
Abstract
Background:
Racism and discrimination are realities faced by Indigenous peoples navigating the healthcare system in Canada. Countless experiences of injustice, prejudice, and maltreatment calls for systemic action to redress professional practices of health care professionals and staff alike. Research points to Indigenous cultural safety training in healthcare systems to educate, train, and provide non-Indigenous trainees the necessary skills and knowledge to work with and alongside Indigenous peoples using cultural safe practices grounded in respect and empathy.
Objective:
We aim to inform the development and delivery of Indigenous cultural safety training within and across healthcare settings in the Canadian context, through repository of Indigenous cultural safety training examples, toolkits, and evaluations.
Methods:
An environmental scan of both gray (government and organization-issued) and academic literature is employed, following protocols developed by Shahid and Turin (2018).
Synthesis:
Indigenous cultural safety training and toolkits are collected and described according to similar and distinct characteristics and highlighting promising Indigenous cultural safety training practices for adoption by healthcare institutions and personnel. Gaps of the analysis are described, providing direction for future research. Final recommendations based on overall findings including key areas for consideration in Indigenous cultural safety training development and delivery.
Conclusion:
The findings uncover the potential of Indigenous cultural safety training to improve healthcare experiences of all Indigenous Peoples. With the information, healthcare institutions, professionals, researchers, and volunteers will be well equipped to support and promote their Indigenous cultural safety training development and delivery.
Keywords
Introduction
Considerable evidence documents the positive outcomes of introducing Indigenous cultural safety training (ICST) for healthcare professionals in all areas of practice.1-7 Cultural safety training demonstrates improvements in trainees’ knowledge based on Indigenous Peoples, histories, culturally safe protocols, and procedures, as well as improves the likelihood of creating healthcare experiences free from racism and prejudice.1-7 The need to improve accessibility and opportunity for cultural safety training is of substantial importance, as Indigenous Peoples continue to face the harmful and lethal impacts of systemic racism embedded within the Canadian healthcare system.8,9 Systemic racism is described in the literature as: systemic racism . . . refers to established laws, customs, or practices that are systematically reflected in and that produce racial inequities in society. Whether. . .overt or unintentional or stems from oppressive or negative race-based policy, systemic racism contributes to health and socio-economic disparities, a greater exposure to risk, hazards, toxic environments, unfair perceptions, treatment, and injustices all of which ultimately influence health.
8
Systemic racism coupled with a lack of cultural safety measures (training, policies, etc.) in public healthcare systems across Canada leads healthcare professionals to act on unconscious discriminatory practices toward Indigenous Peoples.
10
Healthcare professionals often see themselves, or can be seen, as the authority figure in healthcare spaces, thus creating an unequal power dynamic based on their health-related knowledge and expertise over the knowledge of patients.11,12 This power imbalance often leaves Indigenous patients with experiences of prejudice, violence, and a lack of self-determination. With publicly reported incidents of Indigenous Peoples experiencing racism and discrimination in healthcare settings during 2020, there is an increased need to teach, train, and embed specifically Indigenous cultural safety into the perspectives and practices of healthcare professionals.
13
Joyce’s Principle is a key example of the need for this transformative work. In September 2020, Joyce Echaquan, an Atikamekw mother from Manawan, died at Joliette Hospital Center in Lanaudière, Quebec, after livestreaming her experiences on social media that illustrate the racism she experienced from the nurses responsible for her care.
14
In following these events, the Council of the Atikamekw of Manawan and the Council de la Nation Atikamekw
13
established Joyce’s Principle, which seeks to: Guarantee to all Indigenous People the right of equitable access, without any discrimination, to all social and health services, as well as the right to enjoy the best possible physical, mental, emotional and spiritual health.
8
Furthermore, in January 2021, an Ojibway man was forced out of a Toronto hospital after expressing frustration for the prolonged wait times to receive care. 15 He was sent out in harsh winter conditions with a wheelchair he could not operate. After his encounter, the Toronto hospital responded by “acknowledging anti-Indigenous racism is common in hospitals across Canada” and stating, “the fear and mistrust that Indigenous Peoples have of institutions that should be seen as places of safety and care is, sadly, valid.” 15 Joyce’s Principle and the Toronto hospital’s acknowledgment both demonstrate anti-Indigenous racism as a reality in healthcare spaces, and the immediate need for systemic change.
British Columbia’s 2020 report “In Plain Sight: Addressing Indigenous-specific Racism and Discrimination in B.C. Health Care” documents and describes countless experiences of discrimination within the healthcare system by all levels of staff and healthcare professionals. The report uses lived experiences to inform the final recommendations to promote and sustain systemic change. The findings foster a sense of urgency and necessity to address the pervasive anti-Indigenous racism in healthcare institutions. The final recommendations are specific to British Columbia, however, have merit for jurisdictions and healthcare systems across Canada and suggest a pivotal policy focus on mandating cultural safety training as a starting point. 16 In response to experiences illustrated above, we undertook an environmental scan to provide the necessary resources to inform the development and delivery of ICST within and across healthcare settings in the City of Toronto, Ontario. We focus on cultural safety training which has been defined by Baba 17 as occurring when a healthcare professional practices self-reflection and awareness to then “communicate competently with a patient in that patient’s social, political, linguistic, economic, and spiritual realm” 17 and “deliver care free from racism and discrimination.” 18 Cultural safety is used interchangeably with other forms of cultural awareness trainings such as cultural humility (listening and learning with about others without judgment, learning of personal culture and biases); competency (developing the attitude, skills, and knowledge to work with a diverse group of people, while limiting assumptions based on personal biases); awareness (acknowledging the similarities and differences between cultures), amongst many others.17,18 However, it is important to note cultural safety training is part of a larger continuum19,20 which moves from cultural humility, to awareness to competency, to safety.
Methods
We employed an environmental scan methodology, informed by Shahid and Turin’s 21 5-step approach to: define the study’s purpose; identify key individuals/stakeholders to approach; determine relevant information sources; gather resources and information; and consolidate the findings in a manner most useful for the target audience. As describe “one of the many benefits of using an environmental scan . . . is that the assessment can be tailored specifically to the resources available and the people or communities involved, which results in increased efficiency and probability of success” 21 (p. 73). Information was gathered directly from public healthcare organizational personnel and websites, as well as academic literature sources with a specific focus on Toronto, the province of Ontario and then across Canada.
We first scanned gray literature sources from healthcare institutional websites in Ontario to understand where and for whom ICSTs are offered. After which, we then approached organizational personnel through email to gather and chart the following information: name of the ICST, the training provider (eg, specialized staff, the organization), location of training, time commitment to complete the training, subject areas covered, target audience, implementation frameworks (how the training is implemented), evaluation tools (how the training is evaluated), accountability measures/frameworks (how participants of the trainings are held accountable to complete the training and implement its teaching into their daily lives and/or practice). Fifteen ICSTs offered in Ontario were identified, with 6 trainings in Toronto. Next, we conducted academic literature searches (Google Scholar, Scopus, Embase) to identify evaluative studies of the ICST offered in Toronto and across Ontario. This step was informed by the work of Bowra, Howard, Mashford-Pringle, and Ruggiero 22 and Mashford-Pringle et al. 20 Few studies met the location restriction, thereby leading to expanded inclusion of evaluative studies on ICST offered across Canada. Ten journal articles were identified (see Appendix A). The following was charted from the academic literature: setting of the ICST (where participants received the training for example geographic location, healthcare or other institutions, etc.), information on participants (ie, their field of work, how many received the training), title of the ICST, provider, implementation framework, topics covered, and key findings as discussed by the study. Another scan was undertaken in November 2022 which did not generate any additional findings. We included academic literature which focused on, mentioned, or formally evaluated the impacts of an Indigenous cultural safety training for healthcare, as well as some education professionals working in Canada. We conducted the literature search as complementary to the environmental scan of gray literature and websites and was not intended to be exhaustive. We included information that helped us to understand the lived experiences of healthcare staff and trainees including the realities of ICST in practice and provide recommendations and understand the gaps in the literature.
The findings of the scan are presented below according to 5 sections: (1) current ICSTs offered in Toronto, Ontario; (2) ICST toolkits identified; (3) summary of evidence-based evaluations of ICST offered in Canada; (4) information gaps uncovered in the search; and (5) concluding recommendations to inform wise practices. These sections were developed based on the information available, gathered, and relevant to adopting ICST best practices in primary through tertiary public healthcare organizations and institutions.
Limitations: We focused on Toronto, Ontario, Canada (geographically), and examined English only publications, websites, and materials. We had an extremely limited timeframe (3 months). There are 3 constitutionally recognized Indigenous groups in Canada (First Nations, Inuit and Métis) and we did not have time or resources to use a distinctions-based approach, but rather chose a pan-Indigenous approach. We recommend that future research examine distinctions-based First Nations, Inuit and Métis approaches to Indigenous cultural safety training.
Current ICSTs Offered
Toronto-based
The following organizations were identified in this review and offer ICST in Toronto, Ontario, Canada: Anishnawbe Health Toronto offers a self-paced course consisting of 3 YouTube modules; York University offers a 1-day online course in cultural safety for health coaches and navigators including content related to Indigenous Peoples and delivered through a series of live webcasts and self-directed content. Indigenous cultural competency training is available through the Native Canadian Center of Toronto (NCCT); the Ontario Federation of Indigenous Friendship Centers (OFIFC); and the University of Toronto through the Indigenous Initiatives Office. The NCCT and OFIFC trainings are a total of 8 and 6 hours respectively and include modules addressing the history of colonization and its intergenerational impacts on health and wellness. Self-awareness or self-reflection development amongst participants is a key component of the NCCT training. Online cultural awareness training is offered by the Toronto Aboriginal Support Services Council (TASSC) through a series of 3 YouTube videos, and focuses on providing information on basic Indigenous cultural knowledge rooted specifically in the urban Toronto context. Many of the Indigenous-run trainings have been designed for in-person learning and have adapted to online facilitation due to the COVID-19 pandemic.
Ontario-wide
Organizations identified in this review that offer ICST across Ontario include: the Indigenous Primary Health Care Council (IPHCC), Cancer Care Ontario (CCO), and OFIFC. IPHCC regularly offers in-person Indigenous cultural safety training, however, due to the COVID-19 environment and the transition to online engagement, the organization now offers their cultural safety training through San’yas’ Indigenous cultural safety training based out of British Columbia. The San’yas ICST has been adapted to deliver Ontario-specific online training courses with a purpose to address anti-Indigenous racism in healthcare and social service settings, and to promote and sustain cultural safety for all Indigenous Peoples across Ontario. 23 To date, over 100 000 individuals have received the San’yas ICS training. 23 There are 8 self-paced modules, over an 8-week period, and is geared toward educating non-Indigenous social service and healthcare professionals, as well as support staff, working in any of the IPHCC member organizations (eg, Aboriginal Health Access Centers, Community Health Centers, and other Aboriginal governed providers).
CCO offers 13 different online and self-paced trainings that are open to anyone and free of charge. 24 Topics include First Nations, Inuit and Métis cultures, colonization and the determinants of health, the need for cultural competence in healthcare, Indigenous knowledges, and traditional health. CCO also offers other trainings focused on specific subject areas such as chronic disease prevention for First Nations, Inuit and Métis People, and pediatric oncology. All trainings are certified by the College of Family Physicians of Canada, and physicians may complete courses free of charge to continue their professional development. 24
Lastly, OFIFC delivers Indigenous cultural competency training through a series of 4 cycles, each building on its previous section. The OFIFC training “enables participants to build skills, knowledge, attitudes and values essential to fostering positive and productive relationships with Indigenous people.” 25 After 3 cycles, participants will have learned foundational knowledge on contemporary Indigenous issues, treaties, and sovereignty, as well as “begin enhancing their relationship with Indigenous Peoples.” 25 The final cycle takes an operational lens and helps participants adapt their learnings to their organization in terms of both crafting plans for reconciliation, as well as expanding their organization’s overall cultural competency. 25
Accountability measures
The Toronto Aboriginal Support Services Council (TASSC) training in Toronto, Ontario, Canada commits to an ongoing relationship and dialog with trainees to implement and ensure accountability measures are included in ICST. 26 This engagement helps the organization to capture any recommendations for future trainings, as well as respond to any points of misunderstanding or further curiosity. The TASSC ICST was one of the only trainings found to have employed accountability measures intended for their participants. 26 Accountability in this context may help to improve completion among participants involved in non-mandatory ICST, by offering continued support and encouraging engagement.
The trainings offered by both CCO 24 and the Wabano Center for Aboriginal Health in Ottawa, Ontario, Canada 27 emphasize the importance of providing cultural safety and anti-Indigenous racism training to all persons regardless of their societal or professional role. Based on this direction, solely providing ICST to healthcare providers may not be sufficient to eliminate anti-Indigenous racism; rather, the trainings must be provided to all those working within the health system (healthcare providers, technicians, facility staff, volunteers) this serves all Indigenous patients, families, and communities in culturally safe way.
Toolkits
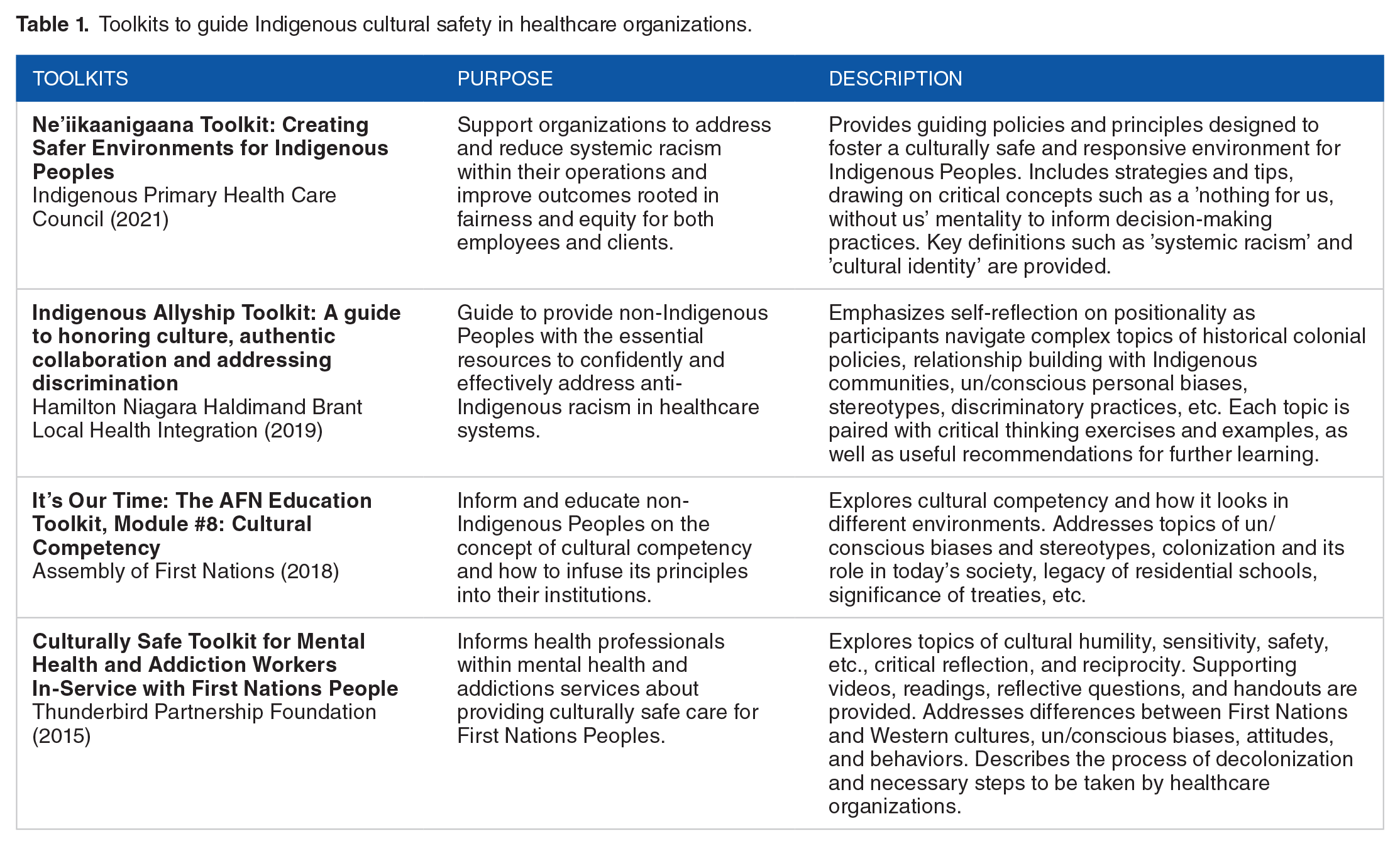
We further identified ICST toolkits designed by and for healthcare organizations on both local and national levels, helping to guide ICST and associated organizational policy development. Table 1 outlines key examples of toolkits that may offer insight into contemporary best practices to address cultural safety within healthcare systems, as well as to generate cross-systems learnings for ICST implementation. Further examples may be available but are not shown in Table 1 below:
Toolkits to guide Indigenous cultural safety in healthcare organizations.
Evaluations Available
Healthcare institutions across the country have implemented unique versions of training modules in response to the Truth and Reconciliation Call to Action #23, calling for all levels of government to provide “cultural competency training for all healthcare professionals.” 28 Researchers have evaluated these trainings for pre-service and experienced healthcare professionals from across multiple sectors.1-7 As such, research suggests in-person ICST is often praised by participants for the opportunity to engage and ask questions,2,4,6,7 as well as involve Indigenous Peoples and Elders from local Indigenous communities. 7 However, registered nurses attending an ICST in Sioux Lookout, Ontario highlighted that the online format of their training better suited their needs and practical availability. 5
The content of the ICST often reflects the socio-demographic and geographic indicators specific to where training is offered and who the healthcare professionals expect to serve.1,4,7 Characteristics of local Indigenous Peoples and communities including traditions, languages, and histories are also often considered.1,4,7 Based on the literature, common examples of key topics covered by ICSTs include (although are not limited to): colonialism, impacts of colonial policies, Indigenous histories, concepts of systemic racism toward Indigenous Peoples in healthcare systems, cultural humility and respect, and culturally safe practices.1-7 These topics in combination begin to provide participants with a knowledge base from which they can continue their journey in Indigenous cultural safety.
Brown et al. 1 found their training (referred to as a health equity intervention ie, “Equipping Primary Health Care for Equity”) raised clinician’s awareness of systemic racism and unconscious bias embedded in healthcare systems to a level which prompted trainees to self-reflect on their personal actions and biases. Similarly, all ICSTs found in this review had modules or programs that raised awareness of barriers Indigenous Peoples face in healthcare spaces, while also highlighting the powerful role healthcare professionals have; as they are able to remove such barriers once grounded in understandings of cultural safety.2-7 Student healthcare professionals, 6 government employees, 29 and registered nurses 5 reported a keen interest to continue learning about Indigenous cultural safety beyond the course or program offered, and many expected to implement their learnings into their prospective practice.
From the ICST evaluations collected in this study, participants often expressed their personal challenges with questioning their own beliefs, as well as the feelings of discomfort when learning the continuing and persistent impacts of colonization thrust upon Indigenous Peoples health and wellbeing.4,7 Moreover, a small number of healthcare professionals reported discomfort in the “tone” of the ICST they attended. 7 Some participants also struggled to situate themselves within their settler identity as it pertains to the historic and ongoing relationship between non-Indigenous and Indigenous Peoples in Canada. The uncomfortable nature of acknowledging settler identity was identified by Yaphne et al 7 as an illustration of training effectiveness, as participants come to terms with their own sets of values and internal biases they may not have confronted before. Thus, demonstrating participants’ genuine engagement in the training material. Furthermore, scholars suggest increasing the time for participants’ self-reflection prior to completing the training, to allow participants a safe and supportive space for critical reflection, which can then lead to behavioral change.4,7,30 In an ICST designed for pre-service educators, Mashford-Pringle and Nardozi 30 highlight the additional need for further time allotments to conduct the training, so as to maneuver the complex and challenging material, as well as allow for ample time for questions, clarification, and reflections.
In all scenarios, ICST training is well received from healthcare professionals from across multiple sectors (eg, clinicians, family physicians, dental hygienist students, registered nurses, etc.). Future research that conducts evaluation of ICST intended for all health professionals (supportive staff, volunteers, physicians, surgeons, nurses, patient navigators, etc.), should also include longitudinal evaluations, as this ensures if trainees are successfully implementing their learnings into their current practice.
Gap Analysis
This environment scan identified 3 key gaps: (a) the need for longitudinal evaluations of ICST; (b) evaluations of mandatory versus optional ICST; and (c) the development of accountability measures to keep trainees engaged and ensure their participation sustains throughout the course and into their practice. To start, the environmental scan did not identify any longitudinal evaluations of ICST provided to healthcare professionals and/or staff. Evaluation methods often solely rely on anonymous surveys (feedback forms) to complete before and after the training, to gather ideas on the participants educational journey and growth in knowledge.5,26,27,31 Therefore, little is known on the best or effective methods to teach or train on cultural safety to produce sustainable and long-term impacts, nor the realities of what ICST can accomplish in terms of shifting individuals and/or healthcare organizational practices, cultures, environments, or perspectives with respect to reducing or eliminating anti-Indigenous racism in healthcare. Evaluations of ICST did not compare the outcomes of participating in mandatory versus optional training, which renders questions on whether the nature of a mandatory training leads to improved learning and practice-based outcomes for participants, or, if attendance should be based on personal interest. As well, if either style (mandatory or optional) leads to improved attendance or active participation of participants. Future research fueled by both qualitative and quantitative methods is suggested to fill these gaps.
Furthermore, no evaluative studies detailed how healthcare organizations implement measures to hold participants accountable to complete their training or to invoke the training they have received. Of particular concern are non-mandatory and/or “self-paced” trainings, in which participants are not guided or supervised to maintain their engagement and check for completion. Only the Toronto Aboriginal Support Services Council and the Wabano Centre for Aboriginal Health in Ottawa, Ontario cultural safety trainings provided insight into their accountability measures. For example, at the Wabano Centre, those responsible for administering the training are motivated by anticipated funding levels, as to receive organizational funding, the Wabano Centre is required to have 15% of their staff (service providers) complete the online or in-person ICS training (Wabano Centre for Aboriginal Health, personal communication, Jan 19, 2021). Nevertheless, based on the study’s findings, much of the literature describes elements of ICST which may be summarized by a 3-step process: learn, reflect, and act. This process is demonstrated below in Figure 1.
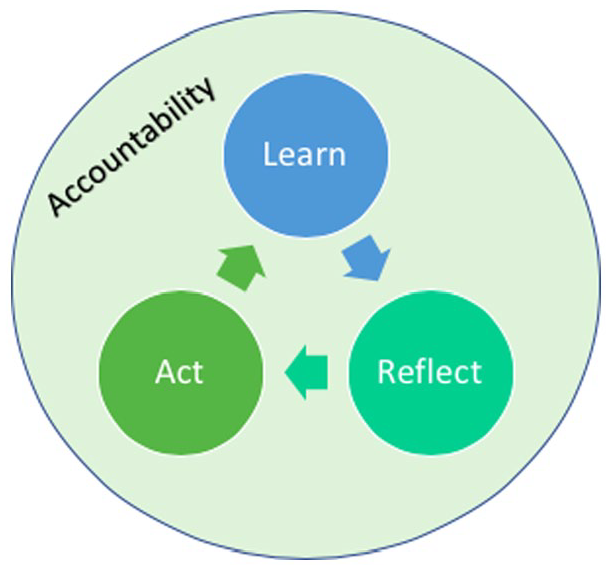
Process of ICST and importance of accountability.
By observation, measures of accountability play a significant role in each step of the process. In keeping participants accountable, an organization may not only guarantee completion of the training, but also provide participants the opportunity to ask questions and engage in further learning, and ensure they are fully equipped to implement their learnings into their healthcare, professional, and personal practices.
Recommendations
This study provides foundational knowledge of important aspects and characteristics of ICST offered in Toronto, Ontario, Canada, and within the greater Canadian context. It may serve as a resource for healthcare institutions and organizations to investigate, plan, and implement ICST for healthcare staff and personnel based on what does and does not exist, work, or may constitute as wise practices. Our key recommendations are grounded in the findings and are intended to guide future ICST development and delivery.
Development
ICST programs must be developed by and in partnership with local Indigenous community members throughout the program design and delivery process. 7 Topics to include range from, although are not limited to, local Indigenous (First Nations, Métis, Inuit) histories, traditions, and worldviews, in addition to relevant policies and legislation (eg, Indian Act, Treaties, United Nations Declaration on the Rights of Indigenous Peoples, etc.); and should be tailored to local communities1,4,7 as well as the relevant cultural and political context. 20 Moreover, content of the training is recommended to identify and articulate the specific impacts of historic and ongoing colonialism including the long-lasting and systemic anti-Indigenous racism present within Canadian healthcare systems1-7 and provide additional resources, recommended readings, and reflective questions to support and advance further learning. 32 Participants should be encouraged to challenge and question internal beliefs, biases, and assumptions about Indigenous Peoples.4,7 The process of learning about these ongoing injustices is challenging4,7,30 and participants should thus be supported physically, mental, emotionally, and spiritually.
Delivery
ICST programs must be offered to all staff within a healthcare institution (healthcare professionals, support staff, volunteers, etc.).24,27 Based on literature, it is suspected that while providing ICST to a specific subset of staff or role (eg, physicians and nurses) may allow for greater uptake or role-specific training, ICST should be undertaken as part of a larger cultural safety initiative offered to all staff. As research findings suggest, ICST alters participants’ interactions and engagement with Indigenous Peoples in a manner of improved respect. 29 Training is therefore recommended for all healthcare staff and workers to ensure all those interacting with Indigenous patients or staff are well equipped to engage appropriately and without harm.
Training is most effective when individuals can gather in-person, allowing trainers to build relationships and trust with and among the group.2,4,6,7 Although, online options are also encouraged to allow for greater flexibility and accessibility. 5 Both in-person training and online options are thus recommended for participants to select according to their availability and needs. Facilitators are also encouraged to establish long-lasting relationships with participants to facilitate ongoing learning and instill a measure of accountability for participants to implement their learnings into their everyday practices. 26
Other considerations and concluding thoughts
Of final considerations, we recommend taking all precautions to create and establish a safe space to conduct the training, ensuring the space is free of judgment and harmful tones (eg, blame, shame, etc.). 7 The training must also be delivered by qualified facilitators which should prioritize self-identified Indigenous Peoples including Elders and Knowledge Keepers, with evidence of advanced knowledge and skills in Indigenous cultural safety training and practices, as well as true and authentic community partnership experience to ensure appropriate, respectful, and safe delivery. Training is recommended to occur over multiple days (2+) to allow time for participants to digest the material, reflect, and situate themselves within the lessons. 4 As well, ample time set aside for personal reflection, questions, and group discussion, which is strongly advised to promote and further advance reflection and learning.4,7,30 Finally, methods and protocols to administer the training are recommended to be thoroughly tested to ensure accountability of participants, and keep participants engaged and interested throughout the duration of the training. 7
The potential of ICST to improve the healthcare experiences of all Indigenous Peoples warrants the utmost successful, proactive, and evidence-based methodology and framework. With this environmental scan it is hoped healthcare institutions, professionals, researchers, and volunteers alike will be well equipped to support and promote their ICST development and delivery.
Footnotes
Appendix
Included articles in this review.

| Buchanan, J., & Salman, N. (2018). Evaluation of the workshop “Building Bridges through Understanding the Village.” University of Victoria: Victoria, BC. |
| Browne, A. J., Varcoe, C., Ford-Gilboe, M., Wathen, C. N., Smye, V., Jackson, B. E., . . . & Garneau, A. B. (2018). Disruption as opportunity: Impacts of an organizational health equity intervention in primary care clinics. International Journal for Equity in Health, 17(1), 1-16. |
| Crowshoe, L. L., Han, H., Calam, B., Henderson, R., Jacklin, K., Walker, L., & Green, M. E. (2018). Impacts of educating for equity workshop on addressing social barriers of type 2 diabetes with indigenous patients. Journal of Continuing Education in the Health Professions, 38(1), 49-59. |
| Doucette, H. J., Maillet, P. J., Brillant, M. G., & Tax, C. L. (2015). Dental hygiene students’ perceptions of a cultural competence component in a tobacco dependence education curriculum: a pilot study. Journal of Dental Education, 79(6), 680-685. |
| Hall, K. (2010). Developing a cultural safety intervention for clinicians: Process evaluation of a pilot study in the Northwest Territories. [Master’s thesis, University of Victoria]. |
| Mashford-Pringle, A., & Nardozi, A. (2013). Aboriginal Knowledge Infusion in initial teacher education at the Ontario Institute for Studies in Education at the University of Toronto. The International Indigenous Policy Journal, 4(4). |
| Rand, M., Sheppard, A., Jamal, S., Kewayosh, A., Mashford-Pringle, A. (2019). Evaluation of the Indigenous relationship and cultural safety courses among a sample of Indigenous Services Canada nurses. International Journal of Indigenous Health, 14(1), 29-41. |
| Rass, R. A. (2012). Supporting newly recruited teachers in a unique area, the Northwest Territories in Canada. Journal of Education for Teaching, 38(2), 141-161. |
| Shah, C., & Reeves, A. (2015). The Aboriginal cultural safety initiative: An innovation health sciences curriculum in Ontario colleges and universities. International Journal of Indigenous Health, 10(2), 117-131. |
| Yaphe, S., Richer, F., Martin, C. (2019). Cultural safety training for health professionals working with Indigenous population in Montreal, Quebec. International Journal of Indigenous Health, 14(1), 60-84. |
Acknowledgements
We would like to acknowledge Thilaxcy Yohathasan for her support in preparing this research for publication.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a contract with the Toronto Central Local Health Integration Network.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
The authors confirm contribution to the paper as follows: study conception and design: AMP. DW, BSK, CH, ST; data collection: DW, ST, BSK, SS, TB, AB, & CH; analysis and interpretation of results: DW, SS, ST, BSK, AMP; draft manuscript preparation; DW, ST, AMP. All authors reviewed the results and approved the final version of the manuscript.