
Abstract
Background:
In this study, the geniatric status of OECD (Organisation for Economic Co-operation and Development) countries was measured, and the effects of aging status on disease patterns in each country were quantitatively assessed. A theoretical model explaining the effects was suggested, and the implications were discussed.
Methods:
Data used in this study were the OECD Health Statistics data and WHO Global Burden of Disease data. The values for each country were paired with disability-adjusted life years (DALYs) presented by the WHO and Institute for Health Metrics and Evaluation (IHME). A cross-country panel analysis was conducted to analyze the effects of senility on the burden of disease in OECD countries.
Results:
Geniatric status had effects on the burden of disease (P = .048). Total health expenditure significantly reduced the burden of disease (P = .001). In the panel model with YLL (Year of Life Lost) as the outcome variable, geniatric status had twice greater effects on the burden of disease than that in the model with DALY (P = .003).
Conclusions:
In medical insurance-related policies, the characteristics of the disease should be considered. In particular, chronic diseases have not received much attention compared to their risk. However, the disease that actually affects the burden of disease is a disease that becomes chronic and requires long-term treatment rather than a disease with a high fatality rate. And, as a result of this study, the higher the level of resource consumption for treatment in OECD countries, where aging is progressing, the burden of disease was rather reduced. Therefore, if there is institutional support to receive appropriate treatment, it will be possible to reduce the national burden of disease.
Keywords
Introduction
From 1970 to 2018, South Korea showed the fastest rate of aging and lowest birth rate among the 37 countries of the Organisation for Economic Co-operation and Development (OECD). The Korea Economic Research Institute (KERI) reported an “international comparison of the trend of low fertility and aging and policy implications” and argued that mid- to long-term measures must be implemented to deal with the slowed growth and weakening of financial capacity caused by the low birth rate and geniatric population. 1 Korea became an “aging society” (elderly population over 7% of the total population) in 2000, and subsequently in 2018, it became an “aged society” (elderly population over 14% of the total population). The OECD predicted that Korea would become a “super-aged society” (elderly population over 20% of the total population) in 2026, only 8 years after becoming an aged society.1-3 This is expected to cause not only economic problems such as decrease in savings and investment rates, in quantity and quality of labor force, and in economic growth rate, but also a national financial crisis, including increased financial burden due to an increase in welfare expenses for the elderly population. 2 These concerns urge for adequate countermeasures and policies.
From the late 1960s, OECD countries began to experience changes in demographic structure. As life expectancy increases and the fertility rate decreases, the policy task of population aging has become a direct challenge. Population aging went beyond simple demographic changes, as a result of a decrease in the economically active population, a decrease in economic growth potential due to an increase in the burden of support for the elderly, and a decrease in fiscal revenue. On the other hand, the scale of financial expenditures on pension benefits, medical expenses for the elderly, and welfare services for the elderly increased significantly. Population geniatric affects the total amount of social welfare expenditure, including direct expenditures for senior citizens aged 65 and over, such as cash benefits, pensions, early retirement, and long-term care for the elderly, as well as indirect expenditures related to family benefits, medical care, and education including children. Accordingly, OECD countries have made efforts to establish various types of aging social security systems, making the issue of efficiently allocating resources while minimizing economic and social impact on the growing geniatric population a top priority for policy attention.2,3
Meanwhile, in developed countries including Korea, as a result of the rapid economic growth in the past, basic living has been stabilized, and interest in health has increased recently, resulting in increased consumption of health care products. Therefore, the health care industry is classified as an age-friendly industry where aging has a positive effect. In addition, in connection with the rapid development and spread of information and communication technology, innovation in medical technology is also rapidly progressing, and as the productivity of the medical field is greatly improved due to technological advances in the supply of medical products, the relative price of medical products is also decreasing. Despite the high share of the health care industry in the economy and the high public interest and the growing trend, studies on the economic level and aging population are poor.
While the pros and cons of the geniatric phenomenon are expected, the disease pattern of the elderly population is progressing in a pattern that consumes a lot of medical resources. As the world population is aging, the proportion of individuals with multiple chronic diseases are increasing. 4 In many OECD countries, adequate data showing the prevalence of multiple chronic diseases and medical expenses is not available. However, approximately 25% of the population has multiple chronic diseases (including hypertension, arthritis, dementia, chronic obstructive pulmonary disease, heart diseases, diabetes), and it is estimated that these patients use more than half of the total health care services.5-7
In this study, the geniatric status of OECD countries was measured, and the effects of geniatric status on disease patterns in each country were quantitatively assessed. A theoretical model explaining the effects was suggested, and the implications were discussed.
Materials and Methods
Data used in this study were the OECD Health Statistics data and WHO Global Burden of Disease data. The OECD Health Statistics data were used to analyze the effects of aging on the burden of disease from an international perspective. To assess the geniatric, economic level, and medical expenditure of each country, figures of population over 65 years of age, GDP, and medical insurance expenditure collected by OECD were used. Cross-country panel data by year were constructed through the OECD Statistics approach for analysis. 1 The data of 37 OECD countries were analyzed, and panel analysis was conducted using statistical data of each country from 2010 to 2019. The values for each country were paired with disability-adjusted life years (DALYs) presented by the WHO and Institute for Health Metrics and Evaluation (IHME) to evaluate the disease burden. The values of disease burden in 2011, 2012, 2015, 2016, and 2019 reported by the IHME were used. To compare the changes in disease burden according to changes in aging index, which is used as an international standard, geniatric index was calculated per year. The burden of disease was divided for early elderlies aged 65 to 69 and mid/late elderlies over the age of 70.
A cross-country panel analysis was conducted to analyze the effects of senility on the burden of disease in OECD countries. OECD Health Statistics data had missing values for each country, and thus, unbalanced data with time differences were used in this study. In addition, a panel analysis of OECD countries was conducted assuming a 2-factor fixed effect model. Cross-region and country panel data do not assess a part of the population. Thus, panel analysis of the fixed effects model is more appropriate than the random-effects model. 8 As OECD health statistics data was population-concept data for all OECD countries rather than sample data, a fixed effects model was applied. In addition, in previous studies that conducted cross-region and country panel analysis, 9 2-factor fixed effects models were used. The problem of endogeneity can occur in estimating the panel regression model. The Hausman test is conducted to solve the problem that endogeneity may occur between these explanatory variables and individual effects. If the null hypothesis cannot be rejected according to the results of the Hausman test, the random effect model is used because there are no explanatory variables and endogeneity problems. If the null hypothesis is rejected, the fixed effects model should be used. As a result, the fixed effect was found to be appropriate, and the characteristics of 37 OECD member countries were treated as dummy variables to control the fixed effect (unique characteristics) of each country. In this study, a 2-factor fixed effects model was assumed to control the characteristics of individual effects and time effects by year in OECD countries. In other words, it was assumed that there were common variables that may affect the burden of disease but were not measured in OECD countries and that there were other variables that may have common effects in each country as they change over time. Thus, a 2-factor fixed effects model was used. Then, a regression analysis was performed using the PCSE (panel corrected standard errors) technique, which provides a correction error considering heteroscedasticity, co-correlation between groups, and auto-correlation. The PCSE (panel corrected standard error) model can alleviate the problem of simultaneous autocorrelation and heteroscedasticity by considering correlation within a panel and heteroscedasticity between panels. This PCSE model has the advantage of enabling a more accurate measurement of the error or result of the analysis compared to the general regression analysis. On the other hand, since the PCSE model does not solve the problem of omitted variables, it is intended to derive analytical implications by supplementing it through a fixed-effects model. SAS 9.4 program (SAS Institute Inc., Cary, NC, USA) was used for panel analysis, and SAS PROC PANEL is a tool developed for the purpose of panel data analysis. A P-value of less than .05 was considered statistically significant. Outcome variables were DALY and years of life lost (YLL), and 2 models were established for each disease burden outcome. For explanatory variables, GDP and national medical expenditure levels were considered as variables for correction. To understand the effects of geniatric, early and mid/late elderly groups were set as major variables. The panel model established in this study is shown in Table 1.
Description of variables.

Results
Here, using OECD’s data on aging and WHO’s disease burden data, changes in disease burden according to the level of medical infrastructure (Gross domestic product, medical technology, medical support) compared to the aging index were analyzed. The disease structure is important for understanding the health status and disease pattern of a specific population group, and the structure is not fixed and can change over time. Changes in the disease structure are closely related to economic development, because an increase in income level leads to improvement in living environment and sanitation, and improvement in national nutrition. Using this longitudinal data approach, this study intended to analyze the net effects of the geniatric by quantitatively analyzing the differences in the burden of disease by aging while controlling for differences in national medical levels and economic conditions.
The mean, standard deviation, and frequency of variables input to the panel model were analyzed to compare the 10-year mean of OECD countries. The results are shown in Table 2. The mean DALY and YLL, which were the outcome variables, were 2712 and 1123, respectively.
Basic statistics of OECD member countries.
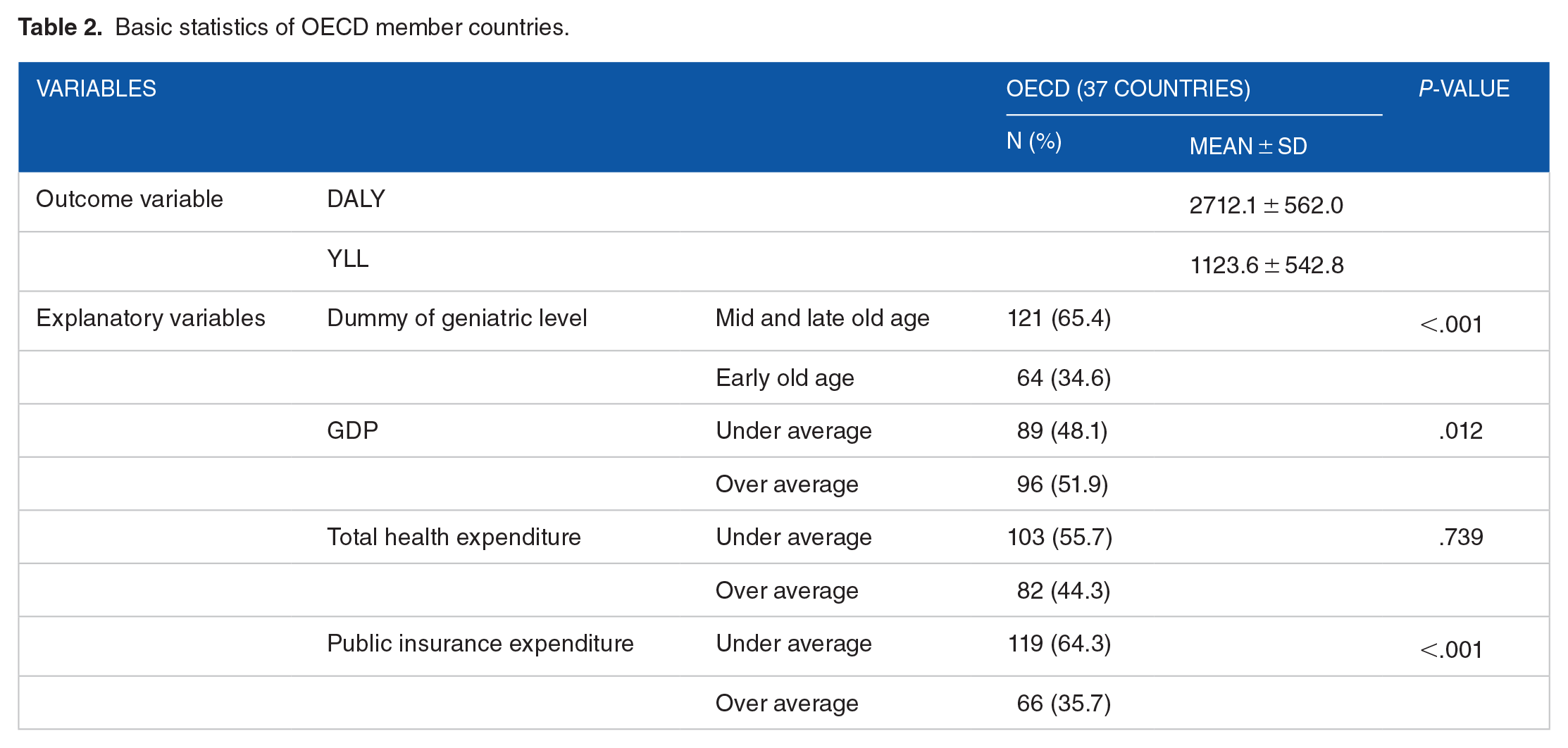
The number of OECD countries analyzed was 37, and the total number of samples is 185 because each of these 5-year data was identified as analysis data. Approximately 65.4% of all OECD countries entered mid/late aging, and 34.6% were in the early aging group. GDP was measured as the economic level of a country, that has significant effects on investment in health care. Approximately 51.9% of countries had above-average income while 48.1% had below-average income. For expenditure on the national health care system and medical expenses, 55.7% had a below-average low expenditure, and 44.3% showed high expenditure. Among them, 35.7% showed above-average public insurance expenditure.
In panel analysis with DALY as the outcome variable, geniatric status had effects on the burden of disease (P = .048). As the geniatric index increased, the value of Disability adjusted life year increased by 2.13 times. In contrast, total health expenditure significantly reduced the burden of disease (−1.02, P = .001). In other words, it was analyzed that the more the country spends on health care, the more the disease burden decreases by 1.02 times. In the panel model with YLL as the outcome variable, As the geniatric index increased and the society moved to a later aging society, the Year of Life Lost was 4.11 times higher (P = .003), which was twice as high as the value on the total burden of disease (DALY). That is, the value that is more affected by the level of geniatric was analyzed as the burden of disease due to death. However, GDP, national health expenditure level, and public insurance expenditure did not significantly affect the burden of disease due to death. Overall, the burden of disease, measured by morbidity and death, was influenced by the level of geniatric as well as the cost of medical expenses used for treatment. However, when looking at death alone, expenditure on medical resources other than the geniatric level had no effect (Table 3).
Panel analysis results for burden of disease.

Discussion
In 2018, Korea has already become an aged society with the elderlies over the age of 65 accounting for more than 14% of the total population. In 2026, it is expected that Korea will enter a super-aged society with the elderlies accounting for more than 20% of the total population.1-4 Aging does not simply indicate an arithmetic increase in the elderly population, but is associated with various social changes. Expected changes include an increase in chronic disease among the elderly and a resulting increase in the use of medical services.10-14 In 2017, in Korea, the cost of health insurance treatment for elderlies over the age of 65 was 27.1 trillion won, accounting for 39% of the total health insurance expenditure of 69.6 trillion won. This has increased by 12-fold from 2.3 trillion won in 2000, and the share of total health expenditure has increased by more than double from 17.5% in 2000. 15 The rate of increase in medical resource consumption is more rapid than the increase in the elderly population.
Here, to analyze the effects of geniatric on the burden of disease, a panel analysis was conducted by combining OECD Health Statistics data and IHME Disease Burden data from 2010 to 2019. The outcome variables of the panel model were DALY and YLL, and changes according to the geniatric of OECD countries were assessed. Unlike previous studies that vaguely predicted that the elderly would use more medical services and have a high disease burden due to poor health, this study is meaningful in that it quantitatively analyzed whether the main cause of the increase in disease burden was disease or death, using a 2-factor fixed effects model. As geniatric status has changed over the past decade in OECD countries, mid/late aging society showed 2.13 times greater DALY, which included both prevalence and death, than early aging society. On the other hand, YLL was 4.11-fold greater in mid/late aging society than in early aging society, suggesting that the increase in the burden of disease due to aging was mainly affected by death. These effects lead to catastrophic medical expenses at the end of lives, increasing the burden on the health care system.
We also expected that this increase in the burden of disease would change according to the national economic level or public health expenditure such as social insurance and tax support. Thus, changes in the burden of disease according to GDP, national medical expenditure, and government medical expenditure were analyzed. As national medical expenditure increased, DALY rather decreased. As this study analyzed panel data of OECD countries, it was thought that developed countries had well-established health care system infrastructures. Thus, national medical expenditure improved health and subsequently increased healthy lifespan, reducing the burden of disease.16,17
In Korea, the baby boomers reached the age of 65 as of 2020, and there is an increasing demand to reform the health care system for the geniatric society. 18 Health care policies must focus on improving the functional ability of the elderly in the aging society, and health care must be converted to integrated older person-centered health services.18,19 Subsequently, education and training of health and medical personnel must be adequately provided. Health care and long-term care must be strongly linked, and an elderly-friendly environment must be established. In addition, monitoring of elderlies should be strengthened. Elderly-centered integrated medical care should be introduced into the national health insurance system for the convenience of elderlies. As the demographic structure and health care environment change, the needs of care are changing. Therefore, service innovation is necessary. For example, people with multiple chronic diseases have a high desire for integrated care of medical and social services. The elderly, whose function declines due to aging, increases their desire for recovery and rehabilitation services after acute treatment. Develop new services to respond to these changes, promote policies to ensure that necessary services are provided as close as possible after acute treatment, reduce the severity of diseases by establishing an organization that supports integrated care, and eliminate catastrophic medical expenses. It is also time to consider reinforcing the system so that it can face death. In particular, at a time when the Korean government expands medical coverage and introduces community care promotion policies, a financial strategy to increase efficiency and system reform for integrated care are required.
Conclusion
This study examined how the scale of disease burden and the number of years lost due to death (YLL) vary according to the level of aging. Previous studies have somewhat vaguely predicted that the elderly will use more medical services because of their poor health, and that the burden of disease will be high. However, this study is meaningful in that the major causes of the increase in the burden of disease are classified as morbidity or death and included in the research model. Based on these results, I would like to propose the following policy-wise. In medical insurance-related policies, the characteristics of the disease should be considered. In particular, chronic diseases have not received much attention compared to their risk. Diseases (eg, high blood pressure or arthritis), which are not usually considered expensive for diagnosis or treatment, are classified as non-fatal diseases compared to cancer or stroke, and are excluded from the government’s policy to strengthen insurance coverage. However, the disease that actually affects the burden of disease is a disease that becomes chronic and requires long-term treatment rather than a disease with a high fatality rate. As a result of this study, the higher the level of resource consumption for treatment in OECD countries, where aging is progressing, the burden of disease was rather reduced. Therefore, if there is institutional support to receive appropriate treatment, it will be possible to reduce the national burden of disease.
This paper has been analyzed based on many assumptions. This is because secondary data is not data collected for a purpose, so operational definitions are often given. It is difficult to generalize the results because the country’s level of advancement was identified as the level of GDP, and the analysis was conducted without distinguishing specific health care systems such as the NHS or NHI. Nevertheless, it is considered a contributing point to analyze the impact of aging on disease burden by country’s GDP level using panel data.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2021R1A2C1091686).
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
EJ analyzed and interpreted the patient data and the transplant. HS was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of National Evidence-based Healthcare Collaborating Agency (IRB No. NECA IRB21-020-5). This study used the National Health Information Database of the National Health Insurance Service (NHIS-2021-1-199).
Availability of Data and Materials
The datasets analyzed during the current study are not publicly available due to information security law of Korea but are available from the corresponding author on reasonable request.