
Abstract
Timor-Leste faces many challenges implementing quality maternal, newborn and child health (MNCH) services due to resource constraints and socio-cultural factors that disproportionately affect the health of women and children. A scoping review was conducted to map the quality of MNCH services against WHO quality standards on: 1. Provision of care, 2. Experiences of care, and 3. Cross-cutting standards. The literature search identified 1058 citations, from which 28 full-text articles met the inclusion criteria. The findings highlight health workers’ limited capacity to provide quality services and referrals. The major reasons for this are: a lack of essential supplies, poor infrastructure and transport, limited opportunities for ongoing learning, and gaps in health information systems. Provision of care standards and cross-cutting standards require attention at a broad systems level. Findings related to experiences of care highlight the importance of effective communication, respect, and emotional support, particularly for vulnerable women and children who have difficulty accessing services, and for those who have experienced violence. These experience-related standards could be addressed at an individual health worker and health service level, as well as at a systems level. This review provides direction to focus quality-improvement initiatives within local health facilities, as well as at municipal and national level.
Background
Health care for women and children has been an important focus of the Sustainable Development Goals (SDGs). This focus is encapsulated in goal number 3: “Ensure healthy lives and promote well-being for all at all ages.” 1 The goal outlines specific targets including, to reduce maternal, neonatal, and child mortality (by 2030), to ensure universal access to sexual and reproductive health care services, and to achieve universal health coverage (UHC). All these targets require the coordination and delivery of quality health services within accountable health systems. Health systems that have the capacity to measure and use data to improve services. 2 Despite substantial progress during the era of the Millennium Development Goals (MDGs), inadequate resources remain a significant challenge to achieving the SDGs. 3 In regions such as Sub-Saharan Africa and Southern Asia lack of access to quality health care and extreme poverty are major contributory factors to high rates of maternal, neonatal, and child mortality.4,5
The World Health Organization (WHO) has widely advocated for improvements in the quality of maternal, newborn, and child health. It has established frameworks and standards for improving the quality of maternal and newborn care, and that of children and adolescents, in health facilities.6,7 These frameworks identify standards vital to achieving quality improvement, including: 1. Evidence-based practices for routine care and management of complications; 2. Actionable information systems; 3. Functional referral systems; 4. Effective communication; 5. Respect and preservation of dignity; 6. Emotional support; 7. Competent, motivated human resources, and 8. Availability of essential physical resources. The first 3 standards reflect “provision of care,” the next 3 the “experience of care” and the last 2 address cross-cutting factors which are pre-requisite standards for providing both the provision and experience of care standards.6,7
Providing quality health services has proved difficult in low- and middle-income countries.8-10 A task made more challenging when resource limitations are combined with ongoing political and social conflict.11,12 Timor-Leste is a post-conflict country situated between South East Asia, Australia and the Pacific; it is the newest nation in Asia. Independence from Indonesia was achieved in 2002 after years of occupation. 13 Substantial progress has been made to rebuild the health care system following Indonesian forces exit from the country, however major challenges remain to achieve health and wellbeing for the nation’s most vulnerable. 14 The 72% of Timor-Leste’s population live in rural and remote areas and 42% live below the poverty line.15,16 The pregnancy-related mortality ratio is 218 deaths per 100 000 live births and infant and under-5 mortality rates are 30 and 41 deaths per 1000 live births, respectively.15,16 Maternal and child health services are provided by a multidisciplinary cadre of health workers including doctors, nurses, and midwives. 16 Delivering quality and accessible maternal, newborn, and child health (MNCH) care remains a priority focus for the Government of Timor-Leste and its development partners.
The aim of this review is to search the literature on MNCH service delivery in Timor-Leste and to map factors affecting quality of care based on WHO quality standards. The review offers a framework for stakeholders who want to improve the quality of care in Timor-Leste, and provides a baseline analysis for designing MNCH quality improvement initiatives linked to WHO evidence-based standards.
Methods
This review was undertaken as part of a larger study on quality improvement of MNCH services in Timor-Leste. A scoping review methodology was chosen to assess the extent of the literature and to explore factors affecting the quality of MNCH services in Timor-Leste. Arksey and O’Malley’s framework was used to guide the review using the following steps: 1. Identifying the research question, 2. Identifying relevant studies, 3. Study selection, 4. Charting the data, and 5. Collating, summarizing and reporting the results.17,18 The review focused on articles published within 5 years prior to commencement of the study in 2018.
Identifying the Research Question
There were 2 main research questions:
What quality oriented MNCH literature exists in the context of Timor-Leste?
To what extent do the retrieved articles address the recent WHO quality standards?
Identifying Relevant Studies
We accessed 7 electronic databases: MEDLINE, Ovid Emcare, Cochrane Library, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Informit, and Scopus. Gray literature sources, including Google Scholar, Google, and One Search, were searched for additional articles relevant to the topic. A targeted search of the Timor-Leste government website was performed via Google to elicit any publicly available government documents or other gray literature.
The search strategy used the following MeSH subject headings: “Quality improvement” OR “Patient-centered care” AND “Maternal health” OR “Child health” AND “Timor-Leste.”
The inclusion criteria were:
Published literature
Unpublished gray literature
Between 2014 and 2018
Written in English
Timor-Leste context
Relevant to MNCH service delivery
The exclusion criteria were:
Articles outside of year range
Languages other than English
Global or regional reports with minimal Timor-Leste content
Articles with context outside of MNCH
Articles that could not be linked to any areas of WHO quality improvement framework
Study Selection
Tricco et al 19 describe a 2-staged screening process utilizing the PRISMA framework. One author (MK) assessed the retrieved articles against the inclusion and exclusion criteria. Ambiguous articles were resolved by consensus amongst the co-authors. A sub-sample was then checked by the second author (DL) for accuracy.
Through title screening, articles were excluded that did not relate to quality of health care or MNCH in Timor-Leste. When abstract screening, the keywords “Quality,” “Timor,” “Maternal,” and “Child” were used to assess eligibility. In cases where these words were not identified in an abstract the full text was searched. Articles that described Timor-Leste within a global context or with other countries were included only if they provided a sufficient level of information related to Timor-Leste. While screening full texts, articles were further investigated to assess whether they could inform 1 or more of the WHO quality standards.
The literature search yielded 1058 articles which, after removal of duplicates, was reduced to 481. Four hundred fifteen publications were excluded after title and abstract review because they did not meet the criteria for publication year, Timor-Leste setting, MNCH topic or were assessed as not relevant. Sixty-six full text publications were screened and a further 38 articles excluded because they did not provide relevant information related to any of the WHO quality standards, or because they were multi-country publications that mentioned Timor-Leste but did not provide detailed, country-specific information. Thus, the screening yielded 28 articles for inclusion in the scoping review (Figure 1).

Search summary using PRISMA flow diagram.
Charting the Data
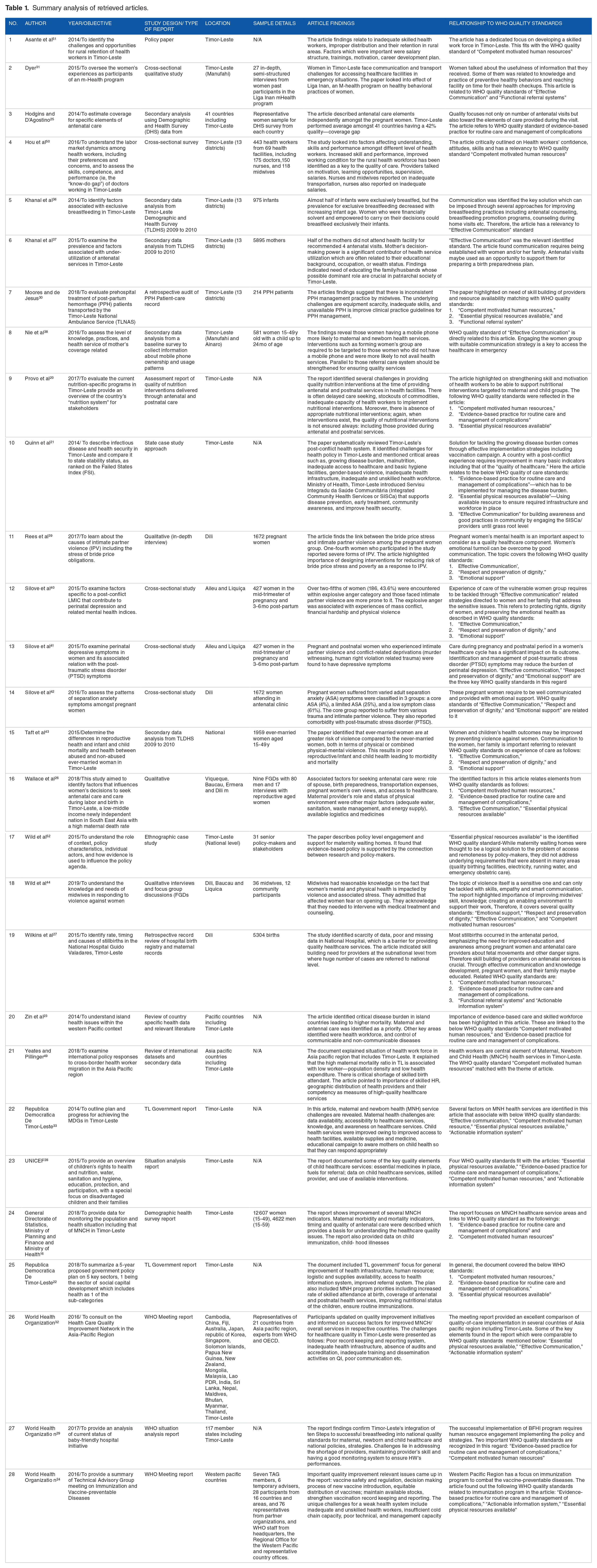
A data extraction table for charting study characteristics, key findings, and relationship with WHO quality standards was developed by the authors through consensus. The extraction table consisted of columns to record information on the author, year of publication, objective, study design/type of report, location/study context, sample/participants, article findings, and relationship to WHO quality standards (Table 1). Data were extracted from the full text articles by the first author (MK) and a sub-sample were reviewed by 2 co-authors (DL, KW) for accuracy. Any discrepancy in interpretation was discussed and resolved by consensus amongst the authors.
Summary analysis of retrieved articles.
Collating, Summarizing, and Reporting the Results
The findings from the retrieved articles were mapped against each domain of the WHO quality standards to provide a narrative overview of existing literature related to each of the themes. A basic description of the number of articles that fell into each domain was included to provide an overview of the extent and distribution of the studies.
Findings
The findings section is presented according to the WHO quality of care standards: 1. Provision of care standards, 2. Experience of care standards, and 3. Cross-cutting standards. A total of 28 articles were included in the review, many of the articles covered multiple standards. Nineteen articles were related to provision of care, 25 articles were related to experience of care, and 24 articles addressed cross-cutting standards (Table 2).
Number of retrieved articles linked with WHO quality standards.

Provision of care
The provision of care domain covers 3 elements: a. Evidence-based care practices for routine care and management of complications, b. Referral, and c. Data management. The review findings on this domain are summarized below.
Evidence-based care practices for routine care and management of complications (11 articles)
The findings indicate the importance of service providers adhering to clinical protocols in managing nutrition interventions,20-22 infectious diseases,21,23 immunization,15,22,24 antenatal care,24-27 and child health services.28,29 One report cites the inadequate capacity of health workers, limited availability or stock-outs of commodities, and delayed care-seeking, as challenges to implementation of nutritional interventions within antenatal and postnatal care services in Timor-Leste. 20 Another article suggests that women will seek health care from a facility when they have confidence in the health care provider, which relies on the provider following evidence-based guidelines. 25
Functional referral system (3 articles)
A functional referral system manages referral cases according to protocols. Rapid transportation to higher-level facilities is used when required. Three articles identified poor road conditions in Timor-Leste as posing difficulties for referral transportation.27,30,31 One article contended that high numbers of referrals to tertiary hospitals were due to low skill levels of health care providers in community settings . 27 Another study described the management of postpartum hemorrhage (PPH) by paramedics while transporting patients to a higher-level facility, using the Timor-Leste National Ambulance Service. 30 The retrospective audits found paramedics diagnosed 85% of cases, but did not regularly use resources available to them such as oxygen and intravenous isotonic crystalloid fluid. This study illustrates how referral systems are linked to other provision of care standards such as the routine management of complications.
Actionable information systems (5 articles)
The review identified gaps in information systems, highlighting improper record keeping practices, missing records, and a scarcity of data, particularly with regard to maternal health, child health, and vaccinations.24,27,28,32,33 According to 1 study, more than 60% of death data was found to be missing or incomplete in tertiary hospital settings. 27
Experience of care
The experience of care standards refer to the experiences of clients at the point of care.6,7,34 The 3 elements covered are: a. Effective communication, b. Respect and preservation of dignity, and c. Emotional support. All these elements are critical in the post-conflict social landscape of Timor-Leste. Several articles in the literature review highlight experience of care through the concept of patient-centered care, a model that prioritizes the needs and rights of the person receiving care and puts them at the center of decisions that affect them.
Effective communication (14 articles)
The review identified 14 articles that addressed the theme of “communication” to facilitate healthcare delivery and improve the experiences of pregnant women and their children.21,26,31-33,35-43 Two articles recommend antenatal counseling by skilled providers, a provision that can impact women’s decision-making during labor and childbirth and influence breastfeeding practices.36,37 Midwives play an important role in the communication of information to women both in-person and by using mobile phone technology. 31 One article describes the implementation of Liga Inan (Connecting Mothers), an mHealth program designed to promote communication between midwives and pregnant women using mobile phone messaging. 38 Women described the usefulness of the service, which provided information on healthy behaviors and reminded them when they had an appointment at a health facility. Having access to a mobile phone helped women receive health information and increased their understanding of health care services. One study found a link between mobile phone ownership and increased use of maternal and newborn health services, however after adjusting for socioeconomic factors, mobile phone ownership was not independently associated with service use. 38
Intimate partner violence (IPV) is common in Timor-Leste. Women who have experienced such violence exhibit higher rates of sexually transmitted infection, low birthweight births, and pregnancy termination than the general population. They have lower attendance at antenatal clinics and are at greater risk of morbidity and mortality. 39 Health providers can play a critical role in addressing the issue of IPV through sensitive communication with women about their needs, and by providing advice on how they can best be assisted to safety. 39
Explosive anger, 40 depression, 41 and adult separation anxiety (ASA) 42 have been observed in women, especially married women, during their pregnancy and postnatal period. 43 If IPV and mental health issues are not addressed there could be significant consequences for women and children’s physical and mental health. In one study, midwives emphasized that, in addition to sensitive communication, women require health system factors like patient privacy and suitable appointment lengths to be in place so that they can talk openly about their problems. 35
In a global consultation forum poor communication was reported as a barrier to the delivery of quality healthcare services. 32 One Government report emphasized women’s lack of knowledge about how to access health care services, indicating the need for broader communication with communities and outreach by health services. 33 The article also highlights the role of educational campaigns in improving people’s understanding of child health issues. For example, Servisu Integrado du Saude Comunidade (SISCa), an Integrated Community Health Service Program introduced by the Ministry of Health, serves as an awareness building platform for the prevention of diseases. 21
Respect and preservation of dignity (6 articles)
Respect and dignity are an essential element of quality of care. Articles from the literature search related to this domain were mostly focused on the needs of women who have a history of trauma and violence.39-44 Health providers’ empathy, confidentiality and communication skills, as well as referral of women to appropriate services, play a critical role in increasing patient safety and preservation of dignity. 44
Emotional support (6 articles)
Similar to the need to show respect and preservation of dignity, women who have experienced trauma need significant emotional support.39-43,45 One article found that a quarter of study participants were subjected to IPV, which was associated with cultural obligations and bride price stress. 39 Midwives providing health services to women acknowledged the fear felt by women speaking out about the violence they face. 45 The midwives recognize the importance of kindness and emotional support when providing counseling and discussing treatment options with these women.
Cross-cutting standards
Cross-cutting standards include competent and motivated human resources, and the availability of essential physical resources. Available human and physical resources were the key challenges identified in this review. Inadequate availability of skilled providers, especially in rural settings, has been a key constraint in Timor-Leste since independence. 46 A study performed in Rivers State, Nigeria found that more than 50% of primary health care workers wanted to move away from their current place of work. 47 Similarly, rural retention has been identified as a problem in a policy analysis in Bangladesh. 48
Competent motivated human resources (14 articles)
A critical element in delivering quality health care is a skilled workforce, identified in the WHO quality standards as a “competent motivated human resource.” Fourteen articles in the literature search included issues related to human resources for health in Timor-Leste.16,20,22,23,26-30,33,44,49-51 Two government reports focus on interventions to do with human resources and identify increasing the number of skilled-birth attendants (SBAs) as a priority program area for MNCH services.22,33 Two articles highlight Timor-Leste’s health workforce crisis within the Asia Pacific region and focus on insufficient number of SBAs.23,49 The latter article also highlights low worker population density and low expenditure on health services as factors that contributed to high maternal mortality in Timor-Leste. 49
One article reports additional challenges in providing skilled nutrition interventions to women and children when there is a scarcity of supplies and commodities, or when the women arrive late for care. 20 Another article stresses that skilled health care workers are required to deliver quality health care services to children 28 The limited skills of midwives was described as a challenge in 1 article, which found inconsistent practices in the management of post-partum hemorrhage (PPH) when transporting women to health facilities. 30
The 2016 Timor-Leste Demographic and Health Survey reported that only 57% of births were assisted by skilled health care workers, and that the number of those workers available to assist with births varied substantially by municipality. 16 Quality antenatal care provision requires the employment of skilled maternal health workers however, less than half (45%) of women received the recommended 4 antenatal visits. 16 One report described Timor-Leste’s achievement in integrating the 10 Steps to Successful Breastfeeding into national quality standards for MNCH. 29 Two articles describe the shortage of health care workers as a critical issue, especially in rural areas.50,51 Midwives are the core providers managing pregnant women and children in health care facilities and are often required to handle sensitive cases of pregnancy-related violence and/or mental health issues. 45 They are therefore a central component of the health workforce providing healthcare services to women and children. 16
Pregnant women reported lack of confidence in the skill of providers as a reason for not visiting health care facilities. 26 One article attributed the high rate of referrals to tertiary level health facilities to the inadequate skill of health care providers in lower-level facilities. 27 Health care workers identified inadequate pay, transport difficulties, lack of training or continuous learning opportunities, and inadequate supervision as important barriers to providing quality MNCH services. 50
Essential physical resources available (10 articles)
Timor-Leste has progressed significantly in rebuilding its health infrastructure since it achieved independence from Indonesia,21,22,32,33 but more development is needed. Two major challenges for the country are continued improvement of the infrastructure and ensuring widespread availability of essential resources.
Lack of adequate water and sanitation were identified as reasons why women do not seek antenatal care. 26 Stock-outs of commodities have been identified as a challenge to implementing nutrition 20 and vaccination programs, 24 making it harder for providers to offer a quality service. Even when skilled health workers are available equipment scarcity poses challenges, for example, when managing PPH patients during transportation via ambulance. 30 Fuel shortages for ambulances result in a threat to successful critical care outcomes. 28
One paper analyzed policy-level support for building maternity waiting homes and found that they were considered an appealing policy option because they attract donor investment in infrastructure. There is little evidence to show that waiting homes improve access to care for women in remote areas. 52
One Government article outlined a 5-year plan for improving logistics, supplies and infrastructure to address quality within health care services. 22
Discussion
This review on the state of MNCH care in Timor-Leste found significant limitations across all 3 of the WHO quality standards including the provision and experience of care as well as cross-cutting standards.
Provision of Care Standards
The review highlights the need for evidence-based guidelines and protocols for managing critical health issues, particularly in maternal and child health, as priority areas for intervention. Evidence-based practice of MNCH was positively influenced by workers’ skill-building through training and support for implementation.53,54 A fact that reinforces the need to continue support for developing the knowledge and skills of health workers. In addition to clinical guidelines and training, it is important to include regular refresher training, based on knowledge and skill gaps, and to support implementation with ongoing mentoring within an enabling environment.
Access to health care and timely referral are ongoing challenges in Timor-Leste.27,30,31 Challenges associated with maternal and neonatal referrals have been widely reported in other low- and middle-income countries. 55 Factors influencing referral systems in Timor-Leste are: low skill levels of health care workers in charge of managing complications, lack of staff in health facilities, poor road networks, fuel scarcity and a lack of functioning vehicles, and poor weather conditions—particularly in the wet season. The challenges associated with referral are exacerbated by the difficulties people face accessing health services, which include: lack of transport, poor road conditions, gender inequality, and poverty. 56 These factors combine to severely limit access to appropriate levels of care, particularly for women and children in remote areas. In the face of these challenges, women and their families tend to rely on traditional medicine and assistance from traditional birth attendants.
In addition to improving referral between levels of service, research from Timor-Leste recommends improving quality of care within health services, increasing the availability and functioning of general patient transport services, and the provision of travel subsidies to patients and their families. 56
Experience of Care Standards
Studies related to experience of care appeared the highest number of times in the retrieved articles (total 25 articles). Health providers, especially midwives who provide the majority of maternal, child, and reproductive health care, have a critical role in establishing a respectful and supportive relationship with their clients, communicating information, and discussing care options with women and their families.
In Timor-Leste there are high rates of gender inequality and normalization of violence against women and children, which result in adverse health outcomes. 45 Other research from Timor-Leste demonstrates the damage domestic violence does to women’s physical and mental health, examples of which include explosive anger and long-term depression.40-42 Health workers are often the first service providers women come into contact with as they seek care for injuries or chronic health problems resulting from IPV. In these situations, it is critical that health providers can offer emotional support, safety planning and appropriate referrals, in addition to medical care. However, in Timor-Leste it is common for health providers to blame women and to ask them what they did to cause the abuse.35,57 Although there are national guidelines for health providers to assist survivors of IPV, 35 there is much to be done to improve communication, respect, and emotional support to vulnerable people given the magnitude of violence against women, children, and people with disabilities in Timor-Leste. 58
Cross-cutting Standards
The availability of human and essential physical resources in the health sector are key challenges identified in this review. A lack of skilled health care workers in rural settings has been a constraint to health service delivery since Timor-Leste’s independence from Indonesia.14,46,56 Factors that contribute to the lack of skilled health care workers in Timor-Leste include: limited opportunities for continuous learning, insufficient supervision, poor working conditions, lack of transport, and low salaries. 50 A study of health worker migration in Asia Pacific reported that retention of health workers in rural areas is a critical problem that could be addressed through education, personal and professional support, financial incentives, and regulatory and health system supports. 49
This review also reinforced the need for sufficient physical resources, without which skilled health workers may not be able to provide adequate care. In Timor-Leste, the delivery of MNCH services continues to be hampered by a lack of infrastructure, stock-outs of essential equipment and medicines, poor water and sanitation facilities, a lack of functional ambulances and emergency transport, and a lack of time and privacy during consultations.
Conclusion
This review has captured recent literature related to WHO quality standards in the delivery of MNCH services in Timor-Leste. As the Ministry of Health and its development partners focus on improving quality of care in Timor-Leste, the findings provide direction on specific areas that can be targeted for MNCH improvement. While many of the issues identified are systemic and require high-level policy and system-wide support (such as evidence-based guidelines, referral systems, health information systems, deployment of human resources, and essential infrastructure and supplies), other issues can be addressed at the provider and health facility level (such as effective communication, respect, emotional support, distribution of clinical resources, and reflection on and use of health system data). There is a growing body of evidence that quality improvement initiatives can be effective in low-resource settings.59,60 However, these initiatives rely on accurate information and health system data. Poor quality data was a major challenge identified in this review24,27,28,32,33and has been documented in MNCH services in other low-resource settings.61,62 An important first step in the quality of care agenda in Timor-Leste is therefore improving case recording, and educating health providers as to its importance. In addition, building skills in data management and the use of information for resource allocation, reflection, and for planning quality improvement initiatives. The country also requires strategies and practical solutions to overcome geographic constraints to accessing care. The challenges facing health services are diverse, and therefore further work is needed to identify specific local needs, strengths, and resources and to consider how this knowledge can be used to improve MNCH services in distinct parts of the country and at various levels of the system. Given the multi-layered and intersecting nature of quality standards, initiatives will need to be addressed in all parts of the health care service, at national and municipal levels, in local health facilities, and by individual health care workers. Stakeholder’s critical understanding of these vital quality standards can enhance policies to improve MNCH services in Timor-Leste. Policy formulation on MNCH quality improvement in Timor-Leste requires critical linkage of matching the existing situation with the available quality standards.
Footnotes
Acknowledgements
The authors would like to thank Stephen Anderson, the Senior Liaison Librarian, James Cook University to provide immense support for facilitating the searching for the review.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MK - Design of the study, development of the search strategy, acquisition of data, reviewing the literature, analysis and interpretation of data, drafting of the manuscript, critical revision of the manuscript. DL – Development of the outline of the manuscript framework, quality checking, and interpretation of data, critical revision of the manuscript. MM - Design of the study, quality checking, interpretation of data, revision of the manuscript. CW - Outline of the manuscript framework, revision of the manuscript. KW - Clarify the search strategy, quality checking, and interpretation of data, and critical revision of the manuscript.