
Abstract
Background:
In March 2020, COVID-19 entered South Africa, resulting in 2.9 million cases, the country took preventative and precautionary measures to control the spread of COVID-19 infection. These measures limited population mobility especially for migrant women living with HIV (WLWH) and the provision of PMTCT services. The purpose of this research was to explore the challenges of the COVID-19 pandemic on PMTCT provision by healthcare providers and understand what strategies could be implemented with lifelong antiretroviral therapy (ART) for migrants to better manage the program.
Methods:
Twelve in-depth interviews were conducted with healthcare providers across city and provincial levels on how the changes to the healthcare system with COVID-19 affected highly mobile patients’ adherence and utilization of PMTCT services. A thematic content analysis was used for emerging themes and guided by The Utilization of PMTCT Services conceptual framework.
Results:
Five main themes emerged: (1) Facilitators and barriers to adherence, which included the need for multi-month dispensing for the long term supply of antiretrovirals (ARVs) and the fear of contracting COVID-19 at the hospital that disrupted patients’ continuum of care; (2) Healthcare providers work environment, where participants felt overwhelmed with the high patient demand and the lack of infrastructural resources to follow social distancing protocols; (3) Financial challenges and opportunity costs, PMTCT proved difficult for migrants due to border closures and documentation required to receive care, this resulted in treatment interruption and left many unable to receive support at the facility due to capacity restrictions; (4) Interpersonal interactions, mistreatment, and xenophobic attitudes existed toward the migrant HIV population; and (5) “Program sustainability” revealed three key areas for strengthening: longer duration of time allocated with counseling for same-day initiation, the increased use of technology, and translation services for migrants.
Conclusions:
It is important to take what was learned during the pandemic and integrate it into routine service delivery, which includes long-term medication supply to reduce risk with multiple visits to collect medication, and the use of technology to alleviate the high-burden of patient demand. Healthcare policies that work toward inclusion and sustainability for migrants are needed to improve the integration of safer and practical methods of PMTCT provision into health systems.
Background
The COVID-19 pandemic has resulted in high mortality for South Africa’s (SA) HIV population, resulting in an overwhelming 550 000 deaths in less than six months alone since its first confirmed positive case in March 2020.1-3 A large proportion of the cases came from Gauteng province, home to the largest migrant population in which rests the city of Johannesburg—full of vast population movements from internal (individuals moving intraregionally or interprovincially) and cross-border (individuals moving between neighboring countries) migration. 4 Most migrants (60%) are located in the peripheral and urban areas of Johannesburg, 32% of which are women, and cross-border migrants that do not access healthcare for fear of being asked for official documentation and deportation.4,5 The pandemic has added a layer to the pre-existent structural discrimination that has largely influenced health-seeking behaviors and social exclusion of both internal and cross-border migrant women within healthcare facilities.6,7 Migrant women utilizing maternal healthcare and HIV services face many of the barriers and challenges that disrupt their ability to adhere to medication and treatment which requires long-term discipline.8,9
The impact of COVID-19 on migrants access and utilization of the healthcare systems during the pandemic is little understood. 10 The increased mobility across long distances resulted in significant risks for migrants accessing healthcare services and a call for government own COVID-19 prevention strategies. 10 Though the SA constitution indicates the right to access healthcare for all who live in SA, and the national health policy provides for free primary healthcare access for all in the country with no mention of nationality and legal status, interpretation of the legislation is less inclusive in practice.11,12
Healthcare service cutbacks for provision of counseling and support to help both internal and cross-border migrant women living with HIV (WLWH) has also resulted in adherence challenges. 12 Border closures during lockdown challenged the second 90 (90% of people living with HIV who know their status being on antiretroviral therapy) with the loss to follow-up (LTFU) because mobile women remained difficult to trace when attending different facilities to access care.2,11,12 Research also suggests ill treatment by healthcare providers can impact access to care for foreign nationals, such as the phenomenon of medical xenophobia (MX) in the contemporary SA public health system. 13 MX refers to the negative attitudes and practices of healthcare professionals toward migrants and refugees based purely on their identity as a non-South African, which impacts the services that are provided for and accessed by patients. 13 Studies point out examples of MX which include declining non-nationals entrance into a healthcare facility and healthcare providers placing non-nationals in a longer queue. 14 This care is often not the best care available due to the presumptions that there is an increased burden on the SA public healthcare system causing stigma and fear of the spread of COVID-19 with migrants. 14
Research shows that both internal and cross border migrants during COVID-19 faced challenges in access and utilization of healthcare services. 5 Despite existing evidence on the diverse population movements within SA, the public healthcare system, on which majority of the population relies, has struggled to integrate mobility or migration.4,15
PMTCT lifelong treatment
PMTCT is a clear example of a maternal and child health program that was offered across SA since 2001. 16 The PMTCT cascade represents a complex system of sequential, interdependent steps that WLWH navigate as healthcare users to receive appropriate care and treatment for themselves and their newborns. 17 A vital component that was not traditionally part of the PMTCT program but was later added was the provision of lifelong ART services for women by the World Health Organization (WHO) consolidated guidelines. 18 Thus, the PMTCT cascade of care does not end at delivery of the baby as there is a need for long term follow-up. PMTCT using ART is a proven, efficacious intervention, and can reduce vertical HIV transmission to less than 2%. 17
In January 2015, Rahima Moosa Mother and Child Hospital (RMMCH) 1 located in Johannesburg was the first public hospital to implement PMTCT lifelong treatment. 18 RMMCH reported 64% of their maternal population accessing maternal newborn child health services were recorded as non-citizens of SA and are a part of the challenging public health service provision. 18 Women who attended ANC outside of RMMCH, were often untested for HIV and delivered their babies at the hospital without an early PMTCT intervention.
The aim of this research was to; (1) explore the challenges of the COVID-19 pandemic on PMTCT provision by healthcare providers to further investigate the encounter between service providers and users and; (2) understand what strategies could be implemented with COVID-19 to address challenges with lifelong ART for migrants to better manage the program.
Methods
Research design
This qualitative study included in-depth interviews (IDIs) conducted with healthcare providers across different units of RMMCH that provided PMTCT services or interacted with service users, specifically migrant women. IDIs were aimed to investigate healthcare providers perceptions on challenges of the COVID-19 pandemic on PMTCT provision and understand what strategies could be implemented with lifelong ART for the highly mobile population.
This design was chosen to stimulate interaction and discussion, creating an opportunity for open input on the challenges and strategies related to the Utilization of PMTCT Services conceptual framework during the pandemic based on participants’ experiences. 19
Conceptual framework
The Utilization of PMTCT Services conceptual framework (Figure 1) was used to explore healthcare providers’ experiences of providing PMTCT services to highly mobile users during the COVID-19 pandemic. Utilization is defined as the healthcare users’ experiences and perceptions of their interactions with the PMTCT program components (i.e., healthcare providers’ treatment of them, and interactions with any hospital staff from point of entry). This includes their perceptions regarding accessibility of the service as well as adherence of their patients to the PMTCT lifelong care. Utilization is made up of (1) adherence issues to the program and; (2) access which comprised of 4 dimensions: availability; affordability; acceptability; adaptability. 20 Adherence is conceptualized as the long-term ability for these women to follow the PMTCT program which includes the ability to take medication routinely, not miss dosages, and attend follow-up appointments. Accessibility is a component of utilization that refers to the equality and equity of care in the healthcare facilities in which these women utilize PMTCT, no matter their nationality and legal status.18,20 Availability dissects the factors such as the range of maternal, newborn child health services (MNCH)/PMTCT services relative to the need that is, hours of operation, ARV supply, willingness of service provider, and information provision.18,20 Affordability refers to costs of PMTCT services and opportunity costs (time a woman can afford to take time from work to get to the hospital), including transport costs, medicine charges, diagnostic tests, special diets, and childcare costs.18,20 Acceptability refers to whether the expectations of the women are met, which includes age, gender, race, ethnicity of provider, decision making, and whether culturally appropriate service are offered.18,20 Acceptability also includes the individuals’ non-medical expectations of healthcare providers’ treatment of dignity and respect of their culture.18,20 Adaptability, however, refers to the sustainability and scalability for the PMTCT program for all women, no matter nationality and legal status.18,20
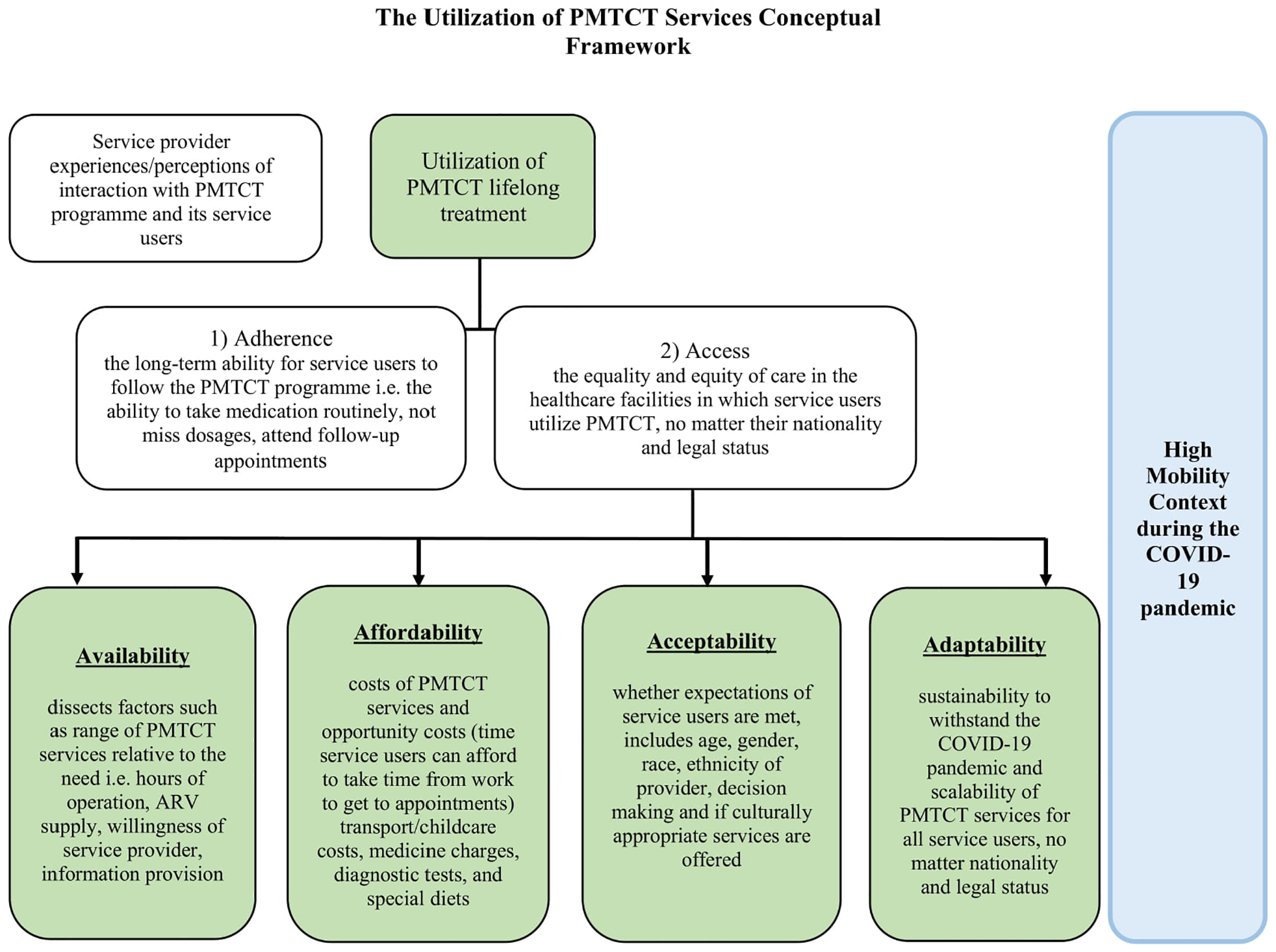
The Utilization of PMTCT Services Conceptual Framework.
Procedure and data collection
IDIs were conducted in the privacy of participants offices at RMMCH or on an audio recording platform (Zoom) where consent was provided due to capacity restrictions of COVID-19. Participants were recruited through purposive sampling and had to meet the following inclusion criteria: had to be 18 years or older; a healthcare provider at RMMCH; works in the public healthcare sector at district, provincial, or national level and; had to have contact with service users on PMTCT since its initiation in 2015 at RMMCH. Participants were not excluded based on race or language. Participants were only excluded if they were newly employed with no previous interaction with patients on PMTCT.
A semi-structured interview guide was used that comprised of the following main topics: (1) adherence, (2) access, (3) availability, (4) affordability, (5) acceptability, and (6) adaptability. For example, some questions asked were, “What documents are needed to utilize PMTCT at RMMCH for non-national women? What ways would you improve the services made available for PMTCT at RMMCH? Specifically for mobile populations? What strategies would you implement at RMMCH to improve PMTCT use? Do you think mobility has an effect on a women’s uptake/adherence with the PMTCT lifelong treatment program? Why?”
The guide was developed by the researchers, which consisted of an HIV medical specialist, migration, and public health epidemiologists who had experience in this field. The topics in the interview guide were structured in a logical and constructive way and were based on findings from literature review and information on the framework. Participants were recruited consecutively until data saturation occurred where the principal investigator and research team were no longer hearing or seeing new information emerging from the data. To establish rapport, interviews started with demographic questions, then moved to challenging topics (i.e. any mistreatment toward patients) with open-ended questions.
Data analysis
IDIs were audio recorded and transcribed verbatim, all transcripts were anonymized but roles and perspectives that were important to answering the question. A thematic content analysis was used to analyze the data using NVivo QSR 12 (QSR International Pty Ltd., 2018). The round of open coding was completed by two authors independent of each other, after which the codes were discussed and re-coded until consensus was reached. 19 A triangulation technique was used to crosscheck and validate IDIs and ensured the credibility of the findings amongst the research team that reviewed the findings from transcription along with literature journaling for social cues, reflection, and continuous refinement to hone the most prominent themes and relationships. 19 Descriptive statistics were reported for demographics of the participants including proportions for categorical variables using Stata 14.
Ethical considerations
The Human Research Ethics Committee (HREC) at the University of Witwatersrand, South Africa approved this study in 2019. Provincial clearance was obtained by Gauteng Province and The National Health Research Database (NHRD No: GP_201912_003) and the City of Johannesburg. Authorization from RMMCH was granted to conduct the study in Coronationville (HREC Protocol No: M190816 MED19-07-084). Participants gave verbal informed consent before the start of the IDI was audio recorded.
Results
Participants
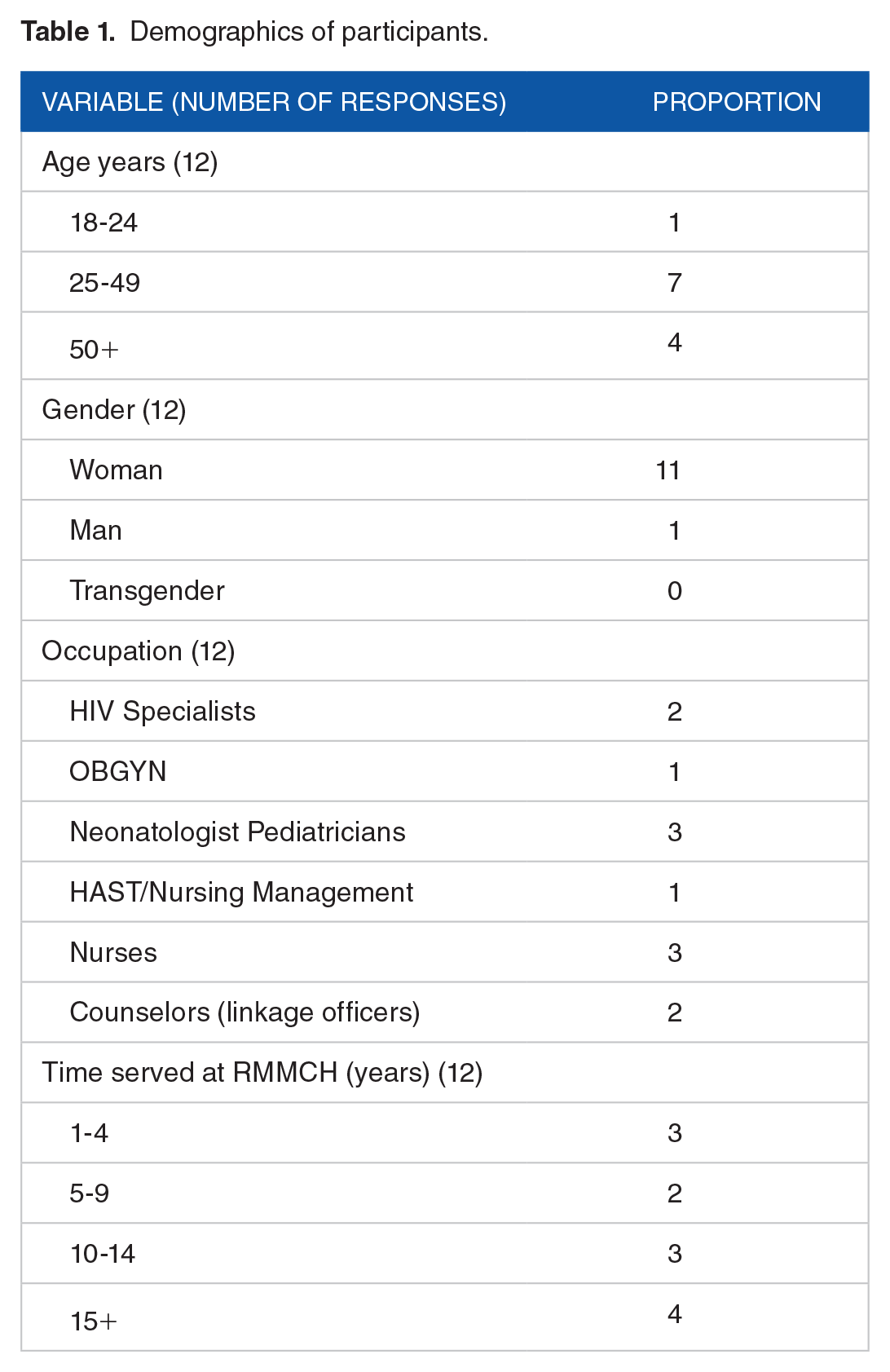
The IDIs included 12 participants both on city and the National Department of Health (NDoH) provincial levels (female: 92%) with a mean age of 43 years (range 25-49 years) across the neonatal intensive care unit (ICU), post/antenatal clinic (ANC), Obstetrician-Gynecologists (OBGYN), and HIV/AIDS, STIs and TB (HAST)/nursing management units, four of which served 15 years or more at RMMCH (Table 1). Management was involved with the provincial PMTCT committee which included training and provincial guidelines. IDIs were 45 to 52 minutes.
Demographics of participants.
Themes
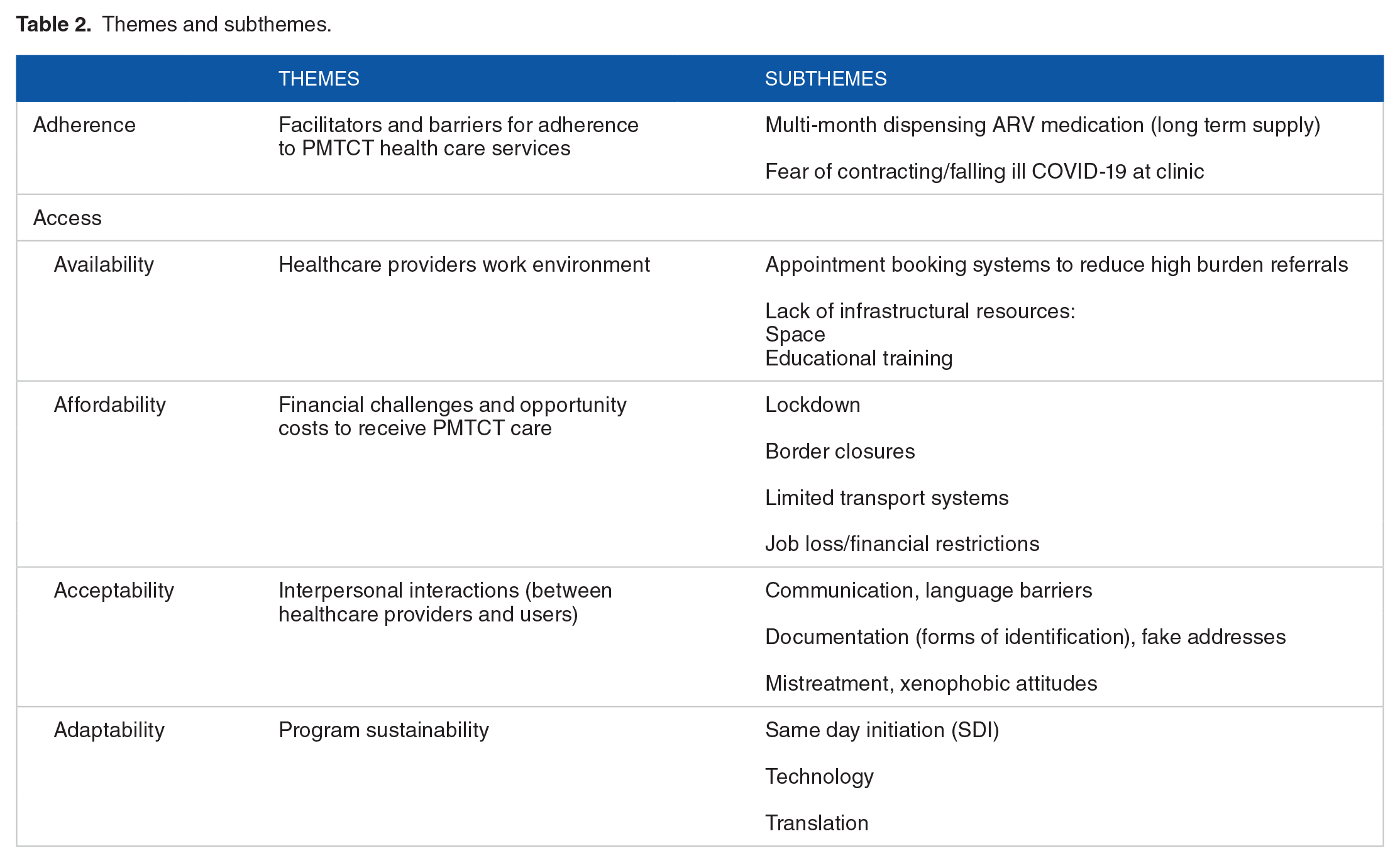
The Utilization of PMTCT framework which included (1) adherence and (2) the four dimensions of access; availability, affordability, acceptability, and adaptability was used to organize sub-themes that derived from IDIs (Table 2).
Themes and subthemes.
Adherence: Facilitators and barriers for adherence to PMTCT health care services
The adherence theme was composed of the subthemes “multi-month dispensing (MMD),” and “fear.”
Multi-month dispensing (MMD)
The pandemic increased strain on both healthcare providers and users, who were unable to access the hospital as they regularly would which led to disruption and higher risk of LTFU. A Neonatologist indicated that the healthcare system had not been informed of the changes with COVID-19 in respect to dispensing ARVs for migrant mothers that are highly mobile, “The problem is the first year of the child’s life, it is good to go because every time the child goes to the clinic for an immunization, then the mom can get the medication and get a viral load (VL) done in the month, but it is after that everything just falls to pieces in the long-term now with COVID-19. It’s like now the mom is not going to go to the clinic for the child and then you can’t give her the medication and she’s moving around. I think we really need to consider this with long-term care” [IDI 10].
Counselors elaborated on challenges that were seen regularly with adherence and VL completion at the ANC with women that move around frequently. Strategies to help address this was discussed, “I feel like with those highly mobile patients we should be allowed to give them treatment that isn’t just one month, but a longer period so that at least they have it. If we can do this during COVID-19 times then I don’t see why two or three months of medication, or six months and a VL can’t be done” [IDI 8].
Therefore, it’s not that multi-month medication dispensing to ease access of ARVs for mobile patients cannot be done, the pandemic of COVID-19 increased the dire need to do so and demonstrated that it was possible.
Fear
Particularly migrant women; feared the pandemic and falling ill; were more often turned away from healthcare facilities and; were unable to obtain their medication or utilize services. A pediatrician explained that there are already time constraints to conduct thorough counseling for migrant women that are virally unsuppressed during COVID-19, “Patients were scared to come because they thought-I am going to come to the hospital and get COVID-19, so then they wouldn’t come for their appointments. The ones that aren’t virally suppressed, to be honest with you, we will get the history from them but we don’t always get the time to counsel in detail [. . .]. We might ask what happened, the mom will say for example, during COVID-19, they told her she had to be quarantined and she couldn’t go and get her medication. She stopped for two months, and you don’t blame her because there were stories that some clinics were turning foreigners away, so that we can understand” [IDI 11].
Counselors expressed that cross-border migrant patients voiced their concerns about the care received from other staff, left feeling scared and neglected. A counselor described that she took it upon herself to ensure that cross-border migrants feel comfortable, “I speak to them and make them feel welcomed. Sometimes they are scared or a nurse has rubbed them the wrong way- they shout and yell. We talk to them and hear their problems but it is so overwhelming that we don’t get much time” [IDI 9].
Access
Availability: Healthcare providers work environment
Participants discussed facilitators and barriers of COVID-19 including; appointment booking systems, the lack of space, and educational training.
Appointment booking systems
RMMCH had an increased burden of patient referrals from outside their catchment area before the COVID-19 pandemic. Doctors expressed frustration with the healthcare system disruptions and clinic closures due to increased COVID-19 cases,
“I think we are going to see the effect of these first, second, third waves, and the fall-out from maternal cases because of COVID. I have had rubbish like the other day, they said they are going to close the one clinic which delivers babies in our area and just send all the patients to us because they had one positive patient, two weeks ago in their clinic. We are going to hit problems like that and it is going to impact on care. We will lose babies and mothers because of it.”
COVID-19 placed pressure on the healthcare facility to make changes in an efficient and effective manner to cope with patient demand. Implementation of a booking system that respected social distancing, reduced the overwhelming number of HIV pregnant women served daily. An HIV Specialist highlighted the positive outcome due to the pandemic, “At the moment, we have about 130 women every Monday at the clinic. We have managed to alleviate two hundred deliveries because you can’t even manage everyone to be in our booking system. Somehow to achieve just getting a booking system was massive and COVID-19 thankfully helped us with that because we were able to wave the COVID-19 banner and suddenly it happened. I think the clinic itself is a much more happier place” [IDI 2].
RMMCH serves a 40% migrant population and had a good reputation for not turning people away upon arrival to ensure the patient received care, “Some clinics refuse to give Road to Health cards to foreigners. In that case, we try and work with the clinic or try to get one from here, it all depends on where they were born” [IDI 11]. However, with the impact of COVID-19, it caused changes to their booking system and provision of PMTCT, “We have a minimal amount of patients as first visits so what we introduced recently since the beginning of COVID is that all our patients must have made an appointment at the facility they attended before, that facility makes an appointment with our ANC for the patient to come in. The patient cannot just arrive without an appointment” [IDI 2].
This increased difficulty for women that do not have documentation and are non-SA citizens. They were left to navigate a complex healthcare system and needed to be referred by a local clinic in order to access care.
Space
Healthcare providers described that COVID-19 precautions placed a burden on infrastructural resources for program components like breastfeeding, “It makes it a lot harder in our unit just simply because we’ve got a lot of numbers and we like the mothers to be there to breastfeed, so the risk for them was higher because they have to pump in an expressing room and we couldn’t have as many people at one time. Also having so many people in the ward, we reached a lot of these shortages with alcohol sanitizer that could have resulted in more infection” [IDI 3].
Educational training
Educational training that was previously conducted with large numbers of nursing staff had to be stopped during the pandemic because of risk exposure to COVID-19. Frontline nurses became overwhelmed and unfocused with PMTCT components, “Now with COVID, [. . .] these guidelines had the two month supply of medication, it’s not something that’s new, since 2015 it has been in the guideline. It is just not implemented as well as it should be. Nurses are concerned about some things with the PMTCT service but they are not always ensuring that mothers get discharged with their medication. They need to be micromanaged to a certain degree” [IDI 4].
Management reinforced that though a pandemic is occurring, it was inexcusable to not follow pre-existing guidelines that were implemented for PMTCT.
Affordability: Financial challenges and opportunity costs to receive PMTCT care
Participants expressed that lockdown caused border closures and limited transport, impacting many internal and cross-border migrant patients, who lost their jobs and were unable to endure any opportunity costs to commute to receive treatment.
Lockdown, limited transport, and finances
Transportation during provincial lockdown across SA was a major concern for mobile women, a nurse provided insight, “with COVID, you couldn’t sit in a taxi with many people and it was a lot harder for patients to come because they didn’t have the same access that they previously had. If someone had their own transport or had a family member that could transport them, then they would come” [IDI 11].
An obstetrician indicated that duplication of appointments occurred frequently during the first wave and that migrants could not take time off work or travel from their home countries to keep visiting the facilities repeatedly, “At one point, when we were initiating a lot then we would initiate the patient, treat the patient and then refer them out to carry on treatment at the local clinic. Then they said no, the patient must collect their treatment at the local clinic and come into us just for antenatal care, which is a huge duplication of visits for these women. I think they must just get their treatment with us while they are pregnant, otherwise it is extra visits for them. The problem is that they don’t carry any kind of information and the majority has no idea what drugs they are on [. . .] and they have no documentation [. . .] clinics don’t write down which treatment they are on [. . .], that is very poor. They don’t put any of the recent bloods or anything so you end up repeating bloods again” [IDI 2].
Acceptability: Interpersonal interactions
Participants discussed facilitators and barriers of COVID-19 including; communication, documentation, and mistreatment.
Communication
Protective masks created a barrier for facial expressions and the ability to effectively communicate that could have been prevented otherwise if doctors had more time allocated to migrant patients who required more attention due to language barriers. A participant explained the interaction she had with a woman from Malawi, which provided an example of the increase difficulty with communication due to masks and the inability to speak the local language, “There was a patient who had a hearing difficulty and didn’t tell us. Only after some time, we realized that she wasn’t understanding any of the counselling because she could only lip read. She would nod and then I would be upset because I was thinking, I explained this to you, why aren’t you understanding [. . .]. She had a unsuppressed VL. I wonder if that was more a function of the fact that no doctors ever took time to talk to her and find out what her disability was. Because once we started talking to her, I got her brother’s number [. . .], you often go very quickly and you miss something so important. With COVID, I think it just made it harder to consult patients and because you have a lot of people on the ward round, you feel stressed when you’ve got your mask on” [IDI 11].
Particularly language barriers contributed to communication gaps for cross-border migrant women that didn’t speak any of the local South African languages, “We have a significant amount of foreign patients. The foreign patients are often from Zimbabwe [and] Malawi. We get a lot of patients speaking Chichewa and it is very difficult to actually communicate about the testing, the result, the feeding choice, and the adherence. If the patients can speak English, they are usually South African” [IDI 3].
The barrier of language contributed to patient misunderstanding the importance of why the healthcare providers make the recommendations they do.
Documentation
The hospital remained reputable for providing care to those outside their catchment area, however RMMCH still had to obey laws in SA that required documentation of non-nationals in order to access specific services, “We don’t dismiss patients who are not South African. The only time we will ask is when the premature babies require oxygen at home and that is not our law. The company wants us to provide a SA ID [identification] and a residential address, and work permits are not adequate, you have to be a SA citizen. A large proportion of patients are from other countries and we know this because when you’re counselling, you ask the persons’ home language, it’s often a minority language that’s Chichewa or Shangaan from Zimbabwe. When we order things like home oxygen for babies who have a chronic disease, you cannot give foreign patients. They have to have their papers, either asylum seeker papers or permanent residency [. . .]” [IDI 11].
Turns out if the cross-border migrant does not have these documents, which happens often, then the child must stay at the hospital, “Unfortunately then the child stays with us. We keep the child and this often happens, you will see children that are five months old, some with oxygen and we just hope that they grow and get off the oxygen” [IDI 10].
Nurses elaborated on the issue that “foreigners” go to extremes and would lie about their addresses to utilize PMTCT, “It’s foreigners [who] have been turned away so as a result, all of them are flocking to us. Then there is this thing about addresses that they tell you they are living around the area and we don’t turn anybody away. If they need our services we are able to give it [. . .] that is the biggest issue we are facing. They use fake addresses, fake IDs and sometimes they don’t have an ID. They are illegally in the country and use the sisters’ or aunts’ ID. It’s creating a problem in Gauteng. We don’t turn away any patient but other hospitals they do, even if the patient is bleeding or is in labour” [IDI 6].
Mistreatment
Poor staff attitudes and behavior existed toward cross-border migrants, “I mean I hear it sometimes, that patients feel they are treated abruptly [. . .] I have seen people being made fun of. I know people complain and I know that there are issues. Yes they have a choice but it appears a lot of treatment is not appreciated [. . .] and it causes a lot of stigmatization if a pregnant women or mother refuses treatment, that is one thing that can make patients become very isolated in a ward and kind of intolerated by nurses and doctors” [IDI 1].
Participants reported they have seen/heard a “lack of respect” in the work environment,
[IDI 8] “We have a lot of patients outside our catchment area, most of them are non-nationals moving around and their comfortability-it differentiates. You will be comfortable with someone who respects you. I am a healthcare worker but my attitude needs to say I am a healthcare worker, it does not necessarily mean to say that just because I am a healthcare worker I am going to mistreat you too. I think it all needs to go with respect, if I respect you as the patient and communicate with you in a proper way then it is possible” [IDI 8].
Nurses expressed frustration with the gaps in the healthcare system and used rhetoric toward migrants which included “causing drainage of hospital resources” from “those who do not belong there,” “I think it needs to become a standardized thing so patients need to know that I must either have my ID or passport and if you get strict about it then at some point, those who do not have, are the ones that need to be picked up and shipped back to wherever, because everyone should have some form of documentation. We have been very laxed in terms of checking who is around and which patients are there. I don’t want to deny care to anyone but it’s not just with healthcare services, it’s everywhere. If someone can’t produce the documentation then they shouldn’t be here, it just drains everything” [IDI 2].
Differences in service provision specifically toward cross-border migrants in comparison to local citizens was discussed with participants, “As far as I understand, yes- but they may be treated differently and we have to be cognisant of that. A South African patient may be treated better than a non-South African patient because of other people’s xenophobia or the stigma they have against patients [. . .] I have seen it quite strongly where I have heard people say to patients why didn’t you give this patient this medication. I haven’t seen it as strongly here but there is that feeling that patients from another country may be treated bad” [IDI 11].
Adaptability: Program sustainability
Participants discussed facilitators and barriers of program sustainability to withstand the COVID-19 pandemic for highly mobile migrant users, no matter nationality and legal status which included SDI, technology, and translation.
Same-Day Initiation (SDI)
There was an alarming need for migrant patients to spend more time with counselors because ART initiation occurred at the same time the patients’ positive HIV status is disclosed to them. Highly mobile WLWH often struggle to return, decreasing retention in PMTCT care. An OBGYN emphasized, “I think there needs to be more of a structed counselling approach, maybe some sort of programme that they work through on the visits that they come for, you can’t add in any extra visits because its economically a problem as it is for these patients. I think that the linkage is poor between us and the clinics. I don’t feel that we have a 100% good relationship, that when we are seeing them out I often feel that we are putting them out into the wild yonder. I don’t really get that strong feeling that they are going to the clinics” [IDI 2].
Technology
Healthcare providers were tested with immense virtual changes to maintain safety, “Everything became online and that was a massive change. I think it was a lot of adaptation. I think everyone did different things to try and still connect” [IDI 11].
The referral system between clinics benefited from technology, where counselors could follow-up patients referred out from the hospital to their regional clinics. “As a region, we have a group chat. I call a clinic, then say, can I please speak to one counsellor and then tell them the patient is referred from RMMCH and that this patient will be coming, she didn’t have her medication, can you please give it to her” [IDI 8, Linkage officer]. Many highly mobile patients missed their follow-up appointments, and still remain a challenge due to the multiple/incorrect contact details provided. Participants suggested having an integrated system to coordinate with other countries for better tracking cross-border migrants could improve LTFU, “If we had this system, it would definitely change things, not just for PMTCT but for everything. You could link for instance, this child was admitted two months ago at a different hospital, their x-rays, blood results, pharmacy scripts, all to one number. From a foreigner point of view, that would require some major coordination with other countries, that if they travel with their booklets and actually write down what they are receiving. Also with patients that thought maybe they were going to go back and fetch their treatment and then something prevents them travelling, so they don’t” [IDI 2].
In addition, staff believed reducing long queues and waiting times and having different access points in which migrants could pick up their ARVs was believed to increase adherence, “I think where patients can pick up their medication from a private pharmacy and don’t have to sit in long queues, those are stable. I definitely think that would probably help with adherence. I think the fact that there isn’t really good paper trails and it is very difficult to see what people are on, and whether it is their disease, that is what hinders the care. I think it’s a reasonable PMTCT programme but it has a bit of a way to go in order to achieve its targets” [IDI 2].
Translation
Participants believed that many migrant patients on PMTCT have challenges when it comes to taking ownership over their health due to language barriers and the inability to communicate effectively. A doctor explained that when this occurred, they relied on other healthcare staff to assist with translation, “We have learnt over the years that we need to ask them if they have enough medication, if they are running out, or other stuff they are on so we can prescribe and get it, so I think that is a limitation- that some of them are not empowered enough to say what they need. We try to get an interpreter, if we can’t get a nurse in the ward to interpret for us because the language barrier may be significant, then we send them to the HIV clinic where there are counsellors, they then counsel the mothers and try to explain and intervene” [IDI 3].
To overcome language barriers unique to migrants, the Google translation application was used to assist with mothers who did not speak any of the local languages, “I worry that I am going to miss something because I cannot communicate properly with them. Things like Google Translate certainly have helped here and there but certainly [is] not the same as just trying to talk to someone properly and hear their story” [IDI 2].
Discussion
Main findings
In this study, we aimed to explore the barriers of a pandemic on PMTCT provision by healthcare staff to understand what strategies could be implemented with COVID-19 to address challenges with adherence to ART for the highly mobile population to better manage the program.
Cross-border migrant women were reported to undergo many healthcare user challenges for PMTCT during COVID-19 due to the documentation required to access care and navigate a more complex healthcare system, now amplified by lockdown and border closures.21,22 The duplication of appointments during the first wave of COVID-19 severely impacted migrants and their mobility leaving many unable to afford opportunity costs to travel from their origin country/province because of border closures and overall maintain their PMTCT care.23,24
The pandemic increased the dire need for multi-month medication dispensing to ease access of ARVs for highly mobile patients, and demonstrated that it was possible. COVID-19 has shone light to an already overburdened healthcare facility and the existing gaps of a network of referral clinics across Gauteng province. Barriers of documentation, missing reports of VLs, and PCR test results have called for a synchronized plan with the South African government and the NDoH.
Migrant women will only build self-capacity if their trust in the healthcare system is reassured through alleviating stressors such as asylum papers and providing clear and concise messaging- including the importance of adherence to ART while breastfeeding. Education made available in different languages can serve mothers that do not speak the local languages for better understanding of the importance of adherence and risks of non-adherence to their baby, even after delivery.25,26
RMMCH has provided PMTCT for 40% of highly mobile patients outside the catchment area. Stretching its resources thin proved to be challenging while enduring the pandemic, which led to poor behavior of staff from the overwhelming patient demand and everchanging work climate of COVID-19. 27 Healthcare providers inability to spend sufficient time counseling and build rapport with migrants who need particular attention due to language barriers, increased the risk of LTFU. Unfortunately, stigma and mistreatment still exists with some healthcare providers toward the migrant HIV population. Immunocompromised HIV migrants remain vulnerable, often feared falling ill from COVID-19, and were unable to receive support at the facility due to capacity restrictions. 10
Research has emphasized PMTCT lifelong treatment management for patients remains difficult because of inconsistent delivery across clinical departments of counseling and support services for SDI of treatment.18,28 Strengthening PMTCT must occur on different levels, while many service providers have been known to place the burden of responsibility on the patient, negotiating the patients’ health beliefs and values to fit a pre-existing healthcare structure that may often ignore cultural sensitivity. 29
Therefore, the success of the PMTCT program is critical for reducing maternal and child mortality and morbidity rates, reducing HIV risk for children, and overall building health awareness and empowerment of women to take control of their health decision-making. 6
Recommendations
The NDoH PMTCT guidelines do not address the complexities of mobility and healthcare access in high mobility contexts. 8 Better understanding could reduce its challenge of reducing the mother to child transmission rate to less than 5%. 30 Particularly for non-national women who are seen as a politically weak group that has not gained visibility on SA’s health policy agenda, and are at an elevated risk of facing inequalities and unfair treatment by healthcare providers when utilizing PMTCT healthcare services across Johannesburg. 31 There is a lack of understanding about how provision of PMTCT care in the healthcare environment can be strengthened for migrant women to better support their individualized needs.
COVID-19 alleviated over 200 deliveries in six months for RMMCH with restructuring the booking system of patients. Strategies to strengthen the PMTCT program gaps with service provision include an integrated electronic database of records or travel book that cross-border migrants could carry with them. These can provide access to patient history within different regions, provinces, or in another South African Development Community (SADC) country and possibly combat lost PCR tests/records, address pharmacy scripts for dispensing and pick-up of ARVs, reduce duplication of appointments and costs for patients to travel, and the demand of healthcare providers.
COVID-19 changed the way staff worked and demonstrated that immense changes could be implemented through technology to alleviate issues with patient demands which included, chatgroups and SMS reminders. Constant and consistent quality improvement to the database at the hospital should be ongoing to reduce LTFU and poor adherence.
To address poor healthcare provider behavior and attitudes, mental health support through Employee Assistance programming should be provided which includes, training, values clarification workshops, and team building exercises that can be conducted by a third party to mediate management and frontline healthcare providers. 27 There are larger systemic issues at play with xenophobia in the SA healthcare system that need to be addressed through mentoring and interdisciplinary training.13,18
In comparison to five years ago, a gap for structured counseling remains with PMTCT programming at RMMCH.18 The clinical flow with counselors must allocate time for patients, especially with the implementation of SDI.21,32 Many women are initiated onto ART but there still remains a lack of understanding the importance of adherence after the birth of the baby, especially during the course of breastfeeding.17,18
A shuttle or transport service with different pick-up points could be provided by NDoH and RMMCH for highly mobile patients to ease the financial costs of traveling that was amplified for migrants, specifically those with multiple appointments during the pandemic. 24
Health education was delivered primarily in English, which acted as a double-sword, providers felt that foreigners who do not speak the language, lose out on education. There is a potential to translate and distribute information, education, and communicative (IEC) materials to the larger migrant population attending RMMCH and its referral healthcare facilities.
Strengths and limitations
This research explored qualitatively healthcare provider experiences of PMTCT in the high mobility context of Johannesburg during COVID-19. Qualitative interviews were conducted with different cadres of staff, this sample is a strength because, despite the small sample size, it has transferability and broad applicability with our results. A limitation is possible self-reported bias from participants, however the strength of self-reported methods is that it allowed participants to both describe their own provision experiences with PMTCT and HIV services in-depth. 33
Conclusion
Future studies are needed that explore the patient perspective to better understand if and how the mobility profiles of women who are on the PMTCT program may have an impact on their utilization experiences, including their overall ability to adhere to lifelong care. 11 Furthermore, the major task for healthcare providers was to reinstate service delivery of PMTCT without putting themselves or patients at risk of COVID-19 infection, and the use of technology to alleviate the high-burden of patient demand. It is important to take what was learned during the pandemic and integrate it into routine service delivery, which includes long term medication supply to reduce multiple visits to the hospital and overall risk of COVID-19 transmission for HIV pregnant women. Healthcare policies that work toward inclusion and sustainability for migrants are needed to improve the integration of safer and practical methods of PMTCT provision into health systems.
Footnotes
Acknowledgements
We would like to thank the staff at Rahima Moosa Hospital for your passion and participation in the study, The Life in the City, School of Governance & School of Public Health at University of Witwatersrand for supporting this research.
Author Contributions
Bisnauth and supporting authors conceived of the presented idea. Bisnauth and Vearey developed the theory. Bisnauth conducted data collection and performed the analysis. Vearey verified analytical methods used. All authors supervised the findings of this work. Bisnauth took the lead in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis, and manuscript.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Life in the City Grant, School of Governance, at the University of Witwatersrand.
Ethics Approval
The studies involving human participants were reviewed and approved by the Human Research Ethics Committee (HREC) at the University of Witwatersrand, South Africa in 2019. Provincial clearance was obtained by Gauteng Province and The National Health Research Database (NHRD No: GP_201912_003) and the City of Johannesburg. Authorization from RMMCH was granted to conduct the study in Coronationville (HREC Protocol No: M190816 MED19-07-084). Written informed consent to participate in this study was provided by the participants/participants’ legal guardian/next of kin.