
Abstract
To provide important evidence for the resource allocation process in Vietnam, this research was conducted to explore the return on investment (ROI) of the national colorectal cancer (CRC) screening program. A decision tree model was designed to estimate the cost and cost savings of a national screening program (ie, providing annual fecal occult blood test [FOBT], following with colonoscopy in case of FOBT positive for the medium-risk group over 50 years old) compared to no screening scenario. This was the first attempt in estimating the ROI of a public health program in Vietnam. Although there was a wide variation due to the uncertainty of the input parameters, especially regarding the coverage of the colorectal cancer screening program in the community, the calculated ROI rates in all different cases were positive, demonstrating that the national colorectal cancer screening program brought benefits to the investment. With a modest coverage of 30% of the population over the age of 50, the corresponding ROI value was 325.4% (95%UI: 321.0; 329.9). The results of this study could be used to advocate for the implementation of a national colorectal cancer screening program in terms of the monetary benefits of investing in the program.
Introduction
Colorectal cancer (CRC) is one of the most common cancers, 1 causing the third largest burden of disease and death in both sexes in Vietnam in 2017 (estimated using Disability Adjusted Life Year—DALY). 2 In response to this health problem, the Government has showed its commitment in implementing the national CRC screening in Vietnam through issuing several legal documents, such as Decision No. 4299/QD-BYT dated August 9, 2016 on the Projects of prevention, early detection, diagnosis, treatment, and management of cancers (including CRC), cardiovascular diseases, and diabetes, chronic obstructive pulmonary disease, bronchial asthma, and other non-communicable diseases in the period of 2016 to 2020; Decision No. 3338/QD-BYT dated September 9, 2013 on the process of screening and early detection of colorectal cancer; Decision No. 3756/QD-BYT dated June 21, 2018 providing guideline for the prevention, early detection, diagnosis, treatment, and management of a number of common non-communicable diseases (including specific guideline for CRC screening) to the grassroots health system (ie, commune healthcare centers and district-level health facilities).
The above guideline for CRC screening in Vietnam has been in line with international guidelines 3 and current practice in other countries 4 : (1) screening for average risk people from 50 to 75 years old; (2) using FOBT or FIT annually or biennially; (3) performing follow-up colonoscopy in people with positive results of FOBT test; (4) performing colonoscopy every 10 years. However, up to now, CRC screening in Vietnam has only been piloted in a number of large cities and provinces (eg, in Hanoi capital) rather than implementing as a national screening program as regulated in the above Decisions. 5
Although CRC screening is proved to be cost-effective in many countries, 6 the cost-effectiveness information regarding the investment for a similar national CRC screening program in Vietnam seems to be inadequate. In the current context, policy makers require information on whether the interventions are “value for money” in Vietnam context. To help inform the discussion of whether invest in the national CRC screening program in Vietnam, evidence on the financial return of an intervention against the total investment is extremely important. To timely provide the aforementioned evidence in the context of limited number of data sources specific to Vietnam, we performed a return on investment (ROI) model rather than other traditional extensive health economic assessments, that is, cost-effectiveness analysis (CEA), cost-utility analysis (CUA), cost-benefit analysis (CBA). This paper presents the findings of a ROI analysis to determine the financial impact of delivering a national CRC screening program in Vietnam.
Methods
Research was conducted in 5 steps:
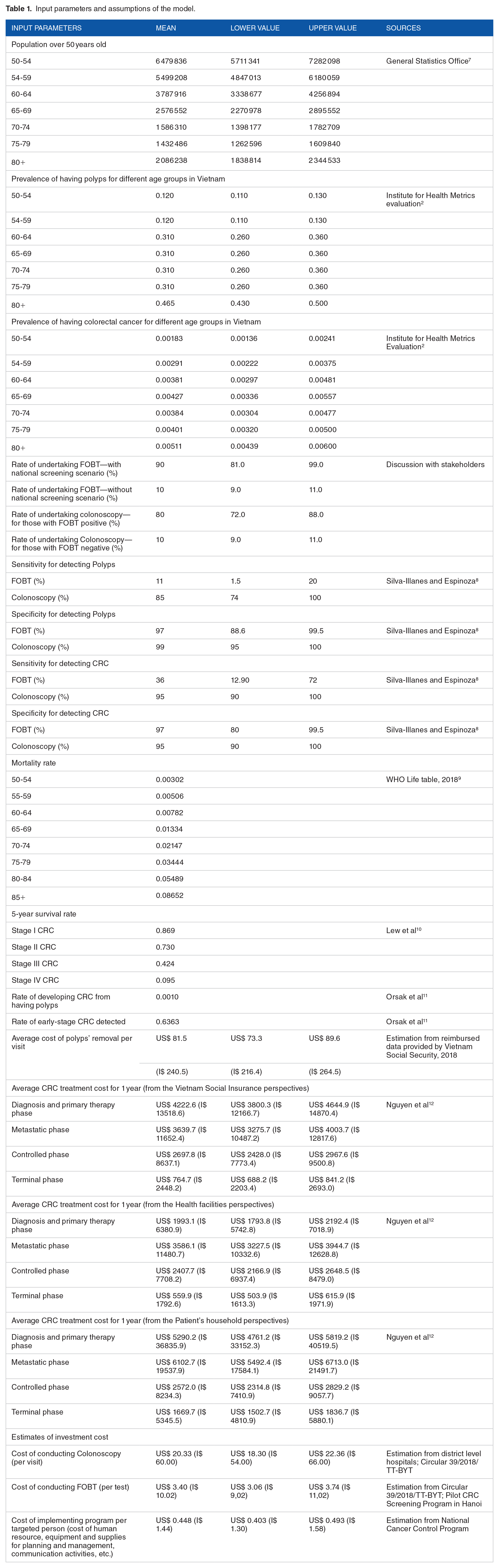
Input parameters and assumptions of the model.

Decision tree model for estimating the cost and cost saving of colorectal cancer screening program
In the deterministic analysis, we assumed that 90% of the population over 50 years old will take the FOBT test in case of implementing the national CRC screening program; only 10% of the target population take the FOBT test in no screening scenario; 80% of those having FOBT positive results will undertake the follow-up colonoscopy and only 10% of those having FOBT negative results will undertake the follow-up colonoscopy. The sensitivity and specificity for detecting polyps and CRC of using both FOBT and colonoscopy were taken from a systematic review of Silva-Illanes and Espinoza 8 Prevalence of having polyps as well as having CRC for different age groups was taken from reliable and available sources.2,13,14 Percentage of patients at each CRC stage in Vietnam was collected from searching the available literature. 2 Moreover, the rate of developing CRC cases from having polyps and the rate of early-stage CRC detected was borrowed from Orsak et al 11
• Net profit (NP) estimated by total benefit/output minus total investment:
• Cost Benefit ratio (CBR) estimated by the ratio of total benefit divided by total investment
• The ROI rate is estimated by NP divided by the total investment:



Negative ROI rate means that investment does not provide additional monetary benefits for this intervention, while positive ROI rate is interpreted as an investment with an additional monetary gain.
Regarding the sensitivity analysis, both one-way and probabilistic sensitivity analysis were undertaken. Due to the uncertainty of the input parameters, we conducted the one-way sensitivity analysis to assess the influence of each input parameter on the model results. After that, probabilistic sensitivity analysis was done using bootstrapping method or Monte Carlo simulation method.17,18 1000 times of simulation were conducted to give expected values and distributions as recommended.17-19 Results were presented as expected values and confidence intervals.
Ethics approval
Research ethic approval for the research was issued by the Research Ethics Committee of Hanoi School of Public Health, Vietnam (Ethics Approval No. 455/2018/YTCC-HD3 dated 7th November 2018).
Results
Return on investment of the national CRC screening program in Vietnam: Deterministic analysis results
Table 2 presents the deterministic analysis results, of which the total investment for the national CRC screening program in Vietnam was estimated at US$ 409.57 million, including costs of human resource, equipment and supplies for planning and management, communication activities, FOBT, and colonoscopy. The total benefit was estimated at US$ 1787.26 million, which was the total cost saved by the early detection and treatment of polyps and CRC cases. Net profit (NP) was estimated by the difference of total benefits and total investment, or in other words, investment in the national CRC screening program in the community that brought the net profit as US$ 1377.69 million.
Deterministic analysis results.

The cost benefit ratio (CBR) was estimated as the total benefit divided by the total investment, with the estimated value in the case of the deterministic analysis being 4.363, or in other words the total benefit of the community CRC screening program was 4.363 times higher than the total investment.
The ROI ratio was 336.4%, which can be interpreted as every US$ 1 invested in the national CRC screening program the country gets US$ 366.4 in return.
Results from sensitivity analysis
Table 3 presents the result of probabilistic sensitivity analysis when coverage rate of FOBT test varies from 30% to 80%. In particular, it can be seen that the total investment ranged from US$ 145.22 million in case of 30% screening coverage (30% of the target population taking FOBT test) to US$ 415.09 million in case of 90% screening coverage (90% of the target population taking FOBT test). In addition, the total benefit was also much higher when expanding the FOBT screening coverage up to 90% of the target population, specifically the total benefit gained in this case was up to US$ 1792.96 million compared to the total benefit achieved when only covering 30% of the target population (US$ 600.30 million). The ROI rate also varied from 325.4% in the case of 30% screening coverage to 342.5%, 349.6%, 351.7%, and 349.2% in the case of 50%, 70%, 80%, and 90% screening coverage, respectively.
Sensitivity analysis result with different coverage rates of the CRC screening program in Vietnam.

Abbreviations: 95% UI, 95% uncertainty interval; Screening coverage, proportion of the target population having FOBT test
Figure 2 demonstrates the estimated ROI values for 1000 simulations in the probabilistic analysis, which shows that the result of the analysis was quite in agreement with the deterministic analysis.

Result of probabilistic sensitivity analysis in the case of screening 30% of the target population.
When expanding the coverage of the CRC screening program to 90%, that is, the proportion of population over 50 years old performing the FBOT test up to 90%, the total investment increased to US$ 415.09 million (95%UI: 409.00; 421.17); At the same time, the total benefit was also increased to US$ 1792.96 million (95% UI: 1785.00; 1800.87), resulting in the ROI as 349.2% (95%UI: 344.0%; 354.4%).
Figure 3 shows the results of 1000 simulations in the probabilistic sensitivity analysis in the case of extended coverage up to 90% for the FOBT test. It can be observed that there are times when the simulated investment of the program can be up to US$ 1200 million

Result of probabilistic sensitivity analysis in the case of screening 90% of the target population.
Discussion
The results of this study indicate that the ROI values of CRC screening program vary greatly due to the uncertainty of the input parameters, especially in relation to the screening coverage of the program. Specifically, at 30% coverage of people over 50 years of age participating in the FOBT test, the corresponding ROI value is 325.4% (95%UI: 321.0; 329.9). However, with the increasing the screening coverage of the program, the ROI value has increased, particularly when the 90% screening coverage was achieved, ROI value increased to 349.2% (95%UI: 344.0; 354.4). Some national public health programs in Vietnam, typically the national expanded program on immunization, has achieved 90% coverage for children population under 1 year of age. The success of this national expanded program on immunization stems from the highly accessible primary healthcare facilities, the long history of implementation since 1982, the achievements of health education and promotion, the tailoring policy to remote areas, 20 and more recently, the adoption of the digital immunization registry. 21 Therefore, observing the lessons learned from the national expanded program on immunization, the national CRC screening program in Vietnam will be able to achieve the same level of coverage, especially, the above programs share the same achievement of a primary healthcare system. However, the national CRC screening program should carefully consider other difficulties, such as the inadequate infrastructure and human resources to deliver the FOBT and colonoscopy. The cost of implementing a CRC screening program may be much greater than the estimate in this study since the estimation in this study based on the assumption that the national CRC screening program is on a “steady state,” that is, the infrastructure and human resources are available to deliver the screening test, and therefore the ROI value may be lower than the estimated value.
Due to differences in socio-economic context and healthcare system, the ROI value of CRC screening program varies greatly in different countries. For example, in the study of Stepanek et al 22 in South Africa, ROI analysis was conducted based on the opinion of the payer, that is, an employer company perspective. The authors estimated the ROI in providing all employees of cancer screening tests. While the investment included the medical cost of screening for all employees, the benefit was estimated based on the cost savings as employees rarely absent to go for medical examination and treatment in the later stages and the company would not have to replace workers. The results of the study show a negative ROI (ie, −0.98), which means the investment has not brought additional benefits for investment. However, it is worth noting that the screening does not occur on a large scale, but rather within the scope of a company, so that the study results could not truly reflect the potential benefit of the screening in a larger scale.
Other authors, Orsak et al 11 evaluated the ROI of CRC screening program in rural Texas. The study evaluates the ROI of the CRC screening program as well as of expanding the CRC screening program in a larger scale. The 2 screening techniques considered in the program are fecal immunochemical test (FIT) and colorectal endoscopy (with a follow-up colonoscopy for those with positive results of FIT or endoscopy). The age of the target population is from 50 to 75 years old. In addition to the cost of communication and education activities to increase the number of people participating in the screening program, cost of delivering FIT, and colorectal endoscopy, the program also provided financial support (US$ 20 gift card for transportation) for people once completing the follow-up colonoscopy. The benefit of the program is estimated based on the cost savings by preventing advanced CRC cases and preventing cases of polyps from progressing to CRC cases. The ROI value estimated in this study ranges from 1.46% to 2.06%. Although the ROI value was positive, it was much lower than the estimate in this study. One of the possible reasons for this difference related to the investment of the program evaluated in this study was much different when authors also took into account the non-medical cost, that is, financial support for people undertaking follow-up colonoscopy. In our study, we also focused on FOBT (follow up with colonoscopy) rather than other screening modalities (eg, FIT, endoscopy). In the future, it is required to further the study on also other screening techniques.
In the world, CRC screening in particular and screening of some other specific cancers in general (such as breast cancer, cervical cancer) have been included in the benefit package (of social health insurance or other public financing).23,24 Especially in Japan, screening for most cancers was covered by the social health insurance fund (with co-payments from the members). However, in Vietnam, the amended Law on Health Insurance 2014 has not yet allowed the reimbursement of technical services such as FOBT or colonoscopy for the purpose of “screening.” Meanwhile, the mentioned decisions, that is, Decision No. 3756/QD-BYT and Decision 376/QD-TTg of March 20, 2015, clearly defined social health insurance fund is one of the basic financial sources for cancer screening activities. To advocate for including CRC screening services (FOBT and colonoscopy, as well as additional costs during colonoscopy) into the social health insurance benefit package, this study may provide important evidence on how much financial benefit the social health insurance fund will receive from its investment in CRC screening. Although reimbursement for CRC screening test on a national scale requires a large investment, our study shows that the savings from averted CRC cases for the social health insurance fund are also very large in the future.
The study has some limitations. Firstly, the cost of implementing program (cost of human resource, equipment and supplies for planning and management, communication activities, etc.) was estimated based on the pilot screening model in Hanoi. This model of services delivery may not reflect the true practice of services delivery in the whole country due to the difference in practice in each province. Secondly, due to lack of data, cost of colonoscopy was estimated based on data provided by some provincial-level hospitals; cost of CRC treatment was collected from other secondary data sources. 12 Thirdly, due to lack of evidence on health-related benefit of the colorectal cancer screening program (eg, changes in CRC incidence and mortality, life-year saved) in Vietnam context, it is impossible for us to apply cost-effectiveness of cost-utility analysis. Finally, we only focused on FOBT and colonoscopy rather than other screening modalities (eg, FIT, flexible sigmoidoscopy). The main reason was that FOBT and colonoscopy techniques were recommended in Decision No. 3338/QD-BYT dated September 9, 2013 on the process of screening and early detection of colorectal cancer in Vietnam. FOBT and colonoscopy were also recommended by majority of guidelines based on a recent systematic review. 3 Moreover, due to the fact that the pilot CRC screening program in Hanoi also employed FOBT rather than other screening techniques, it is impossible to estimate the cost of screening program using other screening modalities.
Conclusion
This is the first attempt in estimating return on investment of a public health program in Vietnam. Although there is a wide variation due to the uncertainty of the input parameters, especially regarding the coverage of the CRC program in the community, the calculated ROI rates in all the different cases were positive, demonstrating that the national CRC screening program brings benefits to the investment. With a modest coverage of 30% of the population over the age of 50 participating in the screening using the FOBT test, the corresponding ROI value was 325.4% (95%UI: 321.0; 329.9). When reaching 90% screening coverage of target population, the ROI value increases to 349.2% (95%UI: 344.0; 354.4). The results of this study could be used to advocate for the implementation of a national CRC program in terms of the monetary benefits of investing in the program.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was financially supported by Vietnam National Cancer Control Program.
Declaration of conflicting interests:
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NQA and NTH contributed equally to the design and implementation of the model. All authors contributed to the analysis of the results and to the writing of the manuscript.