
Abstract
Aim:
We aimed to illustrate and compare the processes of mental health policies aiming at a service delivery shift from the hospital to the community using implementation science, and to identify important implementation strategies.
Methods:
This study had a comparative case study design. The cases were the Belgian mental health reform, and the person-centered model of mental health in Hong Kong, China. Several documentary sources were reviewed, including the published literature and websites. Data on policy processes were extracted, analyzed using directed content analysis, and categorized into constructs of the conceptual model for evidence-informed policy formulation and implementation arranged for the mental health policy.
Results:
Several similarities were identified in the strategies for active implementation and dissemination; official staff allocation, and training to the community psychiatric services, an approach to adjust the number of psychiatric hospital beds, and promoting collaboration between health care sectors and social welfare sectors. Under distinct social contexts, differences were found in all processes.
Conclusions:
Each of the described policy processes can serve as a model for countries in similar social contexts seeking to shift their psychiatric service delivery. Furthermore, our findings suggest widely applicable implementation strategies for policies aiming at a service delivery shift.
Keywords
Background
In the previous few decades, mental health policies have been developed, implemented, and reformed in many countries with different financial and social backgrounds. 1 In the 1970s, mental health reforms were started under deinstitutionalization movements, mainly as national policies, such as in Germany (Psychiatry-Enquete) and Italy (The Law 180). Community treatment models for psychiatric patients have been reported to be more effective than hospital treatment models, because the number of cases of relapse and hospital admissions are expected to be reduced. 1 Chow et al interviewed experts from England, Germany, and Italy, and found that deinstitutionalization is driven by a humanitarian philosophy together with the expectation of cost reduction. 2 As a result of rapid deinstitutionalization, community care was able to provide higher quality care for many patients, but there were many unmet needs, particularly for those with severe mental illnesses who have a high risk of harming themselves and others. 2 Deinstitutionalization is required to be accompanied with the creation of alternative services for these patients, such as residential and forensic services, and enhanced risk management systems in the community. Based on such unmet needs, the assertive community treatment (ACT) model, which was originally developed in the 1970s in the United States, subsequently spread to 21 countries, with local variations. 3 In the ACT, a small, interdisciplinary team provides individualized, time-unlimited services to users with the greatest risk of relapse. 3 These efforts involve integrated support across a wide range of areas, including healthcare, housing, employment, and interpersonal relationships; in other words, social integration. The World Health Organization (WHO) stated that activities promoting the social integration of people with mental health problems and the expansion of their social network are very important for enhancing their well-being. 4 The social integration of people with mental health problems is partially supported by deinstitutionalization movements, with a transition of resources from institutional psychiatric care to community care. 5 Despite the progress in deinstitutionalization movements in recent decades, efforts to socially integrate people with mental health problems has not been as successful as anticipated. 5
In the 2000s, a shift from psychiatric care mainly in the hospital to psychiatric care mainly in the community was implemented in Asia and other regions. Nowadays, many middle-income countries are facing the necessity of mental health reform, whereas most low-income countries are developing their mental health care system with limited resources. It is expected that countries that established their mental health policies later are more likely to reduce number of beds in psychiatric hospitals and other medical settings than countries that have a long-established policy owing to their technical efficiency. 1 However, there have been few reports to date on the policy processes of mental health reform; that is, how mental health policies aiming at a service delivery shift from the hospital to the community have been formulated and implemented in various countries has remained unclear.
Implementation research
Implementation research is defined as the systematic study of how a specific set of activities and designated strategies are used to successfully integrate an evidence-based public health intervention within specific settings. 6 Theories, models, and frameworks (TMFs) used in an implementation study provide a systematic structure for the development, management, and evaluation of implementation by linking study aims, designs, measures, and analytical strategies. Various TMFs are invented for different aims; that is, describing and/or guiding the process of translating research into practice (process models); understanding and/or explaining what influences implementation outcomes (determinant frameworks, classic theories, and implementation theories); and evaluating the implementation (evaluation frameworks). 7 Implementation strategies are defined as methods to enhance the adoption, implementation, sustainment, and scale-up of an innovation, and are thought to be the key to the success of new interventions. 8 There are a limited number of TMFs used in implementation research for policies and their applications, whereas are abundant history in the field of political science and public administration.9-12 Therefore, the accumulation of experience in the field of policy implementation research is needed.
Our conceptual model
To describe the policy process, we used the revised conceptual model for evidence-informed policy formulation and implementation developed by Strehlenert et al. 13 We chose this model because this was the only framework that had been developed for policy implementation research when we were designing our research plan, and furthermore, it covers the entire policy process, including agenda setting, policy formulation, policy implementation, and evaluation. We arranged it for the mental health policies using the context introduced by Omar et al 14 (see Figure 1). In the study published in 2015, Strehlenert et al combined central features of the framework for evidence-informed policymaking and a framework for policy dissemination and implementation, to cover the entire process from policy formulation to implementation, and modified it to identify sub-system actors, capacity building, and overlapping policy processes. 13 Their model reflected the standard illustration of policy processes, including the following phases: agenda setting, policy formulation, policy implementation, and evaluation. 15 In this conceptual model, there were no specified constructs about the context. Therefore, in our study, we used the following constructs for context according to the aim of the study, “Structure and financing of the health system,” “The mental health care system,” “Priority problems and position of mental health,” and “Public attitudes to mental illness,” based on a comparative case study on the mental health policy processes by Omar et al. 14 The definitions and annotations of the constructs on our model are shown in the Supplemental File 1.

Objective of the study
This case study aimed to illustrate and compare how policies aiming at a service delivery shift from the psychiatric hospital to the community are formulated and implemented under different social contexts using implementation science. We also aimed to identify implementation strategies for the service delivery shift that are applicable to different social contexts, by identifying similarities between the policy processes.
Methods
Design
A comparative case study design was used. Each “case” was defined as a policy at either the provincial or national level, aiming to achieve a service delivery shift for psychiatric patients from hospital beds to community services.
Case selection
The criteria used to select cases for this analysis included (a) having a policy aiming to achieve a service delivery shift in mental health; (b) having a policy implemented after 2010; and (c) having a policy publicly available. Two cases were compared to keep the comparison manageable. Based on these criteria, the Belgian mental health reform “Toward a better mental health care system,” which was launched in 2010, and the person-centered model of mental health in the Hong Kong Special Administrative Region of the People’s Republic of China (Hong Kong), which was also launched in 2010, were selected. Supplemental File 2 describes each case.
Data collection
Several documentary sources were reviewed, including (i) published and gray literature using PubMed and PsycINFO on current and previous mental health reforms in Hong Kong and Belgium; (ii) policy blueprints and relevant websites on current and previous mental health reforms in each system, their targets and indicators, and prospects of each reform; and (iii) references from local experts of mental health reform. If the information in a reference was insufficient, additional information was collected through personal contact.
Analysis
First, data associated with the process, actors, and strategies of the reform were extracted. Next, all data sources were analyzed using directed content analysis. 16 The analysis was guided by the conceptual model for evidence-informed policy formulation and implementation arranged for the mental health policy developed from the frameworks by Strehlenert et al 13 and Omar et al. 14 The analyses were discussed with and confirmed by the authors who were native to the country/area of each case (JD from Belgium, and WTLL from Hong Kong, China).
Results
Belgian mental health reform “Toward a better mental health care system”
Social context
Under multilevel political governance (federal, region, and community), psychiatric services were provided mainly by publicly funded private hospitals using a reimbursement system of compulsory national health insurance (for more information about the social context before mental health reform, see Supplemental File 3).
Agenda setting
In 2002, the Ministry of Health and Social Matters of Belgium published a joint declaration on the future policy of mental health. This declaration was partly based on the WHO annual report of 2001, 17 and specified that mental health care, both acute and chronic, will be organized into networks and care systems to best meet the needs and demands for the care of people with mental disorders. 17 Despite various attempts to organize mental health care, the trend of long-term hospitalization and a high number of psychiatric hospital beds remained in 2008, and the federal government concluded that psychiatric hospitals were not making enough effort to reintegrate these patients into society. 17
Subsystem actors
Federal Public Service Health (FPS Health) was the main subsystem actor at the national level. The responsible ministers of federal and federated authorities on public health were involved in the decision-making of this policy at the Interministerial Conference (IMC). Psychiatric hospitals were the main subsystem actors at the area level, which decided the initiation of the network projects in each area. Various services, including Mental Health Care, Formal and Informal Community Care (ie, users and family associations), Primary Care sector, Social/Welfare sector, and vocational rehabilitation were involved in the function committees within the networks. 18
Policy formulation
Sourcing the evidence
In November 2009, 31 Belgian government officials, including the Vice-President, visited Birmingham, UK, to learn about the development of effective community-based mental health services. 19 Between April and October 2010, the FPS Health performed a literature review of the criteria and important aspects for defining the eligibility of the area and the involved partners to launch a network, the process of project development in each area, and the key competencies and profile characteristics of the network coordinators. 17
Using the evidence
The IMC established 5 main foundations to orient mental health care to solve the current issues of the psychiatric service delivery system: deinstitutionalization, inclusion, decategorization using network of care, intensification of hospital care, and regularization of the various pilot projects, at the federal, community, and regional levels. Then, the functions of Belgian mental health reform were developed. Between April and October 2010, based on literature review, the following steps were taken within the FPS Health: (1) Creation of a checklist for applications for the project by each area; (2) Review of the methodological steps in the development of care programs; (3) Creation of general points for the development of a proposal; (4) Overview of evidence-based practices in mobile teams (acute and chronic); (5) Creation of document templates that provide the most favorable method for choosing a “network coordinator.” 17
Active strategy for dissemination and implementation
Considering capacity to implement
Several IMCs on public health were held to consider implementation strategies regarding financial, communication, and other major aspects in September 2009, December 2009, and April 2010. 18
To facilitate communication between health care professionals in the field and the coordination of institutions to amend Belgian mental health reform and to formulate recommendations, the IMC founded the intercabinet workgroup “Taskforce mental health care.” This taskforce consists of political representatives of the IMC and competent administrations.
Capacity building
The legal basis for the reorganization of health care was created by adding an article that defines networks and circuits of care to the Hospital Act. This amendment was implemented in September 2009 to Article 107 of the Hospital Act, which created the possibility to develop alternative funding strategies. 20 Therefore, the Belgian mental health reform became commonly referred to as “Article 107 project,” referring to the small article that is nothing more than a financial strategy that enables hospitals to close beds and reallocate financial resources to care networks in the community. In April 2010, the guide “Toward a better mental health care system,” which consists of the outline of “the Belgian mental health reform,” its implementation, and its communication plan was published. From June 2010, networks could be created, and candidate networks could submit their plan for approval by the federal authorities. Hospitals were also offered incentives to start care networks and to set up the 5 functions of the network. 21 Approval was needed to be able to use the new funding system. The FPS Health recruited and employed network coordinators for the approved areas, and also provided training for sectorial officials, network coordinators, and service providers both before and after the launch of the network in each area. 22
Network weaving was promoted in each approved area using the bottom-up territorial approach. An “Innovative Practices Handbook” was created based on the good practices in each network, and was distributed in 2016 by the FPS Health to boost this approach. 23
Policy implementation
Awareness
From June 1 to October 31, 2010, all service providers were given full information about the overall concept of the mental health care reform (philosophy, general principles, purpose, and objectives), following the steps in the guide according to the communication plan. 17
Adoption
From 2011, actual implementation of the mental health care networks was started, 17 with the first approved network being initiated in the de Louvain area (Network Diletti). In 2019, the Belgian mental health reform was implemented in 20 areas, covering the whole of the country. 21
Implementation
In every network, all the service providers together constitute the strategic working committee, which is responsible for the implementation of the new way of service delivery. 17 The number of psychiatric beds decreased by 10.7%, from 12 779 in 2010 to 11 566 in 2019. 18 Although the reform was intended for adults with all levels of mental health problems, the first steps in the reform were mainly focused on people with severe mental illness, social deprivation, and poor social function. 17
Maintenance
The funding system of Article 107 did not enable the reallocation of budgets to psychiatrists who made the shift from the hospital to mobile teams. To promote the involvement of psychiatrists, an official arrangement of their funding was made among the psychiatrists, hospitals, and the National Institute for Health and Disability Insurance. 24
Policy outcomes
Monitoring
Processes and outcome measures used for the evaluation of elements of the model at the community level, based on its ultimate objectives, were a number of minimal clinical outcomes (number of [re]admissions, degree of reintegration into society, social inclusion, successful crisis interventions, etc.), and process variables (turnover of mobile teams, duration of treatment, training experience and other supervision needs, etc.). They were monitored through an annual audit of all networks. 17
Evaluation
For each network, the following evaluations and feedback were performed by the FPS Health: bottom-up process and impact evaluation with respect to the services provided to the area; facilitating factors and barriers in a local context; and cost of cross-sectorial cooperation (financing arrangements and cost).
A person-centered model of mental health in Hong Kong
Social context
Specialist outpatient services and 90% of inpatient services are provided by public funding of the Hospital Authority (HA) subsidized by the Food and Health Bureau (FHB), through 7 clusters of services. In the 2000s, the number of beds was gradually reduced by the HA 25 (for more information about the social context before mental health reform, see Supplemental File 3).
Agenda setting
In Hong Kong, the Priority Follow Up registry was established for psychiatric patients with a history of violence requiring priority follow-up, after a tragedy in 1982 in which a psychiatric patient killed kindergarten students. 26 In 2007, the Hong Kong College of Psychiatrists (HKCP) submitted recommendations to the FHB for the establishment of a coherent mental health policy, as well as to solve the problem of the fragmentation of mental health care. 27 In 2007, two Australian specialists of mental health conducted a review of existing services, and recommended the development of a more consumer-focused and evidence-based service delivery platform. 28
Subsystem actors
The HA and the FHB were the main subsystem actors. The Social Welfare Department of the Labor and Welfare Bureau (SWD) had taken joint initiative with the HA on the development of community psychiatric services (CPS). 29 The HKCP played roles in the submission of the proposal to the government and in its lobbying. 30 The CPS and a nongovernmental organization (NGO) subsidized by the SWD played important roles toward building effective community networks to support discharged patients. 28 Patients and carers were also subsystem actors. 28
Policy formulation
Sourcing the evidence
In addition to the recommendations from the HKCP and sources from service reviews, the taskforce, which was made within the HA, performed an extensive literature review. 28 International and local evidence regarding case management has been collected, which suggests effectiveness of the intervention. 31
Using the evidence
Based on the collected evidence, the taskforce developed the new service model, “A person-centered model of mental health” based on the treatment and recovery of the individual, because of the evidence of the needs for action toward shared care, burden of illness and lost productivity, and effectiveness of the recovery. 28 The draft was supplemented by other mental health experts in Hong Kong, and 2 external expert advisers from the UK and Australia. 28 Accordingly, the CPS was redesigned as the multidisciplinary case management program (Personalized care program; PCP). 32 The process was negotiated between the HA and the FHB.
Active strategy for dissemination and implementation
Considering capacity to implement
The taskforce drafted a strategic plan to implement the new service model. The contents were validated through an extensive consultation process, and the process was negotiated between HA and FHB.
Capacity building
In 2007, the government of Hong Kong announced that it would commit substantial resources from 2010 to the implementation of a multidisciplinary case management approach. 30 In 2010, the PCP was set up on a district basis (about 140 000-600 000 people per district). Psychiatric nurses and allied health professionals were recruited to act as case managers. 28 The HA and SWD collaborated closely so that the case managers could establish links with service providers of the social welfare sector through the Integrated Community Centers for Mental Wellness, which are usually managed by NGOs. 28 In 2016, the HA and SWD published a service framework to standardize the implementation of the PCP, and to enhance collaboration among major stakeholders. 29 A case management training program was established and provided to staff members. 28 In the CPS redesigned to optimize manpower, the stratification of service intensity and caseload of staff was performed based on risk and needs assessment. 29 The HA adjusted the number of beds so that the occupancy rate of inpatient beds remained at approximately 75%. 28
Policy implementation
Awareness
In 2010, the HA published a mental health service plan to disseminate the idea of a person-centered service model. Before publication of the plan, workshops, consultations, and field visits were held for various health professionals. 28 There were 40 responses to the consultation from individuals and organizations, consisting of 12 responses from the NGO of mental health services, and 2 responses from patient groups. The remaining responses were collected from the HA, other government departments, and professional bodies. 32
Adoption
During 2010, the PCP was adopted at 3 districts, which covered 1515 (44.4%), 1515 (37.6%), and 1560 (36.7%) patients with severe mental illness out of a total of 3415, 4033, and 4253 patients, respectively. From fiscal year 2011, PCP was expanded to 5 more districts. In 2015, it was implemented in all 18 districts. 31
Implementation
In December 2016, the PCP supported approximately 15 000 patients with severe mental illness residing in the community, maintaining a case manager to patients ratio of about 1:47 on average. 33 Regarding psychiatric beds, the total number of psychiatric beds was 4000 in 2009 but remained at 3607 between 2010 and 2018. 32
Maintenance
Service users have been playing an important role in the implementation of a new model, including the involvement of peer support workers, and giving feedback to services. In 2015 to 2016, the HA introduced peer support workers into the PCP, who will assist case managers to support patients in the recovery process through experience sharing. 31
Policy outcomes
Monitoring
The Electronic Health Record Sharing System (eHRSS) was launched in 1995, which subsequently developed into the current eHRSS, which is a 2-way system among public and private healthcare providers, through which all health services are monitored. 34 The HA developed key performance indicators (KPI) as a service management tool to track the HA’s performance in each program. 35 The KPIs for mental health services were “Unplanned compulsory psychiatric admission for patients receiving active personalized care” and “Average length of stay of acute inpatients.” 35
Evaluation
KPIs were reported and evaluated quarterly within the HA. Furthermore, as part of the feedback for mental health service plans for adults, a new group consisting of nominated representatives from service users, carer groups, and relevant NGOs collected their feedback and opinions to enhance service planning. 29
Similarities and differences between the cases
There are 4 similarities in the active implementation strategies between the 2 cases. First, the workforce was officially allocated to the multidisciplinary outreach service in the community. Second, official staff training was provided for launching a new service model. Third, a strategy to adjust the number of psychiatric hospital beds was established to enable budget reallocation from hospitals to the community. Lastly, collaboration between the mental health care sectors and the social and welfare sectors was promoted at both the government and local levels. We found that the strategy for active dissemination and implementation overlaps with policy formulation in both cases.
Cases differed in the following constructs. Regarding the main subsystem actor, in Belgium there were main subsystem actors for both the national (the FPS Health) and area level (psychiatric hospitals), whereas there were 2 main subsystem actors (the FHB and the HA) at the national level in Hong Kong. Regarding the active strategy for dissemination and implementation, a network was developed by the initiatives of each area and the experiences of the advanced areas were shared widely using the good practice handbook in Belgium. On the other hand, the new model was introduced vertically by the HA, and the service framework was shared widely to standardize the quality of implementation and collaboration between medical and welfare sectors. Regarding policy outcomes, both process and outcome data were monitored manually in Belgium, whereas KPIs were defined and monitored systematically using eHRSS in Hong Kong (for more information about the similarities and differences, see Table 1).
Key similarities and differences between the policy processes in the cases.
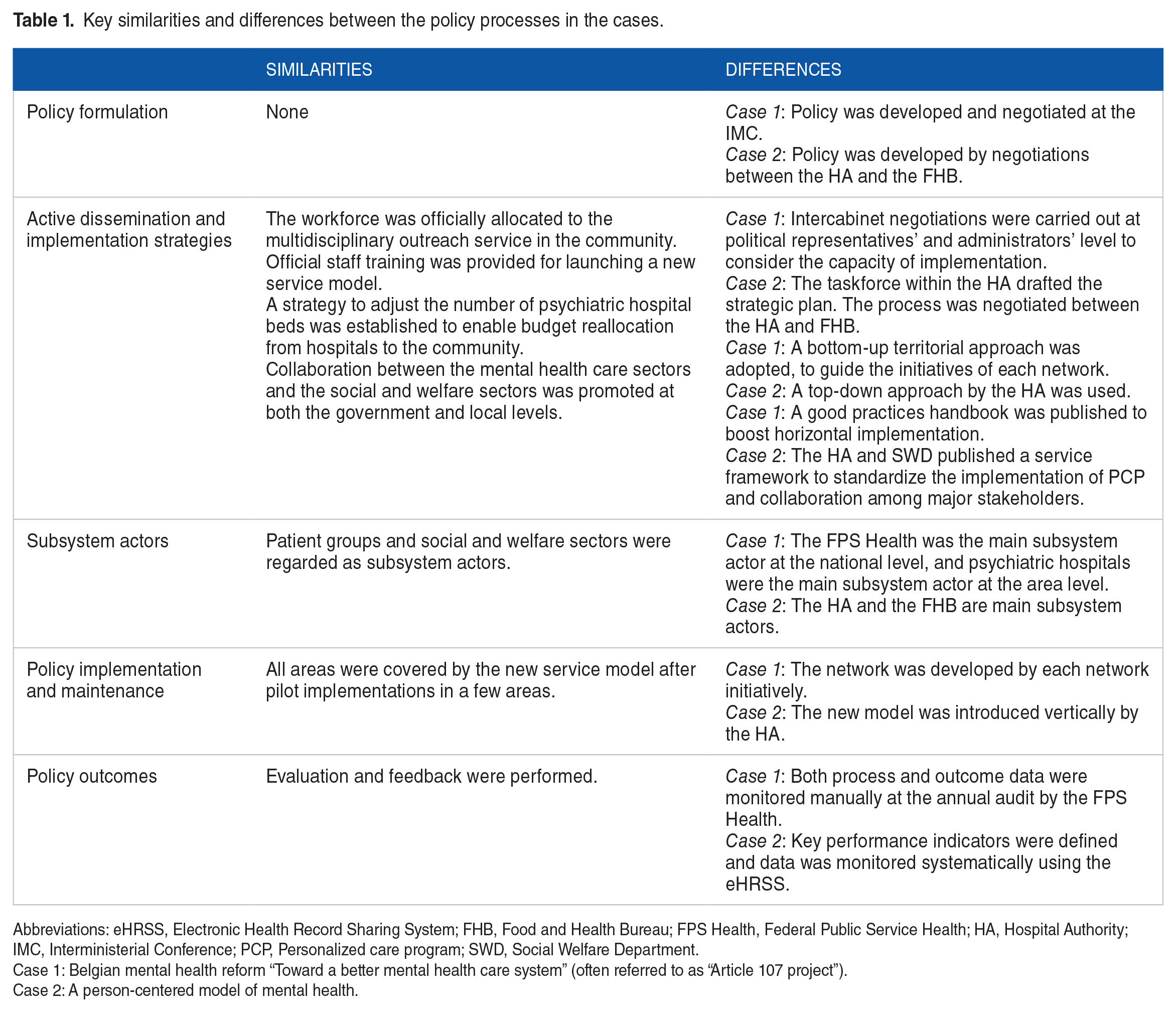
Abbreviations: eHRSS, Electronic Health Record Sharing System; FHB, Food and Health Bureau; FPS Health, Federal Public Service Health; HA, Hospital Authority; IMC, Interministerial Conference; PCP, Personalized care program; SWD, Social Welfare Department.
Case 1: Belgian mental health reform “Toward a better mental health care system” (often referred to as “Article 107 project”).
Case 2: A person-centered model of mental health.
Discussion
To our knowledge, this case study is the first to illustrate and compare the processes of the mental health policy aiming at a service delivery shift between 2 cases using implementation science. Data was collected from the literature, documents, websites, and references from local experts, and analyzed according to the conceptual model (see Figure 1). In Belgium, where the number of psychiatric beds remained high, mental health reform aiming at the integration of care and the reduction of beds was implemented using the reallocation of hospital budgets to mobile care teams, multidisciplinary outreach services, and the construction of territorial care networks. In Hong Kong, after the gradual reduction of hospital beds in the 2000s, a person-centered model using the case management approach, namely PCP aiming at the integration of care, was implemented based on new funding from 2010.
Social contexts have a large influence on the processes and choices of strategies. Thus, we analyzed 2 different cases from the areas and countries aiming to achieve a service delivery shift in mental health from hospital beds to community services. We found several similarities between the 2 cases in the strategies for active dissemination and implementation. We suggest that these similarities in implementation strategies might be applicable to other countries with different social contexts. According to the cross-national analysis of on 193 countries by Shen and Snowden, 1 late adopters of mental health reform are motivated to implement deinstitutionalization for technical efficiency. These cases and strategies might be very important technical cues for countries planning to adopt mental health reforms in the future.
Furthermore, we observed how social context can be facilitators/barriers of mental health reform. For example, we found that one of active strategies is official staff reallocation from hospitals to the community in both cases, and the difficulty in implementing this strategy depends on the structure and financing of the health care system. In Hong Kong, the public medical service system worked facilitatively because under the public working environment, the salary of medical professionals is ensured regardless of their allocation. In Belgium, services of accommodation and nursing activities are financed through a fixed prospective budget system. The income of the hospitals used to be decided according to the number and type of beds. Thus, there was a structural barrier for the reallocation of staff, which required new financing strategies, that is, “Article 107 of the Hospital Law,” which enabled a shift in funds from the hospital to the community. For countries newly adopting the mental health reform, how to enable a shift in funding in accordance with the context of the country/area will be crucial.
We arranged a revised conceptual model for evidence-informed policy formulation and implementation, which includes the new constructs “Sub-system actors” and “Capacity building” proposed by Strehlenert et al. 13 Although this conceptual model was helpful to analyze the 2 cases, one important feature found in this study was the overlapping of the processes between policy formulation and the strategy for active dissemination and implementation. In Belgium, the major active strategy for dissemination and implementation in the Belgian mental health reform “Article 107 of the Hospital Law” appears to be the onset of policy formulation. In Hong Kong, the decision of the government to fund the case management approach appears to proceed policy formation of a person-centered model of mental health. Furthermore, in the policy processes of both cases, strategies are considered and implemented through all the processes. Thus, more cases are required to further refer to clarify the overlapping of the processes.
Methodological consideration
The strength of this study is the use of the conceptual model, which was developed and validated for evidence-informed policy formulation and implementation. A wide range of data collections, including the collection of information from experts was performed. This study has some limitations. Firstly, owing to the limited literature available, the description of some of the constructs and the causal association between the constructs might be insufficient. In addition, we collected some of the information from policy plans rather than policy reports. To compensate for this shortcoming, we chose plans that were assured to be implemented by the local experts in the authors’ team. Another limitation is the restriction in the fields of the contexts and processes. In this study, we only included political and social aspects. However, aspects within the entire social system, such as the basic education system and religion, might potentially have influences on the mental health reform processes. Lastly, there was a lack of description at the level of the individual actors. It is difficult to include individual influences in this type of study. Usually, the influence of individual actors and their leadership and inhibition are very important. However, how to incorporate individual actions requires further consideration.
Conclusions
Each policy process of Hong Kong and Belgium can serve as a model for countries and regions in similar social contexts seeking to shift their psychiatric service delivery. In addition, there were several similarities in the strategies of 2 cases despite that they have different social contexts. These similarities in the strategies might be very important technical cues for various countries and regions adopting mental health reforms in the future. The next step would be a longitudinal qualitative study using both interview and documentary data.
Supplemental Material
sj-docx-1-his-10.1177_11786329231211777 – Supplemental material for Mental Health Reform Processes and Service Delivery Shift From the Hospital to the Community in Belgium and Hong Kong
Supplemental material, sj-docx-1-his-10.1177_11786329231211777 for Mental Health Reform Processes and Service Delivery Shift From the Hospital to the Community in Belgium and Hong Kong by Mina Honyashiki, Jeroen Decoster, William Tak Lam Lo, Taichi Shimazu, Kentaro Usuda and Daisuke Nishi in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329231211777 – Supplemental material for Mental Health Reform Processes and Service Delivery Shift From the Hospital to the Community in Belgium and Hong Kong
Supplemental material, sj-docx-2-his-10.1177_11786329231211777 for Mental Health Reform Processes and Service Delivery Shift From the Hospital to the Community in Belgium and Hong Kong by Mina Honyashiki, Jeroen Decoster, William Tak Lam Lo, Taichi Shimazu, Kentaro Usuda and Daisuke Nishi in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329231211777 – Supplemental material for Mental Health Reform Processes and Service Delivery Shift From the Hospital to the Community in Belgium and Hong Kong
Supplemental material, sj-docx-3-his-10.1177_11786329231211777 for Mental Health Reform Processes and Service Delivery Shift From the Hospital to the Community in Belgium and Hong Kong by Mina Honyashiki, Jeroen Decoster, William Tak Lam Lo, Taichi Shimazu, Kentaro Usuda and Daisuke Nishi in Health Services Insights
Footnotes
Acknowledgements
The authors would like to thank the local experts in Hong Kong (Mental Health Association of Hong Kong; Integrated Community Centre for Mental Wellness [Jockey Club Amity Place]; and Section of Community Psychiatry, Pamela Youde Nether Eastern Hospital) and in Belgium (Psychiatric Care Sint-Kamillus; Federal Public Service Health; and Zorgnet-Icuro). This study received guidance from the Japan Supportive, Palliative and Psychosocial Oncology Group (J-SUPPORT) funded by the National Cancer Center Research and Development Fund (30A-11; 2021-A-13) and the National Center Consortium in Implementation Science for Health Equity (N-EQUITY) funded by the Japan Health Research Promotion Bureau (JH) Research Fund (2019-[1]-4) and Project Fund (JHP2022-J-02).
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the National Center for Geriatrics and Gerontology to Institute of Mental Health, National Center of Neurology and Psychiatry ( JYU·KYOU 253) and Ministry of Education, Culture, Sports, Science and Technology (KAKENHI grant number 20K18897). The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
MH, JD, WTLL, and TS contributed to the conceptualization and design of the research. MH collected the data and drafted the manuscript. All authors reviewed the final version of the manuscript. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the concept.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.