
Abstract
Background:
Strategies to improve sexual health outcomes have evolved over the years due to technology’s evolution to ensure that they are relevant. Challenges have been noticed in different systems that run parallel, particularly in Low-Income Countries where the majority utilise Indigenous Health Systems. Optimisation of resources and minimisation of conflicts could be realised through integrated health systems in the management of adolescents’ sexual health issues. This study sought to develop strategies to facilitate Indigenous Health System and Modern Health System integration to improve the management of Adolescent Sexual Health issues, leveraging results from 3 papers.
Methods:
A multi-stage approach was utilised, with Phase 1 focussing on a preliminary assessment through merging findings from the 4 papers. The Strengths, Weaknesses, Opportunities, and Threats analyses were then used, followed by the Basic Logic Model to identify critical aspects that needed to be considered in building the strategies. The second phase used the Build, Overcome, Eliminate and Minimise framework to build the strategies.
Results:
A total of 5 strategies were proposed to facilitate this integration, and these included revival of committees that were inclusive of all stakeholders; allocating Indigenous Health System space in clinics to work in; establishing adolescent-friendly clinics; intensifying information dissemination on sexual health-related issues, and developing clear Terms of Reference and procedures to govern this integration and ensure it is a success.
Conclusions:
Implementing these strategies could facilitate this integration and ensure that programs are planned and implemented in a complementary manner, thereby reducing conflicts between the 2 systems and ensuring collaborative efforts towards shared goals that would transform to better Sexual Health Outcomes for adolescents.
Keywords
Background
Adolescent sexual health (ASH) programs have been implemented in different settings worldwide.1-4 Strategies to improve sexual health (SH) outcomes have evolved over the years due to technology’s evolution to ensure that they are relevant.1,4 Research has also intensified globally to ensure that evidence-based and robust strategies are implemented to address hindrances towards safer sexual practices among adolescents. 1 It is worth noting that developed strategies should consider critical contextual issues prevailing in that specific population to be served. 5
Different country settings have different contextual backgrounds that aid the success or failure of implemented programs.5,6 Reported factors in literature such as cultural, socio-economic, religious, political, policies, infrastructure, availability of human resources, to mention a few, have been proven to impact on efficiency and effectiveness ASH-related issues. 7 Therefore, strategy development to address weaknesses in ASH programs needs to be systematic, logical, and evidence-based to ensure relevant and effective programs are implemented. 8
In Zimbabwe, it is well documented in the 2010 to 2015 strategy review that there are weaknesses in the adolescent sexual and reproductive health (ASRH) programs as most do not involve most stakeholders who matter.3,4 Behaviour change communication (BCC) strategies such as the utilisation of media such as radio broadcasts, magazines, social media, and other strategies such as sister2sister counselling and support for the vulnerable adolescent girl child have yielded some positive results.9,10 In the Zimbabwean context in line with the sister2sister program, female adolescents were deemed to be vulnerable as the majority are at risk of being sexually abused in the communities they live in as compared to adolescent boys. However, most of these strategies have yielded positive results in most urban areas with adequate infrastructure to support these initiatives.4,10 The scenario is different in rural districts that have network challenges to access these information-sharing mediums.11,12 Since Mberengwa and Umguza Districts are rural, they face similar challenges. 12 Adolescents in these districts rely mainly on available health systems (HSs) in the community (ie, IHS and MHS) that help shape their sexual behaviours, particularly starting from their homes, schools, clinics, hospitals, traditional healers, and many more key stakeholders having a role to play. 11
Integrating all the HSs involved in ASH issues provides a window of opportunity for better health outcomes as far as ASH outcomes are concerned. 13 No evidence in the literature suggests that efforts have been made to strengthen collaborative efforts between IHS and MHS. Most emphasis has been on improving the quality of programs that are implemented in the MHS. This has led to fragmented programs that run parallel as the IHS serves a significant population proportion. Therefore, this paper sought to develop strategies to facilitate the integration of IHS and MHS for improved management of ASH issues as stipulated in the study protocol. 14 The development of these strategies would leverage on the empirical evidence of 4 papers that explored different aspects with regards to ASH and HSs.15-18 The summarised findings of these 4 papers are presented on Table 1.
Merging of findings from 4 papers.

Methods
The strategy development process would be done in 2 major phases: the first phase would involve the interrogation of findings from 4 papers. This would be the preliminary assessment that would merge the results from the 4 papers and set the second phase’s tone. The second phase would leverage on the merged data’s interpretation from phase 1 and develop strategies (though done in stages). This strategy development process would be done in liaison with key stakeholders that are experts in adolescent sexual health, health systems, culture, and policies governing sexual health and human rights. Therefore, the process of development of the strategies would follow a series of steps that are detailed below:
Preliminary assessment
Merging data from 4 papers
This step compared the findings from these 4 papers side by side to have a comprehensive overview of the state of matters concerning adolescent sexual practices as influenced by the 2 HSs (ie, IHS and MHS).15-18 This then enabled for a merged output to be generated to get an overview of the merged output to get a glimpse of key facets that needed to be taken into account and addressed in the development of the strategies in a triangulated manner.19,20 The first paper (tilted Health System Strategies and Adolescent Sexual Health: a systematic review of the literature using Rodgers Concept Analysis Framework, submitted to SAGE’s Journal of Health Services Insights) aimed at reviewing the literature on the relationship between Health System Strategies (HSSs) and ASH issues guided by Rodger’s evolutionary concept analysis framework. The study further sought to leverage the findings of this literature review to develop a Conceptual Framework (CF) that would guide research on ‘Development of strategies to facilitate safe sexual practices in adolescents through integrated health systems in selected districts of Zimbabwe’. 15 The second paper (titled Indigenous Health Systems and Adolescent Sexual Health in Umguza and Mberengwa Districts of Zimbabwe: Community Key stakeholders’ Perspectives submitted to the SAGE’s Journal of Health Services Insights) paper explored the roles that are played by the MHS in the management of ASH issues as well as appreciate the ASH trends in the 2 districts. This paper further challenged HSPs to identify specific IHS factors incorporated into the MHS to improve ASH outcomes. The participants were also further probed on the challenges that were likely to be encountered in integrating IHS into MHS and how best these challenges could be overcome to maximise the benefits of this integration as guided by the study protocol. 16 The third paper (titled Health Service Providers’ Perspectives on the influence of Modern Health Systems on adolescents’ sexual health practices in Umguza and Mberengwa districts of Zimbabwe submitted to SAGE’s Journal of Health Services Insights) sought to explore the roles that are played by the MHS in the management of ASH issues as well as appreciate the ASH trends in the 2 districts. This paper further challenged HSPs to identify specific IHS factors incorporated into the MHS to improve ASH outcomes. Participants were also further probed on the challenges that were likely to be encountered in integrating IHS into MHS and how best these could be overcome to maximise the benefits of this integration as guided by the research protocol. 17 The fourth paper (titled Health Systems Utilisation and adolescent sexual health practices in Umguza and Mberengwa districts in Zimbabwe submitted to SAGE’s Journal of Health Services Insights) sought to explore the extent of the influence of IHS and MHS in moulding adolescent sexual behaviours in Mberengwa and Umguza districts. This paper further explored adolescent sexual experiences. It sought to explore their views (adolescents) in whether it was essential to integrate these 2 systems (IHS and MHS) and, if so, how as guided by the study protocol. 18
The strengths, weaknesses, opportunities and threats analysis
The strengths, weaknesses, opportunities, and threat (SWOT) analysis framework was then applied to the merged findings. This framework will help identify the strengths and weaknesses of the currently implemented programmes/strategies given different contextual factors in the 2 HSs (IHS and MHS) as presented in the findings of all the 3 papers.21,22 This exploration enabled the determination of potential opportunities available for the possible integration of the 2 HSs (IHS and MHS) to aide collaborative efforts and enhanced positive outcomes in ASH-related issues. The framework further allowed for determining possible threats that could derail this integration and set the pace for further interrogation using the Basic Logic Model. 23 Therefore the SWOT analysis as a tool allowed for the interrogation of the papers’ findings in an integrated manner and enabled for the comprehensive needs assessments as attained in the 2 districts in a triangulated manner as the 3 papers used different approaches.19,20
Application of the basic logic model
The findings obtained from the SWOT analysis were further be subjected to scrutiny using the Basic Logic Model (BLM). The BLM is a critical tool that is typically used for evaluating different projects, programmes, and processes to determine the key aspects that need to be optimised to ensure that desired goals and objectives are met.24,25 The BLM has 5 key aspects that were used to brainstorm on key considerations that must be considered to aid in integrating the 2 systems (IHS and MHS). 24 The 5 critical aspects of this framework that would be considered are shown in Figure 1 (ie, resources needed to facilitate this integration; activities that would be engaged with; the outputs; short and long term outcomes, and the impact).24,25 Exploring these 5 key critical aspects would enable key issues to be considered. When building the strategies, there is a clear guide of what needs to be achieved and stipulate the indicators and resources needed to achieve that goal. 25 These, therefore, allowed all fundamentals to be considered and explored in a systematic, logical, and comprehensive manner leaving no stone unturned. 24 After exploring these 5 critical aspects, the actual building of the strategies to ensure that the integration was done was guided by the build, overcome, eliminate and minimise (BOEM) model.

The BLM outcome.
Strategy development
Application of the BOEM model
This model builds strategies that try to aid the attainment of goals and realisation of the impacts of strategies by overcoming, eliminating and minimising potential factors that could undermine the impact of developed strategies. 14 This model is still new and has not been used much but presents an opportunity for a comprehensive assessment of the status quo and strives to get the best out of the strategies considering the different contextual factors. 14 The strategies will be crafted, taking into account the preliminary assessment findings where threats are sought to either be overcome, eliminated, or minimised.14,26,27 The strategies would also seek to leverage the opportunities identified and occupy that opportunity/policy space to aid the integration.26,27 The built strategies would clarify how this integration would be achieved and detail how the strategies would be implemented.
Proposed strategies
All these processes would be draft strategies presented in this paper and would then be further scrutinised through an independent validation process to determine the feasibility, acceptability, and applicability. As stated in the aim of this paper, the proposed strategies would seek to facilitate the integration of IHS and MHS to improve ASH outcomes. This intended outcome would then be the basis for the validation process.
Results
Merged results
The findings of this study point out that a significant proportion of adolescents engage in sexual activities and that there is a significant proportion who suffer or have previously suffered from STIs and being pregnant or impregnating. The findings further point out that IHS and MHS programs targeting adolescents run parallel, though, to some extent, there are complementary. There is also room for integration of the 2 systems (IHS and MHS), as evidenced by the different stakeholders’ willingness to work together. These findings are presented in Table 1.
The SWOT analysis outcome
Basing on the merged findings of this research, strengths, weaknesses, opportunities, and threats were identified to evaluate what is obtaining in as far as HSs are concerned in Umguza and Mberengwa districts. These findings are presented in Table 2.
Outcome of SWOT analysis.

The BLM outcome
The BLM applied to the SWOT analysis findings presents key aspects that are needed under the 5 key areas. There is a need for funding and investment in human resources to ensure the integration of IHS and MHS are kick-started. Furthermore, there is a need for intensive training and awareness campaigns regarding this integrating and extended consultations with key stakeholders to facilitate the uptake of different programs that would foster this integration. The envisaged outputs, short and long-term outcomes and the impact of this integration are also presented. These findings are shown in Figure 1.
Building the strategies
The BOEM outcome
The outcome of the BOEM framework alludes that there is a need to develop strategies that overcome mistrust, financial and human resources deficit, barriers to access to SH services by adolescents at the same time eliminating myths, donor dependency while minimising misuse of resources and ensure collaborative efforts between the 2 HSs. These findings are presented in Table 3.
Outcome of the BOEM analysis.

Proposed strategies
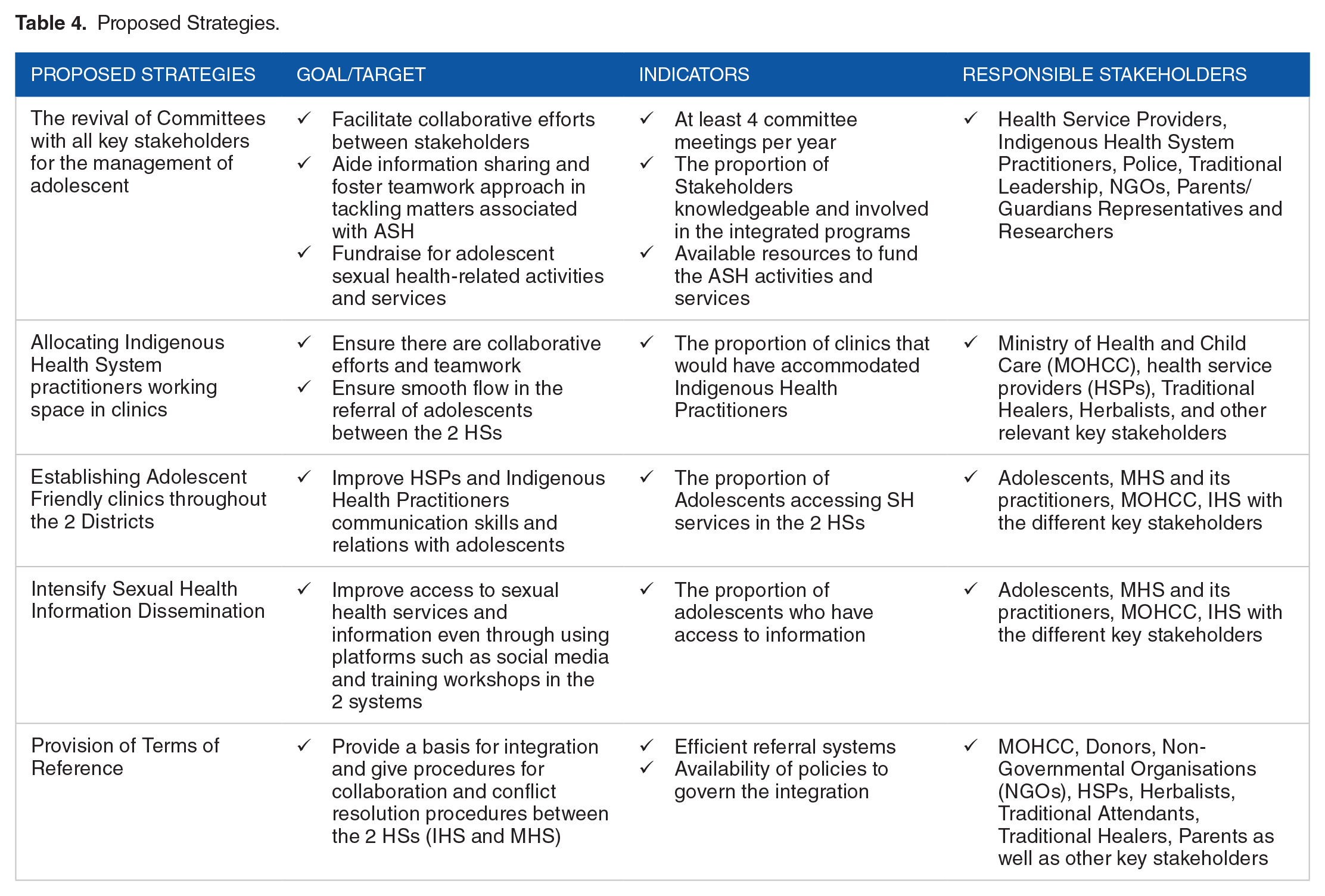
A total of 5 strategies are proposed to facilitate the integration of these 2 HSs. These are the revival of committees, allocating IHS space in clinics to work in, establishing adolescent-friendly clinics, intensifying information dissemination on sexual health-related issues and developing clear Terms of Reference procedures to ensure the government of IHS and MHS as they work together. These proposals are presented in Table 4.
Proposed Strategies.
Discussions
The merged findings pointed out that a significant proportion of adolescents engaged in sexual activities and that there is a considerable proportion who suffer or have previously suffered from STIs and being pregnant or impregnating. It was reported in the literature that the prevalence of STIs and pregnancies or impregnating of adolescents in these 2 districts was significantly higher than other districts.2,4,14,28 Though the prevalence was lower than what was reported in 2013 in a study conducted by Moyo (2013), these prevalence rates still cause concern, thereby needing robust strategies to address these problems. 28 Different stakeholders cited several challenges, 1 of them being the element of mistrust between the 2 health systems. The literature has reported that it is quite a challenge to integrate different systems underpinned by different belief systems.29-31 There is, therefore, a need to first try and identify common grounds for collaborative activities by identifying similar goals and targets of the different systems.29,31
The merged analysis outcome revealed that that IHS and MHS programs targeting adolescents run parallel, though, to some extent, there are complementary. Most of the time, different systems have different objectives and different ways of achieving them. 29 Therefore, in planning, there is a need to consider all contextual factors that drive that HS and ensure that opportunities are identified from that point of view to foster the successful integration of the 2 systems to achieve collective objectives. Furthermore, results from the merged analysis symbolised that there is room for integration of the 2 systems (IHS and MHS) as evidenced by the different stakeholders’ willingness to work together. Most of the time, various stakeholders work in a solo fashion due to a lack of understanding of what the other systems aim to achieve. Such scenarios bring in the element of different systems undermining each other and running in parallel, yet they are working towards achieving similar goals and objectives. 32
The SWOT analysis revealed (as a strength) that the 2 systems are both recognised in Zimbabwe as major drivers of health service delivery to the populace. This is a strength as there is no need first to legalise the HSs rather, the focus is to identify the platforms they could collaborate through and be merged to attain acceptable outcomes as far as ASH is concerned. 33 The potential threats identified, mistrust, myths between actors in IHSs and MHSs, poverty, lack of resources, and lack of knowledge between the different stakeholders as there were no clear terms of reference despite the 2 HSs being legally recognised in Zimbabwe. It is reported in the literature that several stakeholders who are Christians always associate the IHS with evil spirits and witchcraft.34-36 There is always the mistrust and parallelism of systems as the 2 systems do not share the same values though sometimes they have similar and even complementary goals. 36
Therefore, the BLM was leveraging on the SWOT analysis to brainstorm on the key issues that needed to be taken into account to ensure that developed strategies would facilitate the integration of the 2 systems. Some of the key highlights are to ensure that there are sufficient financial and human resources to conduct training and awareness campaigns and extended consultations to operationalise the ideas. The integration process has to be undertaken so that the intended outcomes of such integrations are clear and well understood by the different stakeholders involved in that program. 29
Therefore, the developed strategies were meant to generate some resources and improve access of adolescents to SH services and activities. In Sub-Saharan Africa (SSA), some of the reported barriers to accessing health services are lack of resources, lack of knowledge, lack of training, and parallel health systems. 37 The developed strategies would bridge this gap and ensure that adolescents have improved access to health services. The development of clear Terms of References would ensure that the aspects and platforms for this integration are laid out, and critical stakeholders know precisely how they are expected to conduct themselves. 29 Stipulated policies minimise conflicts and provide clear frameworks for collaboration and define conflict resolution procedures, primarily where common goals are being pursued using different methods. 38
Conclusions
It can be concluded that the findings of this study justified the need for the integration of the 2 HSs as the different stakeholders showed a willingness to be part of the integrated HS. However, there is a need to overcome threats such as mistrust, myths, poverty, and lack of resources, as these have the potential to derail the integration of these 2 HSs. It also emerged that there is a need to have a developed Terms of Reference that would govern all stakeholders and ensure the common goal is pushed forward.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by the National University of Science and Technology under the Staff Development Programme. The funder paid for tuition fees related to these PhD studies. The funder also provided resources to cover data analysis. Researchers wrote and submitted 6-monthly reports to appraise the funder of progress. The funder’s role was to provide resources to carry out this research successfully.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
WNN is a PhD in Public Health student at the University of Venda. The author conceptualised the protocol as partial fulfilment of the requirements of the PhD requirements. LM is the Promoter, while JTM and RTL are Co-Promoters and the 3 contributed by guiding the study in conceptualising the research idea, carrying out the paper’s research, and preparation. All authors read and approved the final paper.
Author’s Information
WNN is a PhD in Public Health student at the University of Venda in South Africa and is also a Lecturer in the Department of Environmental Science at the National University of Science and Technology in Bulawayo, Zimbabwe. LM is an Associate Professor and JTM is a Senior Lecturer in the Department of Public Health under the School of Health Sciences at the University of Venda in Thohoyandou in South Africa. RTL is a Research Professor at the School of Health Sciences at the University of Venda in Thohoyandou in South Africa.
Ethical Approval
This paper was part of the PhD studies that were conducted at the University of Venda. Ethical clearance was sought from the University of Venda’s Ethics Clearance Committee (Ethics Number: SHS/19/PH/17/2608) and the Medical Research Council of Zimbabwe (Ethics Clearance number: MRCZ/A/2611).