
Abstract
HIV-related stigma remains a barrier to ART adherence among people living with HIV (PLWH) globally. People who inject drugs (PWID) may face additional stigma related to their behavior or identity; yet, there is little understanding of how these stigmas may co-exist and interact among these key populations. This study aims to explore the existence of multiple dimensions of HIV-related stigma, and how they may intersect with stigma related to drug injection. The study took place in Vietnam, where the HIV epidemic is concentrated among 3 key population groups; of those, PWID account for 41% of PLWH. The vast majority (95%) of PWID in Vietnam are male. Data came from in-depth interviews with 30 male PWID recruited from outpatient clinics, where they had been receiving ART medications. Deductive, thematic analysis was employed to organize stigma around the 3 dimensions: enacted, anticipated, and internalized stigma. Findings showed that HIV- and drug use-related stigma remained high among participants. All 3 stigma dimensions were prevalent and perceived to come from different sources: family, community, and health workers. Stigmas related to HIV and drug injection intersected among these individuals, and such intersection varied widely across types of stigma. The study revealed nuanced perceptions of stigma among this marginalized population. It is important for future studies to further investigate the influence of each dimension of stigma, and their interactive effects on HIV and behavioral outcomes among PWID.
Introduction
In Vietnam, the HIV epidemic remains concentrated among 3 key population (KP) groups: people who inject drugs (PWID), female sex workers (FSW), and men who have sex with men (MSM). PWID accounted for 41% of PLWH in 2014; HIV prevalence was highest among PWID, compared to other groups: 10.3% in 2013,1,2 and 14% in 2017. 3 Furthermore, PWID is of concern since drug initiation has been shown to start at a younger age and the transition time from non-injecting to injecting use is becoming shorter, while most PWID are not aware of their HIV status. 4
Anti-retroviral therapy (ART) has been rapidly expanded across the country since 2005.1,5 However, stigma and discrimination towards drug use prevented many PWID from accessing HIV testing. 6 Evidence from elsewhere also indicated that drug use-related stigma remained prevalent.7-9 PWID are usually perceived as losing personal control over their behaviors, thus deserved to be blamed,10,11 as drug use is often seen as immoral and criminal.8,12-14 Drug-related stigma was associated with less access to health care in general 15 as well as drug-related healthcare services. 16 Stigmas and dissatisfaction among healthcare providers who provided ART treatment in Vietnam were also reported.17,18 Most research has not investigated both HIV- and drug use-related stigmas concurrently.19-22 The last few years have seen an increasing number of studies examining the role of stigma in ART adherence4,23-25; yet, few have focused on PWID.21,26-28 Only Lim et al 29 and Li et al 30 attempted to quantify these stigmas, but not their joint impact; in the latter study, perceived and internalized stigma were examined among Vietnamese PLWH who use drugs, yet no interactions were investigated. In addition, Li et al 30 only studied those who had not accessed ART; consequently, their results might not be generalizable to those who already initiated treatment.
This study was guided by the HIV Stigma Framework, 31 which posits that stigma consists of 3 distinct yet interrelated dimensions: enacted, anticipated, and internalized stigma. Enacted stigma is the extent to which PLWH believe they have experienced discrimination by others, anticipated stigma is the degree to which PLWH expect that they will be discriminated against, and internalized stigma refers to the extent to which PLWH endorse the negative beliefs and feelings about themselves. 31
Stigma intersectionality
Stigma intersectionality is defined as the simultaneous existence of stigma that is beyond additive stigmas: 2 or more co-existing stigmas can interact to present greater oppression than their simple summation. 32 HIV-positive PWID may experience co-existing stigmas that are related to HIV, drug use, and possible involvement with the criminal justice system, resulting in avoidance of treatment.33,34 They may also experience stigma and discrimination at multiple levels.33,35-37 Turan et al’s 38 and Stangl et al’s 39 frameworks also emphasized that stigma could come from multiple sources, facilitating cross-condition examinations of how stigma related to different conditions can intersect.
Earnshaw and Kalichman’s intersectionality model 40 suggested that the impact of one stigma depends on that of the other; for example, PLWH who inject drugs may be more likely to conceal their HIV status than PLWH who do not inject drugs. 41 Calabrese et al, 42 focused on internalized stigma, also found an interactive impact of HIV and drug-related stigmas on health service utilization. A recent study by Stringer et al 43 found evidence of impacts of substance use stigma on ART adherence, independent of HIV-related stigma. There is a need for a more comprehensive investigation of stigma intersectionality. 44 In this study, using an intracategorical methodological approach, we aim to describe stigma related to HIV and injecting drug use, the existence of multiple dimensions of stigma, and how they may intersect through a series of in-depth interviews with HIV-positive male PWID in a concentrated epidemic. 45
Methods
Data
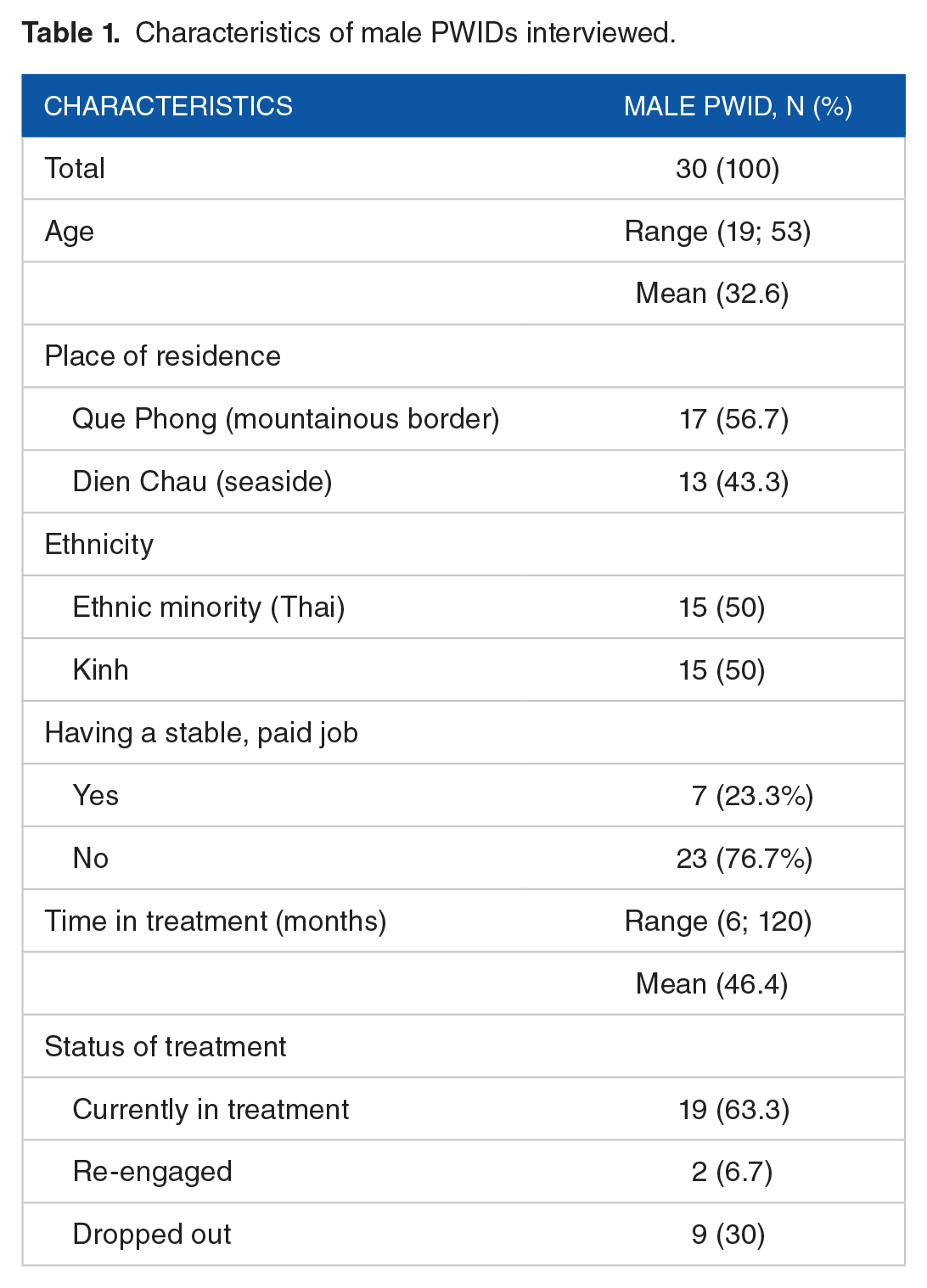
Data for this analysis came from a larger study on barriers to ART adherence among HIV-positive PWID in Vietnam. Male PWID, accounting for 95% of PWID in Vietnam, 2 were the target population; recruitment criteria included: (1) HIV positive status, (2) having been in ART treatment for at least 6 months, even if not continuously, and (3) 18 years old or older at the time of the interview. The final sample included 30 male PWID selected using quota sampling at 2 outpatient clinics (OPCs) with leading ART patient loads in Nghe An province, where the epidemic is concentrated among PWID. 2 Their age ranged from 19 to 53 (mean = 32.4); their demographic characteristics were presented in Table 1.
Characteristics of male PWIDs interviewed.
Semi-structured interviews were conducted in Vietnamese at a place of the participant’s choice, often their homes. The interview guide (see Appendix 1) included questions about challenges that participants might have encountered in accessing HIV testing, ART, and their perceptions and experiences, if any, with stigma and discrimination. There were questions about personal experiences with HIV testing as someone who injected drugs, being HIV-positive, and accessing services. Participants were asked about how they were treated by health care providers, family, and community members, and how such treatment might be different from those of a person living with HIV but did not inject drugs. The interviews lasted between 1 and 2 hours. Each participant received the equivalent of $10 for their time. Ethical approval was obtained from the 2 universities in the United States and in Vietnam.
Interviewers were senior researchers in Vietnam with qualitative method experience, whereas junior researchers transcribed the interviews verbatim. Another team member checked the transcripts against the original audio recordings for completeness and accuracy. Once the interviews were transcribed in Vietnamese, researchers at 2 universities in the US and Vietnam conducted a spot check for completeness and accuracy.
Analysis
Data analysis, using NVivo 11.0, 46 was conducted in Vietnamese in order to preserve the original meanings of responses; quotes were translated into English for presentation. Content analysis was conducted using a priori codes developed for the 3 stigma dimensions, and related concepts that emerged. A codebook was first developed by researchers in Vietnam who conducted interviews. Next, 5 transcripts, diverse in terms of duration of treatment and level of adherence, were coded using the initially drafted codebook. Free nodes were added whenever a new theme emerged. All researchers revised the codebook, each first coded 3 interviews, then re-grouped to discuss and revised the codebook or the codes used, if necessary. Finally, each transcript was coded independently and then merged into 1 data file. For this paper, a deductive, thematic approach was employed to organize the themes around Earnshaw and Chaudoir’s stigma framework. 31
Results
The vast majority of our participants had been in ART treatment for 2 or more years at the time of the study, several had been in treatment for less than 2 years, and only 1 had begun the treatment just over a month before the interview. Adherence was very high, in part because ART medications could be picked up by family members on behalf of the patients; 5 out of 30 participants had their medications picked up for them at the time of the interview. Our data indicated wide variations in perceptions of stigma related to HIV and drug injection among PWID living with HIV. Following Earnshaw and Chaudoir’s 31 framework, we present evidence of possible intersectionality and major themes of stigma related to HIV and injecting drug use. In this section, participants’ age was reported in parentheses, following their ID number.
Theme 1: Enacted stigma
There was a stark difference in enacted stigma related to HIV and drug injection. While the majority of participants reported declines in perceived HIV-related discrimination, nearly everyone reported perceived stigmatization and discrimination associated with injecting drug use. As it could come from multiple sources—spouses and family, community members, and health workers, such stigmatization remained a barrier for PWID to initiate and remain in HIV care and treatment.
Declines in HIV-related perceived stigmatization were attributed to increases in the number of people living with HIV, and increased information and education materials, printed or on TV; the latter contributed to the general public’s improved knowledge of HIV. In contrast, illicit drug injection continued to be perceived as a consequence of one’s losing control of one behavior, and that there was no returning to being a “normal” person once an individual became addicted.
Enacted stigma from families and relatives
It was common to hear about couple separation due to the man’s drug use habits, like this one: “When I returned from the habilitation center, my wife had left me, she had someone else.” (IDI3, 28). In contrast, spouses and families seemed more willing to stay to take care of their HIV-positive men; very few participants reported being separated from spouses or family members solely because of their HIV status:
.. discriminated by people in my family, siblings. . . I can’t even hold my child if he has fever. . . [omitted] me and my wife are not the same anymore. . . my siblings also keep their distance. (IDI13, 31)
Enacted stigma from the community
The most common stigmatization perceived by our participants came from the community. It ranged from a hesitant look, avoidance of interactions, to gossips about the participant’s drug use habits and perceived thefts committed by drug users. In many cases, such stigmatization extended to PWID’s parents and family, which concerned our participants as much stigmatization against themselves. One said:
Our neighbors gossip about us, that makes my parents very sad. If I were not addicted, this would not have happened to my parents. . .. They said things like it was a pity that my parents were government workers but I am a drug addict. (IDI27, 28)
However, it was difficult to tease out if such stigmatization was due to our participants’ HIV status, drug use, or both. In a few cases, like the one below, one may guess that our participant’s reported experience with discrimination was more likely due to his HIV status than drug use:
Sometimes I had to borrow a helmet, when I returned it, they yanked at it and put it away. Or like if I wanted a cup of water, they would try to hide the cups. . . Eventually, I stopped visiting them. (IDI41, 53)
Enacted stigma from health workers
Perceived stigmatization from health workers has frequently been reported as a key barrier for PLWH who inject drugs to going to health centers. Health workers were often seen as unfriendly, unwilling to spend time and answer questions from patients. Stories like the one below were common:
Every time I come to get my medicines, they are always in a hurry; so many patients, one comes after another. I have no time to ask questions. . .. The doctor doesn’t give instructions either, they only give us medicines and we go home. (IDI1, 27)
Other participants felt that they might be a burden to health workers, like this one:
I know the doctor can be under a lot of pressure at work. But their attitudes, to be honest, as a patient I am not happy. Some doctors like doctor Lan (all names in the quotes have been changed) often scolds patients. . . It is actually better here in this district than in XX, it is very uncomfortable there – too many patients, waiting time too long, doctors under a lot of pressure so they can get agitated easily. I can understand that, but still. . . (IDI39, 33)
It was not clear though if this perceived stigma was associated with a patient’s drug use or his HIV status, or if it was due to a possible high patient load as our participants mentioned.
Theme 2: Anticipated stigma
There was strong evidence of anticipated stigma related to both HIV and injecting drug use. Participants frequently talked about potential consequences if their HIV status or drug use habits were known by others. There were fears of being abandoned by their spouse or partner if they disclosed either condition. A man, when asked if he had told his girlfriend, said “Not yet. I am afraid that she won’t accept me. So I don’t dare [telling her that I am positive].” (IDI27, 28). Other participants reported anticipations of being shunned by their friends if their HIV status was disclosed.
They don’t say anything, but since I am infected, I am reluctant to hang out with them. Many times I am afraid that they would say things like “how dare you go out with us when you are sick?” That’s what I think in my mind, just to myself. (IDI1, 37)
Meanwhile, a participant echoed the feelings of many about disclosing their drug use:
People conceal their practice of injecting drugs because even if they only use drugs three times, they will get addicted. The wife will think that if he injects drugs once, there will be the second time, then the third time. . . and addiction is inevitable. Maybe wives find it hard to forgive for that reason. (IDI18, 28)
Several also commented on how they expected more HIV-related stigma and discrimination because they got infected through drug injection, compared to those who got infected through sexual intercourse with commercial sex workers. The same man explained the reason:
Who injects drugs will definitely get addicted eventually. Once addicted to drugs, they will no longer work, leading to stealing. And the society doesn’t accept that. Prostitution, on the other hand, is only considered as an occupation, which does not make people addicted. (IDI18, 28)
Theme 3: Internalized stigma
Feelings of guilt and loss of hope
A prominent sub-theme that emerged was feelings of guilt, where participants blamed themselves for getting infected with HIV and creating a burden for their family. Many expressed more regrets about using drugs and felt more depressed when they compared themselves to HIV-negative drug users:
Many times I feel guilty about the mistakes that I made [engaging in drug use], so now I have to accept the consequence [HIV infection]. I am very heavy-hearted right now, I think a lot about my mother. My mother sacrificed a lot to raise me and my brother, but now both my brother and I are addicted, and now we both got this disease [HIV infection]. I wonder why I was named XX [meaning loyalty and respect for your parents], but I am the opposite. Sometimes I can see my grandmother and mother walk by our room, and my mother cries or talked to herself, I feel such a huge pain in my heart. (IDI3, 28)
Another PWID blamed himself for getting addicted to injecting drugs:
I think about myself a lot, about why I was so stupid when I was younger, how I got down that path [of injecting drugs], which made me infected. I am worried now – if I can ever get back to being healthy, if anyone would help me. (IDI5, 31)
Many felt useless, unable to contribute to the family’s economy or childcare, and lost hope. Living with HIV was constant in their mind—“Wherever I go, this disease [HIV infection] is on my mind.” (IDI38, 41)—which likely further contributed to their feelings of guilt. Some could not help thinking about the end—death—as an unavoidable consequence of this “disease.” One said:
I am always worried inside. . .. Afraid of dying. My kids are very young, while I am not sure if I am still living or will be dying tomorrow. (IDI1, 37)
There also seemed to exist a vicious cycle, where PWID got infected through injecting drugs, making them feel guilty and useless to their family, which in turn contributed to their declining health and increased desires to return to injecting drugs. One man summed this up:
There are times when I feel really desperate. I don’t see any values in living, I don’t want to continue living, and there is no future for me. I am just a heavy burden for my family. So I think I could go back to injecting drugs, giving up everything. . . I will die anyway [sad smile]. Everyone wants to live, but I will die anyway. (IDI20, 22)
Avoidance and self-isolation
In general, reports of self-isolation and avoidance of social interactions due to HIV were more common than those due to injecting drug use, either out of guilt for getting infected, or for mistaken fears of spreading the HIV, like this one: “I was very, very sad when I found out that I was positive. . . I quit my job. I often feel pity for myself. . .[omitted] At home, I can help my wife cook the rice or boil the water, but I let her cook other foods or do other work. I don’t dare do those things anymore.” (IDI8, 33). Despite being a college-educated man, this participant was still afraid of spreading the virus through cooking, which suggested that HIV misconceptions may remain common in the public. Some participants confined themselves within the limits of their home and avoid all interactions, which could potentially make their situation and health worse, mentally and physically.
Several men avoided having a partner or committing to a long-term relationship for fears that they could not become a meaningful part of anyone’s future.
She [my girlfriend] keeps in touch with me but I avoid her. I should avoid her so she can find a husband. I don’t have anything left to give her, to make plans with her. . . (IDI39, 33)
Another man echoed the sentiment:
I don’t think I can carry the burden of the family. Let say I got married, there would be another member of the family, I don’t think I can do my job as a husband, taking care of my family. . .. I think I am too weak, I am like this. . .. (IDI19, 33)
Only a few participants reported being somewhat accepting of the situation and willing to move on. They acknowledged that their mistakes, which got them infected with HIV, but now that ART treatment was available, allowing PLWH to continue leading a healthy and meaningful life, they would plan on doing so.
Discussion
This analysis showed that despite some declines in HIV-related stigma, stigma remained high for PWID living with HIV in Vietnam. Evidence of all 3 dimensions of stigma was prevalent and perceived to be from multiple sources: family, community, and health workers. Our interviews also suggested that there was a potential intersection between HIV and drug use-related stigmas and that the intersection varied across dimensions of stigma, consistent with previous studies in Vietnam.21,47 On the other hand, ART adherence was nearly universal in this sample, in part because ART medications could be picked up by someone in the family, thus reducing the potential of experiencing stigmatization in the public by patients themselves.
While HIV-related enacted and anticipated stigma seemed to have declined, enacted and anticipated stigma related to drug injection remained widespread. This finding is similar to those reported by Li et al 30 ; however, we went beyond the previous study by documenting possible intersections of different types of stigmas among individuals who were both HIV-positive and injecting drugs. We found that a person who was living with HIV might face the enacted stigma that was substantially magnified if he got infected through drug injection, compared to one not injecting drugs. A man who was infected with HIV through other types of transmission, for example, sexual intercourse with a sex worker, was more likely to be forgiven and sympathized, compared to one who got infected through drug injection. Enacted stigma reportedly came from multiple sources, including health workers at OPCs where PWID received treatment. While some participants justified such enacted stigma by the heavy workload of health workers, it is still possible that this structural barrier contributed negatively to the way patients were treated. Recent studies in Vietnam have also suggested that enacted and anticipated stigma was common among PWID, and that stigmatization by health care providers was an important barrier for PWID to access services.48-50 For example, health care providers often described patients using terms like lazy, unreliable and viewed PWID as unable to prioritize HIV treatment and care. 49 While our participants rarely reported explicit stigmatization from health care providers, many reported providers being silent, cold, or not allowing questions from patients. Such treatment could discourage patients from engaging in treatment and care. 51 Courtesy biases cannot be ruled out, thus stronger stigmatization from health care providers than reported as possible. While we did not investigate providers’ perceptions of PWLH who inject drugs, taken together this study and the current literature suggest a clear disconnection between PWID and providers’ views of challenges faced by PWID living with HIV to access ART. It is critical to close this gap to foster a supportive environment for PWID to access and stay in treatment and care.
Internalized stigma related to HIV and drug use, however, both remained high. Together, such co-existing stigma contributed to many participants blaming themselves for having injected drugs and brought HIV to their family and the community. Those who had disclosed their HIV status and drug-injecting behavior became even more depressed and regretful, while those who had not disclosed either status were more reluctant to do so. It should be noted, though, that everyone in our study had accessed ART treatment, which could have either spurred or been a consequence of HIV status disclosure within the family. As a result, we were not able to compare PWID whose HIV status was known versus unknown to family members like in Rudolph et al’s. 47
There are a few limitations in our study. A key limitation of this analysis is that data came from a study originally designed to assess ART adherence among PLWH who inject drugs. Consequently, our sample did not include PLWH who did not inject drugs or PWID who were HIV-negative. The sample design limited our abilities to compare stigma between these groups. However, our interview guides (see Appendix 1) included questions asking specifically about experiences and perceptions related to HIV vs. injecting drug use. Most of our participants were able to distinguish their experiences in this regard. Therefore, our data still provide useful insight into the intersecting stigma in this KP group.
Second, the transferability of our findings is limited, since the sample was small and purposively recruited from 2 OPCs, using specific criteria. Our findings are not transferrable to female PWID living with HIV, as they may have very different experiences with stigma and discrimination due to perceived gender roles.47,52 As female PWID account for only 5% of PWID in Vietnam, oversampling of them would be necessary to draw meaningful conclusions. Third, selection bias is possible as our participants were recruited from OPCs attendees. It is possible that their perceptions of stigma were very different from those not routinely attending or who have never attended OPCs, as well as those who had not disclosed their HIV status to families. Studies have shown that drug use-related stigma and the illegal nature of drug injection were significant barriers for users to get tested and access health services.15,53,54 In Vietnam, the government’s guidelines dictate that anyone in the KP groups who have tested positive for HIV will be immediately referred for ART treatment, 55 and ART retention has been consistently over 95%, 56 consequently we did not attempt to differentiate between PWID who had consistently been in treatment and those who had not since it would be difficult to find the latter group. We also did not examine stigma by the duration of treatment. 50 However, since our focus was on the co-existence and intersection of stigmas instead of a quantitative assessment of stigma, we believe that the study still makes important contributions to the stigma literature. Finally, social desirability and courtesy biases could not be ruled out.
Despite the limitations, the study has several important contributions to the current literature. First, it sheds light on the nuanced perceptions of 3 stigma dimensions not previously understood in a middle-income country with a concentrated epidemic. Second, our study suggested a potential intersection between stigma related to HIV with drug use-related stigma, which varied across stigma dimensions. Future studies should include comparison groups to allow assessment of stigma dimensions related to HIV only, injecting drug use only, or both. Still, our current study serves as a basis to inform the development of a conceptual model of intersecting stigma in Vietnam, which is critical for quantitative assessments of the influence of stigma dimensions on health outcomes. Our findings underline the need for stigma reduction strategies to be planned and well thought out with consideration of the operationalization of different dimensions of stigma within a population group.
Footnotes
Appendix 1
Acknowledgements
This study was conducted with the support of the United States Agency for International Development (USAID) under the terms of MEASURE Evaluation Cooperative Agreement AID-OAA-L-14-0004. The authors appreciate the support from the MEASURE Evaluation Project, USAID/Washington, USAID Mission in Vietnam, and Hanoi University of Public Health. The fieldwork could not have been completed without the support and collaborations of Nghe An Province’s Department of Health, and the outpatient clinics in Que Phong and Dien Chau districts.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted with the support of the United States Agency for International Development (USAID) under the terms of MEASURE Evaluation Cooperative Agreement AID-OAA-L-14-0004.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Note
An earlier analysis of this data was presented at the International AIDS Society Conference. Full citation is: Do, M., Le, H.H., Ho, H.T., Dinh, H.T., Truong, T.Q., Dang, T.V., Nguyen, D.D., and Andrinopoulos, K. (2018) “Influences of gender norms and gender roles on HIV service engagement in Vietnam.” Poster presented at the International AIDS Society Conference, July 23-27, 2018, Amsterdam, The Netherlands.
Author Contributions
All co-authors have contributed to the manuscript as outlined below.
Mai Do: conceptualization of the study, methodologies, data analysis, manuscript writing.
Hien Thi Ho: study administration, methodologies, data collection, data analysis, manuscript writing.
Ha Thu Dinh: data collection, data analysis, manuscript review
Ha Hai Le: study administration, data collectionTien Quang Truong: data collection
Trung Vu Dang: conceptualization, methodologies
Duong Duc Nguyen: conceptualization, methodologies
Katherine Andrinopoulos: conceptualization, manuscript review