
Abstract
Background:
While the community health service system was initially established in rural areas of mainland China, the utilization of community health service resources by the rural elderly population is not clear.
Methods:
Cross-sectional studies on the utilization of community health services by the rural elderly population in mainland China published within the last 10 years were retrieved from the China National Knowledge Infrastructure (CNKI), Wan Fang, Medline and Web of Science (WOS) databases. The quality of the article was evaluated by the Critical Appraisal Skills Programme (CASP), and obstacles to the utilization of community health services by the rural elderly population were analyzed based on the Andersen model.
Results:
Twenty-four studies were analyzed, and 3 gaps were found. (i) The cognition of rural elderly residents does not match the current health security system. (ii) There is a gap between the supply of health service resources in rural communities and the health needs of the elderly residents in these areas. (iii) The health services provided by rural primary health service institutions are not targeted.
Conclusions:
In mainland China, the provision of community health services to the rural elderly population has improved significantly. However, several factors from the individual level to the system level lead to low levels of access and utilization. This finding means that under the leadership of the government, it is necessary to integrate the strength of multiple departments to cooperate in improving the welfare system, policy publicity, health education, financial support, system guarantees and resource exchange and sharing for the elderly population in rural areas and to jointly promote community health services for the elderly population in rural areas.
Introduction
In 2021, the Seventh National Census showed that there were 190.64 million people aged 65 and above in China, accounting for 13.50% of the total population, 1 which is 4.58% higher than the number in 2010. 2 The United Nations Population Agency predicts that by 2025, those aged 65 or older in China will account for 14.03% of the population. 3 When the proportion of the population aged 65 and above exceeds 14%, a country or region is classified as a deeply aged society. The aging level of China’s population has changed in recent years from a short and relatively slow evolution to a “fast track” of rapid growth. China adopted family planning as a basic state policy in the early 1980s, hoping to reduce the total population by lowering the birth rate and keeping population growth in line with the country’s economic and social development plans. To date, China’s population age structure shows an obvious spindle shape; Chinese society has been aging ahead of time, and China has one of the world’s most serious population problems.4,5 Compared with other countries with seriously aging populations (such as South Korea, Japan, 6 and the Netherlands 7 ), China is still considered a developing country. China’s limited financial capacity, its low per capita income and social problems such as “getting old before getting rich” obviously restrict people’s effective use of health service resources.8,9
Elderly individuals are the population most in need of health care services. 10 Physiological aging/disability, the prevalence of noncommunicable chronic diseases, 11 and the absence of health services 12 are all threats to the health of the elderly population in China. According to the China Statistical Yearbook 2020, 67% of China’s elderly population lives in rural and township areas. 13 To solve the problem of health security, attention must be paid to the elderly population in rural areas. Since the founding of China, the urban‒rural dual household registration system has been implemented. In this system, the state clearly divides residents into agricultural and nonagricultural household registration categories. Due to the impact of the dual household registration system between urban and rural areas, most of China’s superior medical resources are concentrated in cities and towns, rural residents have limited access to health services, 12 and the gap keeps widening. 9 Moreover, the phenomenon of the wave of migrant workers, 14 which has continued since the last century, has caused a huge number of left-behind elderly people and children to be present in China’s rural communities, which also poses a new challenge to China’s rural medical system.15,16
Community health services play a very important role in maintaining the health status of the rural elderly population. In China, the rural community health service structure is a public health service network that uses county-level medical and health institutions as guides, township health centers/community health service centers as links, and village clinics/community health service stations as the bottom of the network. 17 In 2009, the Chinese government began providing services such as health record establishment, chronic disease management, maternal and child health care and geriatric care management free of charge to all elderly individuals, patients with chronic diseases, children and pregnant women, aiming to provide basic and equal public health services to all urban and rural residents. In 2019, the National Health Commission issued the New Basic Public Health Service Guidelines, which included elderly health services and the combination of medical care and elderly care as important public health service items. However, although the basic public service system promotes the equality of health opportunities, from the perspective of outcome equity, there are still health inequities between urban and rural elderly residents in China. 18 China’s rural areas have not yet reached a satisfactory level of public health services, and the level of community health services is still in the initial stage. 19
In the past decade, although scholars in China and elsewhere have carried out extensive investigations and analyses of how to improve the utilization level of community health services for the elderly population in rural China, a systematic review of the difficulties and obstacles faced by the elderly population in rural China in using community health services is still lacking. This study reviews articles on the utilization of community health services by China’s rural elderly residents published in the 2013 to 2022 period. The classical model of health service utilization, the Andersen model (2013), is used as the analytical framework with which to explore the use of community health services by the elderly population in rural China, as well as the existing problems and influencing factors in the process of community health services, to effectively improve the utilization of community health services for the elderly population in rural areas and provide related suggestions.
Methods
Retrieval strategy
The article retrieval process was divided into 4 steps. The first step was to retrieve the medical subject headings (MeSH) thesaurus in MEDLINE and to determine the relevant thesaurus and their Chinese expressions. Second, subject words were used in the MEDLINE, Web of Science (WOS), China National Knowledge Infrastructure (CNKI) and Wan Fang databases for retrieval, and each retrieval data point was recorded during the process. Third, we collected the free words in each database and sorted them. Finally, we discussed and modified the expressions to determine the final retrieval expression and combination. The article retrieval expressions are shown in Table 1.
Retrieval strategy (time: 2013-2022).

Inclusion and exclusion criteria
Studies meeting the following requirements were included in this study. (i) The research site was (or included) the rural community in mainland China. (ii) The subjects included elderly individuals aged 60 and above. (iii) The main research content was the utilization status of community health services or basic public health services. (iv) The research type was a cross-sectional survey. (v) The studies were published in the 2013 to 2022 period. (vi) The studies were written in either Chinese or English.
The exclusion criteria were as follows. (i) The abstract, meeting minutes and reports of the full text could not be obtained by searching or by contacting the author. (ii) The main concern was the utilization of hospital services and related indicators rather than community health services.
Article quality evaluation tool
The Critical Appraisal Skills Programme (CASP) was used as the tool with which to analyze the quality of the article. This tool is based on the 1994 JAMA “User’s Guide,” and this study adopted the part of the programme used for qualitative research rules. 20 There are 10 items in total, and each item has 3 answers, namely, “yes” (Y), “no” (N), and “unclear” (U). The more “yes” answers there are, the higher the quality is. Based on the evaluation results, the included articles were classified into 3 levels: high, medium and low quality.21,22 To ensure the quality of the systematic review, the articles with low quality (at least 3 N or U answers) were screened out. For the CASP evaluation results. [See Additional File 1].
A total of 229 related articles were obtained’ after 2 screenings, 24 studies were analyzed, including 20 high-quality articles and 4 medium-quality articles. The article screening process is shown in Figure 1.

Flow chart of research screening.
Article analysis method
The Andersen model was used to analyze the influencing factors of community health services for the elderly population in rural areas. Andersen’s behavioral model of health service use (BMHSU) was proposed by American medical sociologist Andersen in 1968. It has been consistently developed for more than 50 years and has undergone 5 revisions and improvements, with the latest version being formed in 2013.23,24 [See Additional File 2].
The Andersen model was originally constructed to explain why individuals/families use health services and to define and measure equitable access to district health services.25-27 The 2013 version includes 4 first-level indicators, namely, situational characteristics, personal characteristics, medical practices and medical outcomes. Indicators under the dimension of situational characteristics are based on the society/community, while indicators under the dimension of personal characteristics focus on the individual. Medical practices reflect the different manifestations of health behavior, and medical outcomes represent the multidimensional evaluation of health behavior outcomes. There is a bidirectional interaction loop between the four dimensions, which represents the interaction between them. The core structure of the whole model relies on the factors of tendency, enabling resources, requirements and the unidirectional progressive relationship between them. Tendency can be understood as the sociocultural characteristics of individuals/regions, enabling resources represent health resources owned by an individual/family/region, and requirements reflect how individuals/regions evaluate their own/residents’ health status and how they deal with related health problems. 24 The Andersen model provides a theoretical framework for understanding the impact of multiple factors (individual/family, community, behavior and health outcomes) on health service utilization. Because it contains both the integrity of theoretical research and the feasibility of empirical research, it has been recognized as the most widely used and most suitable mainstream model for medical and health service research.23,24 Therefore, the Andersen model was introduced as a literature analysis tool in this study to systematically sort out, discuss and analyze the research results.
Results
Study characteristics
Among the 24 articles, 11 articles were based on official national data, and 13 articles were based on field research data, covering all of mainland China. Ten articles focused on rural areas, and the other 14 articles were from the perspective of comparing the observation indicators of urban and rural elderly residents. The elderly groups involved included permanent rural residents, elderly individuals with chronic diseases, empty-nest elderly individuals, disabled elderly individuals and ethnic minority elderly groups. The articles’ characteristics are shown in Table 2.
Articles’ characteristics.
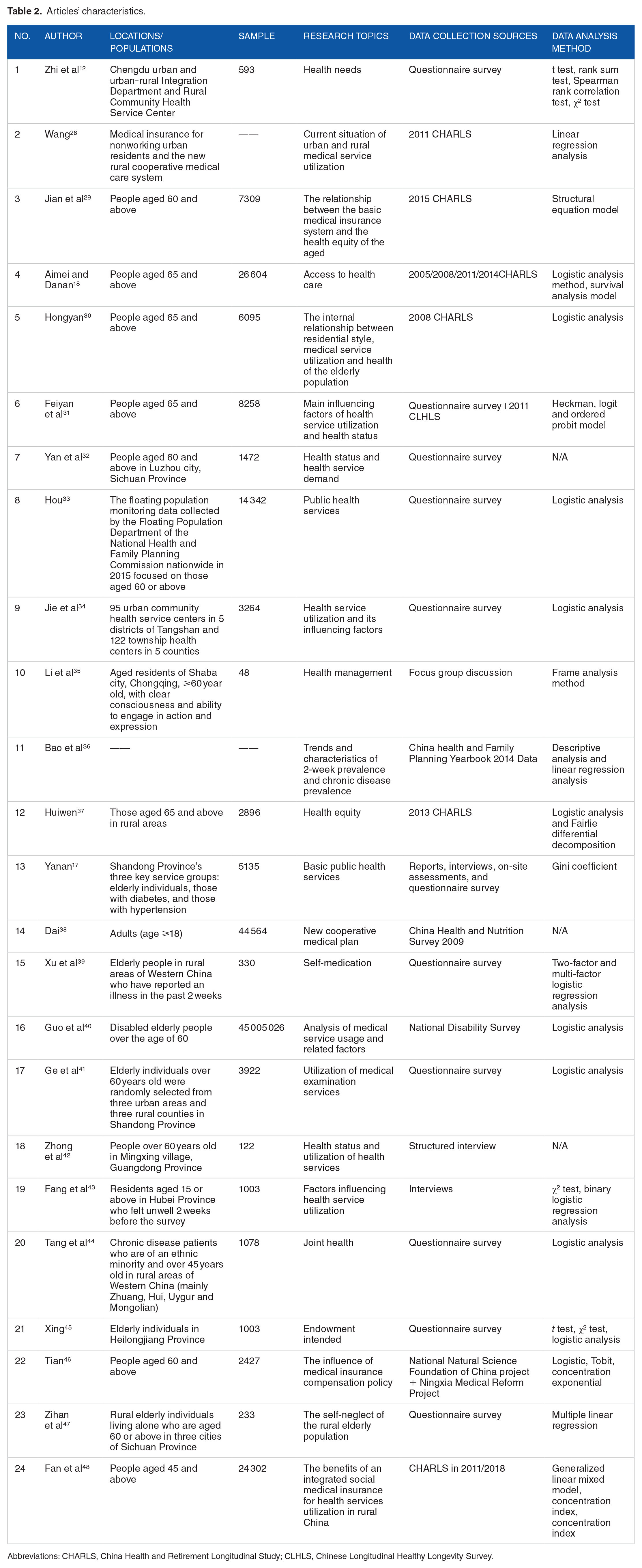
Abbreviations: CHARLS, China Health and Retirement Longitudinal Study; CLHLS, Chinese Longitudinal Healthy Longevity Survey.
Utilization of community health services for the elderly in rural areas of mainland China
The Andersen model was used as the framework for statistical analysis, and the total number of research variables included in the present review was 195. Based on the Andersen model, situational characteristics (34 times, 19 articles), personal characteristics (107 times, 22 articles), medical outcomes 14 times, 17 articles), and medical practices (15 times, 16 articles) were ranked in order. [See Additional File 3.]
Situational characteristics
There were 19 articles on situational characteristics, among which “organization,” “fund,” “community medical equipment” and “Chinese health policy” had an important impact on the use of community health services by the elderly population in rural areas. Several studies have shown that one of the main reasons for rural elderly individuals’ lack of access to a high level of health care is the “economic” level.10,49 Different regions of China have different levels of local economic development. 49 In terms of the economic level, the eastern and central regions are more developed than the western region, the plains are more developed than the mountainous areas, and cities are more developed than the countryside. Regional financial support is an important reason for the difference in health services.18,32,43,44 The lack and low utilization of health resources in rural grassroots institutions, the passive and low service quality of grassroots health service personnel, and the lack of certain supervision and assessment mechanisms also lead to the differences in community service levels between rural residents and urban residents. At the same time, compared with normal rural or urban residents, rural floating elderly residents and disabled elderly residents suffer from the restrictions of the household registration system and disability certification system, respectively, when using health services, which aggravates the unfairness of health services and requires more favorable support from the system. 40 According to this comprehensive review, “demography,” “health beliefs” and “population health indicators” were not described in the included article. [See Additional File 4].
Personal characteristics
There were 22 articles on personal characteristics. For this dimension, the influencing factors are the most abundant among the four dimensions. The factors that have an important impact on the rural elderly population’s use of community health services were “access to medical services,” “self-health assessment,” “insurance type” and “educational level.” Many studies have found that the distance and the time it takes to visit a doctor are negatively correlated with the utilization rate of health services, indicating that the accessibility of health services is the key factor influencing the choice of health services by the elderly population in rural areas. 49 Based on this conclusion, community health service stations are the first choice for rural elderly residents when seeking medical treatment34,35,49,50; however, service stations that are seriously short of health service capacity cannot meet the needs of the rural elderly population in a timely manner39,51. The demand for health services of rural elderly individuals with disease status is “rigid,” and there is a significant positive correlation between disease and health service utilization.10,34 The New Rural Cooperative Medical System (NRCMS) can significantly promote health equity 30 , and the utilization of health services by the elderly insured group is better than that by the uninsured group10,48; however, the NRCMS cannot meet the daily needs of the rural elderly population.39,43 For rural elderly residents, a higher educational level means a higher degree of demand and level of health services. In addition, variables such as “age,” “gender,” “income” and the “number of children” influence the utilization of community health services. Elderly individuals over 65 years old are the group with the highest demand for health services in the social population.29,30,32 Elderly women are more likely to use preventive services.29,40,43 The utilization of health services is high among elderly households with children. 49 Income and expenditure on health care show an inverted U-shaped trend, and when funding is no longer the main obstacle affecting the use of health services, the quality of health services is of primary concern to elderly individuals.21,41 This review found that there was no mention of “genetics” in the personal characteristics dimension in the 24 articles, and there was little discussion of “health beliefs” and “assessment needs.” [See Additional File 5].
Medical practices
There were 14 articles on medical practices. These medical practices have some positive or negative effects on the utilization of health services by the elderly population in rural areas. Among them, “family supervision and medical treatment” 50 and “exercise” 31 play a positive role. A study found that more than 2/3 of elderly residents need to take drugs on a daily basis, but their compliance level is not high, and poor drug use behaviors such as adding or reducing drugs by themselves and buying drugs by themselves are common. 12 The daily supervision of family members is very important for correcting incorrect medication and medical treatment. Physical activity increases health awareness among elderly people and has a positive impact on their utilization of health services. 31 The negative factors that were found mainly included “self-medication,” 43 “pressure,”37,42 “drinking and smoking,”37,42 and “traditional values.” 49 Elderly individuals in rural areas often use a combination of medical consultation and self-treatment to deal with their health needs. “Self-medication” is one of the main reasons why elderly people feel unwell but do not use health services. 43 Although stress does not directly affect health service utilization, it has a negative effect on the mental health of rural elderly people.39,42 Smoking and drinking affect physical health. The traditional concept of “emphasizing treatment over prevention” exists widely in rural areas and affects the level of physical health. 49 In addition, due to the low level of education and single source of health knowledge of elderly individuals in rural areas,41,44,50 they are prone to excessive medical treatment under the guidance of unhealthy medical institutions and businesses. 18 Although such behavior increases the short-term utilization of health services by the elderly population in rural areas, it easily causes dissatisfaction and distrust among residents, and it has a long-term negative impact on the promotion of rural health services. In 24 studies, there was no relevant content on the “medical service process” under the medical practices dimension. [See Additional File 6].
Medical outcomes
There were 6 articles on medical outcomes. The results of the article analysis show that even though the services provided by rural health service stations are limited, elderly residents in rural areas have higher perceived health and satisfaction with health service stations than urban residents.32,35 This finding shows that rural health service stations can meet the basic needs of the elderly population, but it also reflects the low level of health service needs of the elderly population in rural areas. The factors affecting rural elderly individuals’ evaluation of health service stations include their disease type, age and health status. The degree of satisfaction with health service stations varies with the type of disease. 35 The older the rural elderly individual is, the worse his or her self-rated health is,30,31 the worse his or her health is, and the lower his or her evaluation of health service stations is. Most studies under this dimension are carried out from the perspectives of “perceived health,” “assessed health” and “patient satisfaction,” without mentioning relevant content on “quality of life.” [See Additional File 7].
The system of influencing factors of the utilization of community health services by rural elderly residents
Based on the analysis results of the Andersen model, we summarized the influencing factors of rural elderly residents using community health services and drew the framework of influencing factors. See Figure 2.

Systematic framework of the influencing factors of the utilization of community health services by the elderly population in rural China.
Discussion
Based on the Andersen model of health service utilization, this study divides the gap in the use of community health services by the rural elderly population in mainland China into 3 categories. (i) Regarding the contradiction between situational characteristics and personal characteristics, the current health security system does not match the cognition level of the rural elderly population. (ii) Regarding the contradiction between situational characteristics and medical practices, there is a gap between the supply of health service resources in rural communities and the health needs of the elderly population. (iii) Regarding the contradiction between personal characteristics and medical outcomes, the health services provided by rural primary health services are not targeted. This study elaborates on and discusses the 3 gaps in detail and draws a schematic diagram of the gaps based on the research results. See Figure 3.
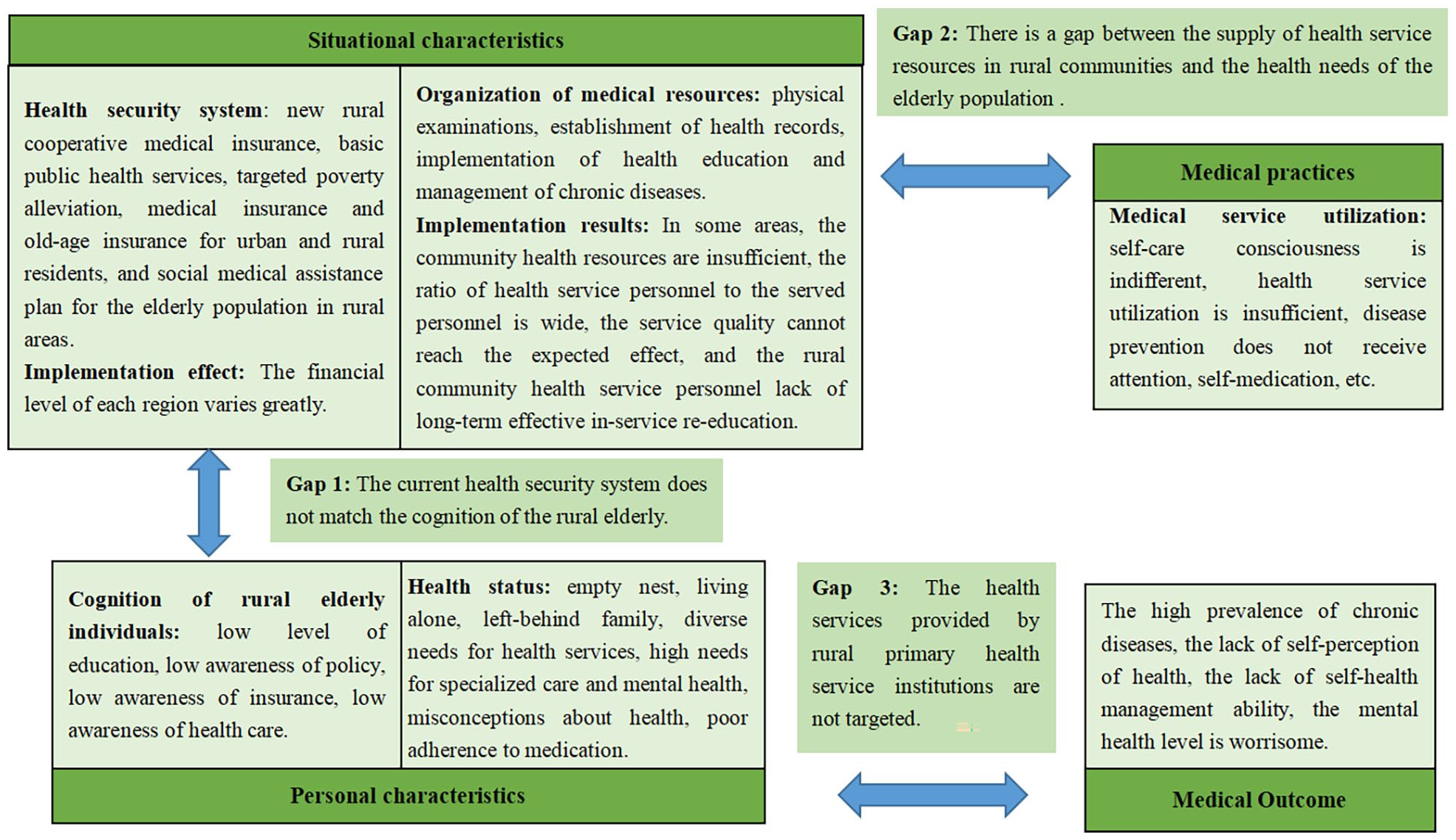
Schematic diagram of the gap in health services for the elderly population in rural areas of mainland China.
Gap 1: The current health security system does not match the cognition level of the rural elderly population
At present, the reasons for the unequal health services for the elderly population in rural areas are mostly economic in nature. For rural residents, income from agricultural activities is their main source of income52,53. However, different from the young labor force, the labor force of rural elderly individuals rapidly diminishes as they grow older, leading to a decrease in economic benefits. Therefore, their financial resources are mainly from family members. However, the support of children is not stable, and the pension function of rural families is easily weakened with the change in the population structure. Thus, the income source of the elderly population in rural areas is often unstable. Chronic diseases have swept through China’s rural areas, 54 the cost of health services has become a heavy burden for elderly individuals in rural areas, and medical expenditure accounts for a large part of their daily expenditure,55-57 while only a few chronic diseases and medicines are covered by the insurance system. 58 As a result of low income and high expenditure, rural elderly individuals fall into deep poverty. In the face of risks, especially disease risks, rural elderly individuals have insufficient financial capacity to pay.39,43,51
It is very important to establish and improve the health security system to solve the economic difficulties of the rural elderly population. The Chinese government has launched many measures, such as “The New Rural Cooperative Medical Insurance” and “The Rural Elderly Social Medical Treatment Plan” issued in 2003, the basic public health services launched in 2009, and the implementation of the “Precise Poverty Alleviation” policy in early 2015. The government has also allowed rural elderly people to participate in urban and rural resident medical insurance and urban and rural resident old insurance.59-63 Through continuous explorations and efforts, the living standards of the elderly population in rural areas have been greatly improved. The relevant policies and measures implemented by the Chinese government and the strength of implementation should be highly appreciated. However, at the same time, the mismatch between the current health security system and the cognition of the rural elderly population is also very obvious.
This study found that although governments have promulgated many policies to promote the use of health services by the elderly population in rural areas, the elderly population in rural areas generally has a low level of education and a lack of correct awareness of diseases. Additionally, these elderly individuals are unable to accurately and actively obtain, understand and use relevant health policy information. Doctors, family members and friends are the main channels for rural elderly people to obtain health information.36,41 The single source of information and the quality of information are easily influenced by human beings, which ultimately leads to the current situation of a low utilization rate of rural health services in mainland China. Furthermore, local governments undertake the main responsibility for financing the old-age health security system. 39 Therefore, the difference in financial capacity between local governments leads to the great difference in rural elderly individuals’ access to medical and health services in different areas. Therefore, the opportunities for the elderly population in rural areas to obtain health care services are still very limited.
Gap 2: There is a gap between the supply of health service resources in rural communities and the health needs of the elderly population in these areas
Since it was officially launched in 2009, the basic Public Health Service Project has grown to include 14 services. 64 The policy stipulates that rural grassroots health service stations should be required to provide free services such as physical examinations, health records, health education and chronic disease management for the elderly population in rural areas. 65 Basic public health services have been built on the basis of public services for all and the connotation behind this basic right. Although the basic public service system has promoted the equality of health opportunities, there are still health inequities among elderly residents from the perspective of outcome equity. Studies have shown that the self-health care consciousness of the rural elderly population is insufficient, even though health services are provided free of charge. In rural areas, the distance to designated care providers is too far, and it is difficult to obtain health services. In particular, elderly patients with chronic diseases or poor activities of daily living may not use health services because of the transportation and time costs involved in doing so. Rural elderly individuals are also less likely to be reminded to use such services than urban residents. According to the statistical Bulletin on the Development of China’s Health Undertakings, by the end of 2020, the number of visits to primary medical and health institutions in China had decreased by 410 million, and there were 1.52 beds and 1.62 staff members in township health centers for every 1000 rural people, indicating insufficient community health resources. Moreover, the service workers in rural communities have a low professional level, a lagging concept and the view of “valuing medical treatment over quality,” leading to passive service. Although physical examinations can identify high-risk groups and documentation can dynamically master the disease status of chronic disease patients, the documentation and physical examination services will become meaningless without the follow-up services of grassroots staff and the basic records of personalized chronic disease management.
Gap 3: The health services provided by rural primary health service institutions are not targeted
Chronic diseases are prevalent among elderly individuals in China’s rural areas, most of whom suffer from one or more chronic diseases 66 . At present, there is no cure plan for all kinds of chronic diseases. The most active method is to prevent them in advance by slowing down the disease process to prevent the disease from developing serious complications.67,68 Due to the low disease cognition level among elderly individuals in rural areas, in their form of cognition, “being able to eat and walk” means being healthy. However, the intake of food with high fat content, high stress, 42 less physical exercise, 31 smoking, alcohol abuse37,42 and other high-risk behaviors are all important reasons for the increase in chronic diseases. In rural areas, the wrong idea of “emphasizing governance over prevention” is widespread.
At the same time, the poor medication compliance level of the elderly population in rural areas is also one of the reasons for the poor control of chronic diseases in rural areas. The behavior of irregular drug use, such as stopping medication at will and not taking medication regularly, seriously damages the physical health of elderly patients with chronic diseases. Communities are the backbone of primary prevention and should play the most important role. However, at present, primary health service institutions have not been able to provide satisfactory and targeted specialized care. The review also found that in daily life, older rural people often use a combination of medical consultation and self-treatment to deal with their health needs. “Self-medication” is not only one of the main reasons why elderly people feel unwell but do not use health services but also causes serious consequences, such as the inability to control side effects or delayed illness and drug resistance. In regard to exploring the causes of “self-medication” behavior, first, the incomplete and ill-timed revision of food and drug regulatory laws and regulations is one of the main reasons. Second, the professional level of some drug-related personnel in rural areas is low, rural areas rarely have the opportunity to receive food and drug safety publicity, rural elderly individuals lack the correct knowledge of drug use, residents lack legal knowledge of drug devices, and the serious lack of self-health management ability also has an important impact. To improve profits, some undesirable businesses have wrongly induced the elderly population to consume medications, leading to blind drug use, which also provides conditions for the elderly population to self-medicate.
In addition, the problem of left-behind elderly individuals in rural areas is very serious. In their old age, most elderly individuals live only with their spouses, and many of them live alone only after the death of their spouses in an empty-nest state. Rural elderly individuals have a high rate of demand for spiritual support in their later life. However, at present, it is difficult for rural basic health service institutions to provide services for mental needs in a timely manner. Mental services are almost nonexistent, 47 and the mental health level of the elderly population in rural areas is worrisome.
In fact, aging is a worldwide issue, and some Western countries have been engaged in research on healthy aging for a long time. For example, the USA, Japan, Germany, Sweden and other countries all have successful health service systems for use by elderly individuals. 69 After studying the systems of these countries, we found that there is a common characteristic among them, namely, mutual assistance. Whether it is mutual assistance between the elderly or between multiple generations or paid or voluntary old-age care mediated by the government, the core issue is that the government no longer plays a leading role in rural old-age care but rather advocates the whole society to share the task of old-age care together. 70 This can not only significantly reduce the government’s pension burden but also form a benign closed-loop pension system. Therefore, this successful experience is worth paying attention to in China. However, the system of “mutual assistance for the aged” becomes slightly “acclimatized” in China after being separated from the social environment of Western countries.71,72 Western countries have small populations, a relatively perfect degree of social development, and a small number of economic differences between urban and rural areas. Thus, a system of “mutual assistance for the aged” can be implemented by taking advantage of sufficient resources for the aged in rural communities. However, in China’s rural areas, the aged population is a large group, health service resources are distributed, elderly residents’ cultural level is low, and the traditional concept of a “family pension” makes the effect of carrying out a system of “mutual endowment” not very strong at this stage. Therefore, the Chinese government still needs to and will play an important role in such systems for a long time. However, with the rapid development of the national economy, the improvement of national literacy and the continuous exploration of Chinese scholars, China will eventually combine the national conditions and the successful experiences of other countries to create similar systems with Chinese characteristics, service targeting and high-quality rural elderly health services.
Future research directions and outlook
Through this systematic review of the 24 included studies, it was found that there is a lack of systematic and consistent research on the health service utilization of the rural elderly population in mainland China. Combining statistical research variables with Andersen’s model of health service utilization, it was found that there are many research indicators under the four dimensions that are not related to relevant content. These indicators under the four dimensions of the framework of the Andersen model are as follows: “demography,” “health beliefs” and “population health index” under the situational characteristics dimension; “inherited genes,” “health beliefs,” and “assessment needs” under the personal characteristics dimension; “medical service process” under the medical practices dimension; and “quality of life” under the medical outcomes dimension. These research indicators can also have a positive or negative impact on the use of community health services by the rural elderly population. The findings show that current research in this field is still not systematic; they also suggest that future research can use the Andersen model of health service utilization as a guiding framework to comprehensively interpret the utilization of community health services for the rural elderly population in combination with China’s national conditions.
Limitations
Although this study collected articles on health service utilization by the elderly population in rural areas of mainland China from 2013 to 2022, only articles written in Chinese and English were included, which may have introduced a certain publication bias. In addition, the Andersen model of health service utilization was introduced as a review tool. However, to ensure a systematic review, given the flow of time and different national conditions, the research content involved in the Andersen model still cannot cover all the influencing factors. Despite these limitations, this study holds some significance for explaining the barriers to health service utilization by the elderly population in rural areas of mainland China.
Conclusion
In mainland China, the provision of community health services to the rural elderly population has improved significantly. However, the current situation of the utilization of community health services by the rural elderly population in mainland China is not optimistic. This finding means that under the current leadership of the government, it is necessary to integrate the strength of multiple departments to cooperate in improving the welfare system, policy publicity, health education, financial support, system guarantees and resource exchange and sharing for the elderly population in rural areas and to jointly promote community health services for the elderly population in rural areas.
Supplemental Material
sj-docx-1-his-10.1177_11786329221134352 – Supplemental material for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations
Supplemental material, sj-docx-1-his-10.1177_11786329221134352 for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations by Shanshan Deng, Chenchen Zhang, Xing Guo, Hekai Lv, Yanyan Fan, Zhuoxin Wang, Dan Luo, Xiaoxia Duan, Xinying Sun and Fuzhi Wang in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329221134352 – Supplemental material for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations
Supplemental material, sj-docx-2-his-10.1177_11786329221134352 for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations by Shanshan Deng, Chenchen Zhang, Xing Guo, Hekai Lv, Yanyan Fan, Zhuoxin Wang, Dan Luo, Xiaoxia Duan, Xinying Sun and Fuzhi Wang in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329221134352 – Supplemental material for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations
Supplemental material, sj-docx-3-his-10.1177_11786329221134352 for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations by Shanshan Deng, Chenchen Zhang, Xing Guo, Hekai Lv, Yanyan Fan, Zhuoxin Wang, Dan Luo, Xiaoxia Duan, Xinying Sun and Fuzhi Wang in Health Services Insights
Supplemental Material
sj-docx-4-his-10.1177_11786329221134352 – Supplemental material for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations
Supplemental material, sj-docx-4-his-10.1177_11786329221134352 for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations by Shanshan Deng, Chenchen Zhang, Xing Guo, Hekai Lv, Yanyan Fan, Zhuoxin Wang, Dan Luo, Xiaoxia Duan, Xinying Sun and Fuzhi Wang in Health Services Insights
Supplemental Material
sj-docx-5-his-10.1177_11786329221134352 – Supplemental material for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations
Supplemental material, sj-docx-5-his-10.1177_11786329221134352 for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations by Shanshan Deng, Chenchen Zhang, Xing Guo, Hekai Lv, Yanyan Fan, Zhuoxin Wang, Dan Luo, Xiaoxia Duan, Xinying Sun and Fuzhi Wang in Health Services Insights
Supplemental Material
sj-docx-6-his-10.1177_11786329221134352 – Supplemental material for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations
Supplemental material, sj-docx-6-his-10.1177_11786329221134352 for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations by Shanshan Deng, Chenchen Zhang, Xing Guo, Hekai Lv, Yanyan Fan, Zhuoxin Wang, Dan Luo, Xiaoxia Duan, Xinying Sun and Fuzhi Wang in Health Services Insights
Supplemental Material
sj-docx-7-his-10.1177_11786329221134352 – Supplemental material for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations
Supplemental material, sj-docx-7-his-10.1177_11786329221134352 for Gaps in the Utilization of Community Health Services for the Elderly Population in Rural Areas of Mainland China: A Systematic Review Based on Cross-Sectional Investigations by Shanshan Deng, Chenchen Zhang, Xing Guo, Hekai Lv, Yanyan Fan, Zhuoxin Wang, Dan Luo, Xiaoxia Duan, Xinying Sun and Fuzhi Wang in Health Services Insights
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Anhui Province Social Science Planning General Project (No. AHSKY2021D24), the Humanities and Social Science Key Project of Education Department of Anhui Province (No. SK2019A0191) and the Postgraduate Research Innovation Program of Bengbu Medical College (No. BYYCX21024).
PROSPERO Registration Number:
CRD42021226794
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
Fuzhi Wang is the guarantor. Shanshan Deng drafted the manuscript. Chenchen Zhang and Xing Guo examined the inclusion and exclusion criteria, Hekai Lv produced the article screening process, Yanyan Fan collected literature, Zhuoxin Wang discussed the shortcomings of the elderly rural population in mainland China in the field of health service utilization, Dan Luo, Fuzhi Wang, and Xiaoxia Duan reviewed the quality of this review, and put forward the final amendment, we also have consulted Professor Xinying Sun of Peking University about the revision of the paper.
Authors’ Information
Not applicable.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article or its supplementary information files.
Consent for Publication
Not applicable.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Bengbu Medical College (No. 2017054), and his study did not involve the use of informed consent to participate.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.