
Abstract
Objective:
Many patients with osteoarthritis experience pain which can lead to higher healthcare expenditures. It is important to understand the factors that drive the excess expenditures associated with pain in osteoarthritis.
Design:
Cross-sectional.
Study sample:
Our study sample consisted of adults (age ⩾ 18 years) from the Medical Expenditure Panel Survey (MEPS, 2018).
Methods:
Adults who were alive during the calendar year and had pain status were included in this study (N = 2804 weighted N = 32.03 million). Osteoarthritis was identified from the medical conditions file and household file. We used multivariable ordinary least squares regression to identify the statistically significant association of pain with direct healthcare expenditures. The Blinder-Oaxaca post-linear decomposition on log-transformed total direct healthcare expenditures was used to estimate the extent to which differences in characteristics contribute to the excess expenditures associated with pain.
Results:
Adults with osteoarthritis and pain had higher average expenditures ($21 814 vs $10 827, P < .001; 9.318 vs 8.538 in logtransformed expenditures) compared to those without pain. Pooled regression weights explained 62.9% of excess expenditures differences in characteristics between the 2 groups. The 2 main drivers of excess healthcare expenditures among adults with osteoarthritis and pain were (i) comorbidities (diabetes, asthma, chronic obstructive pulmonary disease, depression, heart diseases, cancer, and non-cancer pain conditions and (ii) prescription medications (NSAIDs, opioids, and polypharmacy).
Conclusion:
Need factors such as comorbid conditions, and prescription treatment explained the excess healthcare expenditures among adults with osteoarthritis and pain. The study findings suggest that reducing polypharmacy and appropriate management of comorbid conditions may be a pathway to reduce excess expenditures among adults with osteoarthritis and pain.
Introduction
Chronic pain is one of the common symptoms of many chronic conditions and as high as 40% of adults in the United States (US) experience chronic pain.1,2 Studies have consistently linked chronic pain with disabilities, mental health problems, prescription drug dependencies, higher expenditures, and poor quality of life.3-6 Based on the latest data available, between 2008 and 2011, the estimated annual cost of pain in the US was $560 to $635 billion per year,7,8 indicating a significant use of healthcare resources for pain management. It has also been established that individuals with severe or moderate pain incur higher average healthcare expenditures than those without pain. 8 Among adults with chronic pain, 31.4% reported having arthritis. 9 A systematic review found that 15% to 75% of patients with knee pain had radiographic osteoarthritis. 10 According to the Centers for Disease Control and Prevention, approximately 32.5 million adults in the US have osteoarthritis. 11 Osteoarthritis a common form of arthritis, is a progressive degenerative disease, causes wear and tear of the cartilage, bone, and connective tissues, which can worsen over time. For example, most patients with unilateral knee osteoarthritis develop radiographic bilateral osteoarthritis over time. 12 The defining symptoms of osteoarthritis are stiffness, swelling, and chronic pain; a more frequent and intense pain signals a more severe radiographic osteoarthritis.13,14
Although pain is a hallmark symptom of osteoarthritis, pain interference and its sensation can vary widely among adults with osteoarthritis. 15 Not all adults with osteoarthritis experience chronic pain that interferes with daily activities because the site, symmetry, and the total number of afflicted joints can affect the intensity and chronicity of pain.12,16,17 For example, a cross-sectional study reported that only 47.6% of adults with osteoarthritis reported pain interference with normal activity. 18 However, pain experienced by adults with osteoarthritis can add to the disease burden including healthcare expenditures. It has been reported that healthcare expenditures were higher in adults with osteoarthritis and severe pain compared to those with moderate or no pain.19,20 The presence of comorbidities may affect pain severity and contribute to the disease burden including higher healthcare expenditures among adults with osteoarthritis.5,21 Thus, it is important to understand the factors that drive excess expenditures associated with pain among adults with osteoarthritis. Therefore, the objective of this study was to estimate the excess health care expenditures associated with pain among adults with osteoarthritis and examine the extent to which predisposing characteristics, enabling resources, need variables, personal health care practices, and external environment explain the excess expenditures associated with pain among adults with osteoarthritis. We hypothesized that adults with osteoarthritis and pain will have higher healthcare expenditures than adults with osteoarthritis and no pain and the main drivers of the excess expenditures will be the presence of comorbidities and polypharmacy.
Methods
We adopted a cross-sectional study design using data from the nationally representative survey of US households, the Medical Expenditure Panel Survey (MEPS) for the year 2018. The target population for the MEPS is all persons in non-institutionalized civilian households in the US. Institutionalized populations such as those in prisons, nursing homes, or in the military at any time during the year are excluded. MEPS adopts a complex survey design to select the households for the survey. 22 This complex design involves stratification, clustering, multiple stages of selection, and disproportionate sampling of households.22-24 MEPS uses the computer-assisted personal interview (CAPI) questionnaire for collecting data on health conditions, lifestyle factors, cost of healthcare utilization, prescription medications use, and other factors. Because the MEPS household component is a self-reported survey, the survey sponsoring agency, the Agency for Healthcare Research and Quality (AHRQ) validates it by using various quality assurance procedures. MEPS is considered one of the most comprehensive sources of cost data for health care utilization and health insurance coverage.24,25
In this study, we included adults 18 years or older who were alive during the calendar year, had osteoarthritis, and who did not have missing information on pain status, and had positive total healthcare expenditures. Osteoarthritis was identified from the household component and medical conditions files. Arthritis is considered one of the priority conditions in MEPS. Therefore, during the survey MEPS investigators ask all household members aged over 17 years whether they have ever been diagnosed with arthritis, and the type of arthritis they were diagnosed with. If the respondent reports the diagnosis of osteoarthritis, then the investigators record osteoarthritis diagnosis for the respondent in the medical conditions file. Osteoarthritis was identified using ICD-10-CM codes from the medical condition file. Although the site of osteoarthritis is an important consideration, MEPS did not have information on the sites of osteoarthritis or disease severity. We could not distinguish between generalized osteoarthritis and site-specific osteoarthritis.
Pain Interference with Normal Activity
MEPS collects information on pain and other health conditions by administrating a mail survey. 26 By using the MOS Short Form (SF)-12 participants were asked “During past 4 weeks, pain interfered with normal work outside the home and housework.” A 5-item Likert scale was used to record the responses. The options in the response scale include (1) “Not at all”; (2) “A little bit”; (3) “Moderately”; (4) “Quite a bit”; and (5) “Extremely.” In this study, we divided the responses into the presence of pain and no pain by combining the responses as follows: (1) No pain (not at all or a little bit) and (2) pain (moderately, quite a bit, and extremely). Combining pain by using one-item MOS SF-12 is a common practice among researchers.8,27
Total Healthcare Expenditures
MEPS provides data on total healthcare expenditures by using sources of payment and types of services information. Type of services includes inpatient, outpatient, emergency room, prescription drugs, dental care, vision care, durable medical equipment, and others. MEPS collects information on 14 sources of payment. 28 We transformed total expenditures into a natural logarithm scale to facilitate Oaxaca decomposition,29-31 which is explained in the analysis section.
Other Explanatory Variables
We used the Andersen’s healthcare utilization model as the conceptual framework to identify factors that contributed to the excess health care expenditures associated with pain in adults with osteoarthritis. 32 According to the Andersen’s model, predisposing factors, enabling factors, need factors, lifestyle factors, and external factors can influence an individual’s healthcare utilization. Predisposing factors included sex (female/male), age category (18-44, 45-54, 55-64, and 65 years and older), and race (Non-Hispanic White, African American, Hispanic, and other). Enabling factors included marital status (married, divorced/separated, widowed, single); education level (less than high school, high school, greater than high school); income as measured by the percentage of the federal poverty line (FPL) (poor (<100% FPL), near poor/low income (>100-<200% FPL), middle income (>200-<400% FPL), and high income (>400% FPL)); insurance coverage (public, private, uninsured); and prescription coverage (yes/ no).
Need factors included perceived physical and mental health, comorbidities, polypharmacy, and pain medications (Non-Steroidal Anti-inflammatory Drugs (NSAIDs) and Opioids). Comorbidities were selected based on published literature33-35 and included cancer, non-cancer pain conditions, and nervous system pain and pain syndromes. The non-cancer pain conditions consisted of arthritis (except osteoarthritis), low back pain, osteoporosis, musculoskeletal pain (not low back pain), headache- including migraine, fractures, sprains, other specified bone diseases, and musculoskeletal deformities. Nervous system pain and pain syndromes included asthma, chronic obstructive pulmonary disease, diabetes, depression, and heart conditions). Polypharmacy (yes/no) was defined as the use of 6 or more drugs in an individual, excluding NSAIDs and opioids. As lifestyle factors, current smoking status (smoker/non-smoker), exercise (yes/no); and body mass index (BMI, calculated as weight in kg/height in m2), categorized as underweight/normal (<25), overweight (25-29.9), and obese (⩾30) were included. Finally, external factors included the region of residence (Northeast, Midwest, South, and West).
Statistical Analyses
All analyses accounted for the complex sampling design of the MEPS and used survey procedures with cluster, strata, and appropriate weights—sample adult questionnaire weights. We determined statistically significant subgroup differences in categorical variables by pain interference using Rao-Scott chi-square tests (Table 1). We used t-tests to identify statistically significant unadjusted group differences in average total healthcare expenditures among adults with or without pain (Table 2) within subgroup categories and across pain status. We calculated the average mean difference in total healthcare expenditures by subtracting the average healthcare expenditures of adults without pain from the average healthcare expenditures of adults with pain. We used multivariable ordinary least squares regression to estimate the association of pain with total healthcare expenditures.
Description of sample characteristics by pain among adults (⩾ 18 years) with osteoarthritis, Medical Expenditure Panel Survey, 2018.

Abbreviations: BMI, body mass index; GE, greater than or equal; LT, less than; NSAIDs, non-steroidal anti-inflammatory drugs; Pain, pain interference in activity; Wt%, weighted.
Based on 2804 adults aged 18 years and older, alive during the calendar year and have osteoarthritis, MEPS 2018. Statistically significant subgroup differences in categorical variables by pain are based on Rao-Scott chi-square tests.
Means and standard errors (SE) of annual health care expenditures ($) by pain among adults with osteoarthritis, Medical Expenditure Panel Survey, 2018.
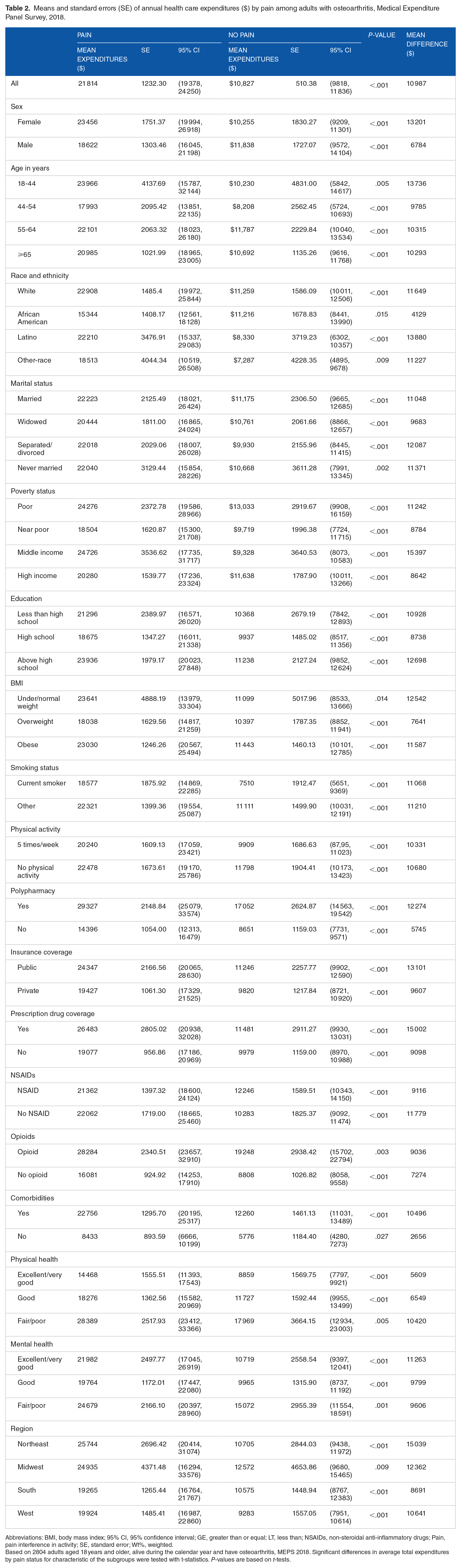
Abbreviations: BMI, body mass index; 95% CI, 95% confidence interval; GE, greater than or equal; LT, less than; NSAIDs, non-steroidal anti-inflammatory drugs; Pain, pain interference in activity; SE, standard error; Wt%, weighted.
Based on 2804 adults aged 18 years and older, alive during the calendar year and have osteoarthritis, MEPS 2018. Significant differences in average total expenditures by pain status for characteristic of the subgroups were tested with t-statistics. P-values are based on t-tests.
Decomposition technique
To estimate the extent to which differences in predisposing, enabling, need, lifestyle, and external characteristics of individuals among the adults with and without pain contribute to the excess expenditures of pain, we used the post-linear decomposition method proposed by Blinder Oaxaca.36,37 This approach divides the differences in average health care expenditures between pain and no pain into 2 parts: an explained and unexplained portion. 37 The difference in average expenditures due to the differences in observed characteristics between osteoarthritis with pain and osteoarthritis without pain groups is represented by the explained portion which is also known as the “characteristics effect.”37,38 The explained portion is calculated by computing differences in characteristics between the 2 groups (pain vs no pain) and weighting by regression coefficient estimates from the pooled regression. 39 The unexplained portion represented differences in average expenditures that emerge either because of differences in unobserved or unmeasured characteristics between osteoarthritis with pain and osteoarthritis without pain or differences in the regression coefficient estimated between the 2 groups. The unexplained portion is also known as the “coefficient effect.”38,39 The characteristics effect can be calculated either using regression coefficients from pooled regression (pooled regression weights) or coefficient from stratified regressions of pain (pain regression weights) and no pain (no pain regression weights). In linear decomposition analysis, we used pooled, pain group, and no pain group weights to calculate the explained portion. Consistent with published literature, the excess healthcare expenditures were defined as the additional healthcare expenditures that adults with osteoarthritis and pain incur compared to adults with osteoarthritis and no pain.40-42 We performed analyses using SAS survey procedures (SAS v 9.4 (SAS Institute, INC)) and Stata 15 (StataCorp LLC, College Station, TX) for decomposition analyses.
Results
The number of adults in our study represented an estimated 32.03 million adults with osteoarthritis in the US in 2018. A majority of the sample were female (64.8%), adults aged 65 years or older (57.6%), White (77.2%), and married (53.6%). The prevalence of pain interference in adults with osteoarthritis was 41.7%. The comparison of characteristics among the 2 groups of adults with osteoarthritis—with pain and without pain, revealed statistically significant differences in enabling factors, need factors, and lifestyle factors (Table 1). Adults with osteoarthritis and pain had higher rates of less than high school education (15.1% vs 7.2%), low income (17.2% vs 6.1%), poor physical health (42.8% vs 12.0%), and lower rates of physical activity (32.0% vs 51.6%), higher rates of polypharmacy (49.7% vs 25.9%), higher rates of NSAID (35.5% vs 27.7%), and opioid use (47.0% vs 19.3%) (Table 1).
Table 2 presents the average healthcare expenditures and standard errors (SE) among adults with pain and without pain using independent sample t-test. Among adults with osteoarthritis, those with pain had higher average total healthcare expenditures (Mean = $21,814, SE = 1232.3) compared to those without pain (Mean = $10,827, SE = 510.3). The difference was statistically significant (Mean difference = $10,987, t-value = 67.3, P < .001). This translated into a difference of $10 987 in the mean annual healthcare expenditures, indicating 101.5% higher mean total healthcare expenditures among adults with osteoarthritis and pain.
We tested the differences in average healthcare expenditures by pain status for each level of the subgroups with t-tests. For example, we tested the differences in mean healthcare expenditures by pain status among men and women separately. Statistically significant differences in average healthcare expenditures between pain and no pain groups were obtained for each of the sample characteristics among adults with osteoarthritis where the average healthcare expenditures were significantly higher for adults with pain. The mean difference in annual average healthcare expenditures ranged from as high as $13 880 (Latino) to as low as $4128 (African Americans).
Multivariable OLS regression among adults with osteoarthritis
The findings from multivariate OLS regression on log-transformed total healthcare expenditures among the adults with osteoarthritis are summarized in Table 3. The percentage change in expenditures associated with pain can be obtained by exponentiating the regression coefficient of the pain variable and subtracting one (eβ – 1). As it can be seen, adults with osteoarthritis and pain had a 33.6% (β = 0.290, SE = 0.06, P < .001) higher annual average healthcare expenditures compared to those with osteoarthritis and no pain.
Parameter estimates and standard errors of explanatory variables multivariable ordinary least squares regression of pooled model on log-transformed total healthcare expenditures, Medical Expenditures Panel Survey, 2018.

Abbreviations: BMI, body mass index; 95% CI, 95% confidence interval; NSAIDs: non-steroidal anti-inflammatory drugs; Ref = reference group. SE = standard error; Wt%: weighted percentage.
Based on 2804 adults aged 18 years and older, alive during the calendar year and have osteoarthritis, MEPS 2018.
Blinder-Oaxaca linear decomposition
The post-regression Blinder-Oaxaca linear decomposition analysis results are summarized in Table 4. The average predicted log-transformed total healthcare expenditures for the pain group was 9.318 units (SE = 0.04, 95% CI = (9.23, 9.40), P < .001); and the corresponding log-transformed total healthcare expenditures for the no pain group was 8.538 units (SE = 0.04, 95% CI = (8.46, 8.61), P < .001). The difference between the 2 groups was 0.78 units (SE = 0.06, 95% CI = (0.66, 0.89), P < .001) in average log-transformed health care expenditures. We decomposed the average differences using “pooled,” “pain,” and “no pain” regression weights.
Decomposition of log-transformed total healthcare differences by pain status among adults with osteoarthritis Medical Expenditure Panel Survey (MEPS), 2018.

Abbreviations: BMI, body mass index; 95% CI, 95% confidence interval; NSAIDs, non-steroidal anti-inflammatory drugs; Pain, pain interference in activity.
% = percent contribution in the explained portion.
Based on 2804 adults aged 18 years and older, alive during the calendar year and have osteoarthritis, 2018. The percent differences of domains of Andersen’s health care behavior model are illustrated in the model.
Based on pooled regression weights, we found that differences in predisposing, enabling, need, personal healthcare practices, and external factors explained 62.8% of the difference in average log-transformed total healthcare expenditures. Thus, if adults with osteoarthritis and pain were to have characteristics similar to those without pain, the difference in log-transformed dollars would reduce to 0.32 units.
Among the explanatory factors, polypharmacy and comorbidities were the major drivers of excess healthcare expenditures associated with pain among adults with osteoarthritis across all weights. As seen in Table 1, polypharmacy rates were significantly higher in adults with pain compared to those without pain (49.7% vs 25.9%). For example, polypharmacy, opioid, and NSAIDs use explained 66.8% (pooled weights), of the excess total healthcare expenditures between the 2 groups. Thus, if osteoarthritis adults with pain were to have polypharmacy, NSAID use, and opioid use rates similar to those of those without pain, the difference in average total expenditures would reduce to 0.45 log units. If comorbidity, polypharmacy, NSAID use, and opioid use prevalence rates were similar between the 2 groups (pain and no pain) of adults with osteoarthritis, the differences in average expenditures would be reduced to 0.169 log units. Similar reductions will be achieved using “pain” and “no pain” weights.
Of the 0.78-unit difference, −0.091 units (−18.6%) were explained by the differences in enabling factors. Finally, lifestyle and external factors had a lower contribution to the log-transformed healthcare expenditures of 3.99% (−0.020 units) and 2.95% (−0.014 units), respectively.
The explained portion rose from 64.0% when no pain regression weights were used to 71.9% when pain regression weights were used.
Discussion
Previously, studies have reported significantly higher healthcare expenditures in adults with osteoarthritis compared to those without osteoarthritis43,44 and higher expenditures due to pain.19,20 In this study, we restricted our analysis to adults with osteoarthritis and examined excess healthcare expenditures associated with pain interference. We found that adults with osteoarthritis and pain had 2.01 times higher annual healthcare expenditures compared to those without pain. After controlling for predisposing, enabling, need, lifestyle, and external factors, we found that the average healthcare expenditures were 101.47% higher in adults with osteoarthritis and pain compared to adults with only osteoarthritis. These findings suggest a higher disease burden in adults with osteoarthritis and pain. The higher healthcare expenditures in adults with osteoarthritis and pain may be due to chronic pain that may lead to increased utilization of health care resources such as frequent use of outpatient services, pharmacy, and increased emergency department visits.45,46
This study expanded the previous literature, by determining which of the differences in characteristics contributed to the excess expenditures associated with pain among adults with osteoarthritis using decomposition analysis. In decomposition analysis, we found that nearly two-thirds of the difference in direct healthcare expenditures was explained by differences in predisposing, enabling, need lifestyle, and environmental factors between those with and without pain.
Among the explanatory factors, polypharmacy and pain medications were the primary drivers of the excess expenditures associated with pain. This finding emphasizes the need for medication therapy management (MTM) services, which focus on medication therapy review as well as medication safety review (MSR). Although not specific to osteoarthritis, studies reported positive effects of MTM services on medication adherence, appropriateness, dose reduction, and hospitalization.47,48 For example, a study that explored the difference in outcomes between patients with pharmacist delivered MSR to patients without such reviews reported that patients with MSR experienced lower medical costs, hospitalization, emergency department visits, and mortality. 49 Another study conducted on chronic polypharmacy patients reported a significant reduction in medical costs due to MTM. 50 A randomized controlled trial on multiple chronic conditions also reported significant cost savings and improvement in humanistic measures in MTM elderly group compared to the usual care group. 51 Applying screening tools that facilitate “STOPP & START” criteria for stopping inappropriate medications and starting appropriate medications may also reduce the risk of polypharmacy 52 and healthcare costs due to adverse effects. 53 Specifically, STOPP and START criteria can be used to reduce inappropriate prescribing in older adults with multimorbidity. 54
Our findings suggest that excess healthcare expenditures associated with pain among adults with osteoarthritis may be reduced with non-pharmacologic treatments. The Osteoarthritis Research Society International (OARSI) guidelines emphasize arthritis education and structured land-based exercise programs as the primary non-surgical treatment for knee, hip, and polyarticular osteoarthritis. 55 OARSI recommends mind-body exercises, dietary weight management, and cognitive behavioral therapy with an exercise component for patients with comorbidities as non-pharmacological treatment options in addition to strengthening exercises. 55
Comorbid conditions and their sequelae on physical and mental health were also major drivers of the excess expenditures of pain in adults with osteoarthritis. In our study, adults with pain had higher rates of comorbidities (93.4% vs 77.9%) as compared to those without pain. Thus, a subgroup of osteoarthritis patients is highly multimorbid and healthcare management can be quite challenging for this subgroup. This emphasizes the greater need for team-based coordinated care. Many studies have reported the positive effects of team-based care coordination provided in medical homes on health outcomes including a reduction of inpatient and outpatient visits.56-58 Medical homes avoid treatment duplication through care coordination and may play an increasingly important role in providing effective care to multimorbid patients. For example, a study on medical home patients reported lower inpatient, outpatient, and emergency room expenditures in the follow-up year compared to usual care. 59 However, studies have also reported a paucity of coordination programs and complexity in care delivery which may result in pain, mental health issues, and medication error.60-62 These findings suggest that care coordination offered through medical homes or accountable care organizations 63 may be a pathway to reduce costs among adults with osteoarthritis and pain.
We also observed that enabling factors, some of which can be considered as Social Determinants of Health (SDoH), were protective against higher costs in the pain group. Adults who had osteoarthritis without pain had higher rates of education above high school (67.5% vs 54.5%) compared to those with pain. Similar findings were observed for income, and prescription drug coverage, highlighting the role of SDoH in cost-containment efforts. Previous studies have suggested that some SDoH such as lower-income, and lower educational levels are associated with higher comorbidities, hospitalization, death, and increased healthcare expenditures.64,65 On the other hand, improvement in SDoH has the potential to reduce costs. When participants’ social needs were met, mean healthcare expenditures were reduced by 10%. 66 However, we cannot rule out the moral hazards associated with access to healthcare which can increase the costs. A recent study conducted on private insurance plans reported 53% additional medical spending between the most and least generous healthcare plans suggesting the existence of moral hazard due to healthcare insurance. 67
It is important to note that nearly one-third of the differences in log-transformed expenditures between osteoarthritis adults without pain and osteoarthritis with pain remained unexplained. The unexplained portions can be contributed by unmeasured factors such as medication adherence, treatment differences, and severity of the diseases.68,69 Therefore, future research needs to evaluate the contributions of such factors in assessing excess health care expenditures among adults with osteoarthritis and pain.
Strengths and Limitations
This study has several strengths. We used a nationally representative, large dataset of U.S. non-institutional civilians and developed a population-based study. Furthermore, we controlled for potential confounding factors by including a comprehensive list of covariates that can be associated with osteoarthritis, pain, and related expenditures. However, this study also has some limitations. A causal relationship between osteoarthritis with or without pain and expenditures cannot be determined due to the cross-sectional nature of the study. Given the self-reported nature of the survey and data collection, the study is subjected to recall bias and other forms of information bias. Moreover, the survey did not capture the severity of osteoarthritis or other chronic conditions. Some of the excess expenditures may be explained by the severity, type of osteoarthritis, and treatment procedures for osteoarthritis pain (eg, knee surgery), which were not included in this study. This study focused on direct healthcare expenditures from a comprehensive list of sources, however, we did not include indirect costs due to disability, mobility limitations, and job problems. The pain question asked participants about the last 4 weeks, therefore, the likelihood of under or over-reporting cannot be discounted. The pain question was not osteoarthritis-specific. Although we included several covariates, the influence of unmeasured confounders such as the severity of osteoarthritis, the number of osteoarthritis sites affected, and the severity of comorbid conditions cannot be ruled out. Polypharmacy was one of the major drivers of the excess expenditures associated with pain, we cannot rule out its endogenous relationship with expenditures. We used the Blinder-Oaxaca decomposition method which does not provide insights on the root causes of the differences between the 2 groups. In addition, the method may yield different estimates based on the regression weights used.37,70 We used log-transformed expenditures which cannot be easily converted to original dollar values. 71
Conclusion
Compared to the adults who had osteoarthritis without pain, adults with osteoarthritis and pain had higher average annual costs. The major drivers of the costs in adults with osteoarthritis and pain were polypharmacy, NSAIDs, opioid use, and comorbidities. Future research should emphasize primary, secondary, and tertiary prevention of comorbidities, use of alternative treatments including non-pharmacological treatment for pain among adults with osteoarthritis.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by the National Institutes of Health (NIH) Agreement No. 1OT2OD032581-01 (Usha Sambamoorthi), and the National Institute on Minority Health and Health Disparities through the Texas Center for Health Disparities (NIMHD), 5U54MD006882-10 (Usha Sambamoorthi). The views and conclusions contained in this document are those of the authors and should not be interpreted as representing the official policies, either expressed or implied, of the NIH.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors substantially contributed to the following- conception and design of the study, methodology, analysis, interpretation of data, initial draft, and revisions. The submitted version of this study was approved by all authors.