
Abstract
Diabetes is a global public health issue. The Public Health Agency of Canada published a Diabetes Framework 2022 which recommends collaborative work across sectors to mitigate the impact of diabetes on health and quality of life. Since 2020, the INMED-COMMUNITY pathway has been implemented in Laval, Québec developing collaboration between healthcare and community sectors through a participatory action research approach. The aim of this article is to gain a better understanding of the INMED-COMMUNITY pathway implementation process, based on the mobilization of network actor theory. Qualitative analysis of semi-structured interviews conducted from January to March 2023 with 12 participants from 3 different sectors (community, health system, research), were carried out using actor-network theory. The results explored the conditions for effective intersectoral collaboration in a participatory action research approach to implement the INMED-COMMUNITY pathway. These were: (1) contextualization of the project, (2) a consultation approach involving various stakeholders, (3) creation of new partnerships, (4) presence of a project coordinator, and (5) mobilization of stakeholders around a common definition of diabetes. Mediation supported by a project coordinator contributed to the implementation of an intersectoral collaborative health intervention, largely due to early identification of controversies.
Introduction
The World Health Organization (WHO) recognizes diabetes as a major public health issue. 1 Diabetes is a widespread chronic disease in Canada which is primarily managed in primary care and integrated into chronic disease management.2-6 Over 3 million Canadians, or 8.9% of the adult population, have been diagnosed with diabetes; this is expected to increase by 12% by 2031. 7 This increase is due to an aging population and an increase in co-morbidity, leading to a significant rise in healthcare expenditure.8,9
Living with chronic disease requires flexible integrated care involving various and well-coordinated care and services, from prevention to end-of-life care.10-12 An intersectoral collaborative approach is fundamental to meeting ongoing needs and achieving this integrated care. 13 According to the Public Health Agency of Canada’s 2022-27 Framework, the management and control of diabetes in Canada requires intersectoral collaboration with stakeholders from public, private, and non-governmental sectors to ensure an inclusive and comprehensive perspective on the social determinants of health, as well as a person-centered approach. 9 Studies on intersectoral actions for people living with diabetes have pointed out how the implementation process can be effective, but few have looked into the impact of intersectoral collaboration on people health.14,15 Social support systems that focus on the complex empowerment processes of people living with chronic diseases can also reduce social inequalities and inequities and impact of diabetes on health. 9
Intersectoral collaboration is a well-established strategy for mitigating complex societal problems and addressing systemic changes.16,17 Intersectoral collaboration can create interconnectivity between different systems (health, socioeconomic, and environmental), to promote comprehensive interventions that address both individual needs and population health.18,19 Different intersectoral initiatives addressing the determinants of health can link public policy to better population outcomes. 20 The present study is based on the WHO definition of intersectoral collaboration in health stated in Nuthbeam and Muscat 21 : “intersectoral collaboration in health constitutes all actions undertaken by different sectors of society to achieve health outcomes in a more effective, efficient or sustainable manner than if one sector worked alone”.
Actor-network theory (ANT)
This study is based on the theoretical framework of actor-network theory (ANT). This theory was developed by sociologists Madelaine Akrich, Michel Callon, and Bruno Latour and recently adapted by Bilodeau and Potvin22-27 to empirically describe and analyze networked action in public health interventions. 28 This framework is adequate in an organizational context where multiple stakeholders from different sectors and social groups are brought together, form alliances and develop ways to act in a coordinated manner. 29 ANT conceptualizes networked action as a process involving human and non-human actors (eg, specialized knowledge, resources, technologies) linked by a problematic situation. 25 Consequently, ANT is used to better understand how sociotechnical networks produce change, 30 through creation, reconfiguration, and extension of the network in which new solutions emerge in response to a shared problematization. 26 Callon and Latour refer to this process as “translation.”22,25 According to Akrich et al and Bilodeau et al, “translation” is a process made up of 5 overlapping phases: contextualization, problematization, interessement, enrollment, and mobilization.23,26 Contextualization enables the effects of social innovations to be measured by the actors and their actions understood in context.31,32 Problematization leads actors to develop a shared vision, rallying them around a common interest. Interessement refers to actions to encourage new stakeholders to join a project, adhere to common goals, and participate in its realization. Enrollment refers to the negotiation and acceptance of new roles and mobilization refers to the effective realization of connections between actors who can act as spokespeople for the network and generate action.
INMED-COMMUNITY pathway
The INterprofessional Management and Education in Diabetes care (INMED) pathway 33 is an participatory action research (PAR)34,35 that emerged from the recommendations of Diabetes Canada 36 and the principles of the Revised Chronic Care Model 37 addressing people living with diabetes in Laval, Quebec. For its part, the INMED-COMMUNITY pathway focuses on development of intersectoral collaboration between the healthcare and community sectors to improve accessibility of community services for people living with diabetes.
The INMED-COMMUNITY pathway developed intersectoral links within a network of actors and complex actions. The 5 main aspects of ANT (contextualization, problematization, interessement, enrollment, and mobilization) were used to analyze the intersectoral collaboration of the INMED-COMMUNITY pathway: (1) restructuring (contextualization), (2) consultation approach (problematization), (3) creation of new partnerships (enrollment), (4) project coordination and joint definition of diabetes (interessement), and (5) alignment of actors, resources, and network support (mobilization). This analysis is based on the modeling of ANT and intersectoral collaboration by Bilodeau et al. 26
The aim of this article is to gain a better understanding of the INMED-COMMUNITY pathway implementation process, based on the mobilization of network-actor theory.
Method
Study estimate
The study is based on an analysis of the development of intersectoral collaboration between health and community sectors of people living with diabetes as part of intervention implementing the INMED-COMMUNITY pathway in Laval, Quebec. The team has been involved in a PAR 32 to facilitate the implementation of the INMED-COMMUNITY pathway in two university family medicine groups (U-FMGs) in the Laval region (Quebec) since April 2022. PAR is particularly appropriate for our research, as it relies on the involvement of health organization and community stakeholders at all stages of the research 38 and encourages action through the creation of spaces where stakeholders can identify needs and propose solutions.39,40 Actors involved in the INMED-COMMUNITY pathway are from health, community, and research sectors (Table 1). Since April 2022, stakeholders have been invited to participate in the process of implementing the INMED-COMMUNITY pathway through formal and informal weekly meetings led by the research team, and through committees whose frequency varied according to the project objectives to be achieved (monthly to quarterly).
Characteristics of professionals involved.

Recruiting participants
Qualitative exploratory research was conducted between January and March 2023 through semi-structured interviews with 12 participants from 3 different sectors (health, community, research) recruited using a purposive sampling process (Table 1).41-43 The criterion used for recruitment was to have participated in the implementation of the INMED-COMMUNITY pathway. This approach recorded the perspectives of different actors involved in the PAR intervention in the INMED-COMMUNITY pathway. Recruitment was done to represent all stakeholders that took part in the INMED-COMMUNITY pathway. Overall, 3 participants were from the community sector, including a patient-partner, a director of a local community organization and a community organizer. Two participants served as project coordinators working with the research team. Seven participants represented different stakeholders from the health sectors: 2 nurses, 4 health administrators and one quality improvement agent.
Study process (action/reflection cycles)
As described by Cargo and Mercer, 44 the PAR approach was based on 3-phase cycle systems: (1) analysis of the situation and the change to be achieved by the actors (research), (2) joint analysis of results and feedback, and (3) reflection on the results of data collection, planning and implementation of the change to be achieved (action). These phases were repeated over several cycles for each action that engaged stakeholders in the implementation of the INMED-COMMUNITY pathway.
The actions of the INMED-COMMUNITY pathway were determined in collaboration with all stakeholders and approved by the multisectoral representatives through an iterative process that followed 6 steps: (1) in June 2022, a brainstorming workshop was organized with all stakeholders so they could get to know each other, initiate collaborative links and clarify their service offers in order to become more familiar with the service offers available in the health and community sectors, (2) in July 2022, a “resource directory” was suggested by one of the patient partners, as a useful and relevant tool for monitoring people with diabetes. This suggestion was discussed and appreciated by the other stakeholders at a project meeting, who collectively adopted the idea and set up a “resource directory committee” to ensure co-creation of the “resource directory” and integration of all participants’ ideas, (3) in October 2022, a “self-care support guide” for people living with diabetes was discussed and adopted by all participants of the “resource directory committee” to better support people living with diabetes and self-managing the disease, (4) in August 2022, participants discussed the importance of creating a form to refer patients from the clinical sector to the community sector. This idea underwent several adjustments and was finally validated and adopted in September 2022 by all the participants, (5) in November 2022, an expanded working committee was created to reflect on the organizational anchoring of this project and the terms of commitment of all stakeholders in the sustainability and 6) in February 2023, a project for an intersectoral table committee emerged following a consultation of all stakeholders to contribute to the sustainability of the INMED-COMMUNITY pathway in the organization. These cycles enabled the gradual implementation of the INMED-COMMUNAUTE pathway, which is still ongoing.
Data collection strategy
A qualitative interview guide (Appendix 1) was developed based on actor-network theory. 26 Interviews lasting approximately 45 to 60 minutes, were conducted by 3 members of the research team via an online video conferencing platform, and then were transcribed. The research team members conducing the interview were distinct from the research coordinators interviewed for the study. Field notes were also taken at various meetings and project activities. The principal investigator (GL) kept a logbook to document her understanding of the phenomenon under study. The elements collected provided multiple data sources that were triangulated to reach data saturation. 45 Data saturation was obtained throughout the analysis as no new code emerged. 46
Analysis
A deductive and inductive qualitative thematic analysis 47 in double coding was carried out using NVivo software 48 and informed by the ANT framework.25-27 Five interviews were coded by 2 members of the research team, to create an initial code tree. A team meeting enabled the code tree to be adjusted based on the 5 main aspects of the ANT framework. The analysis of all interviews was then done by one of the team members (AT) using the agreed codebook. 49 Inductive coding continued after the initial codebook had been developed, and new codes emerged. Preliminary results from the data analysis were discussed in a team meeting to validate any adjustment needed. Data from the interviews were triangulated with field notes taken during meetings and committees with stakeholders and the logbook notes of the lead researcher (GL).
Ethical process and consent to participate
The organization’s ethics committee has given a favorable opinion on the original study (2020-602).
Results
Participant characteristics are presented in Table 1. Three participants were from the community (a patient, an executive director of a community organization and a community organizer), 4 were health system managers (primary care) and 4 were primary and specialized care professionals. Analysis of the qualitative results explored the conditions for achieving intersectoral collaboration in an actor-network theoretical approach for people living with diabetes by mobilizing the 5 main aspects of ANT.22-27 In addition, the implementation of the INMED-COMMUNITY pathway through PAR identified several elements that facilitate collaboration between people from different sectors (community and healthcare). In particular, the meetings held between all the participants from different sectors enabled them to listen to each other and adjust throughout the course of the research. Although people from the community were in minority, the stakeholders ensured that they were listened to and well represented during the meetings. These were grouped according to the 5 components of ANT: (1) restructuring (contextualization), (2) consultation approach (problematization), (3) creation of new partnerships (enrollment), (4) project coordination and common definition of diabetes (interessement), and (5) alignment of actors, resources, and network support (mobilization).
Contextualization
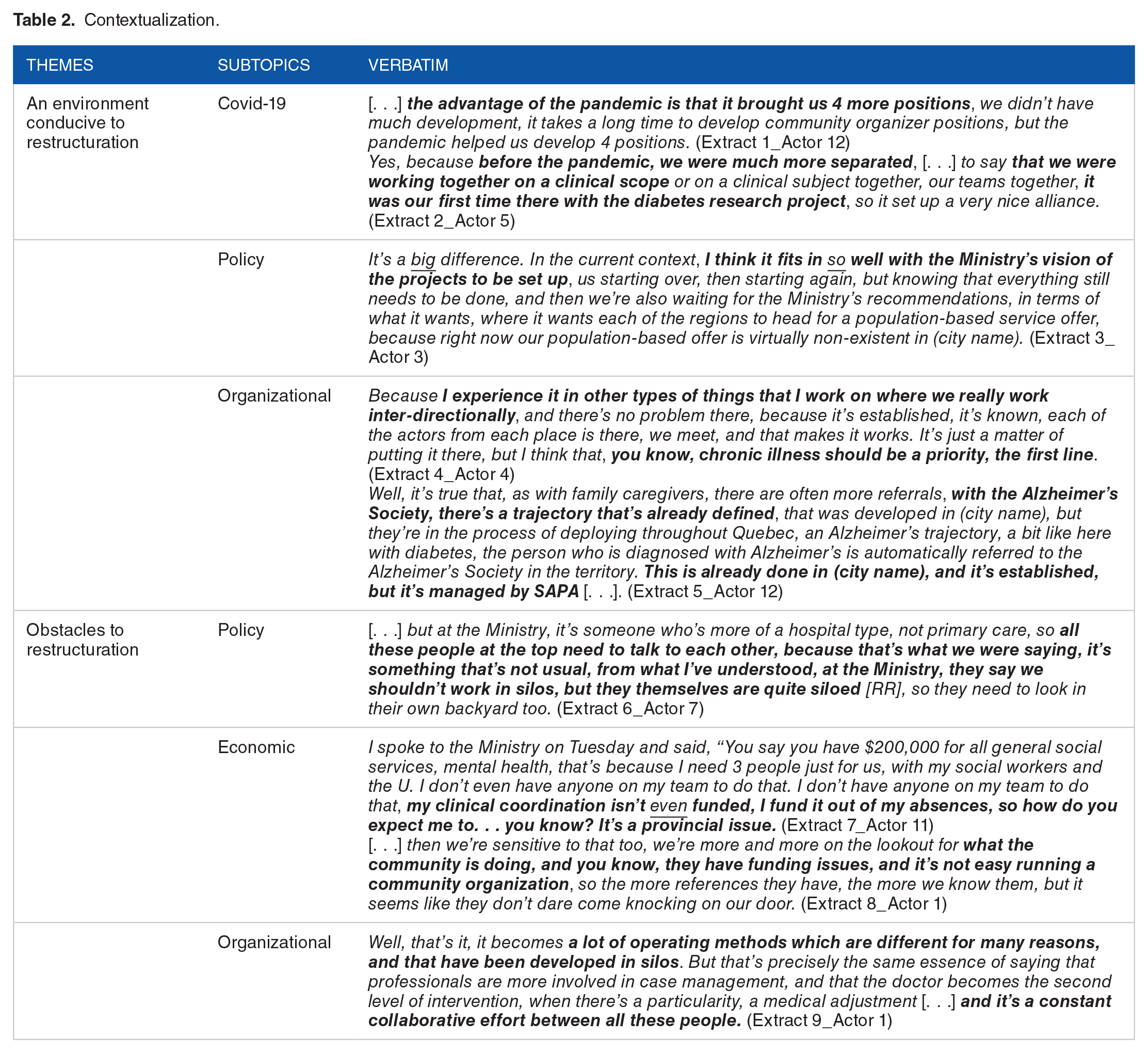
The results of the interviews demonstrate how participatory action research was conducive to the restructuring of each system involved. First, as one of the primary care managers mentioned, COVID-19 fostered teamwork and enabled the stakeholders to “work together on a common project” (Table 2, extract 2). Another primary care manager also mentioned that policies had been favorable to the development of the INMED-COMMUNITY pathway, given that this project “fits in” with current ministerial priorities (Table 2, extract 3). Finally, the community organizer mentioned the implementation of another trajectory project, which in their view facilitated the stakeholders’ adherence to the INMED-COMMUNITY pathway (Table 2, extract 5). On the other hand, the “siloed” organization of policies was perceived as a barrier to restructuring according to a specialized care nurse (Table 2, extracts 6 and 9). Moreover, according to a primary care professional, reduced funding for community organizations led them to reconsider their activities (Table 2, extracts 7 and 8). These results are corroborated by the field notes, which emphasize the collaboration between managers from different departments and sectors working together to overcome the difficulties of the COVID-19 context.
Contextualization.
The consultation approach
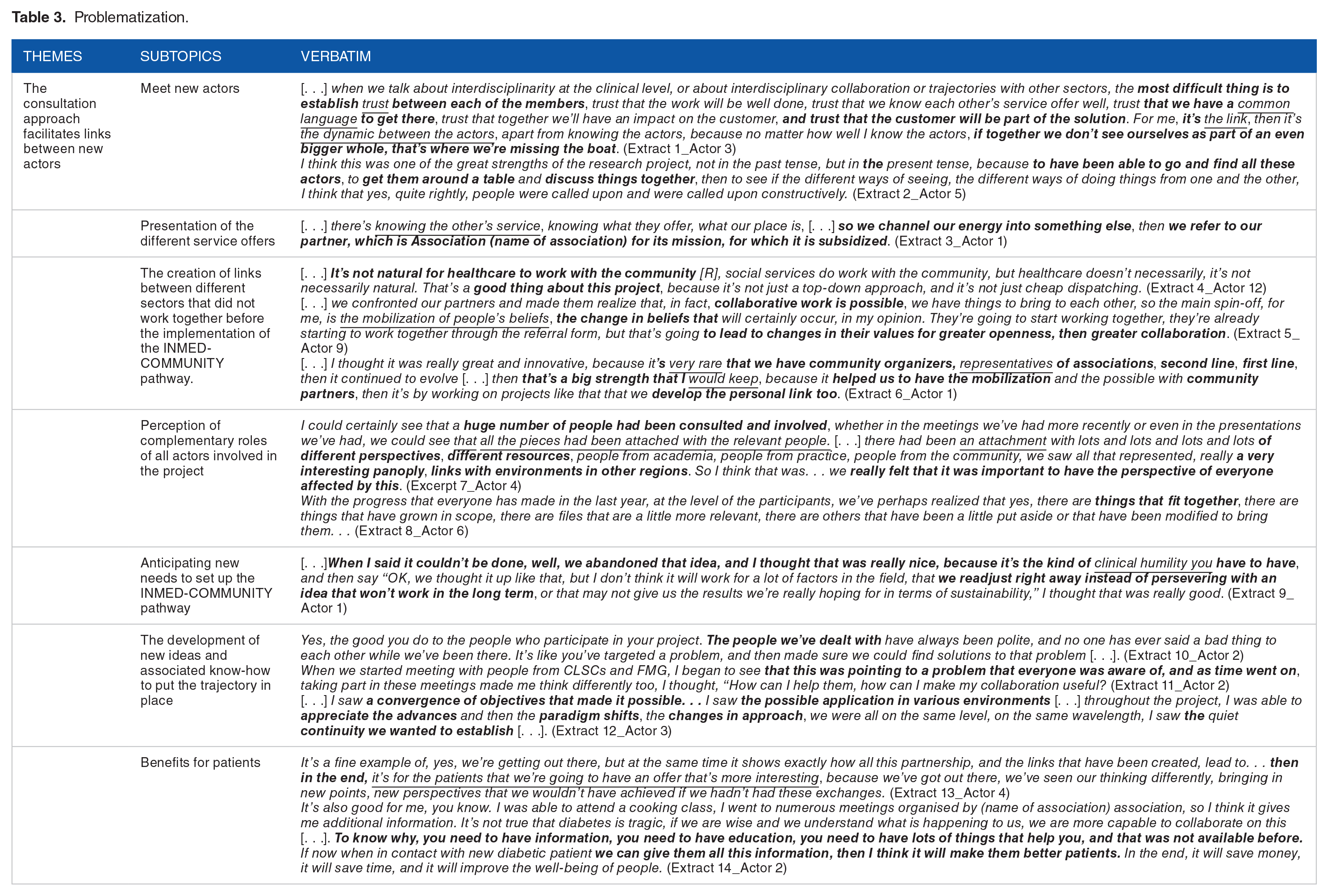
Results of the interviews show that consulting stakeholders through formal and informal meetings and committees helped create new links in the INMED-COMMUNITY pathway. The interviews and field notes highlight that the consultation approach facilitated: (1) meeting of new stakeholders, (2) presentation of different service offerings, (3) creation of links between different sectors that did not collaborate together before the implementation of the INMED-COMMUNITY pathway, (4) perception of the complementary roles of all stakeholders involved in the project, (5) anticipation of new needs to implement the INMED-COMMUNITY pathway, (6) development of new ideas and associated know-how to implement it, and (7) positive spin-offs for patients.
However, this consultation-based approach required favorable conditions to be operational and engage all stakeholders toward a common goal, as mentioned by several different types of participants (Table 3). One of the primary care managers mentioned the importance of “trust” and the adoption of a “common language” to be able to work together (Table 3, extract 1). One of the project coordinators also mentioned the importance of sharing common “values” and “changing the beliefs” of those involved to be able to mobilize them during consultations (Table 3, extract 5). These observations were supported by another manager and a primary care professional, who added that sharing values had required a certain “humility” on the part of the participants (Table 3, extract 9) and required questioning “relevance for patients,” to be able to adopt a common vision of the INMED-COMMUNITY pathway (Table 3, extract 13).
Problematization.
Creating new partnerships
The implementation of the INMED-COMMUNITY pathway has furthered the creation of several partnerships within the health sector (inter-directorate), with the health sector and the community sector (intersectoral), and between the INMED-COMMUNITY project team (research sector) and other external participants (peripheral), as described in the INMED project implementation field notes. Partnership with patient partners was perceived by most actors as central in justifying their commitment to intersectoral action.
Interdirectorate partnerships
Analysis of the field notes shows that PAR activities have furthered the creation of new collaborations between the various actors from different departments. The involvement of new actors in the INMED-COMMUNITY pathway enabled the mobilized actors to rethink the organization of primary care for people living with diabetes differently at health sector level, as mentioned by a manager and a primary care professional (Table 4, extract 1). Most managers also mentioned the value of “limiting duplication of services” by pooling professional resources in primary care to organize care and services for people living with diabetes (Table 4, extracts 2 and 3).
Interessement.

Cross-sector partnerships
All stakeholders expressed a willingness to create partnership links between the community and healthcare sectors. The community organizer mentioned the relevance of calling on community participants to respond to person-centered needs and stated “the potential to perpetuate” these links to work together over the longer term (Table 4, extracts 4 and 5).
Peripheral partnerships
The field notes described the relevance of the collaboration created by the INMED-COMMUNITY project team and a team of professionals from another region of Quebec, who held tools useful for educating and supporting the self-management of people living with diabetes online. This peripheral collaboration was understood by one of the primary care managers as an opportunity to “share expertise” to “enrich the care offer” available to people living with diabetes (Table 4, extract 6).
Patient partnership
All the participants mentioned that the “experiential knowledge” of the patient partners had been indispensable in linking theory and practice, and in reflecting on useful organizational processes for patients; this was present both in interviews and in field notes taken by the research team. One of the managers justified the involvement of patient partners as a contribution to clinical “good practice” and research. Participants were swayed by the importance of “listening to patients first” to enable innovative organizational interventions that can meet their needs, as reported by the community organizer (Table 4, extracts 7 and 8).
Involving stakeholders through project coordination and a shared definition of diabetes
The analysis shows that the partnership with the research team was established through recognition of the role of the 2 INMED-COMMUNITY project coordinators. Their main contribution revolved around controversies arising at meetings and committees. The principal researcher’s field notes show that links established with participants enabled gradually identification of the project’s controversies, explored how to facilitate the evolution of action, and contributed to the formation of network through the realization of various selected deliverables.
One controversy raised during the INMED-COMMUNITY pathway was linked to the fear of duplication for preventive and educational services between a local community diabetes organization and the health sector. This controversy was addressed during the INMED-COMMUNITY pathway in a working reunion where stakeholders from both sectors could share information about their respective services. Subsequently, the local community diabetes organization was invited to deliver 2 presentations about their services within the participating U-FMGs. This initiative aimed to streamline the process of health providers referring diabetes patients to the local community organization.
Despite controversies identified by the principal researcher, they were not raised by participants in the interviews. In fact, most of them spoke of the coordinators’ “facilitating” roles in creating links and engaging in actions (Table 5, extracts 1 and 2). A primary care manager also mentioned that presence of the research team had facilitated the “transformation of practices” desired by the implementation of the INMED-COMMUNITY pathway, and that it had supported the transformation process (Table 5, extract 3). The “pro-active involvement” of the research team was also highlighted by one of the professionals as a facilitating factor for collaboration and its “sustainability” (Table 5, extracts 3 and 4). One of the patient partners mentioned the importance of managers in “gathering ideas, removing what was not useful and keeping the interesting content of exchanges” to create value (Table 5, extract 5). One of the managers mentioned that this role had the potential to be “transferred” to another team to perpetuate the implementation of the INMED-COMMUNITY pathway (Table 5, extract 8).
Enrollment.

The principal researcher’s diary entries highlighted the evolution of the actors’ definition of diabetes throughout the implementation process of the INMED-COMMUNITY pathway, moving from a disease-centered approach to one focused on the needs of the person living with diabetes. The PAR approach led each actor to “step outside the known box,” as one primary care manager put it during the interviews (Table 5, extracts 9 and 10). As one professional stated, the person living with diabetes “needs social and community support” that goes beyond the vision of the disease and care offered by the healthcare system (Table 5, extract 11). A patient partner participating in the INMED-COMMUNITY pathway expressed this and emphasized that collaborations with the community sector would help patient get better health education and information about how to care about their different needs, such as how to manage cooking and alimentation (Table 3, extract 14). Most participants mentioned that development of the INMED-COMMUNITY pathway had the potential to offer a “broader and more efficient” range of services for people living with diabetes, as stated by one professional (Table 5, extract 13). Finally, one of the managers stated that by mobilizing around diabetes, there was potential to adapt the approach to the monitoring of “other chronic diseases” (Table 5, extract 14).
Alignment of actors, resources, and network support
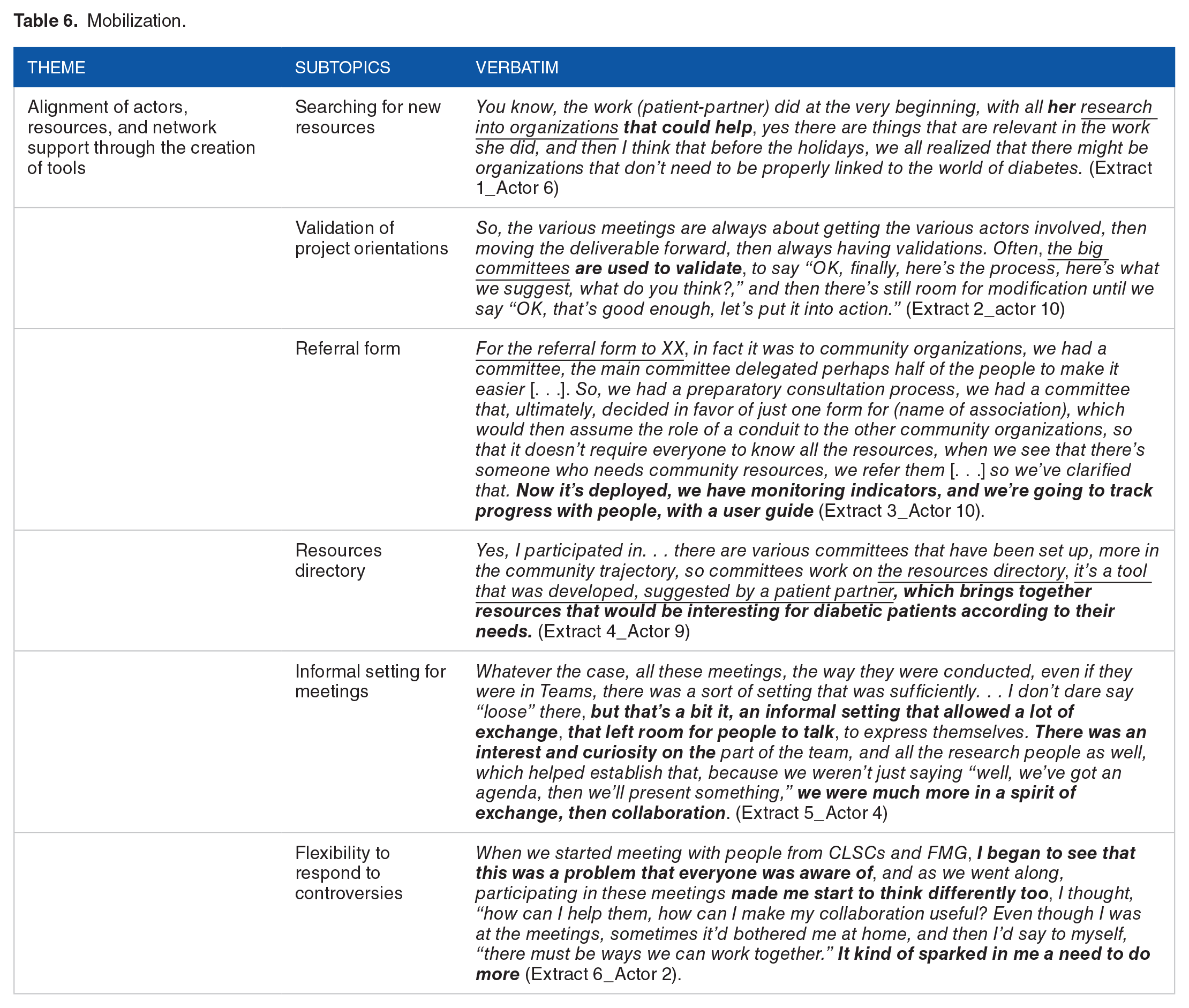
Notes from meetings have shown that creation of new tools has enabled commitment to mobilization in the INMED-COMMUNITY pathway. These notes also show that each action further developed establishment of working “committees” (Table 6, extract 2), 21 which were useful in resolving controversies. In fact, there were several mentions of mobilization to “look for new resources,” “validate project orientations,” and develop new tools, such as the “referral form” for diabetics to the community or the “resource directory” (Table 6, extracts 1, 2, 3, and 4). According to a manager and a patient-partner, these actions have enabled a development of a follow-up over time and established “both formal and informal modes of operation” (Table 6, extract 5), partnerships and flexibility in actively responding to controversies (Table 6, extract 6).
Mobilization.
Discussion
The contribution of our analysis broadens the current understanding of intersectoral collaboration with regards to the complexity of care for people living with diabetes.
The results showed that the actor-network theoretical approach to health intervention in intersectoral collaboration was favorable in supporting a people-centered care for people living with diabetes. In the light of ANT, results showed growth through controversies, contribution of key mediators (project coordination) and shared commitment of human and non-human actors (creation of tools) to engage in an intersectoral collaborative health intervention.
The importance of profit-sharing through project coordination
The results of our project have shown the importance of project coordination in the process of developing intersectoral collaboration. It played an essential role in mediating power relations and supporting progress in cross-sector action. Coordination facilitated exchanges and transfer of knowledge within the network, while also maintaining an appropriate work pace. Trust was created to commit to a common vision supported by the project team. These results support observations by Borvil et al and Christensen et al recognizing the importance of the role of mediators and their recognition at the level of the socio-technical network.50,51
Nonetheless, interactions also generated power dynamics where coordination of actions was important. Certain asymmetrical positions between actors from different sectors generated latent conflicts which impeded progress. Research has identified the risks of focusing on sectoral issues and outcomes that can generate unequal power relationships between actors when seeking cross-sectoral collaboration. For this reason, it is essential that the public policies implemented are not perceived as a burden and that power is shared.50,52,53 As this project is in progress, several issues have remained, for which no resolution could be found. Callon 22 and Latour 25 state that controversies in the translation process can encourage the enlistment of new participants, stabilize uncertainties, and develop interactions in the network through expression of contradictory arguments and viewpoints. Ultimately, controversies are at the foundation of the network, and our understanding show that their presence enable the network to build, make and unmake itself.22,25 Our article thus advances the literature on this subject, going further than Chiari et al 54 who argued about the importance of integrating actors and resources to advance action. Indeed, our results underline the importance of project coordination as a mediator and facilitator to identify controversies and accompany actors in the progress of action. Considering and identifying controversies was a strength of the project, which quickly mobilized stakeholders in a promising start to cross-sector collaboration. However, as the project moves forward, it will be essential to assess the perceived effects of these actions and gain a better understanding of the implementation process. A subsequent article will describe transitional results seen in the cross-sector partnership actions as part of the INMED-COMMUNITY pathway.
Mobilizing stakeholders around a common definition of diabetes
Our results show that the formal and informal meetings held during the various phases of participatory action research have helped mobilization and co-creation of network tools. Stakeholders have been able to learn collaboratively around issues for people living with diabetes. As Hendriks et al, 55 van Eyk et al, 56 and Chiari et al 54 all point out, these actions facilitate the integration of stakeholders in the implementation of cross-sector collaboration. All stakeholders take a stand, share different opinions, improve their knowledge, and reframe the problem in such a way that they have an influence on different sectors. This way of considering diabetes as a multidimensional condition has enabled us to move from a disease-centric to a person-centric approach. Furthermore, this understanding of diabetes addresses the complexity of the network and the integration of common ties without compromising the multiple layers of relationships, practices, and meanings specific to each community or group. 57 In this way, the aim is not to find a standard definition unequivocally adopted, but to remain in a state of questioning, which will continue through the resolution of controversies. 57 Networks must enable cross-sector partnerships, which allow stakeholders to define and share roles organically, while furthering different perspectives, essential in the creation of a broad, innovative network. 58
PAR as a facilitator in the implementation of an intersectoral collaborative health intervention for the follow-up of people living with chronic diseases
The PAR process used to implement the INMED-COMMUNITY pathway facilitated the application of ANT.34,38 The interdependence of the network and actors mobilized facilitated the co-construction of the INMED-COMMUNITY pathway and was of great interest for the application of ANT. In fact, ANT functions as a collaborative lever for flexible partnerships. It enables the operationalization of an innovative project by adapting to the context and adopting a holistic approach in response to a complex health situation. PAR combines research and action to produce knowledge that can inform healthcare practices, services, and organizations. 34 When all team members can act as decision-makers with academics throughout the research process, the likelihood that the results will be relevant and used by these members is increased and therefore beneficial beyond the research objectives.34,35,59
Patient partner participation in the PAR process of the INMED-COMMUNITY pathway is also a contributing factor to the success of the intersectoral intervention. The patient partner acted as a bridge between community and health sectors by centering the objectives of the INMED-COMMUNITY pathway on a more “patient-centered approach” and by enabling the project to consider the needs of people living more broadly with diabetes. Hence, the patient partner position in the PAR process of the INMED-COMMUNITY pathway is not limited to its contribution as a patient but involve a form of citizenship where their whole experience as a person living with diabetes is mobilized to make organizational changes on how different sectors communicate and work together.
Limits
This research has its limitations. First, the fact that the interview guide did not specifically ask actors about controversial issues limited the production of this data in interviews. However, the principal researcher’s field notes and diary highlighted the importance of controversies in the process of intersectoral collaboration. Second, only semi-structured interviews were coded, restricting the rigor of the research; however, these results were triangulated with data from the meetings and the principal researcher’s logbook (XX).47,49 Third, the representation of participants from the community sector was limited to 3 stakeholders. This may have skewed the emphasis toward the perspective of the health sector in this study’s results. Finally, this study was carried out in an urban town in Quebec and may therefore not be transposable to other contexts in Quebec, Canada or internationally, thus limiting the scope of the research. Nevertheless, the complexity of the research justified the mobilization of semi-structured interviews, and saturation of the themes was reached during analysis, as no new code emerged. 47
Conclusion
This study represents an important contribution to studies of intersectoral collaboration in healthcare, as it broadens current understanding of the complexity of care for people living with diabetes and helps describe the conditions necessary to implement intersectoral collaboration in primary care. The presence of project coordination facilitates involvement in an intersectoral collaborative healthcare intervention. The early recognition of controversies by an accepted and recognized coordinator facilitates negotiation between all stakeholders, enabling commitment to action. The use of these approaches will be considered in the future to facilitate operationalization of intersectoral collaborative health interventions and to measure effects on the health of people living with chronic diseases. Furthermore, future studies of intersectoral collaborative health interventions should examine the effects produced on people’s health data and could explore if the PAR approach and the involvement the community sector can have a significant impact on health results and social determinants of health in people living with chronic illness.
Footnotes
Appendix 1
Acknowledgements
The authors would like to thank the professionals, managers, and patient partners of the two participating clinics for their substantial contributions to the ongoing implementation and evaluation of the COMMUNITY INMED care pathway. The co-investigator principal (GL) would like to thank the Canada Research Chair in Adaptive Health and Social Systems for supporting the production of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Quebec Ministry of Health and Social Services grant program, in partnership with the Quebec SRAP support unit and the Fonds de recherche du Québec en santé (FRQS): Patient-oriented research in support of clinical and organizational transformations in community-based integrated care and services.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
GL co-designed the study. AT helped determine research relevance and design the interview guide. GL and AT co-led the data collection and the qualitative analysis. The entire research team helped interpretation of the results. GL, AT and IG wrote the manuscript. SMY provided editorial assistance in the preparation of this article. GL is nominal co-principal investigator. All authors approved the final manuscript.