
Abstract
Background:
Most publicly-funded health systems purchase healthcare from private providers, but the optimal purchasing arrangements between public purchasers and private healthcare providers are yet to be determined.
Objective:
This study compares the healthcare purchasing arrangements made with private providers in 2 social health insurance (SHI)-based systems to identify factors that influence the prices paid for private healthcare service provision.
Results:
France and Japan use different approaches to determine the payment arrangements with public and private providers. The presence of for-profit healthcare providers in the French health system explains the different payment rates for public and private healthcare providers in that country. In both France and Japan, in addition to payment rates, several policy tools are used to assure the provision of public good services and the availability of necessary healthcare for all, which public providers are required to deliver but private providers can choose to deliver.
Conclusion:
This study highlights the importance of considering the profit-making status of the private healthcare providers operating in the healthcare market, and clarity in the roles and responsibilities of the public, for-profit and not-for-profit providers when determining healthcare purchasing arrangements. Regulatory policy instruments, used alongside payment rates, are essential to influence efficiency, equity, and quality in mixed (public-private) health systems.
Background
Many countries undertake continuous reform of their health financing systems to make healthcare more accessible to the entire population and ensure the efficient use of healthcare resources. Most health systems include a mix of public and private healthcare providers however, the role and significance of private healthcare providers in a health system can vary depending on the health system’s history and institutional characteristics. 1 The extent to which publicly-funded health systems should rely on private providers, and the funding of private providers to ensure quality, equity and efficiency in health systems are topics of ongoing debate among policymakers and researchers. 2 Some argue that purchasing private healthcare under publicly-funded systems may optimize the use of public health resources by increasing the availability of healthcare services to meet healthcare needs. 1
However, in healthcare markets where a mix of public and private providers operate simultaneously and market failure can occur, strong public governance is required to ensure that needed healthcare services are available and accessible to all. 1 Private healthcare purchasing can operate under different types of publicly-funded health financing models including: (1) mandatory health insurance systems that purchase healthcare services from public and private healthcare providers; and (2) tax-based systems that contract selected private healthcare providers alongside publicly-funded healthcare services. 3 The optimal structure of the purchasing arrangements with private healthcare providers should encourage private providers to contribute to the objectives of the publicly-funded system when providing services and to improving the health system’s performance. 4
Payment rates are an important lever in healthcare purchasing arrangements and can impact on efficiency, equity, and quality in healthcare service delivery by sending incentive signals to providers that can change their behavior. 4 Payment rates that are too low or too high can have negative consequences on service delivery and health system performance. For example, fee-for-service payment rates that are above the marginal cost of service delivery can result in an over-supply of services, leading to an inefficient use of resources. 5 Low payment rates can make providers reluctant to participate in the health system or to shift risk and costs to patients by charging them additional fees (when allowed), which can result in inequitable access to healthcare services. 6 Payment rates which do not reflect the cost of supplying services can reduce the incentive for healthcare providers to provide high quality services. 7 Consequently, it is important for public purchasers to carefully design the payment rates they offer to healthcare providers.
Payment rates can differ depending on the ownership status of providers, that is, public, private not-for-profit, for-profit. 8 Various factors affect the design of payment rates for public and private healthcare providers, including the regulatory environment, the characteristics of purchasers and providers (eg, negotiating power, provider autonomy, and the authority given to purchasers, etc.), the shared roles and responsibilities of public and private healthcare providers, and differences in service delivery costs.9,10 Health systems can be negatively affected by unjustified discrepancies in payment rates for public and private healthcare providers. For example, higher prices paid to private providers compared to public providers can attract private providers to the market. However, this can also increase public healthcare expenditure by inducing more demand and causing unnecessary costs for the public purchaser. 11 Conversely, low payment rates may result in patient selection wherein private providers focus on the most profitable patients (elective, non-complicated cases), which shifts more the costly cases to public providers. 12 Furthermore, different payment arrangements for public and private providers can result in inefficiencies due to the additional administrative costs required to run multiple payment systems. There have been arguments over whether private providers should have the same payment rates as public providers under the tax-funded system. 10 However, limited research has explored the details of the purchasing arrangements for private providers under mandatory health insurance systems. 4
This study compares the health systems in France and Japan to: (1) examine how public purchasers use purchasing arrangements when procuring health services from public and private healthcare providers; and (2) identify factors influencing service price setting for providers with different ownership statuses. The health systems in France and Japan are based on social health insurance (SHI) which uses multiple, non-competing plans that cover different groups in the population. In both countries, private providers are highly present in the health system, and SHI purchases from both public and private healthcare providers using a range of purchasing arrangements. This paper provides insights into the purchasing arrangements operating between public purchasers and private healthcare providers in publicly-funded health systems and identifies underlying factors which may explain the differences in the purchasing arrangements used with public and private providers.
Methods
Framework for comparison
A common framework was used to collect and analyze policy information from France and Japan (Figure 1). To address the first objective of the study, the purchasing arrangements between public purchasers (eg, government, statutory health insurance funds) and healthcare providers were described according to: (1) payment rates and methods for outpatient and inpatient care delivered by public and private providers, (2) benefit packages available under the publicly-funded system, and (3) registration processes and mechanisms for contracting public and private healthcare providers.

Framework for comparison.
Subsequently, underlying factors which may explain the differences in purchasing arrangements were examined. The price paid for healthcare services by purchasers should reflect the actual costs of providing services, which can vary depending on the ownership status of healthcare providers. Mason et al 9 argued that regulatory factors and the processes involved in producing healthcare services can influence the cost of supplying services. In addition, Waters and Hussey indicates that characteristics of providers can also influence how purchasers pay for health services. Consequently, this study looks at: (1) each country’s health financing system and healthcare market which characterize healthcare providers with different ownerships, (2) regulations for healthcare purchasing, and (3) the production process for the delivery of healthcare services. 10
Factors in the healthcare financing system and market structure that may affect the purchasing arrangements include: (1) features of the country’s healthcare financing mechanism, including population coverage by various funding pools and the market shares of public and private financing schemes; (2) the shares of the healthcare market held by public and private providers, and the types of private healthcare providers in the market (ie, not-for-profit and for-profit); and (3) the specific roles and responsibilities of public and private healthcare providers (including the provision of public health services). 13
Regulatory factors that can influence payment arrangements include: (1) the level of autonomy held by public and private healthcare providers (ie, day-to-day management decision-making power given to providers 14 ), (2) differences in taxation rates for public and private healthcare providers, including both direct taxes (eg, corporation tax on profits) and indirect taxes (eg, VAT on contracted services), and (3) the extent to which accountability is addressed, including monitoring and performance requirements for public and private healthcare providers.
There may be differences in the cost of healthcare service delivery for public and private healthcare providers, which can influence the prices paid to providers. 10 Factors affecting the cost of healthcare services production include: (1) capital costs—differences between public and private providers in terms of access to finance for capital and maintenance of capital assets; (2) labor costs—differences in the cost of human resources for public and private providers; (3) geographical variations in input prices—service delivery costs in different parts of the country and the impacts of costs on payment rates for services; (4) access to cheaper inputs—differences between public and private healthcare providers in the procurement of pharmaceutical and other medical consumables; (5) the contribution and cost of public and private healthcare providers in emergency care, R&D, and teaching and training; and (6) case-mix—the type of care provided to patients.
Data Collection and Analysis
A case study approach 15 was used to examine the arrangements between purchasers and providers with different ownership statuses but operating within publicly-funded healthcare systems. The French and Japanese health systems were selected for the study after considering the provider mix and payment arrangements with public and private healthcare providers in the countries. Both health systems are based on mandatory health insurance, and the markets include a large proportion of private providers (private hospitals account for 55% of total hospitals in France, and 81% in Japan). Nevertheless, there are notable differences in the payment arrangements made by public purchasers with public and private healthcare providers. While the Japanese mandatory health insurance system uses the same arrangements for public and private providers, there are some differences in payment arrangements for public and private providers under the French mandatory health insurance system (Table 1). The study used a multiple case study design to compare the payment arrangements made with private providers under publicly-funded systems, hypothesizing that 3 categories of factors—the healthcare financing context, regulation, and the service production process—affect the payment arrangements made with providers.
Factors considered in the selection of study countries.
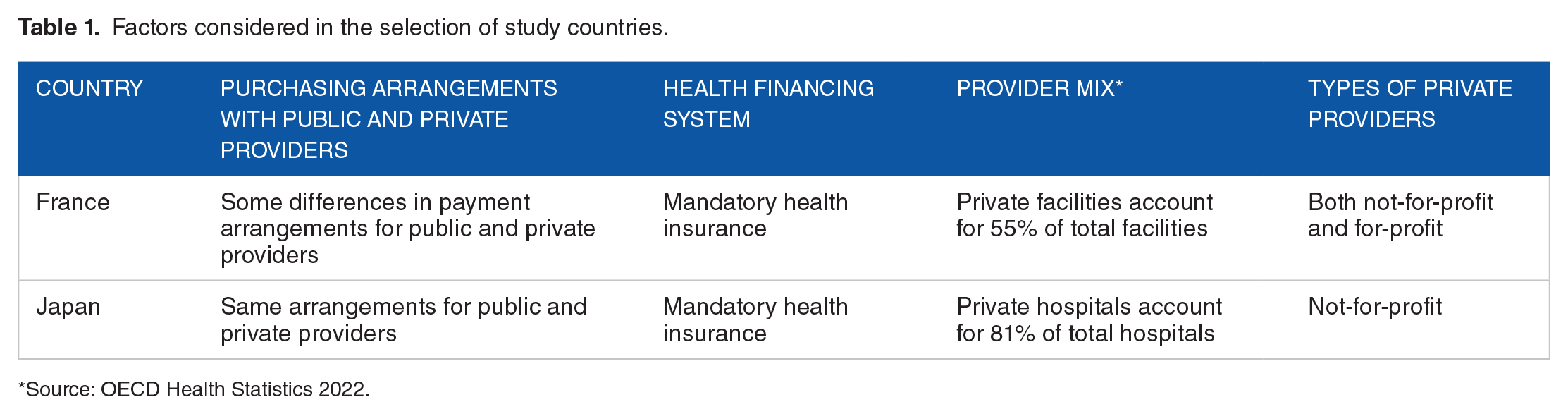
Source: OECD Health Statistics 2022.
The comparative framework presented above guided the collection and comparison of policy information from France and Japan. The information was gathered through a review of policy documentation, academic articles, and gray literature, using a standard template for collecting information on the French and Japanese health systems. A framework approach that uses a pre-determined themes based on the comparative framework was used for analysis.
Results
Table 2 compares the purchasing arrangements made between public purchasers and public and private healthcare providers in France and Japan. In both countries, SHI mostly applies the same payment methods to both public and private healthcare providers. Both countries use fee-for-service (FFS) payments for outpatient care. The French SHI uses case-based payment for hospital care, 16 and the Japanese SHI uses a combination of FFS and case-based per diem payments. 17
Purchasing arrangements, including payment rates, under the publicly funded systems in France and Japan.

The same arrangements are applicable to both public and private healthcare providers unless specified otherwise
The payment method varies for public and private healthcare providers in some areas. For example, private psychiatric hospitals are paid using FFS, while public psychiatric hospitals are provided with a global budget.
DPC-PDPS was introduced in 2003 and, as of 2022, is used in 1764 hospitals (85% of total general hospital beds in the country).
The French SHI contracts Sector 1 and Sector 2 physicians. Sector 1 physicians use the nationally negotiated fee schedule, Sector 2 physicians, who are required to have specified qualifications and experience, can charge more than the regulated fees.
In Japan, a uniform standard fee schedule for FFS and the same case-based per diem payment rates are applied to both public and private healthcare providers. 17 In France, for hospital care, different rates are applied and different factors are used to calculate payment rates for public and not-for-profit private healthcare providers and for-profit private healthcare providers. 16 Specifically, in France, the case-based payment rates at public and not-for-profit private hospitals are determined by total direct and indirect costs. Furthermore, rates for for-profit private hospitals exclude medical fees paid to doctors, the cost of pathology tests, and imaging examinations, which SHI separately pays.
Healthcare providers in Japan are prohibited from practicing balance billing. 18 In contrast, “Sector 2” health professionals in France, who are qualified based on level and experience, are allowed to undertake balance-billing. In 2019, 48% of specialists and 6% of general practitioners were registered as in Sector 2 providers. 19 The “Controlled Tariff Option” (Option de Pratique Tarifaire Maîtrisée: OPTAM), a new annual and optional contract to regulate the prices charged by Sector 2 physicians 16 was recently introduced in response to the situation where some physicians, primarily specialists in for-profit private healthcare facilities and ambulatory care practices, charged higher than regulated fees for services.
In France and Japan, public and private healthcare providers have the same registration processes, contracts, and benefit packages.20,21 In Japan, public health services are not included in the SHI benefit package but are mainly delivered through other public arrangements, while in France, the SHI covers most public health services (including immunization).
Table 3 provides information on the healthcare financing models and the public-private mix of healthcare providers in France and Japan. SHI is both countries’ major healthcare financing system. However, large proportions of the population purchase complementary private health insurance (CHI), that enables them to avoid financial burden by cost-sharing with SHI (eg, co-payments). In France, approximately 96% of the population had CHI in 2019 22 ; and in Japan, 71% of the population had CHI in 2017. In Japan, CHI mainly provides lump-sum cash payments for hospitalization or severe illness, and insurance products are often sold as part of life insurance packages. 23 In Japan, the government sets a maximum monthly co-payment per household which is based on household income. An insured person can claim the costs of medical care from SHI if the total monthly co-payments exceeds the set cap. 24 There is no such cap in France and most health services, including hospital care, require those receiving care to cost-share, but costs are usually covered by the CHI.
Healthcare financing and the public and private mix of healthcare providers.
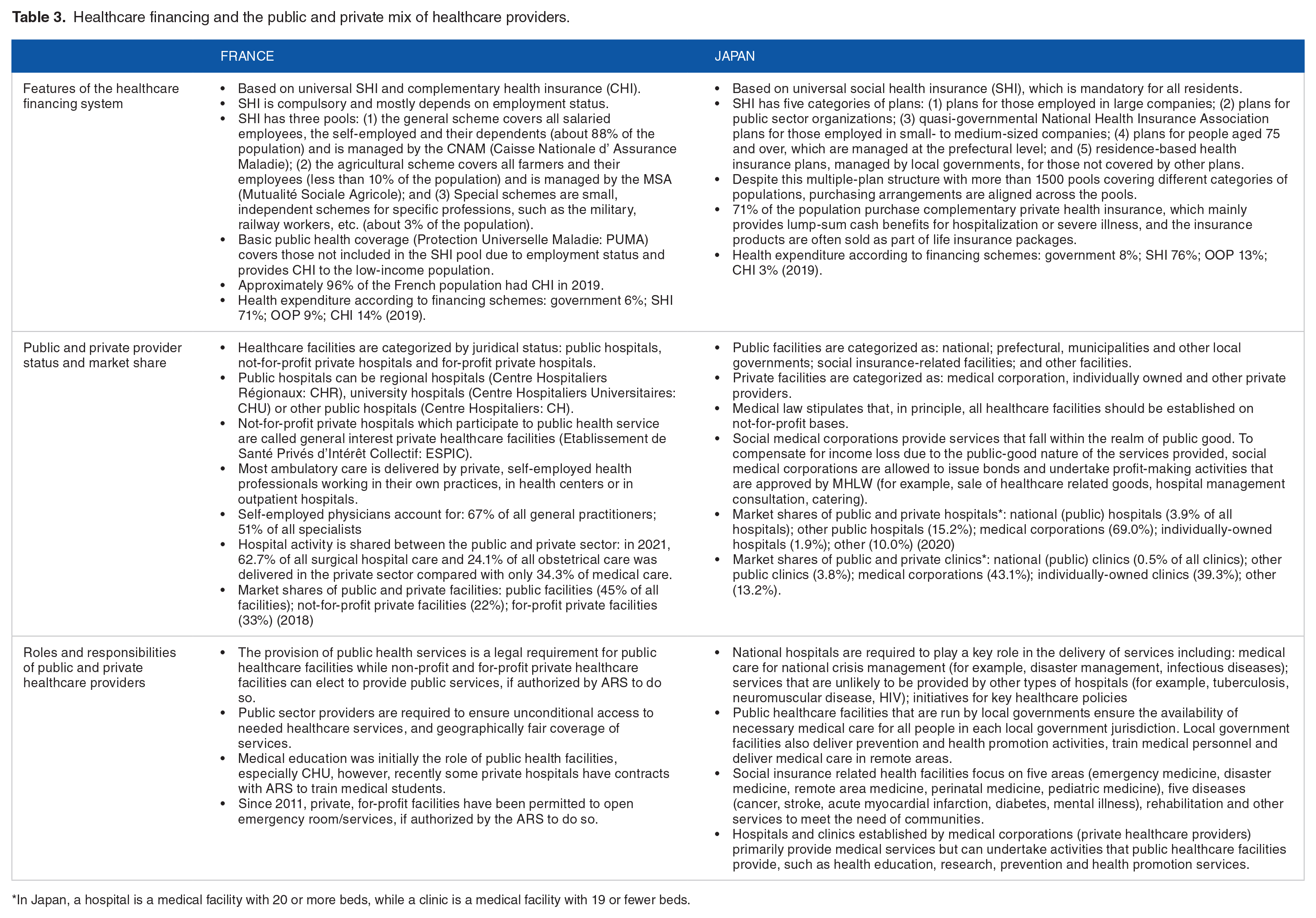
In Japan, a hospital is a medical facility with 20 or more beds, while a clinic is a medical facility with 19 or fewer beds.
In both France and Japan, SHI purchases healthcare services from public and private healthcare providers. Public healthcare facilities in both countries provide public good healthcare services and ensure the availability of needed healthcare services for all. In contrast, private healthcare facilities can choose the services and the level of service that they provide.25,26
In France, healthcare facilities are categorized as: public hospitals, not-for-profit private hospitals, and for-profit private hospitals. Not-for-profit private hospitals which participate in public health service delivery are called general interest private healthcare facilities (Etablissement de Santé Privés d’Intérêt Collectif: ESPIC). Public hospitals can be regional hospitals (Centre Hospitaliers Régionaux: CHR), university hospitals (Centre Hospitaliers Universitaires: CHU) or other public hospitals (Centre Hospitaliers: CH). 25 Most ambulatory care is delivered by private, self-employed health professionals who work in their own practices in health centers or outpatient hospitals. 21 Hospital activity in France is shared between the public and private sectors. In 2021, 63% of all surgical hospital care was conducted in private hospitals, compared with only 34% of medical care and 24% of obstetrical care. 25
In Japan, public facilities are categorized as: national, prefectural, municipal, or other local government facilities, social insurance-related facilities, and other facilities. 27 Private facilities include medical corporations, privately-owned, and other private providers. Japanese medical law stipulates that, in principle, all healthcare facilities should operate on a not-for-profit basis and dividends of surplus are prohibited.28,29 A category of Japanese medical corporations called “social medical corporations,” which are not-for-profit by law, provide public good healthcare services, for example, emergency medicine, medical care in disasters, medical care in remote areas, and pediatric emergency care. Social medical corporations are permitted to issue bonds and engage in profit-making activities (eg, the sale of healthcare-related goods, consultation, and catering services) that are approved by the Ministry of Health, Labor and Welfare (MHLW) to compensate for income losses due to the public-good nature of the services provided. 30 Hospital facilities in Japan comprise: national hospitals (3.9%); other public hospitals (15.2%); medical corporations (69.0%); privately-owned hospitals (1.9%); other (10.0%), and public and private clinics comprise: national clinics (0.5%), other public clinics (3.8%), medical corporations (43.1%), privately-owned clinics (39.3%), and other (13.2%). 27 In Japan, a hospital is a medical facility with 20 or more beds, while a clinic is a medical facility with 19 or fewer beds.
Table 4 presents the regulatory factors associated with the operation of public and private healthcare providers in France and Japan. In France, public healthcare facilities have limited autonomy. 31 The Ministry of Health appoints public hospital directors, but the directors have limited decision-making authority. The government determines the wages bill and services provided by public facilities. In Japan, public healthcare providers are financially independent; however, government subsidies cover losses in delivery of services relating to (1) geographical disadvantage, (2) unprofitable but public health priority services, (3) use of highly advanced medical technologies, (4) deployment of doctors and nurses, (5) the redemption of principal and interest, and (6) other selected activities. 26 In Japan, the Medical Care Act provides the standards for the number of medical personnel allocated in hospitals and clinics with medical care beds, which links to fee-for-service payment rates. 32 In some cases, prefectural Governors have the authority to decide on the services provided by public hospitals to ensure that services align with regional public health policies and priorities. 26
Regulatory factors in the operation of public and private healthcare providers.

Social medical corporation are health facilities that provide public good healthcare services (eg, emergency medicine, medical care in disaster, medical care in remote areas, pediatric emergency care, etc.), in addition to normal healthcare services, and offer an alternative to public healthcare facilities.
In France, public and private healthcare providers are exempt from corporate and value-added taxes (VAT). In Japan, public providers are exempt from corporate and local taxes, while private providers are not exempt, except for social medical corporations, which are partially exempt. 26 In France, health professionals with SHI contracts who charge the standard fee schedule are known as “Sector 1” contractors. Sector 1 health professionals receive social benefit contributions, including health insurance and age pension payments, from the SHI fund. 16 As mentioned, “Sector 2” contractors are allowed to undertake balance billing; however, they must pay their own age pension payments and insurance coverage. Demand to work as Sector 2 contractors is high and access to Sector 2 registration has been restricted since 1990; each year, only 1000 new doctors are accepted to work in Sector 2. 16
Regarding accountability, in France, Regional Health Agencies (Agence Régionale de Santé: ARS) negotiate multi-year agreements with healthcare facilities to define the activity and quality targets that correspond to the allocated resources (Contrat Pluriannuel d’ Objectifs et de Moyens—CPOM). Healthcare facilities are required to report to ARS on progress against targets. 21 The same arrangements are applied to public and private healthcare providers, and ARS has the right to audit the financial accounts of both public and private providers. However, private health facilities are not mandated to provide financial accounts to ARS so their agreements are less stringent than those with public providers. All hospitals and clinics with care beds in Japan must submit service utilization reports to MHLW through public health centers and prefectural governments. In addition, the Medical Care Act holds medical corporations financially accountable to the public via annual business reports that are submitted to prefectural governments. 33
Factors relating to the delivery of healthcare services are presented in Table 5. In both France and Japan, private providers have access to various sources of finance for capital investment. In France, case-based payment rates partly cover the cost of investment in public hospitals, while the Regional Health Agencies can finance capital expenditure for targeted investments to improve quality or access to care in public and private facilities. 34 In Japan, multiple government funding schemes support all types of healthcare providers in the construction of new buildings, refurbishment of healthcare facilities, and purchase of medical equipment. However, such funding is usually limited for use in purposes that contribute to the public good. 35
Production factors in the delivery of healthcare services.

In France, staff employed by public health facilities are civil servants whose wages are regulated in accordance with the national salary scale. 36 Health providers in private facilities are employees under the private labor code and employed using a labor agreement. 37 However, labor agreements for not-for-profit and for-profit providers are different. In Japan, staff at local government hospitals are local government workers and their salaries are determined using the salary scales of local government workers but paid by healthcare facilities. Staff at other public hospitals are employees of the facilities, with some exceptions, and paid by healthcare facilities using the government worker salary scale.
In France, payment rates for providers are not adjusted for geographical variations in input costs, except in Paris, Corsica, and overseas departments and territories, which apply a multiplier to case-based payment rates. In addition, overseas departments and territories use higher FFS rates for physicians than mainland France. 38 In Japan, uniform payment rates are applied to all geographical locations due to the potential for different levels of contributions by the insured according to location of residence and the level of expenditure by insurers according to location. 39 For example, under the Japanese SHI, non-employment-based plans are run by local governments. If higher payment rates are applied to some geographical regions, the local government purchaser may incur higher expenditures than purchasers in other regions and, as a result, may have to increase the contribution rates from members to cover expenditures. However, additional funding is allocated for services provided by health facilities in locations that MHLW designates as having a limited number of healthcare providers, and government subsidies are available to health facilities in remote areas. 40
In France and Japan, product suppliers and healthcare facilities individually negotiate the prices of medicines and medical consumables.16,41 Price negotiations are based on purchase volume, delivery costs, payment terms, and credit status. Consequently, there is no difference in the arrangements for public and private healthcare providers in the purchase of medicines and consumables.
Public providers in France and Japan are mandated to provide emergency care, R&D, teaching and training services. Private providers can undertake these activities after gaining approval from relevant government authorities. 16 In France, emergency care is paid via annual fixed grants and an FFS component that considers providers’ annual activity, and teaching, training and R&D are paid using annual grants. 16
In terms of case-mix, in France, due to the legal obligation to deliver public health services, public institutions cannot select patients, consequently, serve more of the underprivileged population than private providers, which are able to select patients. Therefore, public hospitals ensure access to some complex treatments, including HIV, burns, and multiple trauma, while private hospitals mainly provide elective surgery. 42 Public healthcare facilities in Japan are required to provide public good health services and ensure everyone has access to necessary services. Different types of public providers have slightly different mandates; for example, national hospitals deliver initiatives aligned with key government healthcare policies. 26 The separate mandates can result in different case mixes for public and private healthcare providers, and for public healthcare providers operating at different levels. Public hospitals in Japan are larger than private hospitals. The average number of beds per hospital are 390 for national hospitals; 257 for local government hospitals; 147 for medical corporations; and 93 for privately-owned hospitals. Public providers deliver more services that require advanced medical infrastructure (eg, public providers deliver 78% of pediatric intensive care and 68% of radiotherapy). 27
Discussion
The health systems in France and Japan are based on SHI, which purchases healthcare services from public and private healthcare providers. The payment methods, benefit packages, registration processes and monitoring systems are similar for public and private healthcare providers in France and Japan but there are differences in the payment arrangements in each country. In Japan, a uniform fee schedule applies to both public and private healthcare providers. However, in France, there are different case-based payment rates for public and not-for-profit private healthcare providers, and for-profit private providers. Case-based payment rates in France are lower for for-profit private providers partly because they are based on historical costs. In addition, some cost items relating to services for public health and research are paid separately to public facilities by SHI. In France, certain categories of health professionals are allowed to undertake balance billing, which is prohibited in Japan.
A key factor influencing the payment arrangements between public and private healthcare providers is the types of healthcare providers operating in the health system. In France, private healthcare facilities can operate as for-profit organizations, while in Japan, medical law requires all healthcare facilities to be established on a not-for-profit basis. In France, there is a higher proportion of self-employed health professionals than in Japan.21,27 These self-employed health professionals, mostly specialists, are likely to work in for-profit private facilities and are allowed to undertake balance billing in exchange for the loss of social security benefits (Sector 2 professionals). In Japan, the financial autonomy given to public hospitals, the not-for-profit nature of private providers, and lack of differences in access to inputs for healthcare service production can justify the use of uniform payment rates for public and private healthcare providers.
Public providers in France and Japan are required to deliver public good healthcare services. These services are either paid for directly or subsidized by the government or regulatory tool (eg, taxation). As the results indicate, in France, public hospitals have a legal obligation to provide public health services and ensure continuity of care, including 24-hour emergency care, which is paid for using an annual fixed grant and an FFS component that considers the annual activity of providers. In Japan, public healthcare facilities play a key role in ensuring the availability of necessary medical care for all people, training of medical personnel and provision of medical care in remote areas. Government subsidies cover losses incurred due to the delivery of unprofitable services in areas of public health priority.
Private providers in both countries can choose to participate in the delivery of public services. For example, both for-profit and non-profit private healthcare providers in France can open emergency services with ARS authorization and, if private providers deliver public services, they are subject to the same arrangements as public healthcare providers. In Japan, private facilities run by “social medical corporations” provide public good healthcare services in addition to regular healthcare services. Rather than using payment rates, the government compensates for potential losses incurred when delivering public good services using regulatory levers, such as partial tax exemptions for social medical corporations, bond issuances, and additional income-generating activities that are approved by MHLW.
This study provides a systematic comparison of the insurance-based healthcare systems in France and Japan. Each country’s health system is complex, and examining the healthcare purchasing arrangements requires significant scrutiny, making it difficult to compare many countries simultaneously. However, further investigation of healthcare purchasing from private healthcare providers in different country settings is necessary to gain context-specific implications. Comparison of different health systems, such as SHI-based and tax-based systems, or countries with parallel, mixed financing mechanisms may provide further insight on additional factors to be considered in designing payment rates for public and private healthcare providers. In addition, this study only considered the purchasing arrangements between public purchasers and healthcare providers. It did not look at the influence of private health insurance on purchasing arrangements. With the recent attention given to the role of private health insurance in various health systems, 43 it is important to further investigate the potential impact of private health insurance on the payment rates established between public purchasers and private and public health providers.
While this study is a qualitative, comparative health policy analysis, some of the issues identified in the comparative analysis need to be further investigated using a quantitative approach from a health system performance perspective, for example, efficiency in healthcare service provision, quality of healthcare services, equity in healthcare access, etc. Finally, this study looked at the static nature of healthcare purchasing policies. However, in practice, payment arrangements between public purchasers and providers can be greatly influenced by the power dynamics of the stakeholders involved in healthcare purchasing. Consequently, it is imperative to examine the process of designing and revising payment rates and the engagement of relevant stakeholders from a political economy perspective.
Conclusions
This study compared the purchasing arrangements for providers with different ownership status which operate under SHI systems in France and Japan to identify factors influencing the payment arrangements for public and private healthcare providers. While there are differences in payment rates and arrangements with private healthcare providers in the 2 health systems, there are also notable similarities in the roles and responsibilities of public providers. Key factors influencing the payment arrangements for public and private healthcare providers are the presence of for-profit healthcare facilities and the proportion of self-employed health professionals of different categories that operate in the health system. In addition, public providers in both countries provide public good healthcare services and ensure the availability of necessary healthcare for all. The providers are supported by policy tools other than payment rates to promote the delivery of these services. There is homogeneity among the healthcare providers in Japan, not just in terms of ownership status (all providers are non-profit) but also in the managerial autonomy and access to inputs for healthcare production that are given to healthcare providers. This explains the uniform payment rates for public and private healthcare providers. France has a more heterogeneous healthcare market where public, private for-profit, and non-profit providers have different missions, managerial autonomy, and cost structures, which may explain the differences in payment rates for some services for the various provider types. The study highlights that, when setting prices for public and private healthcare providers, it is important to consider the profit-making status of the healthcare providers operating in the healthcare market, and to clarify the roles and responsibilities of public, for-profit and not-for-profit providers in determining healthcare purchasing arrangements. Regulatory policy instruments, as well as payment rates, are essential to steer efficiency, equity, and quality in health system with public and private provider mix.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was undertaken with funding from the Japan Science and Technology Agency (JST SICORP Grant Number JPMJSC21U8).
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AH conceived the study in discussion with ZO and JoC. JuC and ZO undertook the French case study and SN and AH undertook the Japanese case study. All co-authors contributed to the synthesis of findings from the two country case studies. AH led the process of drafting the article with input from all co-authors. All authors have read and approved the final version of the manuscript.