
Abstract
An evaluation of accessibility, appropriateness, acceptability and efficiency of telephone consultations, implemented at Monash Health Refugee Health and Wellbeing (MH RHW) throughout the COVID-19 pandemic, was conducted. A convergent mix-methods design was used, with both patients (n = 50) and clinicians (n = 11) participating in a survey, and two focus groups (n = 14) involving clinicians being conducted. Service utilization data was sourced from the MH RHW database. During May to December 2020, 61% (n = 3012) of the consultations were conducted by telephone, 42% (n = 11) of these required interpreters in a 3-way conversation Most patients were satisfied with telephone as a medium for providing care and with the quality of telephone-based care. Similarly, clinicians considered telephone consultations to be an acceptable mode-of-care for most patients during the pandemic, however, expressed caution in relation to certain patient cohort. Finally, the provision of care by telephone was considered no more efficient than face-to-face service provision, as reflected in the time required for each consultation, with some clinicians reporting adverse workload outcomes. This study highlighted the benefits and challenges of telephone consultations from patient and clinician perspectives. It also highlighted the types of patients that may not be suited to telephone consultations. Overall, this study showed that telephone service delivery is a feasible option in providing care to people of refugee background and should be considered in future decisions as an ongoing Medicare (Australia’s universal healthcare insurance scheme) billing item. However, clinical discretion should prevail in determining the most appropriate means of delivering care.
Keywords
Background
In March 2020, to combat spread of the COVID-19 virus, the Australian Government endorsed item numbers that subsidised the provision of telehealth services, including telephone consultations, through Australia’s universal healthcare insurance scheme, Medicare. This was to minimise unnecessary attendance in person for consultations at acute and non-acute health services. 1 Accordingly, telehealth was preferentially introduced across Monash Health, Victoria’s largest public health service.
Monash Health Refugee Health and Wellbeing clinic (MH RHW) is located in a Monash Health community facility in South-East Melbourne, providing primary and specialist care to asylum seekers and refugees. 2 Recent research has demonstrated persisting poor general health among adult refugees during the first 3 years of resettlement in Australia, together with an association between poorer general health and economic settlement stressors. 3 Humanitarian groups may be at greater risk for exposure to COVID-19 and increased severity of the disease due to the combined impacts of compromised living conditions and casualised, often crowded, poorly regulated employment, together with language and health care access barriers, and high rates of poor health and multi-morbidities. 4 Thus, it was imperative to ensure uninterrupted access to high-quality health care, which incorporated the provision of COVID-related information and services, to this vulnerable group.
MH RHW opted to provide health care by telephone throughout the pandemic. Telephone access was in preference to telehealth as resources necessary to use telehealth, such as owning a personal electronic device, internet connection with sufficient speed and data, and adequate language command to follow telehealth connection guidelines, was deemed to be inconsistent and often lacking among MH RHW patients. 5 This was consistent with existing evidence that suggests telehealth use is lower in communities with higher rates of poverty. 6 Service-based limitations relating to technological capacity to engage clinicians, patients and interpreters was also a factor in decision making.
Providing care by telephone is not new and has been successfully employed to address access issues in rural and remote areas, and in managing health service demand.7-9 Previous research suggests that telephone consultations were considered an appropriate mode-of-care by both doctors and patients in addressing single, non-complex concerns, 10 with high levels of patient satisfaction reported in the primary care. 11 Further, a systematic review on the impact of telephone triage and consultation found that at least 50% of calls can be effectively managed by telephone advice alone with a subsequent reduction in demand for General Practitioner (GP) services. 11
However, there are inconsistencies in available evidence relating to the applicability of telephone consultations across different population and patient groups, and acceptability of this mode-of-care amongst healthcare providers. For example, a systematic review that collated evidence on the use of telephone consultation as an alternative to face-to-face service provision concluded that telephone consultations offer an appropriate alternative option in certain situations, stating however, that there is a lack of high-level evidence for the use of telephone consultations in a primary care setting. 12 A qualitative study about the impact of the COVID-19 pandemic on the core functions of primary care found that GPs viewed telephone consultations as problematic due to the absence of non-verbal language cues and challenges associated with patients being able to adequately express themselves over the phone. 13 Another recent study investigated a ‘telephone first’ approach in which patients requesting an appointment were first required to speak to a GP on the telephone, after which a decision was made as to whether the patient required a face-to-face consultation, whether they could be directed to an alternative health-care provider or whether the concern could be satisfactorily and appropriately dealt with on the telephone. The study concluded that whilst many health concerns can be addressed over the telephone, the approach does not suit all patients and more research is required to understand how telephone consultations meet the needs of different patient groups. 14 Additionally, while previous research has highlighted the challenges and advantages of using telephone interpreters for patients with limited language proficiency,15,16 investigation into the appropriateness and acceptability of the 3-way remote telephone communication between the patient, clinician and interpreter has not been conducted.
This study aimed to evaluate the use of telephone-based consultations in the provision of care for refugees and asylum seekers with limited English language proficiency, using interpreters as required, in the context of both primary and specialist care clinics, with a view to inform post Covid-19 service delivery. In particular, the study focused on the accessibility and appropriateness of telephone consultations for the MH RHW patients, together with perceived efficiency of this mode-of-care and its acceptability amongst clinicians and patients.
Methods
Setting
The study was set at MH RHW, a State-funded refugee-focused health service, located in a community health facility in South-East Melbourne, Victoria. MH RHW provides integrated and intensive primary care and specialist services to asylum seekers and refugees experiencing significant vulnerability, complex health needs and restricted access to Medicare. The service is comprised of a multi-disciplinary team, including GPs, refugee health nurses (RHNs), infectious diseases physicians, paediatricians, bi-cultural workers, community development workers, psychiatrists, and counsellors, with access to collocated pharmacy and pathology services. 2
Design
A convergent mix-methods design was used in which qualitative and quantitative data were collected and organised separately and then merged to provide complementary evidence to answer the research questions. 17 The study consisted of a survey of MH RHW patients who received telephone consultations from the clinic, and a survey and focus groups with MH RHW clinicians involved in the provision of care by telephone, May to December 2020. Data on service utilisation during May to December 2020 was sourced from the routinely updated Monash Health database.
Participant recruitment
Patients were contacted over the telephone by a bi-cultural community worker after the appointment and invited to share their experience. The recruitment was conducted until the targetted number of 50 participants was reached. Patients were excluded if they were younger than 18 years of age or were unable to provide informed consent. Verbal information about the study was provided to those who expressed interest and verbal consent to participate was audio recorded.
MH RHW clinicians were invited to participate in an online survey by email. Information about the study was included with the request and consent to participate was implied by the completion of the survey. Regardless of the participation in the survey, MH RHW clinicians were invited to participate in a focus group to explore their experience of providing and/or supporting care by telephone. Two focus groups were held during December 2020. All focus group participants provided written informed consent.
Tools and data collection
The patient and clinician surveys were developed by the research team following a comprehensive literature review. The patient survey was comprised of questions pertaining to both the quality of telecommunication and the quality of the health care received during the telephone consultation. Various aspects of the telephone consultation were compared with standard face-to-face consultations, and acceptability of telephone consultations was explored by an expression of willingness to participate in telephone consultations in the future. Some questions were adapted from earlier studies on the utilisation of telehealth.18,19 The draft survey was reviewed by 2 MH RHW clinicians in leadership positions and subsequently amended to address additional areas of interest specific to this patient cohort. The survey was then reviewed by a MH RHW bi-cultural worker to ensure its interpretability and cultural appropriateness. The survey was administered over the phone by 2 experienced bi-cultural workers (CY and RA) both of whom routinely communicate with MH RHW patients regarding appointments. The bi-cultural workers were fluent in several languages and, in addition to English, were able to administer the survey in Dari, Hazaragi, Urdu, Farsi and Arabic. Interpreters were otherwise used as required. The clinician survey was self-administered and consisted of both open-ended and closed questions and aimed at collecting information about the participants’ satisfaction with administrative and operational aspects of remote consultations. The survey questions also explored perceived ability to address patient needs, together with any potential risks that this mode-of-care poses for either patients or clinicians.
The focus group schedule was developed based on the literature review and consultations with the MH RHW leadership team. Two 1-hour focus group discussions were conducted via an online video-conferencing platform (CISCO Webex). An experienced qualitative researcher (MK) facilitated the discussion that was guided by a theme list with prompting questions to explore clinicians’ experiences of providing/supporting telephone-based consultations, the efficiency of the process and its appropriateness in providing routine clinical care to asylum seekers and refugees post COVID-19. Additionally, clinicians were encouraged to discuss any other issues relevant to the study. All focus group discussions were audio recorded and summarised according to the topics discussed.
Data on service utilisation during May to December 2020 was extracted from a Monash Health database.
Analysis
Quantitative data
Initially, frequency distributions were performed to analyse patient and clinician surveys, and service utilisation data. For the patient survey, bivariate analyses using Fisher’s exact test was also performed to determine whether there was an association between specific demographic and clinical characteristics, and negative experience of the telephone consultation. All analyses were completed using IBM SPSS Statistics for Windows.
Qualitative data
Qualitative exploratory descriptive analysis,
20
oriented toward summarising the informational contents of the data to understand the perspectives of the clinicians involved in the provision of telephone consultations, was used to analyse the focus group data. The analytical process was iterative. First, the written summaries of the audio recordings were reviewed and all identifiable details were removed. Then, data were categorised into themes defined as relevant for the evaluation of clinicians’ experiences providing telephone consultations. A list of data-driven codes was then generated, and the pre-existing categories were modified to accommodate new insights from the data. Data saturation was assumed when no new codes and/or themes emerged from the data.
21
The codes and categories were then reviewed by all members of the research team. Interpretation disagreements were resolved by consensus. Data organisation was assisted by NVivo12 software.
Data integration
Narrative integration of quantitative and qualitative data using weaving approach
22
was applied to answer research questions on accessibility, appropriateness, acceptability, and efficiency of the telephone consultations at the MH RHW.
The study was approved by Monash Health Human Research Ethics Committee RES-20-0000-635A.
Results
Service utilisation
During May to December 2020, MH RHW service providers conducted 4964 consultations, with the majority conducted by GPs (40% (n = 1964)) and nurses (40% (n = 1966)). Most consultations were conducted by telephone (n = 3092, 61%), however, variation in uptake was evident across clinicians, from 17% (n = 62) uptake by a Community Development Worker to 83% (n = 559) uptake by a psychologist (Table 1).
MH RHW consultations by profession, May to December 2020.

More broadly, utilisation of telephone consultations reflected the dynamics of pandemic response measures introduced by the Victorian government during 2020. For example, during the strict lockdown period in Melbourne, August to September 2020, nearly 80% of all consultations at MH RHW were conducted by telephone (Figure 1).

Consultations provided at MH RHW, May to December 2020 Number of consultations and mode of service delivery.
Patient data
Out of the 54 MH RHW patients approached, 50 completed a survey about their telephone consultation experience. Most of the patient-participants responded to the survey in English (66%, n = 33), 6% (n = 3) required an interpreter, while for the remainder (28%, n = 14), the survey was administered in one of the languages known to the bi-cultural workers (Dari, Hazaragi, Urdu, Fasi and Arabic). Most of the participants were review patients (96%, n = 48); 64% (n = 32), attended a GP consultation, and 22% (n = 11) a mental health consultation. Compared to the usual MH RHW patient cohort, the sample was slightly skewed towards female participants (68% compared with the usual 52%). Other demographic and clinical characteristics were representative of the typical patient cohort of the service. Patient-participant characteristics are presented in Table 2.
The demographic and service utilisation characteristics of patients who participated in the study (N = 50), n (%).

Most patient-participants (94%, n = 47) reported that they felt safe during the telephone consultation, and did not find the process confusing (96%, n = 48) or concerning (98%, n = 49). Regarding the quality of the connection, all patients (100%, n = 50) were able to hear and understand the clinician and the interpreter, most (94%, n = 47) answered that the clinician and the interpreter were able to hear and understand them, and 98% (n = 49) were able to find a suitable place, without disruptions, to take the telephone call. All patients (100%, n = 50) understood that the consultation would be conducted over the telephone when it was booked (Table 3).
The perception of the quality of telephone consultation of patients who participated in the study (N = 50), n (%).

Regarding the quality of the healthcare received during the telephone consultation, most (96%, n = 48) reported that the clinician listened and understood their health concern, and that they were able to ask questions and understood how to look after their health after the consultation. Similarly (94%, n = 47), reported that their health concern was addressed during the consultation and that they understood how to get help if they felt unwell. Most (92%, n = 46) felt comfortable discussing personal or confidential information over the phone and thought that the amount of time spent with the clinician was adequate to address their health concern (Table 3).
The patients were then asked to compare their experience during the telephone consultation with previous face-to-face consultations at the clinic. A majority of patients reported their experience of telephone consultations to be as good or better than previous face-to-face consultations across a range of domains. Domains explored included: ease of attending the appointment, associated cost, the amount of time spent with the clinician, the overall quality of the telephone consultation, comfort of sharing personal or confidential information, confidence that their health concern would be addressed, feeling the personal connection with the clinician, and ability to explain or show their physical problem (Table 4). Eighty six percent (n = 43) responded that they would want to use telephone consultation again instead of face-to-face consultation.
A comparison of telephone and face-to-face consultations by patients who participated in the study (N = 50), n(%).
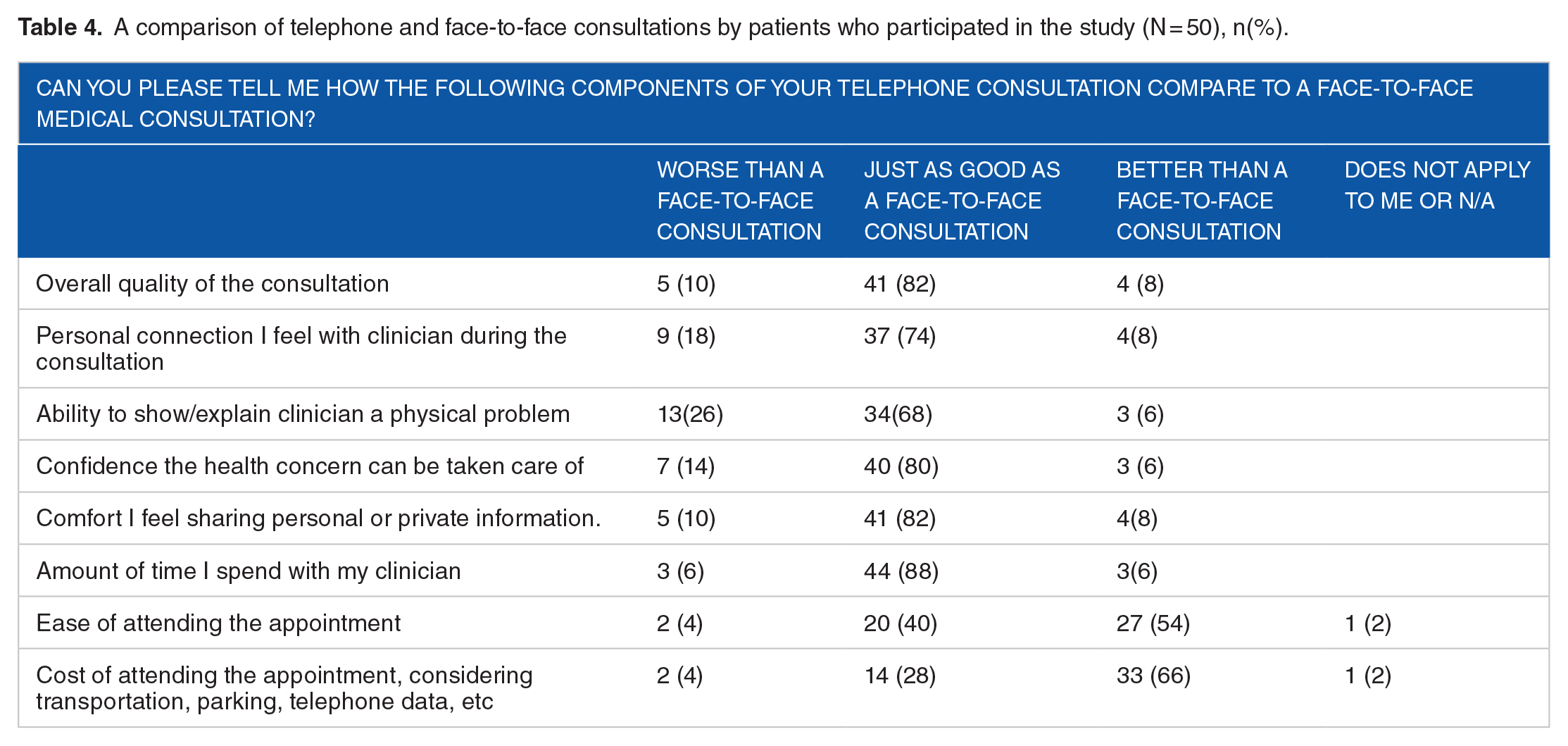
Bivariate analysis revealed that, compared to asylum seekers, refugees were more likely to respond that their health concern had not been addressed during the telephone consultation (0% (n = 0) vs 18% (n = 3), P = .029, respectively); and that the amount of time spent with the clinician was shorter compared to face-to-face consultation (0% (n = 0) vs 18% (n = 3), P = .029, respectively). No other statistically significant associations between patient demographic and clinical characteristics, and negative experience of the telephone consultation were found.
Clinician data
Out of the 22 invited clinicians, 11 completed a survey and 14 participated in 2 focus groups exploring their experience in providing telephone-based care. Table 5 provides details of participating clinicians by profession.
Clinician participation in survey and focus groups, by profession.

Adapting clinical practice
The predominant view of the clinician-participants was that the telephone consultations presented a ‘safe and relatively reliable [service delivery] option’( Specialist consultant 1) when the face-to-face care was compromised by the COVID-19 restrictions. Most agreed or strongly agreed that they were able to assess psychological signs and symptoms (73%, n = 8) and clients’ health related behaviours (73%, n = 8). Further, most felt they were able to communicate effectively with the clients (55%, n = 6) and build rapport (55%, n = 6) and were satisfied with the care they delivered (55%, n = 6). The ability to assess physical signs and symptoms, or functional performance was rated much lower (9%, n = 1 and 27%, n = 3, respectively) (Table 6).
The satisfaction with the telephone consultation as perceived by clinicians who participated in the study (N = 11), n (%).

While most clinicians (64%, n = 7) were satisfied or very satisfied with the sound quality, ease of use and technical reliability during the telephone consultations, it was acknowledged, that when providing care by telephone, they had to adapt the way they consult to ensure optimal clinical care. The majority (82%, n = 9) reported that they had to do more screening, ask more deliberate questions and be more mindful of the choice of words. As well as this, the clinicians recounted always being mindful of the most severe possible clinical outcome for the patient, and often resorting to more frequent follow-up consultations to mitigate clinical risk (Textbox 1, quote 1).
Themes that emerged during the clinician focus group discussion and illustrating quotes.
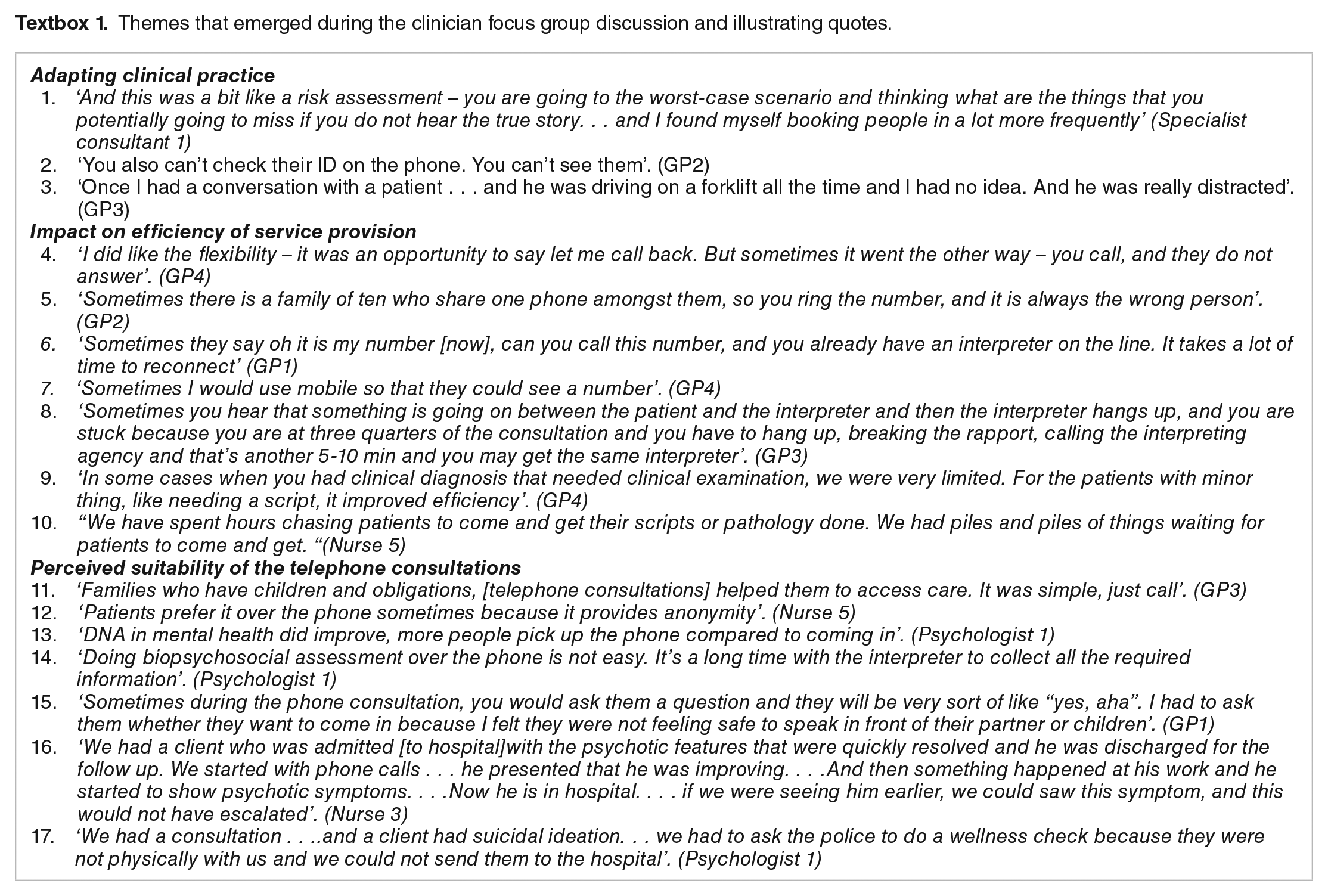
Clinical risk was identified during telephone consultation by 55% (n = 6) of the respondents. One such risk related to the confirmation of patient identity, with clinicians describing additional endeavours required to cross-check demographic data in the absence of visual identification to ensure they were speaking with the correct person (Textbox 1, quote 2). Patient safety was also identified as a participant concern, with clinicians describing the need to routinely confirm that the patient was in a safe environment prior to commencing the consultation call (Textbox 1, quote 3). In the event of health-related risk, patients were requested to present to MH RHW for further assessment, attend the nearest Emergency Department or visit a COVID19 screening clinic, with the option of an ambulance being dispatched to the patient’s place of residence if required.
Additionally, adverse clinician impacts associated with care by telephone were reported by 45% (n = 5) of the participants. Specifically, concerns were raised about potential missed diagnosis and the ability to complete comprehensive risk assessments for mental health patients and other particularly vulnerable patients. The experience of providing care devoid of non-verbal communication cues critical to establishing rapport and formulating clinical opinion, undermined clinicians’ confidence and was described as ‘anxiety provoking’ (Specialist consultant 1).
Impact on efficiency of service provision
All participants reported that use of telephone consultations did not result in increased clinical efficiency with the same number of patients receiving telephone consultations per day as would usually receive face-to-face consultations. Most clinicians (55%,and n = 6%) reported that, on average, the same amount of time was required for telephone consultations as face-to-face consultations (Table 6).
Several operational issues were identified as infringing on the efficiency of service provision by telephone. For example, whilst clinicians commented on the potential advantage of telephone consultations in offering a timely and accessible care alternative for patients, at times the patients saw telephone consultations as being less time constrained and, as such, were not always punctual in responding to scheduled consultation calls (Textbox 1, quote 4). Additional difficulties included frequently changing or disconnected patient contact numbers and the apparent reluctance of patients in responding to calls with a hidden caller identification number. Call hesitancy was attributed to patient privacy and/or legal concerns, with clinicians attempting to overcome this barrier through education and, where possible, the use of call-identifying mobile devices (Textbox 1, quotes 5-7).
A variety of interpreter-related issues were also identified as variables likely to compromise service efficiency, with all clinicians experiencing significant challenges in conducting 3-way telephone consultations. It was stressed, that the quality of interpreting service was crucial, with individual interpreter characteristics having the potential to negatively impact on the quality of the consultation. Technical factors were also detrimental, with telecommunication issues, phone disconnections, delayed interpreter connections, compromised sound quality and compromised ability to judge the quality of interpreting being commonplace (Textbox 1, quote 8).
There was a notable difference in opinion of focus group participants between doctors (GPs and medical specialists) and nurses when the discussion emerged about the impact of providing clinical care by telephone on the efficiency of service provision. From doctors’ perspective, efficiency was largely determined by the nature of the consultation being provided. Routine consultations relating to minor issues, follow-up calls and prescription reviews, for example, were considered well aligned with telephone-based service delivery, thereby affording optimal service efficiency. More complex consultations, such as those requiring physical examination or initial comprehensive biopsychosocial assessment were, however, considered to be more thoroughly and efficiently achieved in a face-to-face context. Nurses reported greater inefficiency with telephone-based consultations, regardless of context, than would ordinarily be achieved with face-to-face service delivery. This was largely due to the additional administrative burden associated with following-up patients to coordinate the collection of scripts, pathology requests and other screening referrals post care by telephone (Textbox 1, quotes 9-10).
Perceived suitability of the telephone consultations
While most clinicians (55%, n = 6) responded that they preferred face-to-face service delivery, the majority were both keen to continue providing telephone consultations (82%, n = 9) and willing to pursue patient consultation over the telephone in the future (91%, n = 10) (Table 6).
Commenting on the suitability of the telephone consultations to the MH RHW patients, the clinicians explained that while some patients clearly benefitted from the opportunity to receive a consultation in the comfort of their home, for others this option was less appropriate and might have reduced access to care. Patients who benefitted from receiving the consultations over the telephone were described by the clinicians as patients caring for young children, patients with low work security who found it difficult to take a day off work to attend the clinic, patients with limited mobility, and those for whom the attendance in person required long-distance travel. It was also noted that health care access improved for those who historically have been poor attenders of face-to-face appointments and for some patients requiring mental health services. In this regard, the clinicians felt that patients valued the flexibility and perceived anonymity of the telephone-based care (Textbox 1, quotes 11-13).
Patients, for whom telephone consultations suited less, included complex patients who required physical examination and/or detailed biopsychosocial assessment, children, and patients with hearing impairment. New patients were specifically mentioned due to the possible difficulty in establishing rapport critical in the initial stages of care. Safety concerns that might impede the access were also raised as contra indicators for telephone consultations, particularly for patients living in a situation of family violence and patients with limited family and social support for whom face-to-face service delivery might contribute to therapeutic outcomes (Textbox 1, quotes 14-15).
Further concern was raised in relation to the appropriateness of telephone consultations for some mental health patients. Despite the observation regarding the improvement in failure to attend rates, it was noted that telephone consultations with some mental health patients may not bring the same benefit as consulting the patient face-to-face because of inability to triangulate the patient narrative with nonverbal behaviour clues. A separate concern was discussed regarding mental health patients who may experience suicidal episodes and the difficulty of addressing this type of concerns, which require immediate response, over the telephone. (Textbox 1, quotes 16-17).
Discussion
The evaluation demonstrated that the provision of telephone consultations to patients of refugee and asylum seeker background was a workable solution during the pandemic response. However, challenges encountered across various domains of service provision must be considered should this initiative continue to be incorporated as an optional mode-of-care post-COVID-19. Table 7 summaries the perceived benefits and challenges associated with telephone-based consultations from the perspective of both clinicians and patients.
Perceived benefits and challenges associated with telephone-based consultations in the provision of care for refugees and asylum seekers.

Accessibility
Patients were able to access services provided by the MH RHW clinicians over the telephone, were satisfied with the quality of the telephone connection, and appreciated the ease of attending the appointment and the reduced associated costs. The language barrier that was flagged in previous research as one of the obstacles for equitable access to telephone consultations in primary care 23 was addressed by MH RHW through routine interpreter use; however, a range of interpreter related issues were highlighted by clinicians as negatively impacting on the clinical experience, including delayed interpreter connections, phone disconnections, poor sound quality and compromised ability to judge the quality of interpreting. Interestingly, the patient survey demonstrated no such concerns which is in line with the results of a systematic review that found no difference in patient satisfaction between in-person interpreting, telephone interpreting or interpretation provided by the treating bilingual physician. 24 This suggests the challenges reported by clinicians likely reflects operational limitations rather than confirming broader access issues from a patient perspective.
Although patients, who received care over the telephone, were highly satisfied with the way they accessed the service, it should be remembered that telephone consultations can infringe on equality of access for some patients. Accessibility of telephone consultations was not considered universal by clinicians and less than optimal, for example, for patients living in a situation of family violence or patients living with a disability such as hearing impairment. Barriers including restricted access to personal telephone and frequently changing contact numbers was another challenge, particularly relevant to new humanitarian migrants who frequently experience social and financial instability.
The service data demonstrated that even during peak restrictions, 20% of the consultations in the clinic were conducted face-to-face, thus confirming that patients who experienced difficulties or were not suited to telephone consultations, were able to access care. Once the restrictions were eased, half of all consultations returned to the face-to-face service delivery. This trend echoes the opinion expressed by clinicians that face-to-face consultation was their preferred mode of service delivery within a refugee context.
Appropriateness
Patients expressed a high level of satisfaction with the quality of care provided over the telephone and the relevancy of this care in addressing their clinical needs. This is consistent with the results of 2 systematic reviews on telephone consultations in primary care that also reported high levels of patient satisfaction.11,14 When comparing the overall quality of the telephone consultation to a face-to-face consultation, interestingly, the favourable results provided by patients were similar to that of a study on telephone and online consultations among older Australians, 25 but were higher compared to that found in general population in Australia. 26
However, similar to the data on service accessibility, patient data on appropriateness should be looked at in conjunction with the data provided by consulting clinicians who voiced concerns about the appropriateness of telephone consultations for some patients. For clinicians, cultural and individual dynamics were critical considerations when determining the appropriateness of telephone consultations. Establishing personal connection to optimise the therapeutic relationship was considered paramount when consulting the new patients and patients with increased social complexity. This was considered best nurtured in a face-to-face environment. Similar to the results of a qualitative study that investigated the impact of the COVID-19 pandemic on the core functions of primary care, 13 previously established doctor–patient relationship was seen as beneficial in ensuring high-quality patient-centred care when provided over the telephone.
Several patient groups, including children and patients requiring physical examinations, were identified by the clinicians as those for whom telephone consultations may also be less appropriate. For some patients, for example those requiring mental health services, telephone consultations were considered as not only inappropriate but potentially risk generating. This needs to be considered in the context of improved engagement with mental health services for other patients.
Acceptability
Telephone consultations were seen as an acceptable mode-of-care during the pandemic, and both the patients and clinicians expressed willingness to continue to engage with it in the future. The clinicians reported being able to deliver high standards of care for most patients, however, changes in routine clinical practice were required to mitigate clinical risks.
Despite the seemingly quick adaptation of the MH RHW clinicians to the provision of care over the telephone, personal and psychological implications were reported. Specifically, the clinicians reported experiencing increased anxiety around a possibility of missing a diagnosis, making incomplete risk assessments for psychiatric and vulnerable patients, and ensuring rigour in patient identification process.
Changes in the distribution of workload and roles between doctors and nurses infringed on the acceptability of telephone consultations among the nurses who reported increased burden in the workload related to patient follow-up. Challenges to the acceptability of telephone consultations in primary care that were linked to the disparity in workload between clinicians were reported in a several studies included in a literature review. 27 These studies, however, focused on the division of workload between doctors ‘on duty’ for taking telephone calls and others who had to cope with the demand for face-to-face appointments, or distribution of calls between doctors based on their demographics (eg, gender). In the case of MH RHW, the prominent role of nurses in managing patients contributed to the ease with which additional clinical tasks, relating to the change in provision of patient care, found their way to the domain of nursing. Should telephone consultations be incorporated into the regular care provision post COVID-19, focus on effective division of workload between doctors and nurses is required to improve acceptability of telephone mode-of-care among nursing staff.
Efficiency
Results from both the clinician survey and the focus groups indicated that the provision of care by telephone was considered, in the main, no more efficient than face-to-face service provision. This was reflected in the time required for each consultation and the number of consultations that a clinician can deliver per day. Efficiency gains were, however, reported regarding routine consultations for minor issues, such as follow-up check-ups and scripts. Unsurprisingly, similar to other studies, 28 lack of physical examination was considered unfavourable to efficiency.
Factors that were noted by the clinicians as infringing on the efficiency of the telephone consultations included added interpreter waiting time, additional administrative work, and increased workload on the nursing staff. Thus, introduction of telephone consultations as an additional mode-of-care post COVID-19 may require administrative considerations including additional time or staff to ensure efficiency and decrease the workload on nurses.
Strengths and Limitations
The small sample size for the clinicians who provided telephone consultations at the MH RHW clinic did not allow detailed investigation into factors associated with their experience of providing care over the telephone. The participation rate was 50% and the reason for non-participation was not recorded. Triangulation of the clinician survey results with the focus group data mitigated this weakness and allowed deeper inquiry into the clinicians’ perspective on challenges of providing care over the telephone to patients from refugee and asylum seeker background. Data from the patient survey permitted cross-validation and facilitated exploration into the patients’ perspectives. Refugees and asylum seekers are usually a hard-to-reach population, however, our recruitment method that involved bi-cultural workers, experienced in communication with this group of patients, resulted in recruitment of a representative sample among MH RHW patients, with 93% participation rate.
Conclusion
The COVID-19 pandemic has challenged health services to think about new creative and flexible models of providing care. Considering social, demographic and clinical characteristics of the patients, MH RHW opted to provide health care by telephone with an option for some patients to attend the clinic for face-to-face appointments when required, in acknowledging barriers associated with telehealth for this particular cohort. Our results showed that the telephone mode-of-care was a reasonable alternative from both a clinician and patient perspective when face-to-face consultations or telehealth may not be an option. However, should adoption of this initiative as an optional mode-of-care within the refugee and asylum seeker context be considered, identified barriers need to be addressed. Whilst patients who accessed telephone consultations were highly satisfied with the ease of access and quality of care they received, telephone consultations should be used with caution because of limited accessibility and appropriateness for some patients of refugee background. Furthermore, differences in opinion between doctors and nurses as to the acceptability and perceived efficiency of telephone consultations, together with any necessary changes to routine clinical practice to mitigate risk and promote best practice, should be considered to ensure optimal transferability in the longer term.
Thus, telephone-based service delivery should be viewed as a useful means of providing certain types of care to some patients of refugee background, rather than as universally applicable and affording significant service efficiencies. Whilst workforce considerations may be required to successfully integrate this mode-of-care into the healthcare post-COVID19, telephone consultations should be considered as one of a suit of service delivery models available to clinicians in providing care. This is particularly relevant to patients of refugee background where known barriers in accessing other forms of remote service delivery compromise health equity and optimal health and wellbeing outcomes. Continued support by government is critical to ongoing sustainability of telephone-based consultations, with the availability of Medicare billing items for all forms of remote service delivery likely to impact long-term clinical feasibility.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MK and JM conceived and planned the study. RA and CY reviewed data collection tools for readability and cultural appropriateness. MK, RA and CY carried out data collection. MK, JM and AD contributed to the interpretation of the results. MK took the lead in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis and manuscript. All authors read and approved the final manuscript.