
Abstract
This study estimates the years of potential life lost (YPLL), years of potential productive life lost (YPPLL), and cost of productivity loss (CPL) owing to injury-related mortalities in Mongolia. By implementing a retrospective cohort study, the study used secondary mortality data for Mongolia from 2016 to 2020 from the Health Development Center. Our study incorporates information on 13 551 fatalities from injuries and external factors, with the aim of estimating YPLL, YPPLL, and CPL associated with the leading causes injury-induced deaths. These include exposure to toxic substances, road accidents, homicides, suicides, and falls. Our findings reveal majority of the losses occur because of exposure to poisonous chemicals, road accidents, suicides, falls, and homicides. Furthermore, 444 550 years of potential life are lost owing to injury-related mortalities, in which YPPLL accounts for 338 482 years. The CPL caused by these premature deaths during the study period accounts for $1.368 billion. Notably, YPLL, YPPLL, and CPL rates are significantly higher in males than in females. The YPLL from exposure to poisonous chemicals is higher than those caused by other factors. This study is the first to calculate the CPL owing to YPLL from injury in Mongolia.
Introduction
Approximately 5 million people worldwide die annually owing to trauma, poisoning, and other external causes, representing 9% of global mortalities. 1 In 2021, preventable mortality owing to injuries are the third most common cause of mortality. Fatalities rising from falls claim over 684 000 lives per year and are on the rise. 2 Asia and the Western Pacific region have the highest number of injury-related mortalities. 3 Children and young adults under the age of 20 residing in Asia and the Western Pacific region account for almost 55% of the total injury-related mortalities worldwide. The leading causes of mortality among children in these regions are drowning, road accidents, burning, falls, intoxication, and intentional self-harm. 4
According to the National Statistics Office of Mongolia, Mongolia’s total population reached 3.3 million by the end of 2020. In the years 2016 to 2020, the population increased by an average of 58 000 to 60 000, which represents a growth rate of 1.8%.5,6 In 1990, the main cause of mortality in Mongolia was respiratory system diseases. Since 1992, however, cardiovascular diseases have taken the lead. In 2020, per 10 000 people, cardiovascular diseases led to 16.4 mortalities, cancer to 13.1 mortalities, and injuries/external factors to 1.9 mortalities, marking these as the most common causes of mortality in the country.
Injury-related mortalities and illnesses in Mongolia have increased drastically in recent years. In 2020, injuries became the fifth highest cause of illness and the third highest cause of mortality, with nationwide reports of 145 497 injuries and 2736 mortalities. 7 Males are exposed to illnesses caused by injuries 1.5 times more than females. Of the injury-related mortalities, 76% are considered unintentional, while 24% are considered intentional. The 5 most common causes of mortalities include unintentional intoxication owing to exposure to poisonous chemicals (28.3%), car accidents (17.9%), intentional self-harm (16.5%), murder (7.6%), and falls (6.8%).
While the Health Development Center of Mongolia diligently records the number of illnesses and fatalities, research focusing on injury-related illnesses and deaths remains limited. Health economics, a nascent field in Mongolia, has yet to estimate the Years of Potential Life Lost (YPLL) and Years of Potential Productive Life Lost (YPPLL) attributed to injury-related fatalities. Consequently, the importance of preventive measures, health education, patient treatments, and the estimation of YPLL owing to injury-related illnesses and deaths cannot be overstated. These actions are vital for policy development at management and planning levels, and to address the adverse impacts of deaths on Mongolia’s socioeconomic environment. This study aims to quantify the loss of life years, loss of productive age population years, and economic losses because of injury-related deaths in Mongolia from 2016 to 2020.
Methodology
Study design
This study uses a retrospective cohort study design.
Data
Quantitative data on mortalities in Mongolia are recorded by the General Authority of State Registration and the Health Development Center. The study utilized data on mortalities in Mongolia from the Health Development Center database from 2016 to 2020. The database, detailing 13 551 fatalities caused by external factors or injuries during this period, aligns with the international categorization of diseases V01-V99, W00-X59, X60-X84, X85-Y09, Y10-Y34, Y35-36, Y40-Y84, and Y85-89. Information on the deceased includes age, gender, education level, birth date, employment status, profession, year/month/date of mortality, cause of mortality, location of mortality, and types of mortality. Data on working-age population and gross domestic product (GDP) per capita are obtained from the National Statistics Office of Mongolia (Table 1).
Inclusion and exclusion criteria for the study.
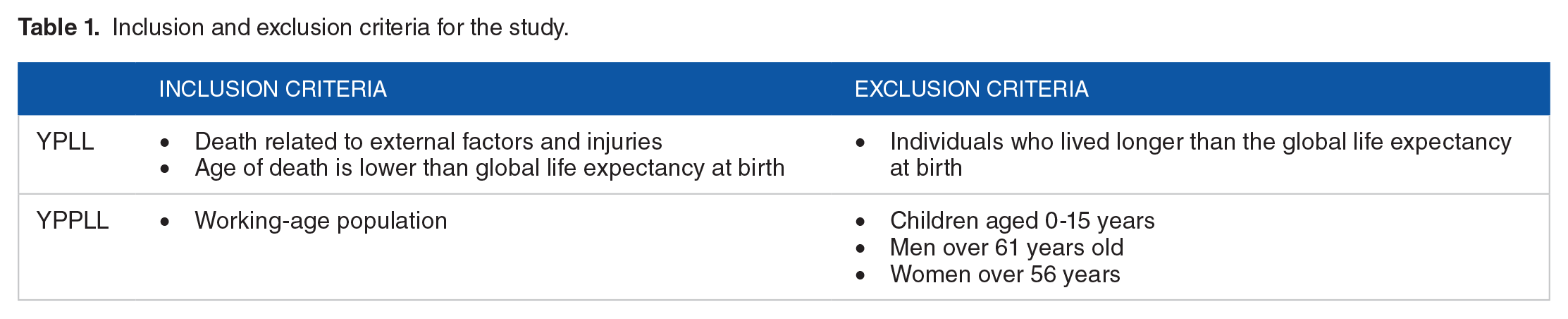
We employ 3 main criteria to estimate the data. First, for the YPLL calculation, we include the number of mortalities owing to external factors and injuries during 2016 to 2020. Second, to estimate the YPLL, we calculate the age of mortality for men and women who died before reaching the global life expectancy during the study period. 8 Participants above global life expectancy are excluded. Lastly, for the YPPLL calculation, study included women aged 15 to 56 years and men aged 15 to 61 years who died as a result of accidents. Children aged 0 to 15 years, women over 56 years old, and men over 61 years old are excluded.
Measures
To calculate YPLL, YPPLL, and cost of productivity loss (CPL), the study included variables such as date of birth, age, gender, date of mortality, education, employment level, and location of the accident. The International Classification of Diseases version 10 (ICD-10) is used to code the injuries.
The age at death in the statistical data is divided into 4 groups: 0 to 4, 5-9, 10-14, and 15-19. The 5 leading causes of injury are defined according to the ICD-10. 9 The YPLL and YPPLL are calculated based on age at death, gender, and cause of injury, whereas the CPL is calculated based on age at death, gender, and employment level.
Estimation methods
Based on the data for 13 551 injury-related mortalities from 2016 to 2020, the YPLL, YPPLL, and CPL are calculated.
Calculation for YPLL
Mongolia’s population grew consistently by 58 000 to 60 000 per year from 2016 to 2020, totaling 3.1 million in 2016, 3.17 million in 2017, 3.2 million in 2018, 3.3 million in 2019, and 3.35 million in 2020. 6 Data on 13 551 injury-related mortalities from 2016 to 2020 are classified according to age groups by the National Statistical Office of Mongolia. They are further categorized according to sex, cause of mortality, place of mortality, working-age population, and employment status. The following formula is used to calculate the YPLL by age group and cause of mortality 10 :
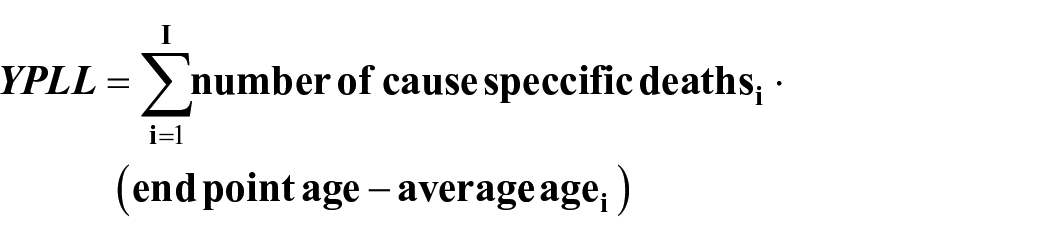
In this equation, i = 1,2,3, . . ., and I refers to 5-year age groups for all the populations.
Calculation for YPPLL
Mongolia’s GDP increased by an average of 21% from 2016 to 2020. Its GDP is $3681 in 2016, $3705 in 2017, $4171 in 2018, $4450 in 2019, and $4128 in 2020. 11 The working-age population is defined as those aged 15 years and above. In 2020, Mongolia approximately had 1.25 million working-age individuals, which accounts for 37% to 43% of the total population. 11 Therefore, the YPPLL is calculated based on the number of mortalities among the Mongolian population aged 15 and above.

In this equation, j = 1,2,3, . . ., J refers to 5-year age groups for all working-age populations (15-61 years).
During the survey period, the retirement age for men in Mongolia was 61 years, and that for women was 56. 12
Calculation of CPL
The CPL owing to potential productive lives lost and injury mortality are calculated by multiplying each YPPLL by GDP per capita of Mongolia within 2016 to 2020:

CPL is likely overestimated, as it is calculated using GDP per capita.
Statistical analysis
Results are presented as numbers and percentages for qualitative variables, whereas the median describes quantitative variables. Jonckheere’s trend test is performed on the number of mortalities owing to accidents per year, utilizing Microsoft Excel 2017 and SPSS 22 statistical software for data analysis.
Research Ethics
The Mongolian National University of Medical Sciences’ Academic Council approved the research methodology on June 17, 2021 (meeting no. 21/22). The Research Ethics Review Committee meeting of the Mongolian National University of Medical Sciences discussed the research methodology in their meeting on December 24, 2021 (meeting no. 2021-3/13), subsequently granting research permission.
Results
Descriptive analysis
Table 2 presents the demographic results of deaths caused by injuries in Mongolia during 2016 to 2020. Over the 5 years, 13 551 individuals died from injuries, of which 79.4% were men and 20.6% were women. Within the age groups, 10 487 (77.4%) of the total deaths occurred in the 20 to 59 age bracket, while 1096 (8.1%) occurred in the 0 to 9 age group. 59.5% of those who died from injuries had secondary education, 12% had higher education, and 11.5% had no education. Considering employment status, 35.6% were unemployed and 31.1% were employed. Of the deaths, 32.9% occurred at home, 20.9% in the field, and 17.9% in a hospital.
Demographic characteristics of injury mortality data.

Out of 82 452 mortalities in Mongolia between 2016 and 2020, 13 551 (16.4%) mortalities are attributable to external injuries. Figure 1 shows the breakdown per year from 2016 to 2020.

Total mortality and Mortality of injuries (2016-2020).
Mortality by age and cause
Table 3 presents the causes of mortality owing to injuries in Mongolia. It also provides a breakdown of the injury-related mortalities by age group and gender.
Causes of injury-related mortality from 2016 to 2020 (per 10 000).

In Mongolia, 61.98 mortalities per 10 000 men and 16.08 mortalities per 10 000 women are injury-related deaths. Men are significantly more likely than women to die from injuries (P = .0001). Exposure to toxic substances is a major cause of mortality for those aged 40 to 44, while road accidents frequently cause mortality for those aged 45 to 49. Suicides peak in individuals aged 35 to 39, and both falls and homicides are more prevalent in those aged 0 to 4 compared to other age groups.
YPLL by specific cause
Table 4 presents the YPLL owing to injury-related mortalities in Mongolia. From 2016 to 2020, injury-related mortalities caused 444 550 YPLL. Men lost 335 637 YPLL, while women lost 108 903 YPLL. It is statistically significant that men lost 3.1 times more YPLL from injury-related deaths than women (P = .0001). The average YPLL for men is 31.7 ± 15.5 years, while that for women is 40.5 ± 19.7 years.
YPLL in Mongolia by main causes of mortality (2016-2020).

YPLL due to injuries in men are 3 times higher than that in women over the 5-year period. Meanwhile, Figure 2 shows that the average annual loss per capita due to injury-related mortalities from 2016 to 2020 has decreased.
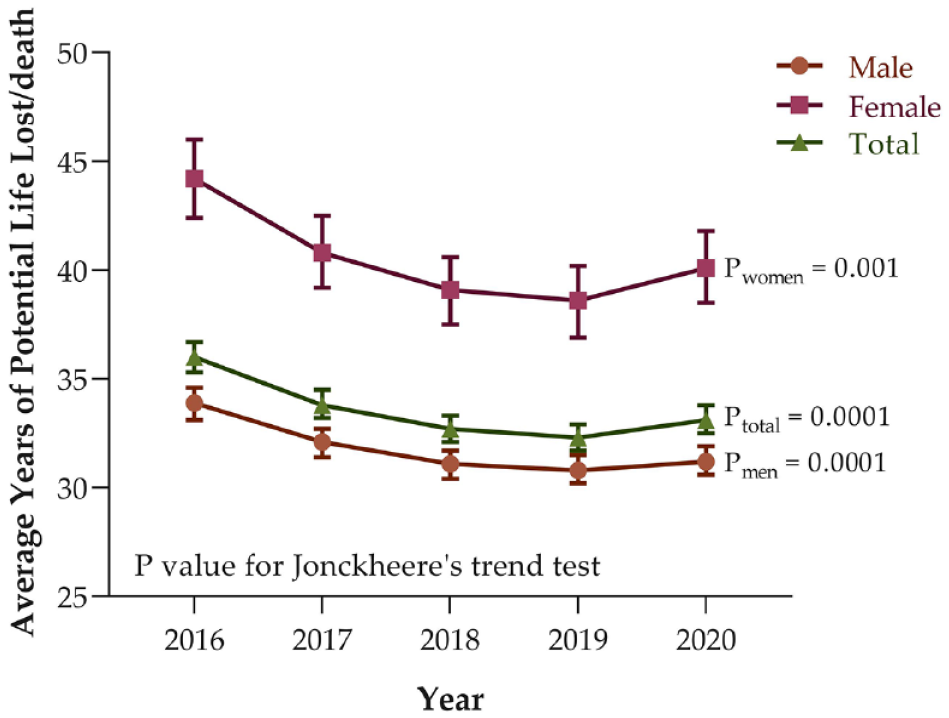
YPLL by gender (2016-2020).
YPPLL
Table 5 shows the YPPLL for the working-age population (aged 15-61 for men and aged 15-56 for women) in Mongolia from 2016 to 2020. Among the 10 857 mortalities in the working-age population, majority of the mortalities are men (83.6%). The total number of years lost by working-age people owing to injuries during the 5 years of the study is 338 482, with an average YPPLL of 31.2 ± 11.3. Exposure to toxic substances caused the highest YPPLL (84 301 years).
YPPLL for working-age population (2016-2020).
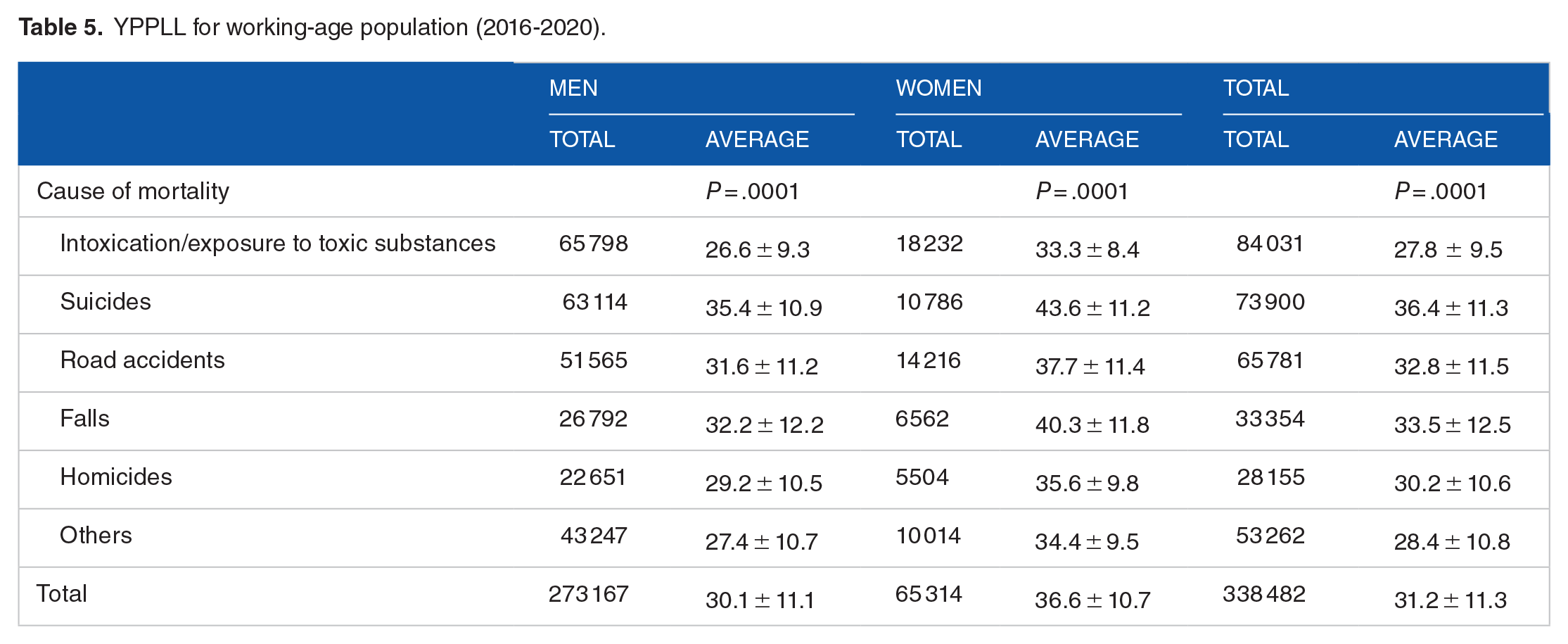
Overall, the YPPLL in men (273 167) is 4 times higher than that in women (65 314). However, the average YPPLL is 36.6 ± 10.7 years for women, while the average is 30.1 ± 11.1 years for men.
CPL
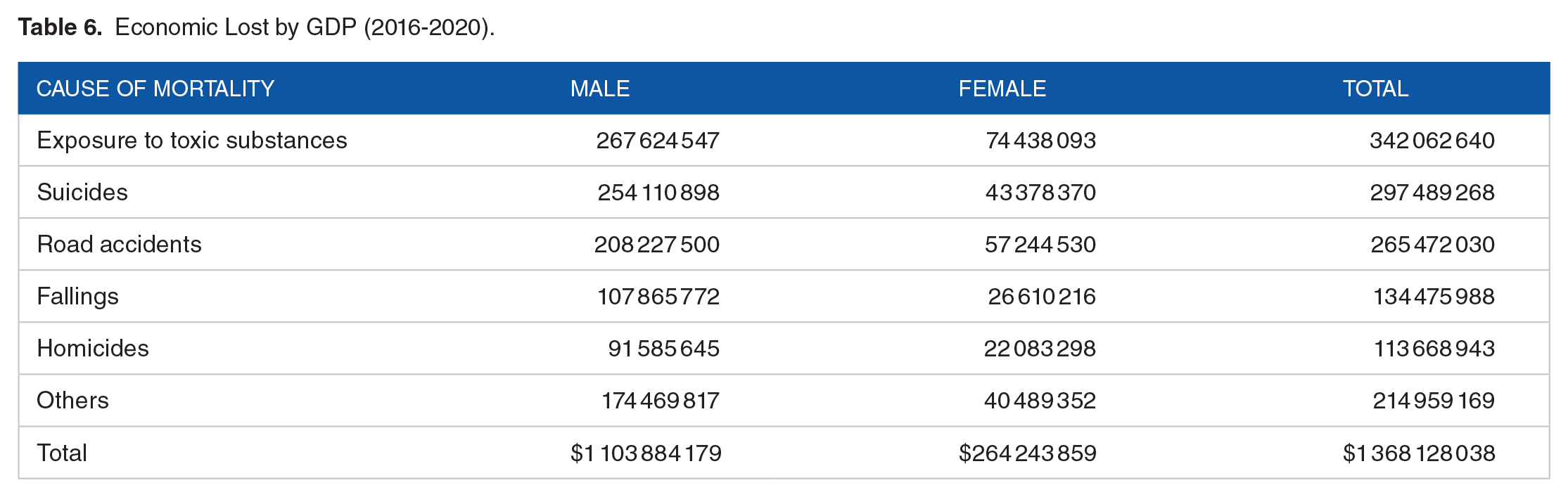
From 2016 to 2020, approximately 36.6% to 39.2% of people who lost their lives owing to injuries were employed, while approximately 60.8% to 63.4% of them were unemployed. The CPL from injury mortalities is estimated at $1.368 billion over the 5-year period. Table 6 breaks down the productivity losses by cause of mortality.
Economic Lost by GDP (2016-2020).
Discussion
In Mongolia, injury-related mortality is the fifth leading cause of mortality in 1990 to 1992, fourth leading cause of mortality in 1993 to 1998, and third leading cause of mortality since 1999 (1999-2020).11,13-15 Therefore, we examine YPLL, YPPLL, and CPL owing to injuries in Mongolia for the first time.
This research has supplied new evidence for policymakers by quantifying the number of person-years lost owing to preventable injury-associated deaths. Despite these contributions, limitations of our study include a lack of exploration into the healthcare system, social and economic conditions, and their impact. Furthermore, the study calculated economic loss per annum without considering the future value of money.
Annually, exposure to toxic substances results in 3436 fatalities, or 274 deaths per 10 000 individuals. Particularly during the chilly months from November to February, when temperatures plunge to an average of −25°C, and at night, even as low as −35°C, Mongolia witnesses a spike in fatalities. Amidst the 3.3 million population, 42% (2016) and 45% (2020) dwell in the capital city, Ulaanbaatar.16,17 Among them, 216 000 households occupy non-centralized heated apartments and gers lacking heating systems. 18 A government decision in 2018 to use improved fuels unfortunately led to many asphyxiation deaths, differing significantly from traditional heating experiences.
Road injuries account for 12.3% of all mortalities, primarily affecting those aged 45 to 49 years (12.3%), 30 to 34 years (11.1%), and 35 to 39 years (10.2%). To combat this, Mongolia implemented road safety policies and educational programs, including a police program for schools since 2013, a seatbelt usage campaign since 2018, and updated road rules for child safety. Violation penalties are stringent, including the potential long-term revocation of drivers’ licenses for drunk driving.
Globally, approximately 800 000 suicides occur annually, with an attempt every 40 seconds. 19 In the United States, suicide rates predominantly affect those aged 40 to 59 years (42.5%). 20 However, the high YPLL linked with suicides signifies that victims are relatively young. 21 In Mongolia, suicides accounted for 16.6% of all mortalities during the study period, causing a loss of 81 846 life years or 18.4% of all mortalities. Additionally, in China between 2004 and 2010, suicides accounted for approximately 16.2% to 22% of all mortalities. 22
Suicides, which were responsible for 15.2% to 18.5% of all injury-related mortalities in Mongolia, have steadily risen over the past 5 years, predominantly affecting young people and thus becoming a significant public health problem. Given Mongolia’s unique history and traditions, suicides are a taboo subject, often under-discussed, and public health responses are consequently limited. Addressing this requires the urgent establishment of a comprehensive community-based system to prevent suicides, increased access to mental health treatment, monitoring, rehabilitation, and continuous management of suicide attempt survivors. As of 2019, Mongolia only had 173 psychiatrists or 0.5 per 10 000 people, 13 underscoring the urgent need to address the human resource shortage in mental health treatment, particularly for substance abuse.
From 2016 to 2020, fatalities caused by falls represented 11.1% of all injury-related deaths in Mongolia, resulting in the loss of 55 295 lives and a consequential cost of $134.5 million in terms of CPL. In the same country, 13% to 19% of injury-related deaths occurred among individuals aged 0 to 19 years. Notably, the highest number of fatalities owing to falls was recorded among children aged 0 to 4 years, with a total of 12 040 deaths.
Accidental injuries and domestic violence are the leading causes of mortality in children aged 0 to 19 years in the United States. Accidental injuries account for 5% of infant mortalities under the age of 1 year and 34.5% of mortalities among children aged 1 to 19 years. The mortality toll caused by falls is the highest in children aged 0 to 4 years. 23
Murder accounts for 14% of mortalities in the 0 to 4 age group and 13% in the 40 to 44 age group in Mongolia. From 2016 to 2020, total YPLL because of murder was 41 978. Of this, children aged 0 to 4 years accounted for (28.5%), while individuals aged 35 to 39 years accounted for 5383 (12.8%). Furthermore, murder claimed the lives of 929 individuals of working age, with the economic losses associated with this age group comprising 8.3% of the total CPL. Research indicates that in the United States, infant mortality due to murder is more prevalent in infants under 1 year of age. 23 Moreover, murder accounts for 59.5% of injury-related deaths among individuals aged 20 to 39 years. 20 Another study reveals that, from 2016 to 2018, 93.5% of the 201 victims were men, with one partner involved in 15.3% of cases, and both partners involved in 25.2% of cases. 24
Conclusions
Between 2016 and 2020, injuries caused 13 551 mortalities in Mongolia, resulting in a total of 444 550 years of potential life lost (YPLL). This implies that, on average, an individual lost 33 potential years of life. During the same period, there were 10 857 mortalities among the working-age population in Mongolia, with the majority being men (83.6%). The total YPLL for this period was 338 482, averaging 31 years of potential life lost per person. The cost of productivity loss (CPL) from injury mortalities over this 5-year period was approximately $1.368 billion, with men accounting for the majority of these losses (80.7%).
Footnotes
Funding:
The authors acknowledge the financial support received for this research, authorship, and/or publication of this article. This study was supported by the Health Promotion Fund, Ministry of Health, Mongolia, under grant number 2021-2-4.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors have made substantial contributions to the design of the work; or the acquisition, analysis, or interpretation of data for the work. All authors have substantially contributed to drafting the work or revising it critically for important intellectual content. All authors have given final approval for the version to be published.