
Abstract
The Department of Veterans Affairs (VA) Intensive Dysphagia Treatment program serves a critical role in facilitating improvements to quality of care, standardization of outcomes, and increased access to structured therapy for Veterans with dysphagia. It has been implemented at 26 sites nationally and continues expanding. An explanatory sequential mixed-methods design was utilized for program evaluation to identify barriers and facilitators to implementation as reported by speech-language pathologists (SLPs) participating in the program. All 23 IDT program SLPs were invited to participate in an online survey. SLPs were asked to describe etiologies referred for SLP evaluation, most and least clinically useful program aspects, and characteristics of patients recommended for therapy. Qualitative interviews/focus groups were then conducted with 9 SLPs at 3 facilities with varying levels of program experience. Transcripts underwent systems engineering framework informed deductive thematic analysis. Interview/focus groups revealed overall positive feedback. Barriers included data entry challenges and provider understanding of long-term program goals, while facilitators included program structure enabling increased patient follow-up, outcomes tracking, and training in new treatment modalities. Through this evaluation process, program leadership garnered actionable feedback to improve further implementation of the IDT program. Ongoing efforts will further improve data entry, site onboarding procedures, and program communication.
Background
Oropharyngeal dysphagia or swallowing dysfunction, is a serious condition that has been estimated to occur in 1 out of 25 adults each year in the United States. 1 Oropharyngeal dysphagia is characterized by impairments affecting oral preparation of food and liquid and/or initiation and transport of food/liquid boluses through the pharynx and into the upper esophagus. Esophageal dysphagia refers to difficulty with efficient passage of the bolus through the esophagus and into the stomach. The focus of this study was oropharyngeal dysphagia, referred to herein as “dysphagia”.
Dysphagia typically develops as a symptom of various diseases (eg, cerebrovascular diseases) or from the sequelae of therapeutic interventions (eg, treatment for head and neck cancers including chemoradiation and/or surgery), but is also observed as a manifestation of aging and frailty. Inpatients with dysphagia are at increased risk of mortality, longer length of hospital stay, and increased cost associated with their hospitalization than those without dysphagia. 2 Major complications of dysphagia include malnutrition,3,4 dehydration, aspiration pneumonia, 5 and decreased quality of life.6-10
Veterans experience medical conditions known to result in dysphagia (eg, head and neck cancer, progressive neurologic disease, stroke, respiratory disease) at higher rates and have more complex health needs compared to non-Veterans. The Department of Veterans Affairs (VA) services differ from most other health services due to its integrated network of hospitals and clinics, as well as the number of clinicians employed and the duration for which many Veterans are followed for healthcare through the VA. The number of dysphagia-related procedures conducted by speech-language pathologists (SLPs) in the VA suggests a large number of Veterans experiencing swallowing disorders. In 2019 alone, SLPs working in the VA completed nearly 108,000 evaluation procedures for oropharyngeal dysphagia and nearly 85 000 dysphagia treatment procedures.
Despite this, surveys assessing practice patterns for SLPs managing dysphagia show variability in utilization of evidence-based techniques, 11 follow-up of treated patients, 12 and employment of validated outcomes tools for measuring post-treatment change in swallow function or quality of life.13,14 To establish a comprehensive and consistent standard of care for Veterans with dysphagia, the Intensive Dysphagia Treatment (IDT) quality improvement program was established in 2013 at William S. Middleton Memorial Veterans Hospital in Madison, Wisconsin. The IDT program is a patient-centered multidisciplinary approach to the treatment of oropharyngeal dysphagia. The program’s main goals are to improve quality of dysphagia care for Veterans to optimize health, foster standardization of assessment and treatment through use of evidence-based protocols and validated outcome tools, increase access to therapy, and support SLPs implementing the program by offering forums for collaborative learning and tools to advance their skills. Intervention approaches included in the IDT program are intensive and progressive in nature based on exercise physiology literature showing that these components are critical to inducing lasting change in muscle function. 15
Several key features address the program’s goals. To improve the quality of care, an interdisciplinary team comprised of SLPs, dietitians, primary care providers, respiratory therapists, and/or nurses coordinate care to ensure early identification of adverse health outcomes of dysphagia and prompt initiation of treatment. To promote standardization, program leadership developed an assessment and outcomes toolkit; created a clinical framework to provide SLPs with care pathways based on the patient’s swallowing impairments; and incorporated evidence-based progressive, intensive rehabilitative intervention modalities. 15 To increase access to therapy, the program capitalizes on existing VA telehealth infrastructure to provide greater choice to Veterans who opt to receive care in the home or the community rather than an institution. Finally, to support program implementation, monthly meetings allow for discussion among facility points of contact and program leadership. All sites also receive an IDT program manual to support training in use of the devices and protocols.
Two device-facilitated dysphagia protocols were included in the IDT program: lingual strengthening (LS) 16 and expiratory muscle strength training (EMST). 17 Details regarding the protocols are featured in Table 1. These therapies were chosen based on dose parameters that are well-described in the dysphagia literature for replicability in a clinical setting 15 with regular follow-up visit intervals to allow for skilled adjustment of treatment targets and monitoring of patients’ progress toward their therapeutic goals. Typical timelines are provided in Figure 1. In addition, these therapies each utilize a device to provide biofeedback for enhanced learning, 18 allow for in-home re-calibration by the patient or caregiver (with the guidance of an SLP), and reduce travel burden typically associated with return clinic visits. Current LS tools (eg, Iowa Oral Performance Instrument®) include technology capable of obtaining objective lingual pressure measures, recording daily adherence, and providing visual biofeedback on exercise success. EMST tools used as part of the program are analog, pressure threshold devices 19 (eg, EMST150™) and provide auditory biofeedback when sufficient expiratory pressure load is produced to “open” a spring-loaded valve. Devices are reviewed by each facility’s equipment purchasing (ie, Supply Chain Management or Prosthetics services), sterile processing, and infection control teams to ensure local compliance is met in acquisition of devices, any required patient safety processes, and environmental safety procedures.
Device-facilitated dysphagia interventions.


IDT Visit Timeline (Lingual Strengthening and Expiratory Muscle Strength Training).
To reflect on improvements to quality and access, a VA Research Electronic Data Capture (REDCap) 20 database was constructed to allow for collection of outcomes, observe trends in patients enrollment, and review provider adherence to treatment schedules. All SLPs participating in the program receive training and education specific to use of VA REDCap data to ensure understanding of correct procedures. VA REDCap forms are designed and organized to replicate the typical flow of clinical practice to reduce cognitive load during treatment sessions and minimize time spent on data entry. SLPs are encouraged to input their session data as soon as possible following visit completion. Data collected at each treatment session include whether a visit was successfully completed, the modality in which the visit was conducted (eg, in-person, telephone, telehealth to home, or telehealth to a VA clinic), and clinical measurements taken to measure progress and device settings. Provider adherence to prescribed treatment schedules is measured as the number of sessions per patient that an SLP either conducted or attempted to conduct a treatment visit out of the total number of possible SLP-guided visits per therapy protocol (see Table 1).
As the program grows, evaluations of key stakeholder experiences are critical in identifying factors that impact patient participation and provider implementation of IDT. Although provider adherence to prescribed treatment schedules is excellent (84.5%), some sites have enrolled substantially fewer patients than others despite identical onboarding procedures. This highlights the need to examine provider perspectives on barriers and facilitators to participation in IDT to enhance ongoing implementation at additional sites and inform future dissemination efforts. This manuscript describes a systems engineering guided program evaluation process through which we explored barriers and facilitators to IDT program implementation by obtaining perspectives from key stakeholders on the front lines of clinical care for patients with dysphagia.
Methods
An explanatory sequential mixed-methods design 21 included an initial online survey followed by a series of interviews/focus groups to explore perspectives of IDT providers with varying levels of clinical experience. The survey and qualitative sessions were deemed a quality improvement program evaluation by the University of Wisconsin-Madison Institutional Review Board and the Madison VA Research Office.
Provider Survey
A combination of open- and close-ended questions were developed by 3 team members (NRP, RM, and BS) which focused on determining the utility of existing tools to facilitate the program and what changes could be made to improve incorporation of the program into day-to-day clinical practice. In addition, we sought to identify factors integral to selection of specific dysphagia treatment regimens across providers. All SLPs participating in the IDT program were invited to respond to the survey, which was administered via VA REDCap.20,22 The survey was comprised of 13 questions; these are presented in Tables 2 to 4. The time to complete the survey was approximately 10 minutes. Results were calculated as a percentage of SLPs reporting each response from the survey. In cases where SLPs provided multiple responses, the frequency of a given response was reported.
Participant characteristics.

Provider Focus Groups
Following survey administration, providers participating in the program across 3 VA facilities were invited to participate in structured interviews or focus groups. These were conducted virtually via video teleconferencing and led by a trained facilitator with expertise in conducting interviews and focus groups (MJK). The facilitator had no previous exposure to the IDT program and no prior relationship with any of the participants. Sites were purposefully selected to represent a range of IDT participation times and SLP clinical experience. Questions were open-ended and designed to elicit reflections from providers regarding perceived factors influencing patient enrollment in and adherence to structured therapy programs as well as barriers and facilitators to IDT program delivery. The goal of these focus groups was to identify any modifications or improvements that would support establishing this program as standard of care. Multiple team members reviewed the interview guide, which was refined based on their feedback. Questions were piloted via test sessions prior to administration during the qualitative sessions.
The focus groups were video-recorded and transcribed verbatim by 1 research team member (SD). Another team member (JY) inductively coded the transcripts in NVivo 12 software for identification of themes related to barriers and facilitators to implementation using the Systems Engineering Initiative for Patient Safety (SEIPS) model,23-25 a framework for characterizing work system components (Person, Organization, Environment, Tasks, Tools, and Technology), care processes, and outcomes in healthcare, and their interdependent relationships.
Results
Provider Survey
23 SLP providers from 8 facilities were invited to participate in the survey; 12 providers responded (52.1% response rate). Participant demographic data can be found in Table 2 and participant responses can be found in Tables 3 and 4.
Participant responses on patient population factors.

Abbreviation: VFSS, Videofluoroscopic swallow study.
Participant responses specific to outcomes and tools.

SLPs reported varying levels of experience in the program with 50% indicating more than 3 years of program participation. The top 3 medical etiologies with the greatest responses were head and neck cancer (n = 12), progressive neurologic disease (n = 9), and stroke (n = 8). SLPs identified that the opportunity to provide biofeedback during patient sessions (n = 12) and frequency of exercises (n = 11) as the most clinically useful aspects of IDT related to enacting positive changes in swallowing function. Lower rated program aspects included validated tool for interpretation of VFSS (n = 6), standardization of outcomes (n = 4), and variety of treatment device options (n = 4).
SLPs highlighted the top 3 patient factors critical to decision making in therapy approaches, focusing on cognitive status (n = 12), swallowing impairment (n = 11), and familiarity with technology (n = 7). Most SLPs indicated minimal impact of the IDT program on their daily clinic workflow (n = 10). Of the SLPs using telehealth (n = 6), all reported that telehealth improves adherence to the program. Tools for screening the patient’s ability to complete activities of daily living (n = 5) and cognition (n = 4) were highlighted as items that should be removed. When asked what additional outcomes should be used as part of the program, responses provided by SLPs included an additional follow-up 1 year post-treatment or that no other outcomes should be added. 58.3% of SLPs (n = 7) agreed that the VA REDCap database was easy to use. Finally, SLPs indicated that a standard operating manual would be the most helpful in implementing the IDT program at their site (n = 7).
Provider Interviews/Focus Groups
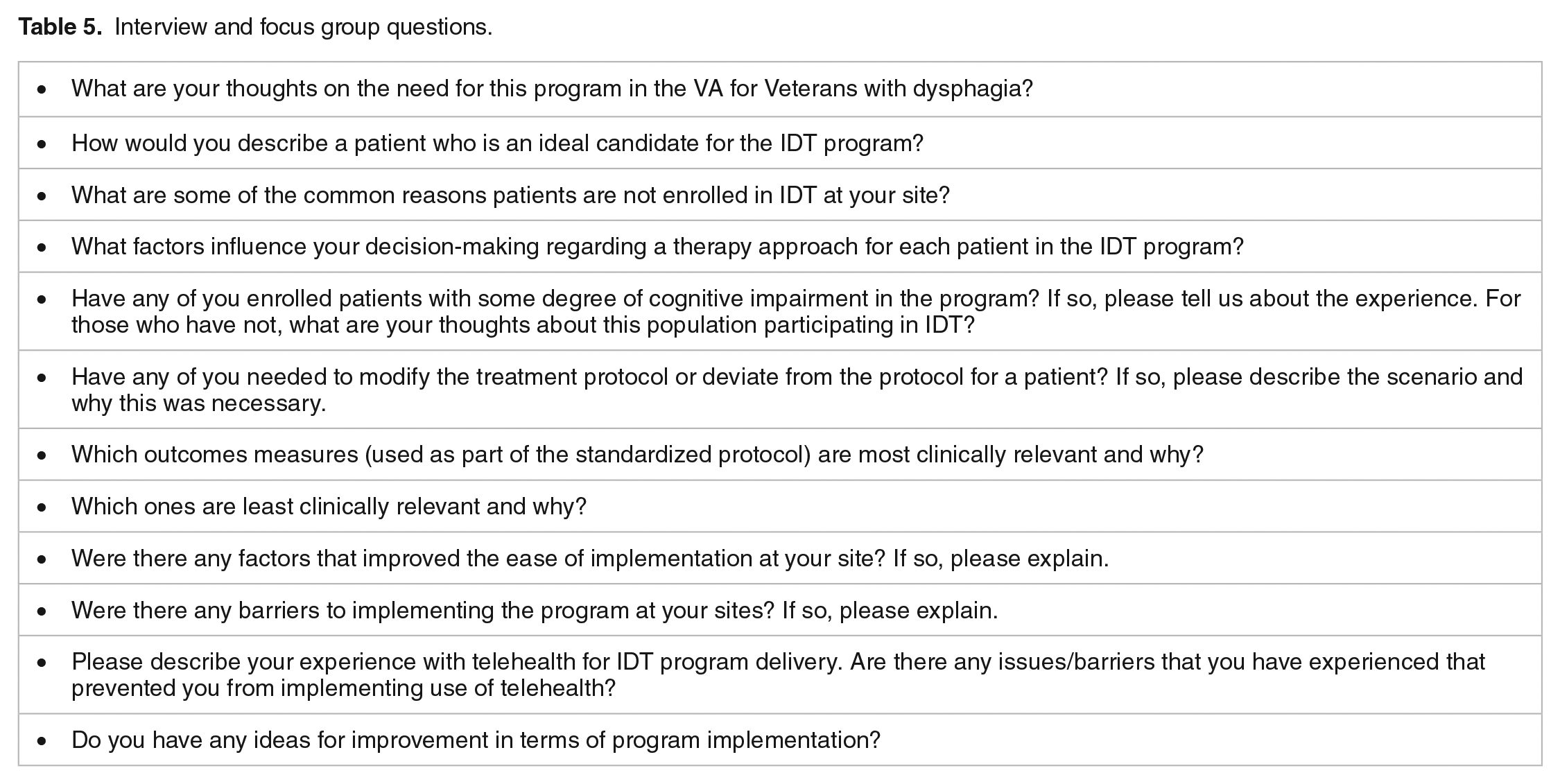
Nine SLPs were invited to participate in either a structured interview or focus groups at 3 separate VA facilities. Each of the 2 focus groups had 4 participants and 1 individual completed a structured interview. Questions are listed in Table 5. Themes identified through these interview/focus groups were mapped to specific components in the SEIPS model (Table 6).
Interview and focus group questions.
Key component and elements of the SEIPS model.

Person
SLPs generally had positive remarks regarding the need for and benefit of the IDT program and its focus on structured interventions and outcomes:
“There’s certainly a need for swallowing intervention programs that are carefully monitored in terms of follow-up and patient participation and compliance. Where pre- and post-treatment data is collected so that some level of evidence as to whether or not the rehabilitation program that was selected was effective for the Veteran.”
“The program has shown that it is has excellent outcomes, particularly for pneumonia and financial outcomes, so from a hospital business systems thinking standpoint, not only are we able to provide dysphagia therapy, where there’s good quality of life and personal outcomes for the Veteran, but then from a hospital-wide sense, there’s been some good outcomes.”
SLPs described factors that improve a patient’s candidacy for dysphagia rehabilitation through IDT. These included (1) interest in participating in intensive therapy; (2) intact cognition to follow instructions and therapy protocols; (3) strong caregiver and/or family support; (4) patient motivation to improve swallow function; (5) comprehension of their etiology or diagnosis associated with swallowing disorder and insight into their swallowing impairment(s); (6) agreement to return to clinic for follow-up visits; and (7) technological capability to navigate therapy devices. One SLP noted specific characteristics that may influence a patient’s desire to participate in therapy:
“Patient motivation. It also goes along with, is it a temporary dysphagia that will resolve in an acute setting? Or is it more chronic and they’ve acknowledged that they’ve lost some ability and want to work to get it back?”
All SLPs reported other contextual factors that served as facilitators to patient participation. These related to setting (ie, inpatients were easier to keep on consistent schedules) and caregiver support (ie, set up of therapy materials and facilitation by a family member).
“We have had a few Veterans with a very supportive family member who has helped them to implement the program at home and that has worked fine.”
Several SLPs indicated that patients’ comorbid conditions and changes in medical status were barriers that resulted in dysphagia not being adequately addressed:
“We have people who enroll and then subsequently get admitted to the hospital and they have other issues they have to deal with. Or sometimes they feel like they are already working so hard at physical therapy right now. They just don’t feel like they can add another thing to their plate.”
Organization
All participants confirmed the need for swallowing intervention programs using a standardized outcomes toolkit and reported that the IDT program was helpful in addressing this gap.
“I think there’s certainly a need for swallowing intervention programs that are carefully monitored in terms of follow-up and patient participation and compliance.”
“I appreciate the effort to standardize a little bit more. I like putting everyone on the same page and looking at outcomes. I like those efforts.”
They specifically highlighted the value of once-monthly all-site calls in communicating with IDT program leadership and felt that their input was valued.
“The monthly conference calls have been helpful as well to see what other sites are doing. I think collaboration between the VAs has been wonderful.”
Additionally, SLPs emphasized increased coordination with other disciplines for whom dysphagia is a concern (eg, dietitians) and reported receiving excellent staff support from IDT program leadership level as well as locally:
“It’s been helping us collaborate with other disciplines for their swallowing impairments, so it’s been a wonderful addition to our clinic.”
However, 1 SLP cited the challenge of trying to match schedules with other disciplines while completing other tasks necessary for patient care:
“One of my barriers would be to pull in the respiratory therapist or dietitian. Those are oftentimes areas where I don’t get to, whether it’s a video swallow study and then I’m trying to get all this other stuff done. Or they’re an inpatient and I’m trying to get my agenda done in an area. So that’s a barrier for me to try and pull them in.”
Other organizational challenges reported by SLPs included navigating the device ordering process with affiliated services and receiving the appropriate approvals from infection control services.
“For a long time we didn’t have any of the equipment we needed. We only ever got one [lingual strengthening device] and we didn’t have that for the majority of the first fiscal year that we implemented the project, along with the mouthpieces too.”
Environment
SLPs reported in-home therapy as beneficial for patients who were motivated and cognitively intact, or who had an involved caregiver. SLPs indicated that patient distance from clinic could be challenging for follow-up but that VA telehealth services were beneficial in facilitating this.
“I believe that Veterans are very interested in programs that involve not coming into the main hospital. The convenience aspect of these dysphagia treatment programs that can be administered via telephone or telehealth contact is very useful for the Veterans and really helps to improve participation in any kind of rehabilitation program.”
SLPs noted that cognitive deficits presented challenges for ensuring outpatient follow-up but this was less concerning for patients in the hospital setting:
“I think you can take on people with cognitive deficits if they’re an inpatient and you are going to be providing that support.”
Tasks
SLPs highlighted the high clinical relevance of repeat administration of instrumental examinations (ie, modified barium swallow study) and outcome measures assessing quality of life, functional status, and physiologic change.
“I certainly feel the repeat instrumental exam is highly clinically relevant. The bottom line is that we would like to see that using these exercise-based interventions is going to generate some kind of physical change in function. Like, that’s the whole point. So, we’re always looking carefully at that information. The subjective measures are really important too. Like their [swallowing-related quality of life] scores, their EAT-10 [Eating Assessment Tool] scores, and what they’re eating. Have we been able to change their diet? We want to see if they have made any progress.”
However, they noted the challenge of identifying appropriate patients who were interested and motivated to participate:
“We don’t try to convince patients very hard to enroll because if we are getting a sense that they are really not interested or dysphagia is not something they want to work on at this time. We’ve learned the hard way that in general enrolling them is not going to be beneficial to them or us in terms of the amount of time and effort it takes to collect the baseline data and set-up the program.”
They reported appreciation of streamlined clinic workflow, including fewer outcome measures:
“I feel the outcome measures have been pared down enough over the years that the ones we are still using are all relevant.”
SLPs reported difficulty in consistently finding time to enter data in the context of clinical care and that additional training of local site coordinators to review data quality would be beneficial.
“It does take some time to enter information into REDCap. The first time I sat down to do it with that baseline MBS and initial patient baseline visit it took me an hour to enter in data.”
They also expressed the desire for flexibility in outcomes reporting, noting that some instruments are not commonly used clinically with certain patient populations.
“A barrier is the time and amount of information we’re looking to gather. [We are] understanding that whatever we can get done is better than nothing, so that helps.”
They described difficulty interpreting certain outcome measures for patients with cognitive impairment or poor insight into deficits:
“As they get better and they get better awareness, their scores might go up. It doesn’t mean that swallowing got worse, it’s just that they’re just more aware of their issues. It’s not a very accurate measure of progress with someone that’s cognitively impaired.”
Tools and technology
SLPs identified the benefit of utilizing a multi-site VA REDCap database for outcomes reporting, noting that prior databases were more challenging to use and that VA REDCap required little to no training in data entry.
“The database has really been reworked and modified from the beginning of the program. There was another one that was used before we had the REDCap one. But that was kind of challenging to use. And all of that has really been thoroughly reworked since they redeveloped it. I think now it’s really good.”
With respect to therapy tools, SLPs indicated that they appreciated opportunities to learn about new devices for facilitating dysphagia therapy. They described familiarity with several treatment modalities utilized as part of the program, which they noted helps to encourage buy-in from patients:
“One other thing is that most of the things within the treatment program are already in our wheelhouse. So we’re already doing [expiratory muscle strength training], we’re already doing [lingual strengthening] for set patients. It’s not completely novel for our patients to buy into this thing. We’re familiar with it.”
They also highlighted the benefit of biofeedback to maintain patient engagement and provide concrete feedback on therapy success during home program sessions:
“. . . The immediate feedback and the recording of each time they completed the exercise, I think just knowing that they were being monitored promoted completion of the exercises. And when they do that, then they have improvements.”
“The first time I did [lingual strengthening] with someone. He loved seeing those numbers going up and up every week. I think that was really rewarding for him with [lingual strengthening].”
They emphasized the benefit of a clinical decision framework to aid in determining the most appropriate tool based on clinically relevant patient factors.
“Along with the standardization, having some criteria for implementing set devices or treatment modalities. So, if they perform at this rate on this study consider x, y, and z, but not this. It allows a framework.”
Additionally, SLPs noted that the VA infrastructure supporting telehealth was beneficial in retaining patients in the program without adding the burden of travel:
“Now that we have VVC [telehealth] we have a renewed interest and positive feelings about using telehealth. We have been doing that very successfully with some of our Veterans already.”
“We do a lot of telehealth here, so we’re all pretty familiar with the different options. For the most part, most of our Veterans are very happy with just the phone call follow-up. They prefer that method. But we always do offer telehealth in case they want to be seen either in person or over the computer.”
Some providers expressed that more complex technology (eg, a tablet interface) could be frustrating for patients, particularly when devices were not working correctly and the SLP could not troubleshoot problems remotely. However, they reported that the addition of other therapy tools increased options available for patients, regardless of familiarity with technology.
“I will say. . . if we felt like somebody could benefit from a progressive isometric strengthening program, using certain lingual strengthening devices was great for people with a higher level technology knowledge whereas other devices may be more beneficial for somebody who was a little bit more low-tech and had trouble with the touchscreen and looking at all of the numbers and things like that.”
Discussion
Results from the survey and qualitative sessions revealed that SLPs participating in the IDT program are generally positive and enthusiastic about the program and the benefits it offers to SLP workflows and patient outcomes. There was broad consensus about the need for a structured program with a standardized toolkit and established follow-up visit points as well as the benefit of innovative therapy devices to facilitate swallowing therapy. Participants highlighted successful efforts by IDT program leadership to streamline outcomes tools and clinical workflows. They also noted that the device-facilitated therapy approaches included in the program offer greater choice to Veterans, expanded knowledge and skillsets for both experienced and newer SLP clinicians, and engendered patient motivation to stay engaged in treatment.
There was also general agreement on factors associated with identifying patients as appropriate candidates for intensive therapy programs and the characteristics that may enhance or impair adherence and participation in intensive therapy. Specific factors included cognitive functioning, support from the patient’s family and/or caregiver, patient insight into deficits and motivation for improvement, and treatment setting. Several of these factors aligned with those identified in a recent publication by Krekeler et al, 26 which describes a conceptual model of adherence comprised of a variety of fixed and modifiable factors that may influence patient adherence to dysphagia-related treatment recommendations.
Barriers to program implementation were identified by stakeholder providers through this program evaluation process. Although most survey participants indicated that there was minimal impact to their daily clinic workload, focus group participants emphasized that the time required to enter data into the VA REDCap database secondary to documentation in the electronic healthcare record system was a particular challenge. In addition, SLPs identified a desire for more frequent communication from program leadership regarding the broader programmatic goals, particularly as treatment options expand. These are key factors to address going forward in reducing barriers to implementation, and communication has specifically been highlighted in the literature as a critical element for sustained quality improvement efforts.27,28
While research on barriers and facilitators to clinical implementation of evidence-based therapy specific to dysphagia is limited, several themes identified throughout these qualitative sessions are congruent with barriers and facilitators identified in a recent publication from the aphasia literature by Baker et al. 29 Specifically, barriers found in their study included changing routines and time investment as well as patients coping with acute medical problems. These are consistent with comments from SLPs in this study reporting challenges with finding time for data entry and for coordinating interdisciplinary team meetings, in addition to patients’ medical conditions impacting desire and motivation to participate in treatment. Facilitators included the availability of structured guidelines to facilitate evidence-based clinical practice and having a supportive peer and leadership environment to implement stepped-up psychological approaches. These aligned with SLP-reported facilitators of having an evidence-based framework to assist in guiding treatment decisions and monthly calls with other participating sites for support and collaboration. These commonalities highlight the need to develop additional supportive tools to aid clinicians (eg, documentation templates and patient education materials) while being minimally disruptive to already-busy clinical schedules as well as continuing to promote supportive environments for provider peer support.
To our knowledge, only 1 other study to date by Carnaby and Harenberg (2013) has obtained clinician’s perspectives on factors influencing success in swallowing therapy. Results of this survey study showed that clinicians report premorbid disease progression and cognitive impairment as primary reasons for limited therapeutic performance. 12 Clinicians in the current study also identified cognition as a limiting factor. Given that cognitive impairment may be concomitant with many dysphagia-related diseases, future research is needed to assess the feasibility and acceptability of rehabilitative dysphagia interventions in patients with impaired cognitive status.
The findings of this study have already informed program improvement initiatives leading to the creation of additional resources to support new and existing IDT program facilities. A national VA SharePoint site has been created which allows for more efficient deployment of program materials, availability of monthly call recordings, access to demonstration videos for improved learning, and clinical tools and templates to reduce provider burden. This SharePoint also hosts guidelines for purchasing and for sterile processing of program equipment that can be adapted to any facility within the VA system. Monthly communications with sites provide updates regarding program-wide enrollment, progress toward program goals, and upcoming opportunities for education. Additionally, monthly surveys now are administered through VA REDCap for facilities to report enrollment as well as challenges and successes regarding program implementation. To more efficiently deploy equipment, new facilities complete questionnaires defining equipment needs. Each site also meets regularly with the national program manager to work through implementation barriers. SLPs at newly added sites are provided with a training plan to foster skill development specific to program treatment modalities and can participate in bi-monthly office hours, as needed. Finally, routine review of outcomes by IDT program leadership seeks to further streamline data collection and entry burden while maintaining high clinical relevance.
Although this mixed-methods analysis generated important insights for program improvement, it is important to highlight some limitations to this work. The response rate on the survey was 52.1%, which raises concern for non-response bias. Due to staff and time constraints, participants from only 3 of 8 potential sites at the time were able to participate in the interview/focus group sessions. This may have reduced our ability to achieve conceptual saturation specific to program barriers and facilitators. Future program evaluation efforts will offer opportunities for more IDT program facilities to be involved. In addition, only SLP providers were surveyed at this time; future evaluations will include other stakeholder providers from ancillary services. Furthermore, the program has grown to encompass additional treatments since this evaluation process. It will be important to continually elicit feedback from stakeholder providers as we work to further hone and improve the program for broader dissemination. Finally, it is essential that future evaluation efforts account for the patient perspectives specific to program delivery.
In conclusion, while the IDT program provides an evidence-based framework for dysphagia assessment and treatment, provider stakeholder perspectives on how to optimize program implementation at additional sites and improve patients’ experiences will be critical as we seek to integrate this model into standard of care. The IDT program has a unique opportunity to increase access to and improve the quality of dysphagia-related care both within the Department of Veterans Affairs and across the field of speech-language pathology.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Geriatrics and Extended Care and Office of Rural Health services of the VA and to N.R.P. from the NIH (grant number 1K76AG068590). The manuscript was prepared at William S. Middleton Veteran Affairs Hospital at the Geriatric Research, Educational and Clinical Center in Madison, Wisconsin (GRECC manuscript 009-2002). The views and content expressed in this article are solely the responsibility of the authors and do not necessarily reflect the position, policy, or official views of the Department of Veteran Affairs or the U.S. government.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
N.R.P., R.M., and B.S. developed survey questions. J.Y., N.R.P., M.P., and N.M. analyzed the survey data and formulated interview questions. M.K. conducted interviews. S.D. completed transcription. J.Y. inductively coded the transcripts. J.Y., M.P., and N.R.P. wrote the manuscript with input from all authors.