around 10% until Wave 2 and 3 when it increased to 14.5%.

Fractures, delirium, and end-stage disease by admission setting from March 2019 to March 2021.
Discussion
Our serial cross-sectional study found that residents admitted to LTC during the pandemic were generally more medically complex than prior, but differences varied across provinces and pandemic waves. The most striking differences were observed in the increase in residents admitted from hospital, who had signs of delirium, severe functional impairment, had recently had a hip fracture, or were expected to live <6 months.
In our study approximately 10 000 fewer residents were admitted to LTC across all 3 provinces during the first year of the pandemic than in the year prior. Our results are in line with previous work conducted across Canada (Newfoundland and Labrador, Nova Scotia, Ontario, Manitoba, Alberta, British Columbia, and the Yukon) that found a 40% decrease in admissions between March 1 and August 31, 2020 and the same period in 2019. 2 Likewise, another study found an 18% decrease in residents admitted to LTC in Ontario during March 2020 to March 2021. 19 Similar to our results, the largest decrease in both studies was observed in admissions from the community which was hypothesized to be a result of altered admission practices to limit infection spread, or because older adults and their families were more reluctant to choose LTC admission because of the sector’s challenges with the pandemic.2,19
While the absolute number of newly admitted residents with delirium was similar pre- and during the pandemic, the proportion of residents was lower during the pandemic, particularly the first wave. These results are similar to previous work done on a smaller scale in 7 LTC homes in New Brunswick, Canada, where LTC residents with dementia were less likely to experience delirium during the first wave. 26 The mechanism behind the decrease in delirium prevalence is unknown as little work has been done to date examining the prevalence of delirium in LTC during the pandemic. However, it may be related to a calmer environment within the LTC home with fewer people moving around throughout the building. A higher number of precipitating factors, such as noisy or busy environments, infection, or medication changes, increases the risk for delirium development. 27 Thus, a quieter environment may decrease the risk. In contrast, the decrease may reflect an underestimate of the true prevalence of delirium if LTC staff were not able to observe residents for signs of delirium because of understaffing during the pandemic. Further work is needed to understand the reasons behind a decrease in the proportion of newly admitted residents with delirium.
Likewise, the absolute number of newly admitted residents with fractures prior to and during the pandemic were similar. However, there was an increased proportion of residents with fractures prior to admission during the pandemic where a higher proportion of those admitted from the community had recently experienced a fracture. This may be a byproduct of inpatient settings discharging patients (eg, inpatient post-acute rehabilitation) to clear beds in anticipation of increased COVID-19 admissions, and instead admitting residents to LTC. Further, the post-fracture care received in hospital during the pandemic may have been different. For example, Hadfield and Gray 28 found that patients treated in COVID-19 positive wards received less specialist input and reduced surgical specialty review during the pandemic, increasing mortality and complication rates post hip fracture. Likewise, Pereira et al 29 reported hospital mobility was at an all-time low during the pandemic. Therefore, residents admitted to LTC from hospital may have been more deconditioned during the pandemic and subsequently requiring more assistance with ADLs.
The increase in the proportion of residents being admitted to LTC having taken antipsychotic medication across all provinces and time periods during the pandemic is potentially worrisome. Significant work has been done nationally to decrease inappropriate use of antipsychotic medications in LTC 30 and the incremental increases observed in our work could be indications of a threat to this work. Other authors have found similar increases in the use of antipsychotics in LTC during the pandemic.19,31 However, our work is specific to newly admitted residents, indicating LTC staff may be faced with discontinuing inappropriate antipsychotics for newly admitted residents.
The observed increase in new residents at end of life could be a result of admissions from hospital of seriously ill older adults or increased crisis placements from the community. Indeed, we found an increased proportion of residents admitted from the community who were at end of life during the first wave of the pandemic. The increase in the proportion of new residents with pneumonia may reflect COVID-19 cases. Symptomology between pneumonia and COVID-19 are similar and often hard to distinguish, 32 and accuracy of diagnostic tools varies widely. 33 Further, there is no diagnosis variable for COVID-19 in the MDS 2.0 so residents may have been classified with pneumonia instead. LTC homes require significant resources and skilled workers to support chronic disease management of residents living with multicomplexity and good palliative care, 34 and this need has increased across the pandemic.
There are several potential explanations for the observed variation in our results across provinces. First, the total number of cases and rates of cases of COVID-19 varied across provinces: during the peak of wave 1 in May 2020 Ontario had a rate of 171.8 COVID-19 cases per 100 000 individuals while BC and Alberta had rates of 47.3 and 149.1, respectively. 24 Further, the proportion of these cases that were in LTC varied across provinces: during the first wave 20% of all COVID-19 cases in Ontario were in LTC, while this was 7% and 10% in Alberta and BC, respectively. 35 Second, provinces deployed resources and implemented different policies at different time points throughout the pandemic. For example, Alberta limited visitors in LTC homes to one essential visitor on March 16, 2020 while Ontario and BC restricted all visitors on the same day. 36 These 2 regional differences could alter the effect of the pandemic on admission practices and characteristics of admitted residents as the homes dealt with the changing landscape of the pandemic around them. Finally, there were differences in the LTC population across Canada prior to the pandemic 37 which could also explain some of the observed variation. For example, the proportion of residents with end-stage disease was much higher in Ontario than British Columbia and Alberta prior to the pandemic. Thus, factors external and prior to the pandemic may also explain the observed variation.
A strength of our study is our sample included the year prior to the pandemic for comparison of baseline characteristics. We were also able to stratify our results by pandemic wave and province, providing a fulsome picture of the change in newly admitted resident characteristics over the first year of the pandemic. A limitation of our work is that it is descriptive in nature, and we could not examine associations between service provision and changing characteristics. Therefore, we cannot confirm the reasons for the observed changes. We did not complete a power analysis for sample size because we did not statistically test a hypothesis. However, we provide a baseline description of the population in LTC during the first year of the pandemic which can be used to understand the sector’s health needs. For example, we confirm that there was an increase in the proportion of residents entering a LTC home at end-of-life. This suggests that palliative care may be in higher demand and that policy makers and service providers should devote resources to these services. Further, we could not establish whether antipsychotic use was inappropriate. Finally, our study examined only 3 provinces thus results may not be generalizable across the country. Future studies should examine the association between changes in service provision in LTC during the pandemic and resident-level outcomes.
Conclusions
Our study confirms an increase in medical complexity of residents admitted to LTC during the pandemic. We observed a higher proportion of residents admitted to LTC during the pandemic were admitted from hospital, had severe functional impairment, had recently had a hip fracture, or were expected to live <6 months. Results can be used to plan services and interventions for the increasingly complex LTC population during the pandemic, and as a baseline for continued monitoring in changes in population characteristics over time.
Footnotes
Acknowledgements
None.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported in part by funding from the Government of Canada’s New Frontiers in Research Fund (NFRF; NFRFG-2020-00500) for collaboration in the EU Horizon 2020 research and innovation project Individualized CARE for Older Persons with Complex Chronic Conditions in Home Care and Nursing Homes (I-CARE4OLD, Grant Agreement No 965341). In addition, it received funding through the Canadian Institutes of Health Research (CIHR Reference # GA6-177780).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Brief Summary:
Long-term care residents admitted during the COVID-19 pandemic were more medically complex. Our results can be used to plan services and interventions and as a baseline for continued health status monitoring in this population.
Author Contributions
RA contributed to conceptualization and data analysis. JPH contributed to data curation, conceptualization, data analysis, and critical manuscript review. GH and LT contributed to conceptualization and critical manuscript review. CM contributed to conceptualization, data analysis, manuscript writing, and supervision.