
Abstract
Our objective is to analyze the economic burden of chronic kidney disease (CKD) in Vietnam, particularly in District 2 Hospital at Ho Chi Minh City in 2019. This is a descriptive cross-sectional study. The data source is the medical records of the patients. Encoding the data, analyzing treatment cost, regression modeling, and verification were performed using Stata 15 software. Patients with stage 3 CKD account for the highest proportion of the CKD patient population. CKD comorbidities include hypertension, diabetes, cardiovascular disease, and anemia, which increase the treatment fees of patients. Approximately half of the patients with CKD have diabetes or cardiovascular disease. Treatment costs increase as the condition of the patient worsens (except for stage 1 and 2 CKD). The total expenses of all CKD patients in District 2 Hospital were USD 916 423 988.60. Five main factors that affect the treatment fee of a patient: CKD stage, age, gender, and the presence of diabetes, cardiovascular disease, and anemia. The regression model correctly predicts 96% of cases and can explain 64.15% of the fluctuations in costs. The cost of CKD treatment was higher than Vietnam’s per capita GDP in 2019, and the primary factors affecting costs are comorbidities and dialysis.
Introduction
Chronic kidney disease (CKD) is a serious global health issue, which causes a burden of disease in populations. 1 In the U.S, 1 in 10 adults will have CKD, 2 and the total annual direct costs attributable to CKD are approximately USD 49 billion. 3 In 2016, approximately 9.6% (5.8 million people) of Italian patients had CKD 4 which resulted in an annual loss of 1.81 billion euros. 5 In Thailand, the total annual cost (including ambulatory costs and hospitalization costs) for patients with CKD stage G3a, G3b, or G46 was 5701.34 Thai Baht (equivalent to USD 189.92). 6 In China, according to the 2012 report by the Shanghai Hemodialysis Quality Control Center, 77.5% of dialysis patients had CKD and the average annual cost per patient is approximately $16 625 USD. 7 In Vietnam, according to research by Lan Phuong et al in 2018, the average annual cost of treatment per patient at stage 1 to 3 was USD 2826.3; USD 3320.3; and USD 9498.3 for patients with stage 4 to 5 CKD. In 2018, Vietnam’s GDP per capita was USD 2566.6. This demonstrates that expenses associated with CKD during its initial stages are greater than the average annual income of a Vietnamese citizen, suggesting that a large number of people are unable to afford their own CKD treatment.
District 2 Hospital is recognized as a first-class hospital by the Ministry of Health. During the past year, the hospital conducted over 5500 CKD treatments, which accounts for approximately 1% of the total number of medical examinations and treatments at the hospital in 2019. The cost payable is estimated to be more than the average cost of other diseases. However, no research has been conducted to understand the cost components of the treatment to determine the factors that contribute to increasing the cost (age, gender, clinical condition, etc.) in CKD patients at District 2 Hospital. Therefore, the purpose of this study is to structurally analyze and determine the factors that directly affect the cost of CKD treatment in District 2 Hospital to propose effective interventions and control measures to reduce the burden and improve the lives of patients.
Methods
Study design
This is a cross-sectional study of CKD treatment expenses using a prevalence-based approach based on the administrative database of District 2 Hospital in 2019. The objects were demographics and treatment cost information of all CKD patients in District 2 Hospital from January 2019 to December 2019 (1175 cases). The selection criteria are based on the primary or secondary disease diagnosis code (according to the ICD10) of the patient with the N18 or sub-codes of N18.
In this study, we synthesized the demographic and treatment cost data for each subject in 2001. Next, we analyzed the demographics and treatment costs to determine the factors that directly affect the expenses associated with CKD treatment in District 2 Hospital.
Estimation of cost
This study analyzed the direct medical expenses of CKD patients at each stage, age group, and comorbidity. This analysis also includes variables such as cost of visits, surgery/operation, drugs, blood, laboratory and medical imaging, medical supplies, hospital beds, and transportation. Data were extracted from the administrative database of District 2 Hospital in 2019. All expenses have been converted into U.S. dollars using average exchange rates updated in January 2020 (1 U.S. dollar = 23 172.50 VND). The description of the variables is provided in Supplemental Material 1.
Data analyses and statistical methods
Descriptive statistics were used to summarize the demographic information, clinical status, and component expenditures of the data. Modified Park was used to determine the accuracy of the format distribution. 8
Generalized linear regression was applied to identify the factors associated with the direct medical costs of CKD.5,8,9 The variables adjusted in the model were the stage of CKD, age, gender, comorbidities (diabetes, CVD, anemia) which greatly impact the CKD treatment costs (other studies also used the same variables).5,9 The link test was used to evaluate the accuracy of the model (link function or error case). 5 The Kullback-Leibler-divergence-based R2 was used to describe the degree of variation of the data which was estimated from the generalized linear regression. 9 The P-value <.05 was considered statistically significant. In addition, the study also performed random grouping sampling to make predictions, thereby evaluating the predictability and applicability of the regression model.
Data analysis and statistical tests were performed using Stata 15 software.
Ethical considerations
Written informed consent was obtained from participants who were involved in the study. The research protocol was approved by the Biomedical Research Ethics Council at the District 2 Hospital and the University of Medicine and Pharmacy in Ho Chi Minh City, Vietnam
Results
Patient characteristics
At District 2 Hospital, patients with stage 3 CKD accounted for the highest proportion (482 patients; 41.0%) of the total 1175 CKD cases diagnosed. In general, CKD patients at District 2 Hospital often have high blood pressure (957 patients; 81.4%) and ischemic heart disease (554 patients; 47.1%). On average, patients had 9 (16.8%) outpatient visits and 10 (11.0%) days of inpatient treatment annually. The results are presented in Table 1.
Demographics of CKD patients at district 2 hospital in 2019.
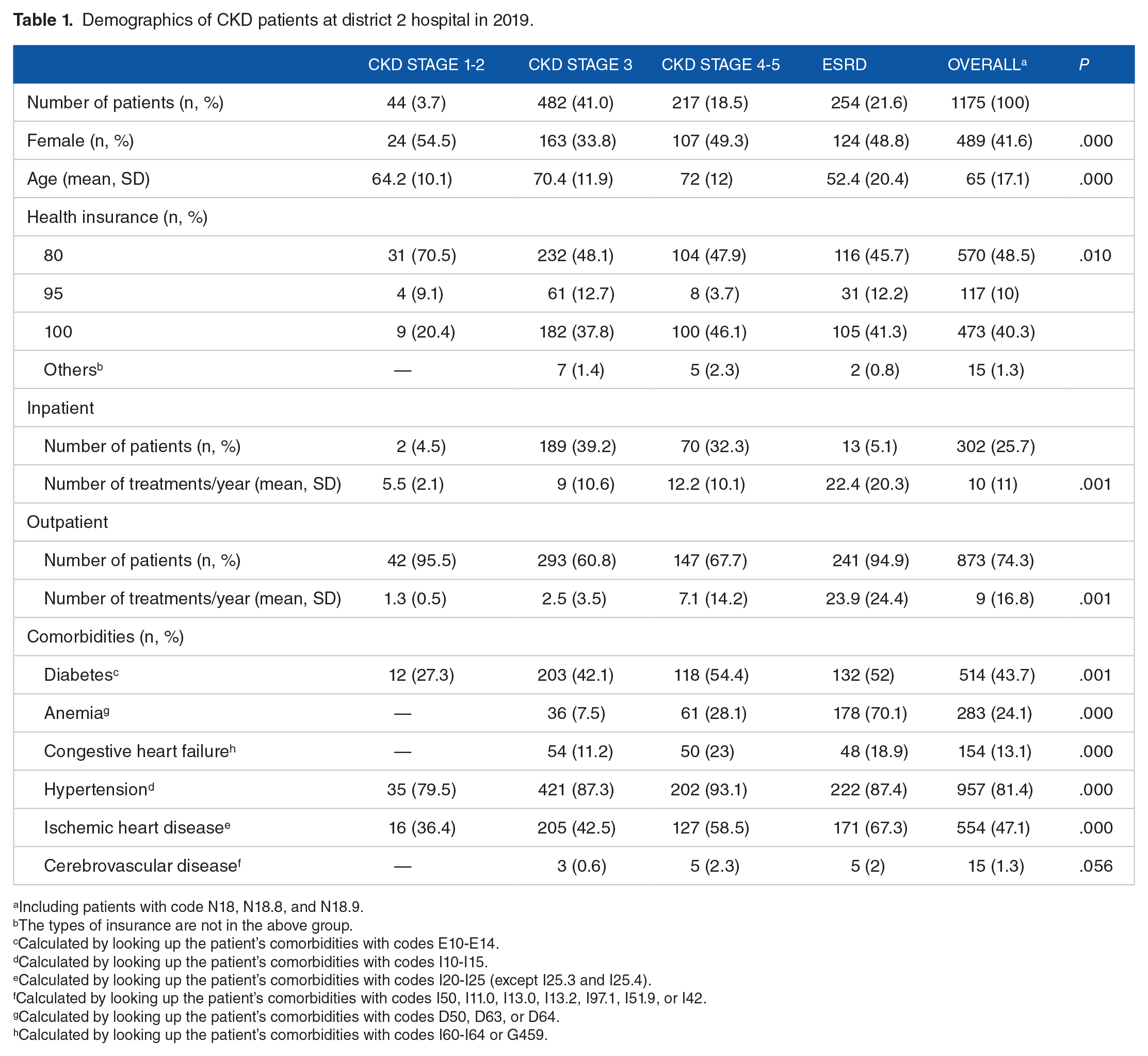
Including patients with code N18, N18.8, and N18.9.
The types of insurance are not in the above group.
Calculated by looking up the patient’s comorbidities with codes E10-E14.
Calculated by looking up the patient’s comorbidities with codes I10-I15.
Calculated by looking up the patient’s comorbidities with codes I20-I25 (except I25.3 and I25.4).
Calculated by looking up the patient’s comorbidities with codes I50, I11.0, I13.0, I13.2, I97.1, I51.9, or I42.
Calculated by looking up the patient’s comorbidities with codes D50, D63, or D64.
Calculated by looking up the patient’s comorbidities with codes I60-I64 or G459.
Treatment costs of CKD
The total expenses of all CKD patient at District 2 Hospital were USD 916 423 988.60. The per-patient costs disaggregated for different CKD stages are shown in Table 2. Treatment expenses differed between inpatients and outpatient patients, similarly, expenses differed between men and women. There is a significant transformation in the structure of the cost list over the disease stages. In general, drugs, surgery/operation; laboratory tests and medical imaging are expenses that account for the largest proportion of CKD patients at District 2 Hospital (Table 2).
Direct medical cost of CKD patients in each stage (Unit: USD).

Kruskal-Wallis test.
Based on the Gamma distribution.
Generalized linear regression
The study utilized the generalized linear regression model (GLM) with its most common form of the log link function and the gamma distribution, the results are presented in Table 3.
Regression results for the estimated model by treatment costs and drug costs.

Compared with patients with CKD stage 1-2.
Compared with male patients.
Two-tailed Z test.
The average differences in costs between patients in the 1 to 100-year age group.
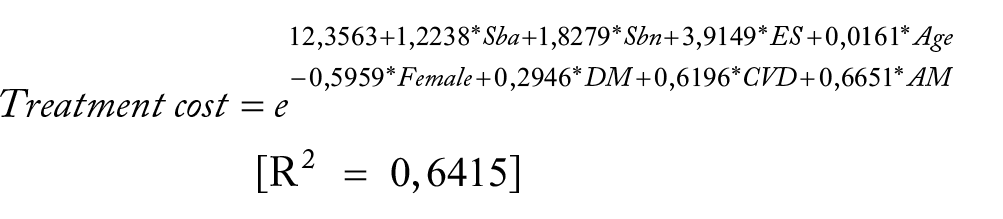
The intercept coefficient in the treatment cost regression model of CKD is 12.3563. This parameter implies that the median self-determined average cost of a patient with CKD at District 2 Hospital was e12 3563 = USD 10.03 when the patient had background pathology such as CKD stage 1 to 2, male, 0 age, and absence of comorbidities of diabetic, cardiovascular disease, or anemia. Note that costs are only valid arithmetic.
The cost GLM regression formula in CKD patients:
Regression formula by treatment cost:
Regression formula by drug cost:

Where
Pseudo-R² is measured by the Kullback–Leibler divergence.
SBa: The dummy variable represents patients with stage 3 CKD (Sba = 1 if the patient has stage 3 CKD; Sba = 0, otherwise).
Sbn: The dummy variable represents the patients with stage 4 to 5 CKD (Sbn = 1 if the patient has stage 4-5 CKD; Sbn = 0, otherwise).
ES: The dummy variable that represents the patient is in ESRD (ES = 1 if the patient has ESRD; ES = 0, otherwise).
Age: A discrete quantitative variable representing the age of the patient.
Female: The dummy variable representing the patient is Female (Female = 1, if female; Female = 0, if male).
DM: The dummy variable represents the patient with diabetes (DM = 1, if the patient has diabetes; DM = 0, otherwise).
CVD: The dummy variable representing patients with cardiovascular disease (CVD = 1 if the patient has cardiovascular disease; CVD = 0, otherwise).
AM: The dummy variable representing patients with anemia (AM = 1 if the patient has anemia; AM = 0, otherwise).
The results indicates that multicollinearity does not affect the regression model by treatment cost and the Regression model by drug cost, because all GVIF (generalized variance inflation factor) values <2 (variable of CKD stage [1, 83], age [1, 35], gender [1, 03], DM [1, 09], CVD [1, 28], AM [1, 48]).
Random samples were divided into 2 groups. The training set was used as input parameters to estimate the model (approximately 85% of the total number of patients) and the test set was used to verify the predictive ability of the model (approximately 15% of the total number of patients). The results are shown in Figure 1, where the average predicted value line (dark green), 95% confidence interval of the predicted value (light blue area) and the actual values, the cost of CKD patients corresponds to the age and stage of each person. In patients with CKD stages 1 to 2, the regression model predictions when the approximate actual values are in the 95% confidence interval. In patients with stage 3 CKD, it indicated that the actual cost value had a significant deviation from the forecasted value. For patients with CKD stages 4 to 5, the actual cost value also deviates from the forecast range, although not as much as in stage 3.
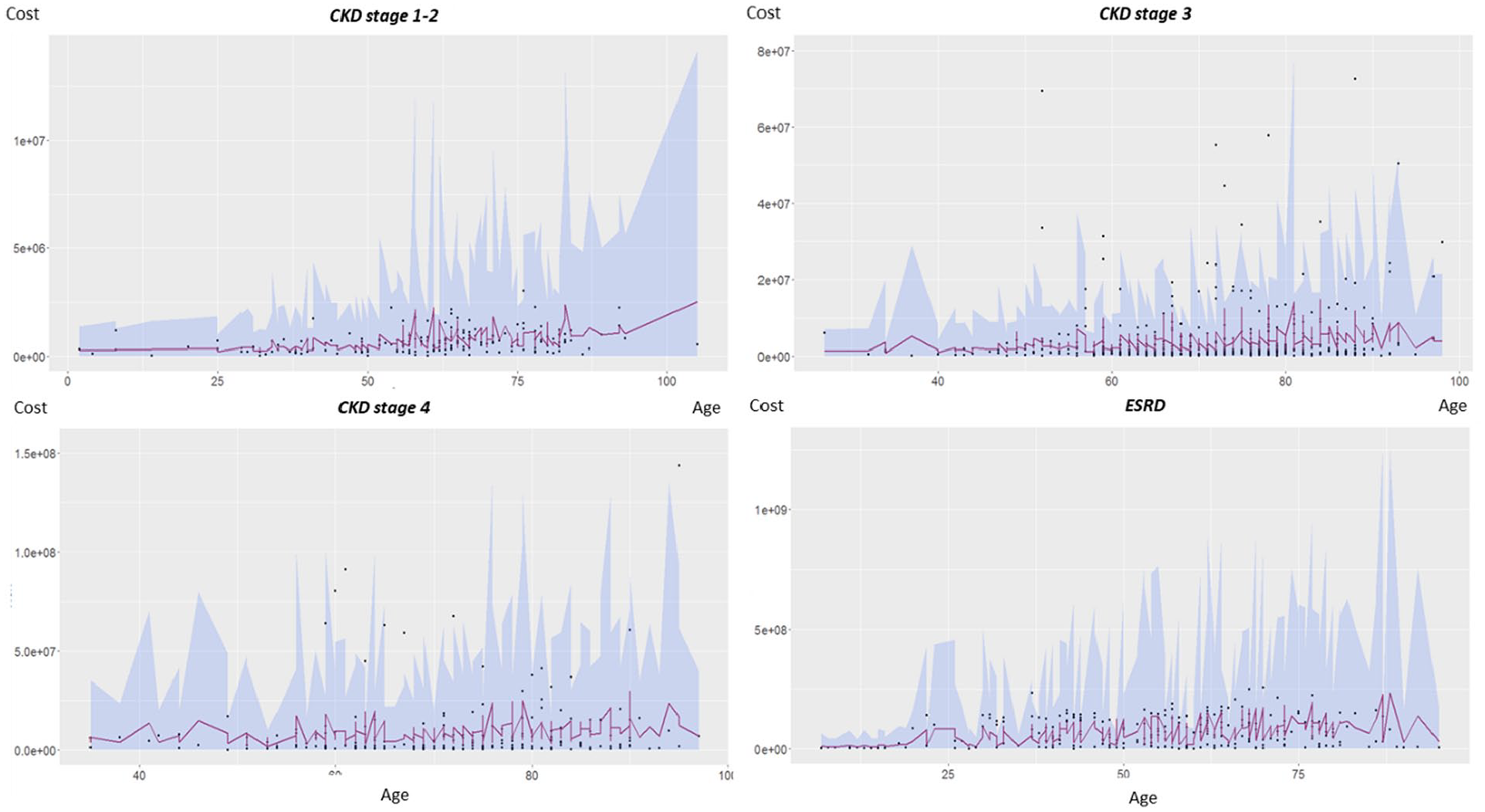
Predicted cost and actual cost at different stages by age.
Discussion
At District 2 Hospital, the demographic results also show that more than half of the patients treated for CKD are in stages 3 to 4, which indicates that the hospital’s management and intervention policies should focus on this stage to achieve the best results. In addition, according to global epidemiological studies,7,10 the prevalence of CKD stages 1 to 2 is usually greater than of other stages. However, according to District 2 Hospital data, the proportion of CKD stages 1 to 2 accounts for only 3.8% the total patients with CKD treated at the hospital. This could be since the majority of patients with stages 1 to 2 CKD are currently undetected.
At District 2 hospital, drugs account for the highest proportion of CKD treatment costs among inpatients. Among outpatients, surgery/operations account for the highest proportion (50%), and drugs for the second-highest proportion of CKD treatment costs. There is no cure for CKD. In the early stages of the disease, treatments with reversible causes may prevent disease progression. With end-stage renal disease (ESRD), patients need dialysis or a kidney transplant to live. 11 Therefore, the cost of drugs and surgery/operations (especially the cost of regular dialysis) is the primary reason for the economic burden on CKD patients. Policies can be proposed to strictly control medication and reduce drug costs, or support ESRD patients to significantly reduce the burden on patients.
For the results of the generalized linear regression, it was difficult to predict the treatment cost of patients with stages 3 to 5. For CKD stages 1 to 2 and ESRD, the regression model accurately predicts the approximate actual values in the 95% confidence interval. This is also consistent with the theory of pathogenesis and treatment of CKD. Since stages 1 to 2 are the early stages of CKD, kidney function is not greatly impaired and does not require much medical intervention or treatment, so the cost is usually low and “predictable.” For ESRD patients, dialysis is usually mandatory and accounts for most of the cost, so the cost is less volatile. Compared to other studies,12-14 it is observed that the most important factor affecting the treatment cost of CKD patients is always mentioned as comorbidities. Therefore, hospitals need to pay attention to different treatment methods focusing on the management of associated comorbidities to improve treatment efficiency and reduce the treatment cost of patients.
Conclusions
In District 2 Hospital, the cost of CKD treatment was higher than Vietnam’s per capita GDP in 2019. The important factors affecting the cost are comorbidities and dialysis. Further, research on this topic can improve data, which can increase the accuracy of the regression forecast and its applicability in practice. This improves the medical quality of District 2 Hospital.
Supplemental Material
sj-pdf-1-his-10.1177_11786329211036011 – Supplemental material for The Economic Burden of Chronic Kidney Disease in Vietnam
Supplemental material, sj-pdf-1-his-10.1177_11786329211036011 for The Economic Burden of Chronic Kidney Disease in Vietnam by Hai-Yen Nguyen-Thi, Thanh-Nhan Le-Phuoc, Nhan Tri Phat, Dat Truong Van, Thuy-Trang Le-Thi, Nguyen Dang Tu Le, Hong-Nguyen Tran-Thi and Luyen Pham Dinh in Health Services Insights
Footnotes
Acknowledgements
The authors would like to show their appreciation to the board of directors and the hospital staff of the District 2 Hospital for offering the great opportunity for us to conduct our research at their sites.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
The authors confirm contribution to the paper as follows: study conception and design: HYNT and NDTL; data collection: TNLP; analysis and interpretation of results: NTP, NDTL, HYNT; draft manuscript preparation: NTP, NDTL, DTV, TTLT, HNTT, LPD. All authors reviewed the results and approved the final version of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.