
Abstract
This study examined the coronavirus disease 2019 (COVID-19) preparedness and response of the health system (HS) in Hanoi, Vietnam, and identified enabling factors and barriers. This cross-sectional, mixed-methods study was conducted in 4 urban and peri-urban districts that included some wards with COVID-19-positive cases and some without. The US Centers for Disease Control and Prevention (CDC) analytical frameworks were used. Overall, 10% of health facilities (HFs) failed to fully implement COVID-19 risk determination; 8.8% failed to fully implement stronger community partnerships with local stakeholders to support public health (PH) preparedness; 35% and 2.5% incompletely implemented and did not implement evaluation of PH emergency operations, respectively; 10% did not identify communication channels to issue public information, alerts, warnings, and notifications; 25% incompletely implemented identification, development of guidance, and standards for information; 72.5% had good preventive and treatment collaboration; and 10% did not fully implement procedures for laboratory testing and reporting results. Enablers included sufficient infrastructure and equipment, strong leadership, and good cross-public-sector collaboration with police and military forces. Barriers included workforce constraints, overburdened and inconsistent reporting systems, inappropriate financial mechanisms, ambiguous health governance, and lack of private-sector engagement. Nonetheless, the HS preparedness and response were satisfactory, although further coordinated efforts in evaluation, coordination, communication, and volunteering remain necessary.
Background
As of November 10, 2020, coronavirus disease 2019 (COVID-19) had spread rapidly in 72 countries, causing more than 49.7 million cases and over 1.2 million deaths. 1 As of November 12, 2020, South East-Asia had 9.9 million confirmed cases and 152 723 deaths. As of December 24, 2020, Vietnam had 1421 confirmed cases, 102 of which were receiving treatment, 1281 of which were recovering, and 35 of which had resulted in death. 2
Due to heightened global concerns around the COVID-19 pandemic, the World Health Organization (WHO) has published more than 100 relevant documents since January 2020. This novel coronavirus has been addressed by undertaking activities to monitor and investigate outbreaks; to identify and characterize the nature of the virus; to minimize transmissibility, morbidity, and mortality; to minimize the burden on and support the health system; and to inform, engage, and empower the public. 3
Healthcare facilities in Vietnam are divided into the following 4 levels according to their administrative structure: central (Level I); provincial (Level II), covering a population of 1 to 2 million; district (Level III), covering a population of 100 000 to 200 000; and commune/ward (Level IV), covering a population of around 5000 to 10 000. 4 The healthcare system has a mixture of public and private provision. A health-insurance system was introduced in 1993, and the government has made a considerable effort to achieve universal coverage, reaching 89.2% of the population in 2020. 5
Vietnam has mobilized its entire political system to fight COVID-19 by developing pandemic-control guidelines for all healthcare levels, including grassroots levels, on procedures for controlling, detecting, and quarantining cases or at-risk groups. 6 During the national lockdown, the prime minister stated that success in the fight against COVID-19 would result from Vietnam’s “national consensus,” including coordination among state agencies, and between state and society. The level of coordination within the political system has been remarkable. Ministries—notably those of Defense, Health, and Information and Communications—have coordinated closely with provinces/cities, communes, wards, and residential quarters, where local officials have informed individual households of government policies.
As a country with a history of successfully managing infectious diseases since the severe acute respiratory syndrome (SARS) pandemic in 2003, 7 Vietnam has learned lessons about increasing investment in public-health infrastructure with the establishment of a national emergency operations center in 2013. 8 The political/administrative system has made operational plans. This groundwork led decision-makers to perceive the Wuhan coronavirus’ potential for devastation early on, and to prioritize public health (PH) over the usual economic imperatives. It helped legitimize the operational plans’ implementation, providing institutional arrangements for coordination both across sectors and vertically, and a “toolbox” of both classical and new apparatus. To protect frontline health workers (HWs), the Vietnamese health system also adapted to remote consultations to mitigate exposure. 9
With these experiences, Vietnam’s healthcare system effectively minimized the spread of COVID-19 using the following strategies: first, proactively investigating epidemiology and monitoring to detect early infections or suspected cases; second, spray disinfectants such as chloramine B at quarantine sites; third, coordinating with other departments to supervise “social isolation”; and fourth, receiving information about infected and suspected cases from the community for appropriate treatment plans.6,10
However, there are some remaining limitations of Vietnam’s health system in terms of pandemic preparedness and response due to health system-level issues, including a constrained national health budget, insufficient human resources, poor health-management apparatus, and insufficient equipment and medicine. 11
Additionally, there has been limited research focusing on the preparedness and responses to the COVID-19 pandemic in Vietnam. This study examined the COVID-19 preparedness and responses of the Hanoi primary healthcare system and identified enabling factors and barriers to implementation.
The findings of this paper will provide important lessons in promptly responding to future waves of the COVID-19 pandemic for health managers and policymakers.
Methods
Study setting
We used mixed methods, including quantitative and qualitative approaches. The study was conducted in 2020 in 4 districts of Hanoi: Ba Dinh (221 893 population, 14 commune health stations or CHSs) and Hoan Kiem (135 681 population, 18 CHSs) (urban districts); and Me Linh (244 555 population; 18 CHSs) and Soc Son (348.153 populations, 26 CHSs) (peri-urban districts). Each district included 1 commune/ward with COVID-19-positive cases and 1 commune/ward without COVID-19-positive cases. Regarding the burden of the pandemic, only the Me Linh and Ba Dinh districts had positive cases (12 and 1 confirmed cases, respectively). They had no deaths due to COVID-19. 12
Quantitative study
Study subject
In total, 80 health facilities (HFs) of 2 urban districts and 2 peri-urban districts were selected for the present study: 4 district health centers (DHCs) and 14 CHSs of the Ba Dinh urban district; 18 CHSs of the Hoan Kiem urban district; 26 CHSs of the Soc Son peri-urban district; and 18 CHSs of the Me Linh peri-urban district.
Study tools
Preparedness tools and checklists to enhance the readiness of healthcare professionals and facilities responding to COVID-19 provided by the US Centers for Disease Control and Prevention (CDC) were used; specifically, the Public Health Emergency Preparedness and Response Capabilities (version 2018) framework.13,14 The framework described the components necessary to advance public HF preparedness and response capability. For the purposes of this component study, “response capability” encompasses both clinical care and PH services, and is measured regarding both the actual capability of service delivery, and the performance of those services. 15
Study variables
Quantitative research was conducted to assess emergency response to the COVID-19 pandemic at the grassroots level including the following: preventive services related to COVID-19; identifying infected people; tracing contacts of infected individuals (using the WHO document entitled “Contact tracing in the context of COVID-19” to develop criteria assessment for contact tracking capability); identifying people at risk; isolation; and testing and diagnosis. The following aspects were assessed: regulations, processes, facilities, equipment, human resources, financial resources, and associated services
Qualitative study
Study subject
We conducted an in-depth interview with 6 representatives of the district level units (including 4 centers of preventive medicine and 2 district hospitals); 2 managers of CHS in each district; 4 grassroots HWs directly involved in COVID-19 pandemic prevention; 3 representatives of mass organizations and local authorities in each district. Additionally, 2 focus-group discussions were conducted with the participation of inhabitants in isolated areas and non-isolated areas.
Study variables
Facilitators and barriers to the implementation of the COVID-19 pandemic emergency response at the grassroots level were examined as follows.
Governance/leadership: (1) Interagency coordination activities; and (2) Participation of the private sector in emergency response activities to the COVID-19 pandemic.
Health financing: (1) Affordability of COVID-19 diagnosis and treatment services; (2) Funding for specific activities related to COVID-19 prevention; and (3) Insurance coverage.
Health workforce: (1) Quantity of HWs; (2) Quality of HWs; (3) Allocating health staff and rearranging the work of HWs to cope with the rise of COVID-19 patients; (4) Mobilizing HWs from the private sector, the Red Cross, and the military medical staff; and (5) Lack of HWs if they have to isolate, test positive for the COVID-19 virus, or work overtime.
Medical consumables, technologies, and medicine: (1) Infrastructure and equipment related to COVID-19; (2) Testing; and (3) Clinical guidance at an HF.
Health information system: (1) Synthesize, monitor, and report cases of infections, suspected infections, high risks, and deaths; and (2) Reporting system.
Data analysis and management
Study tools were developed by the Hanoi University of Public Health (HUPH). All the interviews were directly conducted by research team members. The audio recordings from each interview were transcribed by researchers and analyzed by research topics. Quantitative data were collected and managed via Research Electronic Data Capture (REDCap) software. Descriptive statistics were carried out with means, count, and proportions for corresponding variable types. We also collected and compared secondary data from multiple sources (quarterly reports, monthly reports, and so on) to improve the reliability of the primary data. All analyses were conducted with the STATA 16 software (STATA Corporation).
Ethical considerations
Respondents were asked to provide informed consent prior to commencement of the interview. All collected data were confidentially kept, coded, secured, and used only for research purposes. The ethical considerations of the study were approved by the Institutional Review Board of the HUPH.
Results
General characteristics of studied HFs
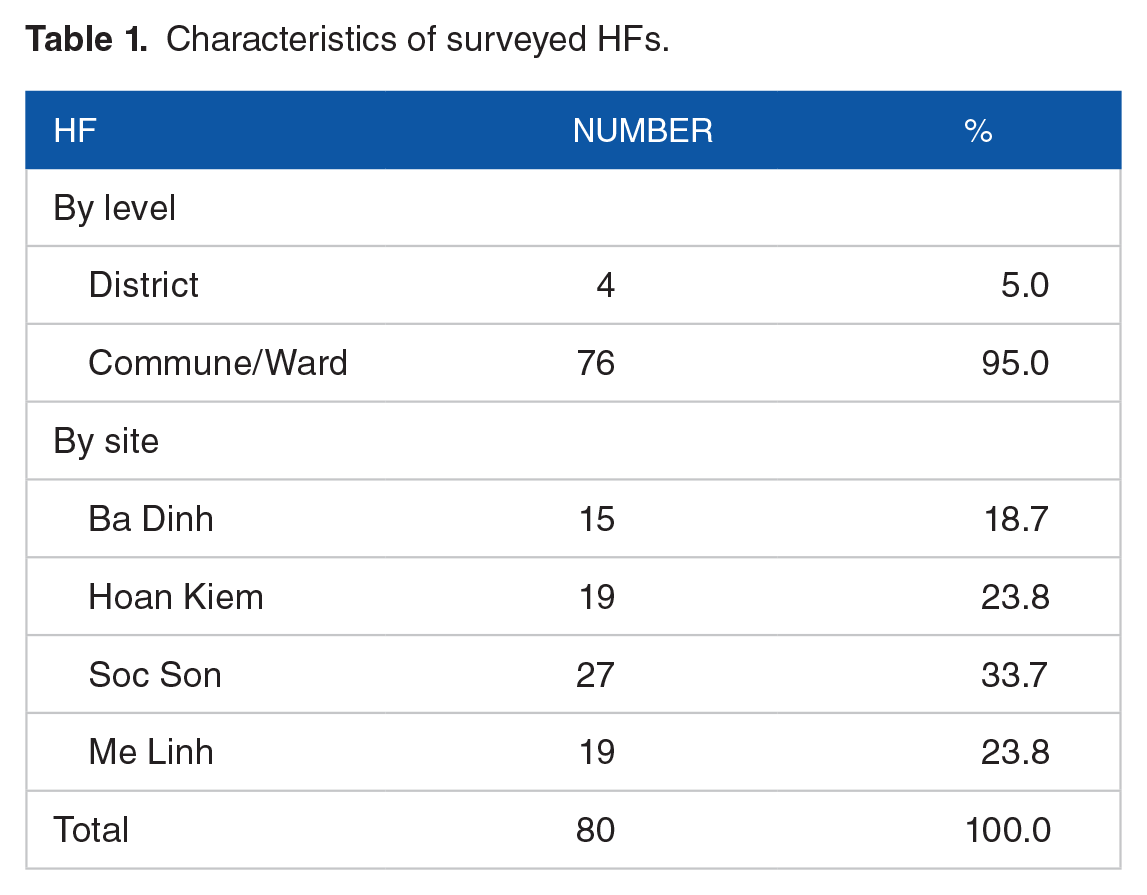
The present study was conducted in 4 districts of Hanoi comprising Ba Dinh, Hoan Kiem, Soc Son, and Me Linh. The evaluative questionnaire of the capability of district level HF was 4 (5.0%) and the questionnaire for commune/ward level HFs (CHS) was 76 (95.0%). The number of questionnaires distributed for each district was different due to the specific number of CHSs in each district. Ba Dinh district has the least number of questionnaires (15) (accounting for 18.7%) while Soc Son had the most (27) (33.7%) (Table 1). The response capability to COVID-19 of Soc Son district’s general hospital and Me Linh district’s general hospital were also surveyed.
Characteristics of surveyed HFs.
COVID-19 preparedness and response capability at primary HFs (preventive medicine)
Table 2 shows that overall, all applicable activities were implemented by some of the HFs.
COVID-19 preparedness and response capability at primary HFs (preventive medicine).

The community preparedness function
“Strengthening community partnerships to support PH preparedness” was fully implemented at most facilities, but incompletely implemented at 7. “Coordinating training and providing guidance to support community involvement with preparedness efforts” was fully implemented by 68 HFs (85%), but incompletely implemented by 12 (15%).
The emergency operations coordination function
“Conducting preliminary assessments to determine the need for activation of PH emergency operations” was fully implemented by 72 HFs (90%). There were 77 HFs (96.3%) fully implementing the plan to “Activate PH emergency operations,” but 1 HF did not implement this activity. “Evaluating PH emergency operations” was only implemented fully by 50 HFs (62.5%), 28 HFs incompletely implemented this activity, and 2 HFs did not perform this assessment at all.
Emergency public information and warning
“Activating the emergency public information system” was fully implemented by 69 HFs (86.3%) but 1 HF had not yet implemented it. The Selection of information integrated into communication content was incompletely implemented by 7 HFs (8.8%), 1 HF had not identified the main content integrated into the communication channel.
Information sharing
All HFs identified the right parties to share information and the shared content, although 5 HFs incompletely implemented this activity. Only 58 HFs (72.5%) fully implemented the activity of “Developing guidance, standards, and systems for information,” and 1 did not develop this guideline. Only 67 HFs (83.8%) could fully exchange information among agencies, 11 HFs had incompletely implemented this, and 2 HFs did not perform this activity.
Care and support for cases or isolated cases
All HFs had identified their roles and duties in supporting quarantine cases. However, 5 HFs incompletely implemented this activity. Preventive and treatment coordination measures were fully implemented in 58 HFs, 17 HFs (21.3%) had not completely implemented, and 5 HFs had incompletely implemented this. Eight HFs had incompletely implemented the sampling procedure for testing, and an additional 2 had not yet implemented a sampling procedure. The training for sampling procedures and outreach skills had been fully implemented in 68 HFs (85.0), while 9 (11.2%) had incompletely implemented this activity, and 3 HFs had not received any training.
PH surveillance and epidemiological investigation
The development and implementation of case and suspected case surveillance processes were fully implemented in most HFs (93.7%), only 5 incompletely implemented this activity.
Volunteer management
Only 50 HFs (62.5%) fully implemented the selection and training of volunteers, 5 did not implement this activity, and it was deemed unnecessary in 2. Also, only 72.5% of the HFs had assigned specific tasks to volunteers, and only 41 (51.3%) had completely assessed the specific activities of volunteers.
Comparison of COVID-19 preparedness and response capability in areas with and without positive cases
Table 3 shows the COVID-19 preparedness and responses classified by 2 areas: districts with positive cases and districts without positive cases. A comparison was made among the main group (capability group) and all criteria, which were scored from 1 to 4 points, with 1 point indicating “fully implemented” and 4 points indicating “not applicable.” Thus, the lower the score, the greater the response to the pandemic.
COVID-19 preparedness and response: areas with and without positive cases.

For the “Community preparedness” capability, areas without positive cases implemented the activity more fully than areas with positive cases (1.08 points vs 1.13 points); however, this difference was insignificant. Similarly, for the “Emergency preparedness” capability, areas without positive cases implemented the activity more fully than areas with positive cases (with a difference of 0.6 points, which was statistically significant [P < .05]). For “Emergency public information and warnings,” areas without positive cases also implemented the activity more fully than areas with positive cases (with a difference of 0.1 points, which was not significant). With “Information sharing” and “Care and support for cases or isolated cases,” there was seemingly no difference between the 2 areas, with the difference of 0.02 and 0.04 points, respectively, which were not significant. Testing equipment in areas without positive cases was more fully implemented than that in areas with them, with the difference of 0.1 points; however, this difference was not significant. For “PH surveillance and epidemiological survey,” areas without positive cases had 0.03 points less than areas with positive cases, and this difference was not significant. Regarding “Volunteer management” activity, there was not a large difference (only 0.06 points), and it was not significant. Ultimately, based on the total points, the activities in areas without COVID-19-positive cases were more fully implemented than those in areas with COVID-19 positive cases; however, this difference was not significant.
COVID-19 preparedness and response capability at the district hospitals
The results (data not shown) revealed that the contents of the emergency response to COVID19 were implemented relatively completely in 2 district hospitals. However, some criteria such as “HWs and service staff need to be screened for COVID-19 symptoms and risk factors before each work shift, before entering HF” and “visitors and caregivers are educated about COVID-19 prevention” were not fully implemented. The criteria for “private rooms for patients who receive positive results for COVID-19,” “natural ventilation: minimum open area” and “self-ventilation” were not implemented at 1 district hospital. Two criteria, “no more than 1 person per 6 square meters” and “the minimum distance between 2 beds is 2 m” were fully implemented in 1 of 2 studied hospitals. “Hand hygiene” was incompletely implemented in 1 district hospital.
Enabling factors and barriers to emergency preparedness and response to COVID-19 at the study sites
To enhance the effectiveness of the activities of emergency preparedness and responses to COVID-19, it is necessary to assess the impact factors of the quality of implementation for disease prevention and control.
Service delivery
Lacking good coordination and a clear referral classification made it difficult for patients with chronic diseases to adhere to their treatment at the time when quarantine and isolation measures were executed.
“Difficulties are obviously seen. In the time of quarantine and isolation, there were some chronic disease patients who could not visit monthly HF like before when they would like to be periodically checked up. In cases where they lived in quarantined/isolated areas, we could not bring them out. Drug provision to those patients is a little bit difficult I think.”
(An HW)
To promptly meet the needs of communication to provide knowledge for local people, the grassroots health system also mobilized population collaborators, members of the Elderly Association, the Red Cross Association, the Youth Union, and the Women’s Union.
Medical consumables, technologies, and medicine
Personal protective equipment (PPE) for healthcare staff was scarce when the first COVID-19 wave occurred; however, that was not the case for the second wave.
16
“[. . .] How much for the district level, how much for the commune level, how much for the provincial level? There must be a base for people to prepare. Without a guideline, we do not know how we can sufficiently prepare [. . .]”
(An HW)
“We should be guided on how much PPE should be in stock in case of emergency. For instance, it should depend on the community transmission level, if it is community transmission Level I, you must prepare like this, if it is community transmission Level II, you must prepare like that, then, we can be well prepared”.
(An HW)
Health workforce
One respondent stated that if COVID-19 occurred wave-by-wave, their HWs could handle the workload; however, if the pandemic took longer and spread widely in the community, then they would need a new human-workforce strategy, which would supplement the existing ones.
“[We were] hard hit! Extremely hard hit! In the normal condition of having no pandemic, health staff were just sufficient. At the height of the COVID-19 outbreak, our health staff were apparently insufficient.”
(HC representative)
Almost all HWs were not being professionally trained and searched for and accessed COVID-19 disease information via mass media on their own.
“[. . .] Knowledge about COVID-19 is extremely important, training courses help us not to be overwhelmed. To be honest, I had never thought that we would have to cope with a COVID-19 pandemic like this. I did not attend any training course at all. Therefore, when the pandemic occurred, we were totally overwhelmed.”
(An HC representative)
After the government had specific instructions and information about COVID-19, HWs were fully trained in procedures for the implementation of response activities and followed the instructions of the National Steering Committee for COVID-19 prevention and control. Overall, grassroots HWs’ professional knowledge about COVID-19 was adequate to respond to the pandemic.
Governance/stewardship
Cross-sector collaboration
All-level People’s Committees, the police force, and the military force/local boards of the military had close collaboration with the health sector.
“Without the police force, it is difficult for the health system. People here do not want to cooperate with the health sector (contact tracing, investigation, isolation, quarantine and so on); with the participation of the police force, the cooperation will come more easily.”
(An HW)
Ineffective governance
Lacking specific guideline documents for pandemic prevention drove stakeholders’ difficulties, resulting in pressure on the health sector; decisions were considered impractical sometimes.
“When COVID-19 occurred, there were job assignments, however, there were no specific instructions for every participating agency/unit; thus, they let the health sector do everything. For instance, for F1 transportation, why must it be the responsibility of the health sector, it could be the responsibility of the military, right? Additionally, we lacked instructions for how to establish the medical quarantine area when the first positive case was present. It was because of having no instructions and clear responsibility among stakeholders that the health sector had to undertake all the tasks.”
(An HC representative)
Contribution and participation in COVID-19 prevention and control by the private sector is supposedly insufficient.
“The private sector? Totally inadequate! What do they participate in? Who directs them? Who mobilizes them? Who cares about them? We requested them to give us a list of their patients with fever, but they did not do so. Having no mechanism for mobilizing them at all, no one (in the private sector) wanted to shoulder this work.”
(An HW)
Health financing
The financial sources used for COVID-19 pandemic prevention and control included the following: the state budget; health insurance; and official development assistance (ODA) grants and financial support from individuals nationally and internationally. Funds should be allocated to participating HWs who directly participate in COVID-19 pandemic prevention and control.
Interviews showed that DHCs were confused when applying financial regulations to pay allowances to subject groups who were involved in pandemic prevention and control (Resolution 37/NQ-CP).
Health-information system
The reporting of COVID-19 statistics was considered burdensome at the primary healthcare level. Specifically, there were requests to make many daily reports at different times, and different statistical reports were asked to be sent to different stakeholders.
“Obstacles include consolidation, statistics, and data reporting. For instance, for me, after fulfilling my duties, if I did not consolidate and check data thoroughly, the results could not be precise. The preparation work for data meeting and announcement is important. We should invest in human resources for data reports.”
(An HW)
"[. . .] there is always a comrade at the reporting center; reporting to the Hanoi Department of Health, reporting to the CDC Hanoi twice a day; reporting to the District People’s Committee [. . .] many reporting channels with frequent reports.”
(An HW)
Discussion
General information
In Vietnam, Hanoi had the highest number of COVID-19-positive cases and suspected cases in the first wave who needed isolation; thus, the characteristics of the COVID-19 response could be a basis to evaluate disease prevention for Hanoi in particular and for Vietnam in general. The present study was conducted in areas where there were both positive cases and negative cases (76 CHSs); thus, it objectively reflected the existing state of the COVID-19 response by HFs. The grassroots level was at the front line of disease prevention, and the role of the HWs was important in detecting suspected COVID-19 cases, isolating them, and informing higher levels about these cases.
COVID-19 preparedness and response capability at primary HFs
Full implementation of activities at the time of the first COVID-19 wave in Vietnam was dependent on the actual condition of each HF regarding the health workforce, infrastructure, equipment, and so on. In the context of the newly emerging infectious COVID-19, knowledge and understanding of the pandemic was sparse; therefore, guidance about COVID-19 for HWs was also lacking. In other words, COVID-19 preparedness and response at the primary healthcare level was not always fully implemented and sometimes not implemented at all. This has also been found through evaluative studies on COVID-19 preparedness and response in other countries, ranging from developed countries like the United States and Italy to developing countries in Africa. The results of these studies revealed that in the first COVID-19 wave, primary healthcare facilities were not well prepared for its prevention and control.17-19
For “Emergency operations coordination,” evaluation of the effectiveness of measures requires the assessor to have certain skills and experience, which are difficult to obtain. Because most of the surveyed HFs were at the front line, some were still at the stage of implementing pandemic control measures, and thus cannot be evaluated until these finishes. “Health education” was one of the important missions of the CHSs, thus, it was clear that most had experience in implementing this activity. “Information sharing” was not well implemented by the CHSs; since they did not receive instruction or guidance, information about the pandemic was not provided in a timely manner and disseminated. “Care and support for cases or isolated cases” activity revealed that the coordination between preventive care and treatment was not good, and only 82.5% of HFs had cooperated with treatment facilities for patient support; this could be due to having no or unclear coordination mechanisms between the 2 specialties. “Volunteer management”-related activities were affected by specific characteristics of CHSs (such as small scope); therefore, HWs at the DHCs or CHSs had not yet needed to mobilize volunteers, and because volunteer support mechanisms were not clearly specified, only 50 CHSs’ health staff joined in the training and recruitment of volunteers for future pandemic prevention.
Comparisons between the COVID-19 preparedness and response of areas with and without positive cases showed that there was no statistically significant difference in most activities. This could be due to the similarity between the 2 areas, which received the same direction and training courses on COVID-19 from Hanoi’s Department of Health. However, there were statistically significant differences in “Emergency preparedness” between these areas, such that those with no positive cases had better performance. This result revealed the foresight of areas without positive cases, where the COVID-19 prevention and control work was implemented preemptively. In contrast, areas with existing positive cases were less able to be proactive in COVID-19 prevention and control.
Compared with the usual benchmark of 80%, the following areas should be strengthened: evaluating PH emergency operations; identifying and developing guidance, standards, and systems for information; coordinating between preventive-care measures and patient-treatment measures; enhancing laboratory communications and coordination; recruiting, coordinating, and training volunteers; notifying, organizing, assembling, and deploying volunteers; and evaluating the specific activities of volunteers.
Enabling factors and barriers of implementation
In parallel to adopting restrictive measures to limit viral diffusion in communities, countries also need to ensure appropriate health-system responses to reduce mobility and mortality.
Service delivery
The present study reveals that service delivery during COVID-19 was still lacking linkage; a lack of clear referrals for chronic disease patients made it difficult for them to utilize their healthcare services when isolation measures were applied. This finding is in line with the fact that when health systems are overwhelmed, morbidity is exacerbated, disability intensifies, and both mortality from the outbreak and mortality from vaccine-preventable and treatable conditions increase. Responding exclusively to COVID-19 cases, without considering how the delivery of essential healthcare services will be maintained across the continuum of care from prevention to palliation, comes with several risks. 20 Nonetheless, the evolution of the COVID-19 pandemic around the world shows that people aged 60 years and over have a higher risk of serious illness after being infected by the virus, especially those who were already suffering from serious chronic diseases such as heart disease, diabetes, lung disease, or immune system damage.21,22 Other studies also indicated that fatalities were high in countries with a high percentage of elderly people in the population, large population density, or weak testing, diagnostic, and treatment capacities. 23 Disruptions to the health system will likely cause more deaths among those with a variety of urgent health needs than of patients diagnosed with COVID-19. 24 In these regards, severe cases affect patients with underlying conditions such as cardiovascular disease, hypertension, diabetes or older age; the latter is a particular concern in Vietnam with its aging population.
Medical consumables, technologies, and medicine
Most Hanoi-based HFs had facilities in better condition compared to other locations. PPE in the initial period was lacking drastically. This issue was experienced not only by Hanoi HFs but also Ho Chi Minh-based HFs, and other HFs based in other provinces. These findings are in line with those of Zeenny et al, who reported the results of a study on hospital pharmacists in which the majority experienced a shortage of masks, gloves, and hand sanitizers during the COVID-19 pandemic, 20 as well as in other studies worldwide.25-28
Health workforce
Regarding the health workforce for the COVID-19 response, for the initial phase they were able to meet the requirements of disease prevention and control work, however, they will need to be well prepared for the occurrence of many positive cases. With the existing health workforce, it will be impossible to address the future burden of disease. These findings were in line with those of a study in Sri Lanka, which reported that it experienced a shortage of trained healthcare providers, with the potential for the situation to be further exacerbated by the non-compliance of some people with safety measures. 27 Our findings of good knowledge among HWs was in line with Huynh et al, 29 who reported that 88.4% of participants had sufficient knowledge regarding COVID-19. The reviewed literature also mentioned that special emphasis should be given to the psychosocial needs of healthcare providers, so that they can fulfil their professional responsibilities during this pandemic. 30
This present study also revealed that during the COVID-19 pandemic, the mobilization of HWs from different sources was important for each locality. CHSs’ representatives were also members of the National Steering Board for COVID-19 prevention and control at the level of communes/wards; therefore, they could efficiently cooperate with related stakeholders, who were also under the same umbrella. There should be clear job descriptions and job assignments for each participating member. In practice, the literature also has shown the importance of community HWs as allies in confronting pandemics, especially in awareness-raising among the population and fighting the stigma related to the disease 25 ; as well as in the mobilization of retired HWs or training of HWs not presently practicing so they could return to service in the US 24 ; and in the mobilization of PH nurses in Japan to avoid dysfunction of public COVID-19 responses. 28 These were all lessons learned for Vietnam to mobilize its HWs in the case of a pandemic outbreak.
Governance/stewardship
The roles of the police and military forces were important regarding cross-sector collaboration. HWs have no role and function to sanction violations of the pandemic control principles; thus, in this regard, the role of the police is important. This finding is in line with those of Erkhembayar et al, 31 who reported that multidisciplinary cooperation, early engagement, and guidance from the WHO office enabled health authorities in Mongolia to successfully undertake early risk management. This also pairs well with the findings of Hunte et al, 32 who reported that the COVID-19 health system response of Trinidad and Tobago demonstrated that, although developing countries face many health-system challenges, political will, evidence-informed decision-making, respect for science, and timely, coordinated, collaborative actions can strengthen the resilience and response of the health system during a health emergency.
Health financing
By interviewing related respondents, it was learnt that at the time of conducting the survey, financial sources were assessed to be sufficient for the needs of COVID-19 preparedness and response. However, we should have a long-term vision for financial resources, because of the persistent impacts of COVID-19 on the economy, the collection sources of the State budget, as well as financial hardships in the community (ie, it will be hard to mobilize contributions from the community while they also have to meet with financial difficulties due to the pandemic).
Health-information system
For the current study, the reporting of COVID-19 statistics was considered burdensome at the primary healthcare level. Specifically, there were requests to make many reports at many different times during the day, and different statistical reports had to be sent to different stakeholders. This finding is in line with Bibaa, 26 who reported that weak information-management systems were key among the factors and social determinants of COVID-19 spread. The WHO recommends the involvement of primary healthcare in the triaging of patients presenting with COVID-19 symptoms while ensuring the continuous service delivery of essential healthcare.
Other studies have also revealed lessons of relevance to Vietnam. For instance, one revealed that robust health information system (HIS) that are adequately financed and developed before a future outbreak can cyclically strengthen health systems, pandemic preparedness, and response capacities. 33 HIS can redirect the allocation of resources precisely to where they are most needed across regions and over time, so that total demand is met within the constraints of the limited resources available. Taiwan successfully demonstrated this by leveraging its integrated HIS to analyze multiple national datasets for transparent distribution of PPE to citizens in locations of greatest need. 34 Strengthening HIS may lead to more resilient health systems with community-based approaches to emergency preparedness and response, while strengthened health systems provide the foundation for robust and sustainable HIS. 33 In another context, Brazil’s primary healthcare system also showed that, in view of the potential for many HWs having to stay away from work during the epidemic, telehealth is a possibility for them to work remotely. 25
Limitations
This study evaluated the performance of HWs through structured self-reported questionnaires, so there may be a lack of objectivity in the comments. The criteria for assessing the complete/incomplete level of activities were based on the research subjects’ feelings without clear quantitative criteria; therefore, the collected information could be considered as subjective. COVID-19 is also an emerging disease, and the documents and guidelines on assessing the adequacy of activities are not yet sufficient, so it was difficult to assess the completeness of the studied activities.
Conclusions
Despite some lack of capability and resources, the Hanoi health-system preparedness and response have been satisfactory; however, further coordinated efforts such as evaluation, coordination, communication, and volunteer management are required for more efficient COVID-19 preparedness and response in Vietnam.
Health-system level enabling factors included sufficient infrastructure and equipment to promptly respond to the COVID-19 pandemic; strong leadership from higher levels to lower levels; and good cross-public-sector collaboration (the engagement of police and military forces). On the contrary, health-system level barriers included the health workforce (constraints, overload, and pressured working conditions in cases of rapid surges of the pandemic); HIS (overburden and inconsistent reporting systems); health financing (complicated inappropriate financial mechanisms for purchase and allowance); and governance/stewardship (ambiguous governance and lack of private sector engagement).
Footnotes
Acknowledgements
This study has received support of South Asia Field Epidemiology and Technology Network, Inc (SAFETYNET, Inc), a non-stock, non-profit organization in the Philippines and General Department of Preventive medicine (Vietnam’s Ministry of Health) and health faculties where the study was conducted. We thank all health facilities and community people for participating in the interviews for this study. We thank Melissa Barberan for editing the English contents of this paper.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Study design: Minh Van Hoang, Data analysis, writing: Minh Van Hoang, Tuan Kim Duong. Revision of the manuscript: Anh Tuan Tran, Trang Thu Vu. Approval of final manuscript: all authors.