
Abstract
Background:
The Medicare Accountable Care Organization (ACO) Program has created a vehicle for providers who practice cost containment and exceed quality for the Medicare population. The success of ACO’s nationwide have been well documented. However, there is little research evaluating if there is a cost saving benefit in trauma care with respect to participating in an ACO. Thus, the primary objective of this study was to evaluate inpatient hospital charges associated with trauma service utilization of patients participating in the ACO compared to non-ACO patients.
Methods:
This case-control retrospective study includes a comparison of inpatients charges of ACO patients (cases) and general trauma patients (controls) presenting to our trauma center in Staten Island, New York from January 1st, 2019 to December 31st, 2021. A 1:1 matching of case to control was performed based on age, sex, race, and injury severity score. Statistical analysis was performed with IBM SPSS, with P < .05 as significant.
Results:
A total of 80 patients were included in the ACO cohort and 80 matched in the General Trauma cohort. Patient demographics were similar. Comorbidities were similar with the exception of a higher in incidence of hypertension (75.0% vs 47.5%, P < .001) and cardiac disease (35.0% vs 17.5%, P = .012) in the ACO cohort. Both the ACO and general trauma cohort had similar Injury Severity Scores, number of visits and lenght of stay. Both charge total ($76 148.93 vs $70 916.82, P = .630) receipt total ($15 080.26 vs $14 180, P = .662) charges were similar between ACO and General Trauma patients.
Conclusion:
In spite of increased incidence of hypertension and cardiac disease in ACO trauma patients, mean Injury Severity Score, number of visits, length of hospital stay, ICU admission rate and charge total was similar compared to general trauma patients presenting to our Level 1 Adult Trauma Center.
Introduction
The Affordable Care Act of 2010 (ACA) authorized the implementation of a wide variety of health care delivery system reforms. One of these notable reforms was the establishment of an entity known as an Accountable Care Organization (ACO) by the U.S. Department of Health and Human Services in 2011. 1 ACOs are composed of groups of doctors, hospitals, and other health care providers, with a goal of coordinating high-quality care to their Medicare patients. Through the coordination of care, the ACO was designed to achieve the “Triple Aim” of improving population health outcomes, improving the patient experience, and lowering the per capita cost of health care. 1 The ACO model was intended to align interests of payees and providers through innovative shared savings payment arrangements that compensates providers for the quality of the care delivered rather than volume of health care services provided. 1 Nationwide, the Medicare ACO Program has continued to evolve from a purely “no risk” or Shared Savings Program (SSP) into other models. Of the 477 Shared Savings ACO’s, 59% of them are in a one-sided model and 41% are participating in a 2-sided model. 2
Richmond Quality ACO, located in Staten Island, New York, has been participating in a CMS Shared Savings ACO Model since 2015. Over the 6-year duration of the Program, it has generated over $30+ million dollars of savings with over $16 million dollars retained in shared savings and distributed amongst the providers and hospital sponsor. This is a reflection of the cost containment practices and pro-active care involved with the ACO patients. This quality level demonstrates the commitment and success of health screening and prevention to pre-empt disease along the continuum. Richmond University Medical Center, sponsor of Richmond Quality ACO, is a 448 acute care full-service hospital. Like the Richmond Quality ACO, it too is considered a low-cost provider when viewed by payors and industry benchmarks.
Despite this positive evidence from primary care settings, it remains unknown whether ACO participation will have similar cost benefits for delivery of more technically challenging care, such as that of a Level 1 Adult Trauma Center. This is important to consider because Trauma systems model a system of care consistent with the goals of the Affordable Care Act, as they coordinate care among multiple health care professionals and across the continuum of care. Thus, the primary objective of this study was to compare inpatient hospital charges associated with trauma service utilization of patients participating in the ACO compared to non-ACO patients. We hypothesized that the data of the ACO Trauma patient compared to the traditional trauma patient would mirror the lower charges found in the Richmond Quality ACO experience.
Methods
This study was conducted at Richmond University Medical Center (Staten Island, New York), a Level 1 Adult Trauma Center in Staten Island Yew York and was reviewed by the IRB at New York Medical College and received an IRB exemption. (Protocol Number: 14802). This retrospective study included a review of the all trauma patients seen at Richmond University Medical Center, a Level 1 Adult Trauma center from January 1st, 2019to December 31st, 2021. The primary objective of this study was to evaluate inpatient hospital charges associated with trauma service utilization of patients participating in the ACO compared to non-ACO patients. A secondary analysis of patients presenting with fall diagnosis, fracture/orthopedic injuries (displaced/non-displaced extremity fracture, pubis fracture, multiple rib fracture, vertebral fracture) and cranial injuries (concussion with or without loss of consciousness, subarachnoid/subdural hemorrhage, unspecified intracranial injury) was performed. Charge data analyzed included charge total (amount hospital charged to payors) and receipt total (amount hospital received from payors).
A case-control study design was utilized where ACO patients trauma patients (Cases) were matched to control general trauma patients who were not participating in the ACO. Cases were identified by ICD-10 code. A 1:1 matching of case to control was performed based on age, sex, race, and injury severity score. Controls were randomly chosen from the trauma registry data base. All patients presenting to the trauma center were eligible for inclusion with the exception of those under the age of 18, and patients with pre-existing chronic renal disease currently on dialysis.
National Trauma Registry System (NTRACS) was queried to identify the trauma patients. Diagnoses and procedures were encoded according to the International Classification of Diseases, 10th Edition, Clinical Modification (ICD-10). Data elements were extracted directly from our trauma registry’s electronic health records using the ICD-10 codes to identify subjects. Additional data points collected included: patient age, gender, comorbidities based on diagnosis coding, mechanism of injury, hospital admission service, Intensive Care Unit (ICU) admission, length of hospital/ICU stay, and need for mechanical ventilation. Lightbeam Health Solutions ACO Software (Irving, Texas) was used to identify which patients in the Trauma Registry were enrolled in the Richmond Quality ACO. Once identified, the inpatient charge data for both cohorts were extrapolated out of the information available in the electronic medical record system.
Statistical analysis was carried out using IBM SPSS 27.0. Univariate analyses for continuous variables was be compared using the Student’s t-test or Mann-Whitney U-test. Categorical data was be compared using χ2-test or Fisher’s exact tests. A P value of <.05 was considered statistically significant. A power analysis was performed to determine sample size. We anticipated approximately 100 ACO patients “cases” presenting to the trauma center during the study periods. During the same time period, we anticipated 2500 non-ACO trauma patients to serve as available controls. Based on data from Geyer et al, 3 ACO trauma patients had a 7.2% lower overall cost of hospitalization compared to those not in a ACO. Using this data, we approximate a medium effect size (0.47). Using a 2-tailed test, alpha of 0.05, and 80% power, we would need a total of 152 patients, with a minimum of 76 patients in each group.
Results
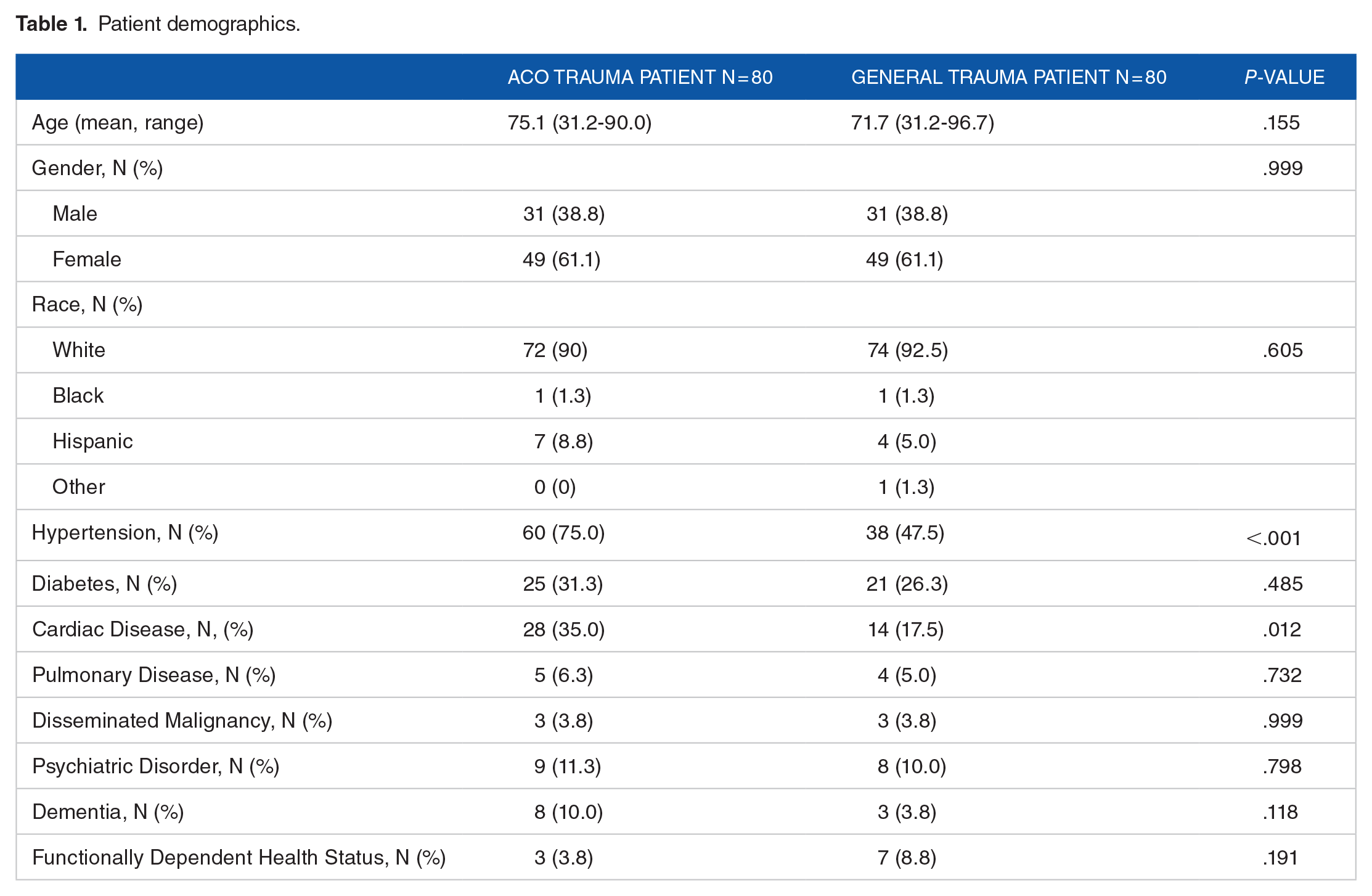
A total of 80 patients were included in the ACO cohort and 80 matched controls in the general trauma cohort. Gender and race were similar between to 2 cohorts (Table 1). However, there was a greater proportion of females compared to males in both cohorts, and over 90% of our patient population was white. The mean age of the ACO cohort, 75.1 years (31.2-90.0 ) and non-ACO cohort, 71.7 years (31.2-96.7) were similar (Table 1), Comorbidities including pulmonary disease, psychiatric disorders, dementia, functional status dependent, and disseminated malignancy were similar, with the exception of a higher incidence of hypertension (75.0% vs 47.5%, P < .001) and cardiac disease (35.0% vs 17.5%, P = .012) in the ACO cohort (Table 1).
Patient demographics.
Both the ACO and general trauma cohort had similar mean Injury Severity Score (4.81 vs 4.87, P = .936), number of visits (3.28 vs 2.92 days, P = .537), length of hospital stay (3.0 vs 3.1 days, P = .839) and ICU admission rates (7.5% vs 6.0.7%, P = .840) respectively (Table 2). For those patients admitted to the ICU, the average number of days in the unit, as well as the number of days on ventilatory support were similar between both cohorts (Table 2).
Patient outcomes.

The Injury Severity Score (ISS) assesses the combined effects of the multiple injuries and is based on an anatomical injury severity classification, the Abbreviated Injury Scale (AIS). The ISS is calculated as the sum of the squares of the highest AIS code in each of the 3 most severely injured ISS body regions (head or neck, face, chest, abdominal/pelvic, extremities or pelvic girdle, external). Injury Severity Scores range from 1 to 75. If an injury is assigned an AIS of 6 (identifying a currently untreatable injury), the ISS score is automatically assigned 75.
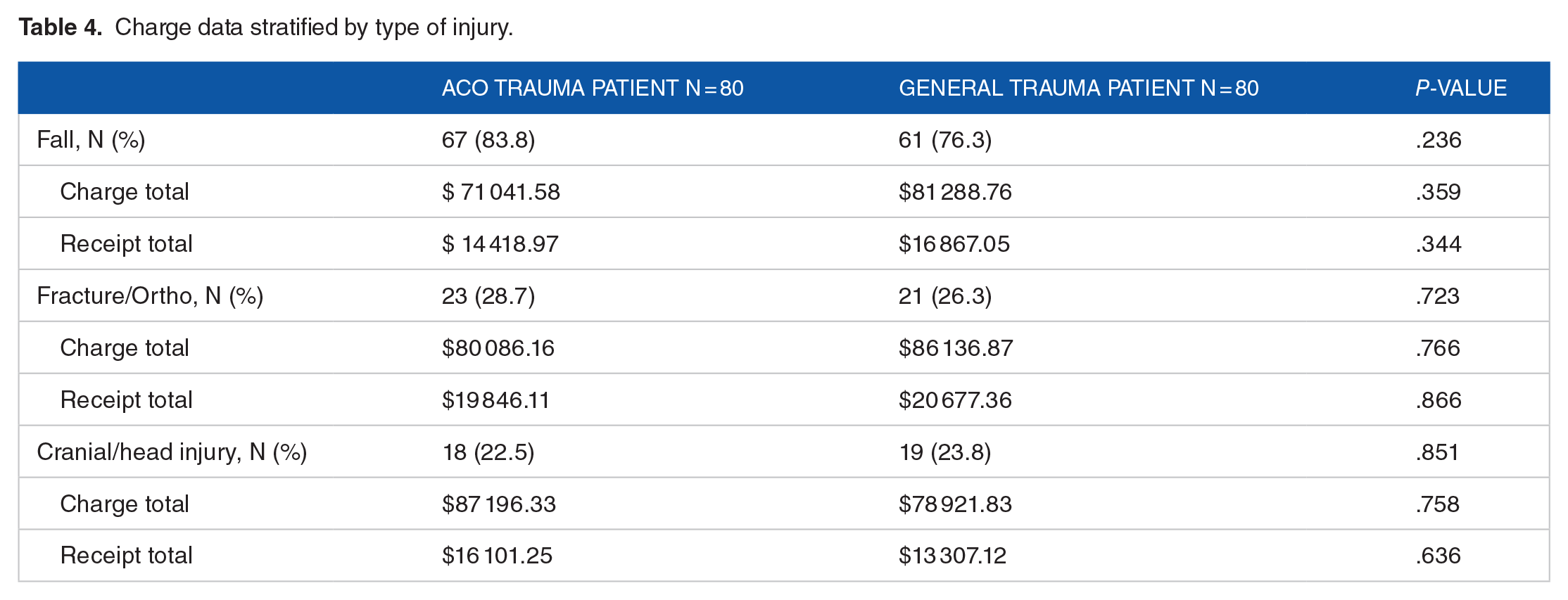
The charge total and receipt total were similar regardless of ACO participation (Table 3). A sub-analysis was performed for the 3 most common types of injury presenting to the trauma center. With regards to type of injury, there was a similar number of patients presenting with either a fall diagnosis (83.8% vs 76.3%, P = .236), fracture/orthopedic injury (28.7% vs 26.3%, P = .723), or cranial/head injury (22.5% vs 23.8%, P = .851) in the ACO and general trauma cohorts respectively (Table 4). Charge analysis revealed no differences in charge or receipt total costs for these diagnoses (Table 4).
Total charge analysis.

Charge data stratified by type of injury.
Discussion
The success of the ACO Medicare Program in achieving cost savings and improving quality is well documented. However, very little has been studied or published regarding cost or quality disparities at a Level I Adult Trauma Center with a hospital sponsored ACO. Our study showed no difference in inpatient charges of trauma patients in ACOs compared to non-ACO patients. We chose utilize use charge data analysis as a metric of cost because it closely reflects service utilization and hospital reimbursement. We did exclude patients who were less than 18 years of age to focus our work on the adult population. Additionally, patients with chronic renal disease currently on dialysis were excluded. Previous studies have shown that these patients have longer lengths of hospital stay as well as more variable healthcare utilization. 4 Inclusion of these patients may have skewed our analysis. However, further study of this group of patients is warranted to determine if ACOs add to cost containment in this setting.
Citing the high costs of managing a trauma center as well as the benefits of a centralized approach to trauma care coordination, Eastman et al recognized the increased costs that a trauma center contributes national health care costs. 5 The study found that hospital costs for patients treated in trauma centers were 71% higher than patients treated traditional emergency departments, while citing the life-saving “value” as worth the expense. However, their analysis is more generalized and did not differentiate with the trauma patients being traditional patients or ACO members.
In 2016, Geyer et al evaluated monetary savings associated with transfer of trauma patients within an ACO in terms of overall hospitalization costs. Of the 7696 patients studied over a 5-year period, they identified 7.2% lower costs associated with the ACO. 3 The ACO cohort had similar length of stay, disease, and mortality. Through their review of patients, Geyer et al noted that those from the ACO had 0.47 fewer advanced imaging studies than the non-ACO cohort. There was no indication as to whether participation in the ACOs effected image decision making. Although our research showed no significant charge variance, Geyer et al found those within the ACO to have lower costs.
Our study did not find any differences in charges associated with a fracture/orthopedic diagnosis. However, disparities in care after spinal fractures has been studied by 3 large academic medical centers in Boston with focus on ACO versus non-ACO patients. 6 Lipa et al, studied 245 704 spinal fracture patients of which 2% of the cohort received care in an ACO. 6 While specific costs were not included, the team studied the re-admission rate, mortality, and complications of ACO versus non-ACO patients, all suggestive of additional health care spend for non-ACO patients. The study also found that non-whites had a significantly higher odds of readmission in 2009 to 2011; however, this became non-significant in the context of care provided by the ACO in later years. Overall their study reinforces the idea that ACOs could improve health care disparities among non-whites. Furthermore, reduction in re-admission rates, mortality, or complications in ACO patients, regardless of race, may suggest overall decreased healthcare costs. Our ACO and general trauma cohorts were over 90% white, and thus we were not powered to assess differences in outcomes based on race.
Similarly, Pediatric ACO strived to improved costs and curtail growth of expenses in comparison to the traditional fee for service (FFS) and Medicaid (MC) products on the market. Their results showed a $2.40 rate increase in Price-per-member-per month (PMPM) which was much lower than the PMPM increase of $16.15 in FFS and $6.47 in MC. 7 While this article does not cite the specific cost savings of emergency care between the traditional pediatric trauma patient and the ACO Trauma patient, the authors found a modest improvement in gastroenteritis admission rate, pediatric quality acute composite scores, and overall pediatric quality composite metrics favoring the ACO.
As discussed by Eastman et al, trauma is known to drive healthcare costs for individuals who seek care at a trauma center. Additionally, surgery is attributed to high healthcare costs for older adults. 8 Thus, Modi et al sought to evaluate the effect of ACO participation on surgery costs in both the inpatient and outpatient setting. 8 Modi et al found that ACO participation resulted in $181 reduction in spending throughout the beneficiary year. Additionally, they found that payments for surgical visits were $956 lower for individuals in an ACO. Their findings included the identification of savings from a shift to outpatient surgery and reduction of inpatient surgery. We found no noticeable cost savings for individuals with trauma, but did not analyze outpatient care for the purpose of our study.
Our study found that mean Injury Severity Score, number of visits, length of hospital stay, ICU admission rate, and overall charge was similar, despite the ACO cohort having more patients with hypertension and cardiac disease. Additionally, there was a non-significant trend to reduced length of ICU stay compared to general trauma patients. Thus, a possible improvement in population health, better care coordination, and reduction of cost may be due to the participation in the ACO. In line with this, McWilliams et al noted that one area typically associated with ACO cost reduction is the management of chronic illness and the ultimate reduction in complications with these diseases. 9 The authors note that robust disease management approaches are supported by the Quality Measures of ACOs, which emphasize care coordination and prevention for patients with certain conditions, including cardiac disease. The authors also note that despite this presumption, the research so far has yet to highlight this saving associated with high-risk patients. In fact, they noted that reductions in inpatient costs were reduced similarly in both high and low risk patients. 9 They believe this would indicate that the cost savings is not driven by the risk profile of the patient, but rather the initiatives on cost reduction for all patients. 9 Our findings may indicate that ACO participation may keep chronic disease complications under control and aide in annual cost reduction. Interestingly, we are uncertain about why patients with cardiovascular disease were more likely to enroll in our ACO. It is plausible this group of patients were more aware of the benefits of joining ACO, including improved patient experience, better care coordination, and cost-containment. It is also possible that our providers were more proactive at reaching out to these patients and educating them of these benefits. Further analysis of our ACO population, including reasons for enrollment, may be of interest to policymakers.
Strengths of our study included a robust cost analysis of both charges and reimbursement. The cost/claims data were extracted from the Hospital EMR. This ensured consistency with the cost information coming from the same source for both cohorts. We summed the total overall cost billed and respective reimbursements received. Studies previously discussed utilized other approaches. Geyer et al obtained costs from a hospital database but did not examine reimbursement. 3 Other studies utilized Medicare claims and enrollment data or extrated information from their State Department of Medicaid Projected Medicaid Service Expenditures report to derive costs.7-9 Finally, Lipa et al utilized secondary metrics such as re-admission rate, mortality, and complications rather than actual costs. 6 The findings discussed must be analyzed considering the limitations of our study. The sample size for the 2 cohorts was small. Additionally, 90% of the study population was white, and this study may not be accurate for the non-white population. Our approach to this analysis was a retrospective study, which inherently has limitations. Additionally, we utilized the electronic health record to analyze charges; this provided the annual total of costs per patient at the center and was not specific to the trauma visit. Our electronic medical record system did not allow us to specifically identify and isolate trauma-specific costs. A future study could control for this by analyzing inpatient and outpatient hospital charges specific to an index trauma encounter. Additionally, ACO savings incorporates outpatient activities into their prevention and approach; due to lack of access to non-ACO outpatient costs, this research only evaluated total costs of inpatient care. Further research in both the inpatient and outpatient setting is needed to determine if ACOs lower costs in trauma centers.
Conclusions
In spite of increased incidence of hypertension and cardiac disease in ACO trauma patients, mean Injury Severity Score, number of visits, length of hospital stay, ICU admission rate, and charge data was similar compared to general trauma patients presenting to our Level 1 Adult Trauma Center. As the ACO focuses on prevention and reduction of costs, trauma may be a mitigating factor in avoiding an acute care hospital visit. Additional research in the incorporation of injury prevention in the ACO practices may be beneficial.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors Contributions
All authors keenly participated in the research project, including study design (RS, NL, DG-S, VR), data acquisition (DG-S, HM, JE-D), analysis (DG-S, HM, JE-D, NL), and manuscript writing (DG-S, HM, NL, RS). All authors read and approved the final manuscript (RS,DG-S, HM, JE-D,VR, NL).