
Abstract
Background:
Health professionals (HPs) coping with the coronavirus pandemic are at risk of working under stressful conditions impacting their professional well-being. The aim of this paper was to explore HP’s professional quality of life and occupational stress during the COVID-19 pandemic in Greece.
Method:
A cross-sectional study was conducted (from October to December 2020) in a COVID-19 reference hospital, one of the biggest in Attica. The method of convenience sampling has been used. Data collection was carried out through an anonymous, self-administered questionnaire including, apart from HPs’ demographic and occupational characteristics, Professional Quality of Life Scale (ProQoL) and Job Stress Measure. A total of 250 questionnaires were distributed to physicians and nurses. One hundred eighty-six questionnaires were fully completed (response rate = 78.8%). The analysis was based on descriptive and inductive statistics, using SPSS v25.
Results:
Participants’ mean age was 41.5 ± 10.4 years; 75.3% were women and 62.4% was nursing staff. ProQoL analysis showed that the majority had moderate compassion satisfaction (74.2%) and burnout (78.5%), while 48.8% had moderate level of secondary post-traumatic stress. The mean value of occupational stress was estimated at 2.76, showing a moderate level of stress. HPs’ demographic and occupational characteristics seemed to affect both work stress and ProQoL (P ⩽ .05). Occupational stress was positively correlated with both burnout (r = 0.461, P = .001) and secondary post-traumatic stress (r = 0.596, P = .001), indicating that an increase in health professionals’ stress at work corresponds to a simultaneous increase in ProQoL.
Conclusions:
HPs’ professional quality of life and occupational stress seemed to be moderate during the COVID-19 pandemic in Greece. In order to achieve an improvement in HPs’ overall professional well-being, priority should be given to the strengthening of the capacity of the healthcare system as well as to supporting HPs in both stress management and psychological resilience.
Introduction
The coronavirus disease 2019 (COVID-19) outbreak has been acknowledged as a global health threat negatively impacting countries’ health care systems and economies.1-4 Numerous cooperative efforts have been initiated by international and European organizations focusing on the implementation of health strategies, funding programs, policy recommendations and socioeconomic recovery plans.5-7
The disruption caused by the COVID-19 pandemic has drastically altered people’s everyday lives and global mental health has become an urgent issue, identified as the tenth leading research topic. 8 Plenty of studies have deduced that COVID-19 has devastating effects on the mental health of the general population, such as depression and anxiety.9-11 A global systematic review regarding mental health symptoms in the general population during the COVID-19 pandemic, showed levels of anxiety ranging from 6.33% to 50.9%, levels of depression from 14.6% to 48.3%, post-traumatic stress disorder from 7% to 53.8%, psychological distress from 34.43% to 38%, and final levels of stress ranging from 8.1% to 81.9%. 12
Additionally, the foregoing results are in accordance with a multinational population-based study conducted in middle-income Asian countries; respondents scored high level of stress, anxiety and depression. 13
As far as the general population is concerned, gender (female), age (⩽40 years), low educational background, chronic diseases, COVID-19 infection, contact with COVID-19 patients and delayed lock-down measures are risk factors associated with adverse mental health.12,14 Another factor that has to do with poor mental health relates to people’s mood, that is, people with mood disorders may be at greater risk for COVID-19 hospitalization and death. 15
As far as the health professionals (HPs) specifically are concerned, sociodemographic and occupational risk factors relating to increased mental disorders include gender (female), age (⩽40 years), limited experience, working in intensive care units (ICU), emergency settings with direct patient contact or working on the frontline. 16
The pandemic brought a wide range of challenges for healthcare professionals, such as witnessing a large number of deaths, facing rational decisions, risk of infection and family members’ exposure, increased workload and working without sufficient equipment.17-19 These stressful conditions also brought symptoms of mental disorders and somatization to healthcare workers.20-22 These short and long term challenges are impacting health professionals’ efficiency, occupational stress and patient care, by influencing their professional quality of life (ProQoL).23,24
ProQoL is a complex concept associated with the degree to which employees are able to fulfill their personal needs through their work environment experiences. 25 It incorporates 2 aspects, the positive (Compassion Satisfaction-CS) and the negative (Compassion Fatigue-CF). Compassion Satisfaction includes people feeling invigorated by their work whereas Compassion Fatigue includes people suffering from burnout (BO) and secondary traumatic stress (STS). BO is characterized by feelings of unhappiness, disconnectedness and insensitivity to the working environment. STS includes inability to sleep and distinguishes between private and professional life. 26 Previous studies suggest that better professional quality of life is associated to less mental disorders27,28 and perceived stress.29,30 Many factors relating to HPs’ professional and social role, such as ambiguity, role conflict and workload can provoke work stress, resulting to the reduction of professional efficiency, especially during the coronavirus pandemic.31-33
Numerous studies focusing on the 2003 SARS epidemic reported that health professionals working in SARS units showed high levels of intensity, anxiety symptoms, hostility, and insomnia.34-36 Furthermore, due to direct exposure to patients with the virus, psychological burden, such as fear, insecurity, and secondary traumatic stress have been recorded. 37 Difficulties have also been reported regarding the ability to manage their personal, family and social life. 38 However, nowadays, there is an even higher prevalence of adverse psychiatric outcomes compared to the pre pandemic period.39,40
Greece, along with many other European countries, was hit by the COVID-19 pandemic in early 2020. The government responded immediately by implementing policies aiming to contain the spread of the virus, such as social distancing, suspension of economic, educational and cultural activities and restrictions on citizens’ mobility (lockdown). These measures resulted in minimizing the number of cases and deaths.41,42 It is worth noting here that the COVID-19 measures that Greece implemented came after a severe economic crisis period lasting more than a decade, with significant restrictions in health and pharmaceutical expenditures, inefficiencies in the healthcare workforce and in hospital equipment and supplies.43-45
There are limited studies assessing health professionals’ stress level (emerging from their work environment) and its impact on their personal and professional lives during the COVID-19 pandemic. Therefore, the objective of this study was to explore healthcare professionals’ ProQoL and occupational stress during the pandemic outbreak in Greece.
Methods
Study design and sample selection
A cross-sectional study was conducted at the «Evangelismos» COVID-19 reference hospital. This is one of the largest general hospitals in the region of Attica, with a resource capacity of 943 beds and approximately 2300 physicians and nurses. The study was performed during the second pandemic wave, that is from October to December 2020.
Convenience sampling was the methodology applied and data collection was carried out through a self-administered questionnaire. A total of 250 questionnaires were distributed to physicians and nurses, out of which 186 were completed (response rate = 78.8%). Participants met the following inclusion criteria: they were professionals who were on duty during the aforementioned period and came in contact with patients. Laboratory, administrative and auxiliary staff were excluded from the sample.
Study instrument
An anonymous questionnaire was distributed to the physicians and nurses aiming to assess the professional quality of life in relation to work stress during the period of the COVID-19 pandemic in Greece. The questionnaire was divided into 3 sections. The first section included questions on the socio-demographic and occupational characteristics of the sample. The other 2 sections consisted of the «Professional Quality of Life Scale—ProQoL» and the «Job Stress Measure», respectively.
ProQoL consists of 30 questions-statements examining the quality of professional life of employees through 3 dimensions: (a) compassion satisfaction (CS), (b) burnout (BO), and (c) secondary traumatic stress (STS). Each dimension is psychometrically unique and is not a binding factor for the rest. The tool is measured at a 5-point Likert scale, where 1 corresponds to “never” and 5 to “very often.” A high score in each dimension refers to high levels of compassion satisfaction, burnout and secondary traumatic stress respectively. The questionnaire has been designed by Stamm 26 and is available in several languages, including Greek. 46
Job Stress Measure explores job stress through 16 questions covering 3 dimensions: (a) the characteristics of work including workload, time pressure, occupational safety and bureaucratic procedures, (b) clarity of objectives focusing on tasks’ distribution and conflicting roles, (c) business travel or meetings indicating high travel frequency and length of meetings. The answers are given at a 5-point Likert scale, where 1 corresponds to “no stress” and 5 to “a great deal of stress.” The tool has been translated and validated in Greek by Sakketou et al. 47
Statistical analysis
The data was analyzed by using SPSS v25 (Statistical Package for Social Sciences). The Cronbach alpha index for ProQol and Job Stress Measure showed adequate internal structure and reliability, a = 0.721 and 0.899, respectively. Descriptive statistics such as frequencies, percentages, mean and standard deviation were performed. The variables were normally distributed and, in order to explore any differences, parametric tests were chosen. Statistically significant differences among ProQoL and Job Stress Measure with dichotomous variables were investigated using Student t-test. Also, one way ANOVA was carried out for the analysis of the differences among variables when examining 3 or more groups. Pearson’s correlation test was applied for the relations between professional quality of life and job stress measure. Finally, linear regression analyses using backward method were carried out in order to investigate which factors predict professional quality of life of the sample. The significance level was set at P < .05.
Results
The socio-demographic and occupational characteristics of the sample are presented in Table 1. The mean age of participants was 41.5 ± 10.4 years; women represent the highest proportion (75.3%), 45.2% had a postgraduate educational level, 47.3% married and 45.2% without children.
Socio-demographic and occupational characteristics.

The mean years of working experience was 15.04 ± 10.3, 62.4% was nursing staff, 28% worked in surgical departments and 17.2% in the newly established COVID-19 clinics. The majority (91.4%) of health professionals stated that they came in contact with COVID-19 patients.
According to the ProQol analysis as presented in Figure 1, the majority of the participants had moderate CS (74.2%) and BO (78.5%). As far as STS levels are concerned, participants were almost evenly split among moderate and low levels of STS. The mean value of CS was 36.24 (±6.11), BO 26.53 (±5.17), and STS 23.45 (±6.34).
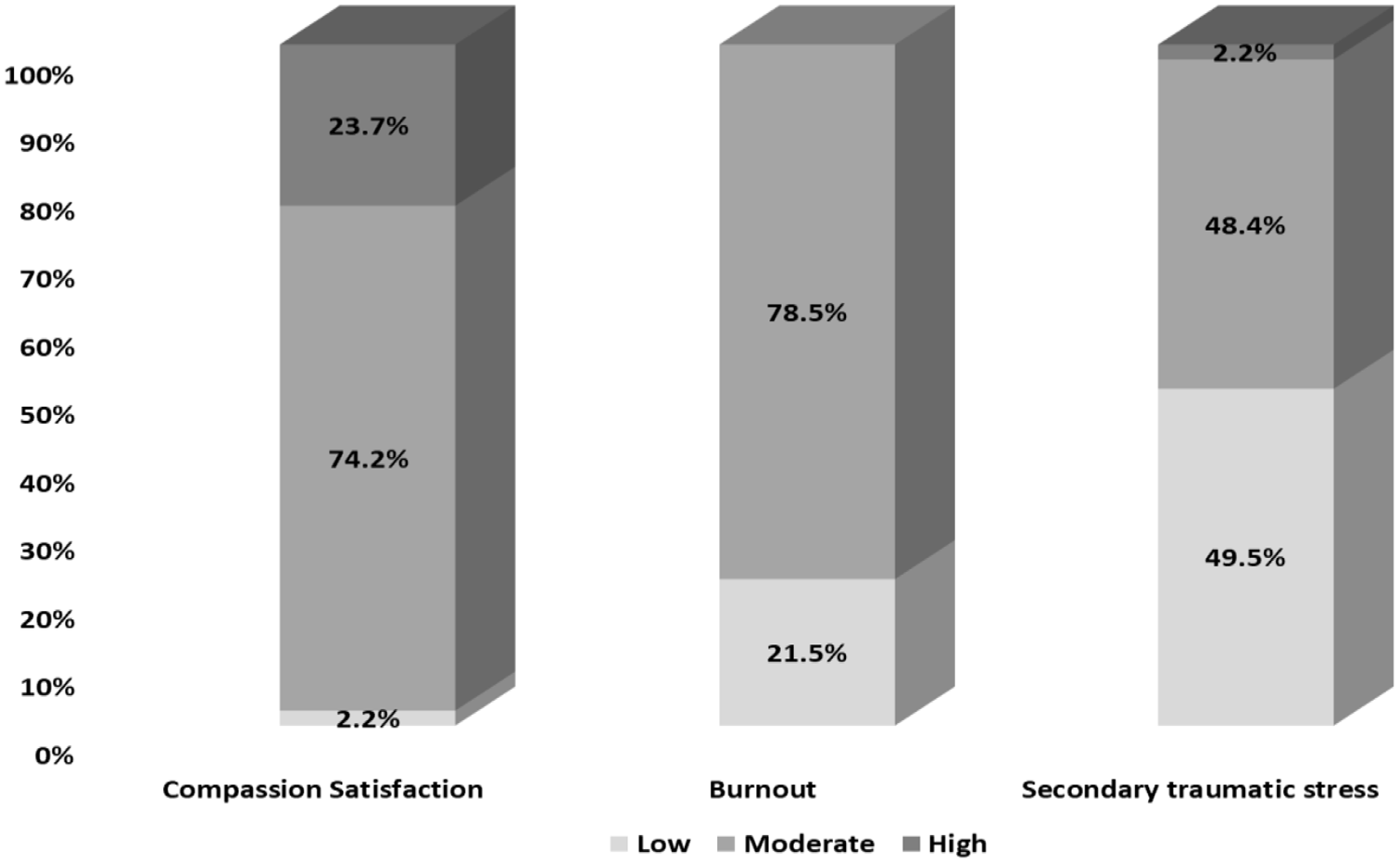
Levels of ProQol dimensions.
As shown in Table 2, the ProQol results are analyzed with respect to the socio-demographic and occupational characteristics of the participants. Women scored significantly higher in CS than men (P = .024). Additionally, unmarried participants scored higher compared to married or divorced/widowed (P = .015) and also, participants with none or one child scored higher in CS compared to those with 2 or more children (P = .001). As far as work experience is concerned, participants with more than 11 years of work experience scored higher than the less experienced ones (P = .010). Those working at emergency departments scored the highest CS while those working at pathological departments scored the lowest CS (P = .001). Regarding BO, significant differences were only found in relation to the working departments (Table 2). Participants working at the pathological, emergency and the COVID-19 units scored a high BO (P = .003). Finally, a high score in STS was found in the following categories of participants; health professionals with secondary education (P = .018), those working in emergencies and COVID-19 units (P = .005) and physicians (P = .020) (Table 2).
Comparisons among health professionals’ ProQol and socio-demographic, occupational characteristics.

The mean value of job stress measure was 2.76 (±0.67) showing a moderate stress level among health professionals. More specifically, as shown in Figure 2, the characteristics of the working environment (2.96 ± 0.7) and clarity of objectives (2.60 ± 0.8) had a moderate impact on stress compared to business traveling or meetings (2.07 ± 0.7).

Dimensions of job stress measure.
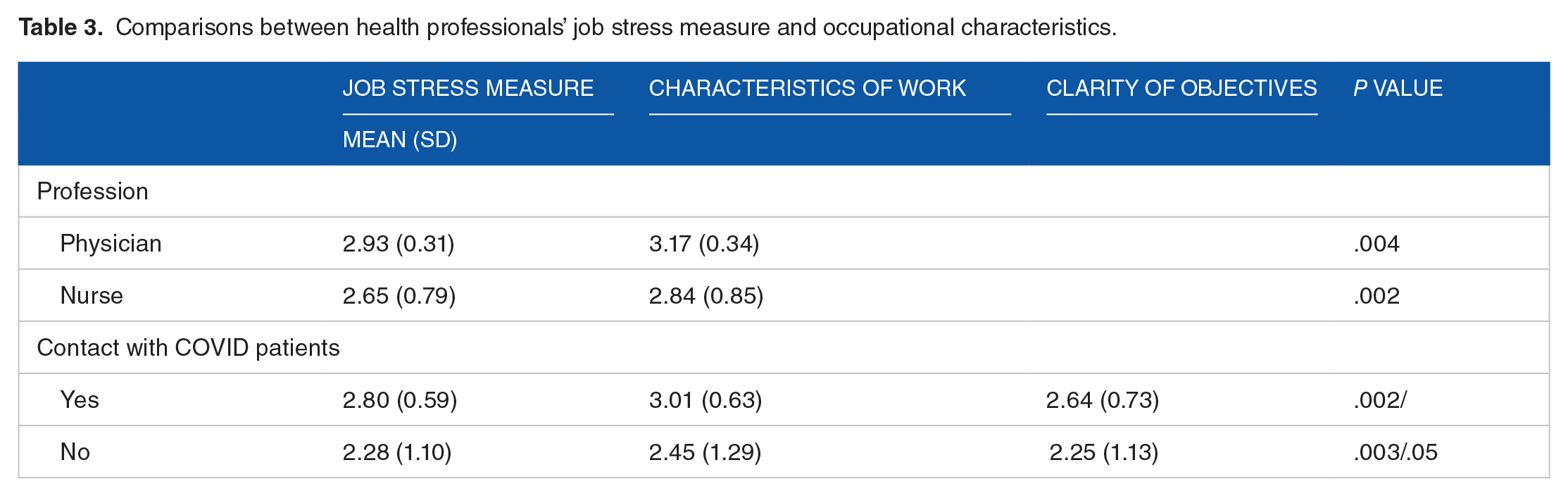
In Table 3, job stress measure with respect to the occupational characteristics of the participants is presented. Physicians were more likely to be stressed from their job and its characteristics compared to nurses (P = .004 and .002, respectively). Additionally, health professionals who came in contact with COVID-19 patients showed higher stress levels.
Comparisons between health professionals’ job stress measure and occupational characteristics.
Job stress and its dimensions are positively correlated with burnout and secondary traumatic stress (Table 4), showing that an increase in health professionals’ stress at work corresponds to a simultaneous increase in the above-mentioned ProQoL dimensions.
Correlation analysis among ProQoL dimensions and Job stress measure.

P < .01.
Finally, in order to investigate the factors that predict ProQol, linear regression analyses were conducted (Table 5). Significant models were found for CS (F[6, 179] = 35.818, P < .001, R2adj = 0.530), BO (F[4, 181] = 82.831, P < .001, R2adj = 0.639), STS (F[6, 179] = 28.847, P < .001, R2adj = 0.475).
Linear regression models for ProQol.

Abbreviations: CS, Compassion Satisfaction; BO, Burnout, STS, Secondary traumatic stress.
Physician = 0, nurses = 1.
Discussion
To our knowledge, this is the first empirical study assessing the degree of stress emerging from the work environment and impacting health professionals’ ProQoL during the COVID-19 pandemic in Greece.
Our ProQoL results revealed that a high percentage of health professionals stated moderate CS, BO, and STS levels. This could be explained by their willingness to efficiently provide their services and the satisfaction they receive by offering them to people in need, especially during these stressful times. Gender, professional experience and educational level seem to be factors that significantly influence health professionals’ ProQoL. More specifically, women as well as health professionals with longer work experience indicated high CS levels, while those with higher education seemed to cope better with STS. Health professionals working in emergency and COVID-19 units were found to be more likely to report high levels in all ProQoL dimensions. Furthermore, physicians indicated higher levels of STS compared to nurses. This finding could be explained by comparing the responsibilities of the 2 groups of health professionals (physicians and nurses) as well as their exposure to extremely stressful events, such as the care of COVID-19 patients.
As concerns job stress, our results showed that health professionals felt moderate stress originating from hard working conditions, heavy workload and multiple responsibilities. This is an expected finding, given the fact that the Greek health care system has been recovering from a long lasting economic crisis43,45 and there are shortages in both human and financial resources. This status, in combination with the stressful conditions of the pandemic, brought ambiguity in the working roles of health professionals. Finally, it is worth mentioning that job stress was positively correlated with burnout and secondary traumatic stress.
The moderate levels in both CS and BO and the moderate and low levels in STS found in our study, may seem as a paradox concerning the interpretation of ProQoL. To explain this, the higher the level of CS is, the better the ProQoL, while the higher the level of BO and STS, the worse the ProQoL is. However, health professionals exposed to COVID-19 experienced both negative and positive psychological outcomes simultaneously. This contradiction could be explained by the fact that, during the coronavirus pandemic, health professionals were feeling exhausted from the workload and saddened by the unpredictable number of deaths but, at the same, they were satisfied with the services toward their patients, aiming to improve their health. Our findings are almost consistent with a study conducted by Cuartero-Castañer in the United States. 14 However, other studies in Spain, Italy and China19,24,48,49 showed that health professionals scored higher levels in the same dimensions. This could partly be explained by the early outbreak as well as the impact of COVID-19 in the aforementioned countries.
Moreover, several studies revealed that health professionals, who are providing care to COVID-19 patients in need of immediate admission and are on the frontline facing large numbers of deaths and managing high-risk procedures, were found to be more likely to report higher levels in all CS, BO and STS.50-52 Additionally, a study conducted in Greece reported that the prevalence of post-traumatic stress symptoms was high mainly in health professionals who are greatly exposed to the virus. 53 Furthermore, various international studies demonstrated an increase in negative psychological consequences relating to working conditions during the COVID-19 outbreak.54-56
Despite the fact that women are prone to develop depression, prior to 40 and during the pandemic, 12 our results showed high levels of CS in female health professionals. This finding is in accordance with 2 studies conducted by Dosil et al. 57 and Ozamiz-Etxebarria et al. in Spain, 58 however the latter only focused on the general population. This was an expected result given the social role that women have with respect to caregiving.24,59 Another similar finding is that health professionals indicate high levels of CS when they have long work experience. 60
An association between health professionals’ occupational stress and BO and STS has also been demonstrated by other researchers. This is a finding negatively impacting their ProQoL. There are numerous studies reporting that the pandemic exposes health professionals not only to biological factors, but also to occupational, social and other factors, thus making occupational stress a major public health issue.61,62 Various studies conducted prior to the COVID-19 outbreak, also reported that health professionals are prone to high levels of stress and consequently, to low levels of ProQoL.63,64
There are various measures which could be implemented in response to the health crisis such as, mobilizing the existing workforce, changing working patterns, calling on volunteers and non-governmental entities and recruiting health professionals. 65 Protecting their mental health and well-being through adequate training could also help in maintaining the health workforce and especially those who suffer from work exhaustion or psychological distress. Shorter work schedules, regular rest periods and rotating shifts for staff who work in high-risk environments can be considered. 66 Furthermore, support from colleagues and supervisors, clear communication of directives and precautionary measures can reduce psychiatric symptoms. 67
Apart from the above-mentioned managerial measures, mindfulness-based therapy could cultivate compassion and foster psychological resilience. This could ultimately enable professionals to cope with suffering and death and prevent burnout and work stress. 68 Additionally, online psychological interventions such as cognitive behavior therapy (CBT), enhancement of team spirit and praise of valuable outcomes could also work toward supporting and strengthening HPs well-being.66,69
Limitations
Evidence that has emerged from this study should be interpreted in light of some limitations. First, the data has been obtained from a cross-sectional design study, which did not determine the causality of the variables analyzed. Prospective longitudinal studies might inform on causal long-term effects of COVID-19 on health professionals. Moreover, a convenient sample was used in order to collect data in a timely manner regarding the COVID-19 outbreak. This makes it difficult to generalize results to the broader population of health professionals in Greece, despite the fact that participants are working in one of the largest general hospitals and COVID-19 reference units in the country. Thus, further investigations in larger scale studies should be performed to provide more representative findings. Also, the subjectivity and bias of the sample responses should be taken into consideration, due to the fact that the questionnaire was self-administered.
Conclusions
During the COVID-19 pandemic, professional quality of life and occupational stress of health professionals of the specific hospital seemed to be moderate and are associated with their socio-demographic and occupational characteristics. The higher the occupational stress, the higher the burnout and secondary traumatic stress. Our findings brought to light the necessity of decision makers’ immediate interventions aiming to support health professionals’ quality of life and strengthen the capacity of the healthcare system. Health professionals’ continuing education initiatives as well as strategies for coping with stress and psychological resilience, should be included in health systems’ internal control assessments. Furthermore, it would be useful to conduct in-depth research through face-to-face interviews with HPs and focus groups, with the aim to examine their needs and provide personalized and integrated support in times of crisis. Despite the psychological burden that the COVID-19 pandemic has brought to Greek health professionals, it is acknowledged that they remain the most valuable and compassionate resource addressing the COVID-19 outbreak.
Supplemental Material
sj-docx-1-his-10.1177_11786329221096042 – Supplemental material for Professional Quality of Life and Occupational Stress in Healthcare Professionals During the COVID-19 Pandemic in Greece
Supplemental material, sj-docx-1-his-10.1177_11786329221096042 for Professional Quality of Life and Occupational Stress in Healthcare Professionals During the COVID-19 Pandemic in Greece by Dimitra Latsou, Fevronia-Maria Bolosi, Lorena Androutsou and Mary Geitona in Health Services Insights
Footnotes
Acknowledgements
We want to express our thanks to the staff and office of the General Hospital of Athens “Evangelismos,” for their support throughout this study.
Author Contributions
All authors contributed and provided input in the study design and data collection, analysis of the results and the writing of the manuscript.
Disclaimer
The information and views set out in this article are those of the author and do not necessarily reflect the official opinion of the European Commission.
Ethical Approval/Patient Consent
The study was approved by the Scientific Council of the “Evangelismos” hospital (protocol number 478/15.10.2020). Health professionals were informed about the aim of the study and their agreement for participation was requested, providing an informed verbal consent. The survey was voluntary and anonymous, with a withdrawal option at any stage. The questionnaires were collected in a closed envelope submitted to the secretariat of each department.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.