
Abstract
In Vietnam, social health insurance (SHI) benefit package has been defined in a more explicit approach with the introduction of a regulation on the list of conditional reimbursed and non-reimbursed medical services. This paper aims to analyze the implementation results of this regulation from an economical perspective as well as the implementation challenges. Mix-method approach was employed. The quantitative component was employed to understand the implementation results. Desk study and qualitative components (2 inteviews with key informants from Ministry of Health; 6 discussions with key informants from provincial Social Security Offices and Departments of Health in Hanoi, Ho Chi Minh City, Hue, Tuyen Quang, Thai Binh and Soc Trang provinces; the other 23 discussions and 31 interviews with key informants from 23 selected hospitals) was employed to summarize the implementation challenges. The regulation seems to not able to mitigate the reimbursement of high-technology and expensive services in higher-level providers. There is a sign of increasing out-of-pocket payments for those regulated services in higher-level providers. It has also posed greater influence on lower-level providers in terms of the proportion of reimbursement amount rather than to higher-level hospitals. Applying World Health Organization’s 6 building blocks of health system to analyze the implementation challenges, we provide policymakers evidence to improve the regulation, as well as point out the relating health system weakness need to be strengthened.
Keywords
Introduction
Social Health Insurance (SHI) scheme was first introduced in Vietnam in 1992, marked by the implementation of a compulsory scheme for civil servants and pensioners. 1 The first Health Insurance (HI) Law No. 25/2008/QH12, approved by the National Assembly was promulgated in 2008 and then amended in 2014. 2 The implementation of SHI until now has obtained certain achievements in expanding the population coverage from 5% of the population in 1993 to 81% of the population in 2016; contributing increasing shares in total health expenditure from 5% in 1993 to 48% in 2016; increasing pooling of risk (from 61 provincial funds in 1992-1998 period to a single pool administred by the Vietnam Social Security (VSS) in 1998 onward) and introducing financial protections for vulnerable. 3
Under SHI scheme, insured members could receive their benefit in any health facilities that have contracted with the VSS. The contracted health facilities include both public and private hospitals with the dominance of the public providers. They are divided into 4 levels by administrative structure: central-level hospitals (offer highly-specialized teriary care), provincial-level hospitals and district-level hospital (offer teriary and secondary care), and commune health care centers (CHCs) (provide basic primary care and prevention services on an outpatient basis). The contracted providers are responsible for providing services for insured members and claiming the expediture with the VSS. Subsequently, the VSS reviews the claims and reimburses for the providers. Although it is considered as unsustainable mechansim,1,3 fee-for-service (FFS) (i.e. the provider is reimbursed for each service provided) remains the dominant payment mechanism from SHI fund to healthcare providers. In addition to FFS, capitation (i.e., the provider is paid in advance a predetermined fixed rate to provide a defined set of services for each individual enrolled with the provider for a fixed period) were applied only for primary care providers from 2004 4 and payment by diagnosis related group (i.e., the provider is paid at a fixed rate per discharge based on diagnosis, treatment and type of discharge 5 ) was defined by the 2008 HI Law but has never been implemented in practice accept during the pilot period in 2009. 1
The co-payment rate of 0% to 20% has been applied for insured members. To receive the maximum level of payment, each insured member is required to first attend their allocated ‘primary health care facility’ (i.e. district hospitals and CHCs) before referral to higher-level facilities. For insured members that bypass the referral system, a higher co-payment rate is applied, that is, 30%, 40% and 60% at district, provincial and central-level providers, respectively. 3 Insured members pay out-of-pocket (OOP) expenditure for co-payments and other uncovered services directly by using their incomes, savings as well as by cuting down on essential consumption (food, education and production means). 6 The share of OOP in Vietnam remains high in total health care spending, that is, 45% in 2018. 7
One of the reasons lead to the high OOP expenditure is discussed to be related to the benefit package – which is including nearly all expensive high-tech medical services without clear inclusion criteria. 1 The SHI benefit package in Vietnam is also based on an inclusive list that covers all ambulatory and hospital basic as well as advanced diagnostic, curative health services, and therapeutic services under the general guidance of HI Law. 2 It is believed to be a genrous benefit package compared to that provided in most other countries with similar income in the Asian region, 3 and lack of specific criteria for including or excluding services in the benefit package. This way of defining benefit package is refered as ‘implicit approach’ (i.e., no restrictions are expressly laid out and so most or even all services are provided in theory). 8 By contrast, in explicit approach, services to be covered or excluded are clearly defined, often via positive or negative list. 8 Without explicitly defining the benefit package, it is difficult for tracking the actual commitment of the government in delivery the healthcare service toward the goals of universal health coverage; controlling the healthcare cost; ensuring service quality; and responding to health policy priorities. 9 To address the above limitations, many countries in the world employing the explicit approach to define their benefit packages include European countries, 10 Latin American countries, 11 and other low- and middle-income countries 9 - regardless of whether they have tax-based or social insurance-based finance.
In Vietnam, we also observed the sign of the similar transformation with the introduction of Circular No. 35/2016/TT-BYT, promulgating the list of conditional reimbursed and non-reimbursed medical services (dated September 28, 2016) 12 and some related amendments in Circular No. 50/2017/TT-BYT (dated December 29, 2017). 13 Circular No. 35/2016/TT-BYT and Circular No. 50/2017/TT-BYT (hereinafter refered to as Circular 35/50) issued the list of conditional reimbursed and non-reimbursed medical services under 3 categories: Category 1 includes 15 expensive medical services with their detailed reimbursement conditions and rates; Category 2 includes 109 medical services with their detailed reimbursement conditions; Category 3 includes 16 non-covered medical services. Circular 35/50 was developed by Department of Health Insurance – Ministry of Health (MOH) as requested by the VSS to response to the fact that many healthcare services are unnecessarily overused. The initial goal of Circular 35/50 is to ‘control the reimbursment expenditure of medical services that are expensive and tend to be overused’ and ‘improving quality of healthcare services’, thus helping to ensure the efficiently use of the SHI fund. The Department of Health Insurance – MOH developed the draft Circular mainly based on meetings with medical experts. There is no document reported how the services are selected and how the reimbursement conditions are reviewed. After a period of implementation, there were questions raised about as if the implementation of Circular 35/50 has achieved the preset goals and what challenges hinder the implementation. Thus, this paper aims to analyze the results of the implementation of Circulars 35/50 from an economical perspective as well as key challenges relating implementation.
Methods
Mix method approach was employed, combining desk study, quantitative and qualitative components. The study was conducted from September 2018 until Jun 2019. Quantitative component was used to understand the results of policy implementation. Desk study and qualitative component were employed to summarize the challenges to policy implementation.
Desk study
We performed the review of published and unpublished literature by searching PUBMED database as well as using Google Scholar and manual search on the website of related international organizations (including World Bank (WB) and World Health Organization (WHO)) and related national organizations (MOH, Health Strategy and Policy Institute) using the main key words ‘social health insurance’, ‘benefit package’, ‘payment conditions’ and ‘reimbursement list’. We also performed the review of policy documents relating to the study as well as technical reports, meeting documents and other related documents provided by Department of Health Insurance – MOH and Vietnam Social Security (VSS). The literature was employed to describe the implementation results of Circular 35/50 and key challenges to implementation. Different technical reports as well as related documents provided by key informants from Provincial Department of Health (DOH) and hospitals were also summarized. We also collected the identified documents (e.g. related meeting minutes, response to the related dispatch) from key informants and had them clarified with key informants as necessary. We also expanded the search for relevant documents as suggested by key informants.
Qualitative component
We selected key informants who are experienced and knowledgeable in developing and implementing Circular 35/50 in both central and provincial-level using the purposeful sampling approach. We conducted 2 in-depth interviews (IDIs) with key informants from Department of Health Insurance, MOH (deputy director and senior staff). In 6 selected provinces (Hanoi, Ho Chi Minh City, Hue, Tuyen Quang, Thai Binh and Soc Trang), a total of 6 focus group discussions (FGD) was conducted with key informants from provincial social security offices (SSO) (head or vice head person from department of SHI inspection) and DOH (head or vice head person from related departments, such as department of planing and finance). In each province, we also selected 23 hospitals to visit. The hospitals were intentionally selected to ensure the diversity of types of providers (including central hospitals, provincial-level general hospitals, provincial-level specialized hospitals, district hospitals and private hospitals). A total of 23 FGDs were conducted with key informants in 23 visited hospitals (including director boards, head of finance and accounting departments, head of departments of planning and administration, head of clinical departments and head of para-clinical departments). Besides, 31 IDIs were also undertaken with key informants (including head of clinical and para-clinical departments, physicians, administrative nurses) from selected hospitals. A lead interviewer and a note-taker conducted FDGs and IDIs in person. FDGs were facilitated by a member of the research team with experience of moderating focus groups. Another research team member took notes in FDGs. Interviewers and note-taker for IDIs were well-trained for the study.
The preset open-ended questions were designed differently for FDGs with SSO/DOH and FGDs/IDIs in the hospitals. The general questions were addressed including: (1) What is the results of the implementation of Circular 35/50? (2) What are the implementation challenges? All FGDs were voice recorded while 27 IDIs were only taking notes (due to lack of permission for recording). The study was reviewed and approved by the Department of Health Insurance – MOH. Participants gave informed consent to prior the FGDs/IDIs.
Quantitative component
We used a pre-designed template to collect information (on the reimbursement results of medical services listed in Circular 35/50) from the VSS, 6 SSO in 6 provinces (Hanoi, Ho Chi Minh City, Hue, Tuyen Quang, Thai Binh, Soc Trang) and from 23 visited hospitals. Due to the limitation of information system and the time restriction in data collection, we only selected 100 medical services having the highest requested amount for reimbursement for collecting from the VSS. Besides, a questionnaire (to collect information on (1) the reimbursement results of medical services listed in Circular 35/50; (2) problems arise when implementing Circular 35/50 at the hospitals) was sent to 63 provincial DOHs via official dispatch. 146 hospitals in 49/63 provinces re-turned the completed questionnaire via email.
Data analysis
Quantitative data were imputed into prepared tables in Microsoft Excel version 10. Reimbursement data collected from different sources were compared to check for trustworthiness. Data were presented in undiscounted values in billion Vietnam Dong (VND). Records of FGDs/IDIs were transcribed while the notes from other IDIs were reviewed by the research team and both checked with senior staff from Department of Health Insurance -MOH for accuracy. The data from all FGDs and IDIs were analyzed manually using thematic analysis. The identified themes of the statements were illustrated by direct quotations (if available) from FGDs/IDIs, which were translated from Vietnamese. We employed the WHO’s six building blocks of health system, 14 in which focus on (1) governance; (2) service delivery, (3) health workforce and (4) health information system to analyze the related challenges to the implementation of Circular 35/50. Governance building block involves ensuring the existence of policy frameworks combined with effective oversight, coalition building, regulation, attention to system design and accountability. A well-performing health workforce is one that works in responsive ways, fair and efficient to achieve the best health outcomes possible, given available resources and circumstances. The service delivery building block is concerned with how inputs and services are organized and managed to ensure access, quality, safety and continuity of care across health conditions, across different locations and over time. A well-functioning health information system is one that ensures the production, analysis, dissemination, and use of reliable and timely information on health determinants, health system performance, and health status.
Results
Policy implementation results
We selected 100 medical services having the highest requested amount for reimbursement in 2018 to analyze the implementation results of Circular 35/50 (Table 1). Indeed, among those 100 medical services having the highest requested amount for reimbursement in 2018 nationwide, there are 9 medical services under Category 1 and 23 medical services under Category 2, accounting for 9.1% and 13.6% of the reimbursement amount requested, respectively. At central-level hospitals, there are 14 medical services under Category 1 and 14 medical services under Category 2, accounting for 14.8% and 12.9% of the reimbursement amount requested, respectively. At CHCs, 41 out of 100 medical services having the highest amount requested for reimbursement are defined in Category 2, which accounts for a large proportion, corresponding to 41.6% of the total amount requested for reimbursement. They are mainly rehabilitation services (typically, reflexology massage) and acupuncture services.
Summary of 100 medical services having the highest amount requested for reimbursement in 2018 by different levels of health facilities across the country.

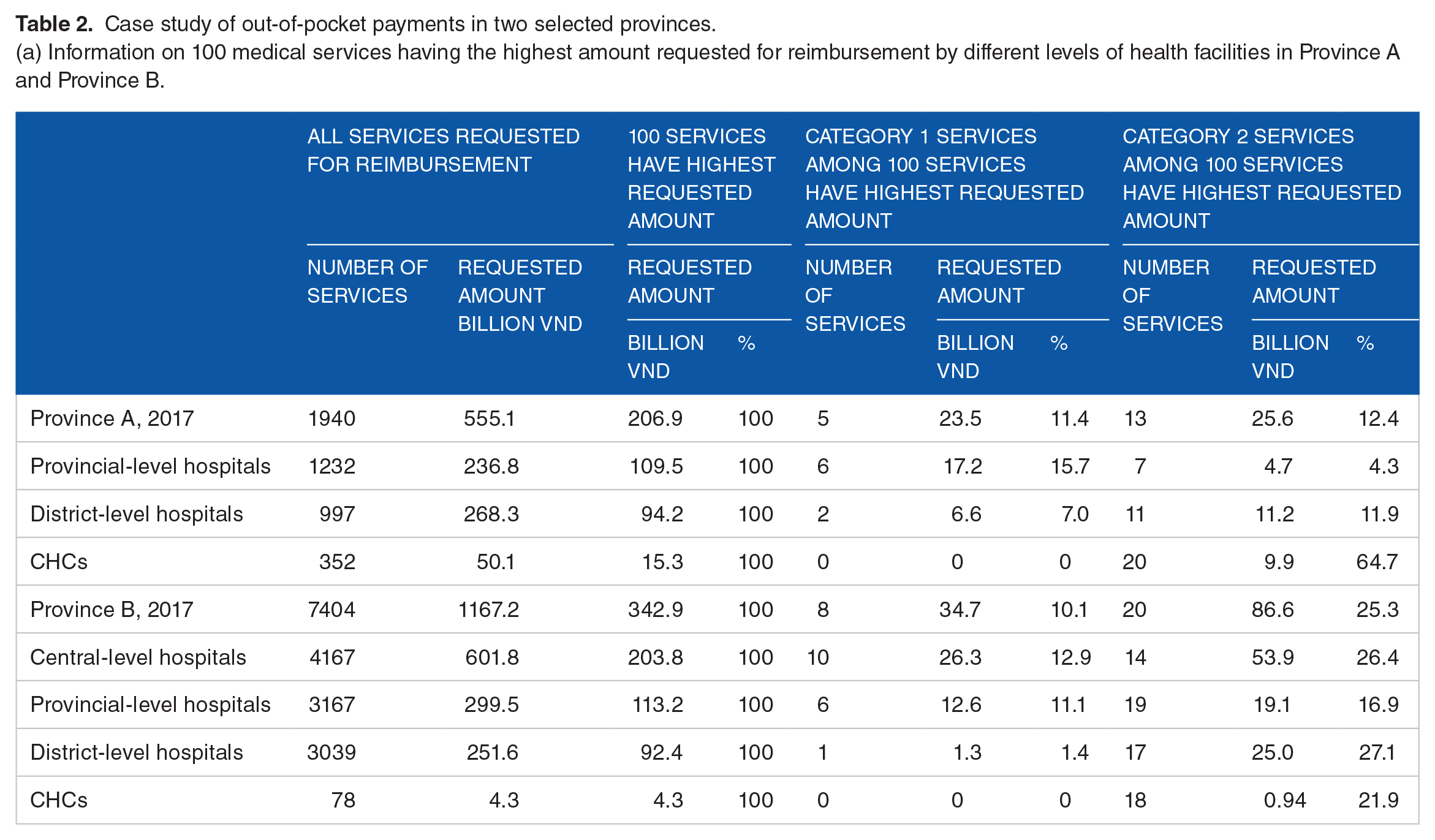
Table 2 presents a case study on the results of Circular 35/50 implementation in a provincial-level hospital (hospital A) in Province A and a central-level hospital (hospital B) in Province B (among 6 sampled provinces). Indeed, Table 2a provides general information on Category 1 and Category 2 medical services among 100 services having the highest requested amount in two provinces. The current situation in Province A and Province B was similar to the situation across the country that shown in Table 1 in the way that Category 1 services appear more frequently in provincial and central-level hospitals and proportion of reimbursement amount requested for Category 2 services was higher in district-level hospitals and CHCs. Table 2b provides detailed information on OOP payments the in the 2 selected hospitals. The total reimbursement amount hospital A requested the SSO paying for all medical services was VND 75,754 million while the total OOP was VND 103,844 million. It means for every VND 1 hospital A requested for reimbursement, patients paid OOP of VND 1.37. For Category 1 and Category 2 services, for every VND 1 hospital A requested for reimbursement, patients paid OOP of VND 2.15 and VND 3.57, respectively. Similarly, for hospital B, we observed similar trend with the rate of OOP in Category 1 services (2.35:1) and Category 2 services (1.38:1) is considerably higher compared to other services (0.18:1).
Case study of out-of-pocket payments in two selected provinces.
(a) Information on 100 medical services having the highest amount requested for reimbursement by different levels of health facilities in Province A and Province B.
(b) Information on OOP payments in two selected hospitals in province A and province B.

Including copayment for services covered in the SHI benefit package and direct payment for uncovered services.
Until 31/7/2018.
Challenges of Policy Implementation
Challenges relating governance
Unfavourable policy environment to implement Circular 35/50
Discussion with key informants from MOH and DOH revealed that the broader health financing context, i.e. the hospital autonomy policy for particular, is one of the reasons that Circular 35/50 not able to mitigate the use of Category 1 and 2 services in central and provincial-level hospitals. Along with the hospital autonomy policy, the current dominant provider payment method of FFS allows hospitals to increase the utilization of services in general and Category 1 and 2 services for particular.
‘the more services they (the hospitals) provide, the more revenue they earn to cover their expenditure. They have no benefit to control the use of high-technology medical services’ (IDI, male, MOH) ‘no matter how many conditions are required in the circular, they (the hospitals) have to implement the autonomy policy. They will try to satisfy all requirements to have the services reimbursed because their main revenue is from health insurance’ (FGD, DOH, province 2)
Moreover, qualitative results suggested that autonomous hospitals have incentives to guarante their revenue by covering the unreimbursed amount by OOP from patients: ‘in case it is difficult to be reimbursed by the VSS, they (the hospital) will let the patients pay by themselves’ (FGD, DOH, province 2)
According to a report of a provincial general hospital (province 6), the number of documents regulating the reimbursement of benefits package is substantial, particularly, the hospital’s archive from 2012 onwards has a total of 274 different documents including 106 documents from the MOH and 274 documents from the VSS regulating the health services reimbursement under SHI scheme. The existence of a large number of different regulatory documents from MOH and VSS leads to fragmentation and inconsistency, thus, Circular 35/50 may not meet its goals because its implementation has been affected by and conflict with other policy documents: ‘The documents of the Ministry of Health and the Department of Health are too many and there are some overlapping and inconsistent contents, so it is difficult for health facilities to apply and it is difficult for us to monitor. . ..’ (FGD, DOH, province 3) ‘the documents are still overlapping, conflicted, and inconsistent. Not mentioning the VSS have also introduced their own documents without agreement with us (ministry of health)’ (FGD, DOH, province 4)
Controversial content of Circular 35/50
The results of IDIs/FGDs as well as the questionnaire returned by 146 health facilities show that many arguments raised due to the controversial instructions of Circular 35/50 on the reimbursement conditions. In particular, rehabilitation services were mentioned with the highest frequency of complaints (26% of complaints from the hospitals) because of the ambiguous instructions, such as the unclear definition of the similar treatment mechanism (e.g., parafin wax bath and infrared therapy are consider having the ‘same mechanism’ as they are both categorized as thermotherapy), and the limitation on number of services to be paid in a hospitalization day: ‘the Ministry of Health has not specified any definition on the technical services of the same effect mechanism for implementation, so it is problematic to apply. Instruction on paying no more than 6 technical services in a day is very difficult to implement because each technique has different characteristics and patient’s response to treatment differently’ (FGD, general - provincial hospital 1)
Hemoglobin A1c test (Hba1c) is another example. It was mentioned with the second highest frequency of complaints (22% of complaints from the hospitals) because of limitation on the time frame of payment (no payment for tests within the past 3 months): ‘It is very difficult for Hbac1C to be tested only once in 3-month period for a pregnant woman diagnosed with gestational diabetes. While (Hba1c) is quite simple, cheap, necessary for good monitoring, the regulation of once-in 3 months is not possible’ (FGD, general - provincial hospital 5)
Quality of policy development
Discussion with the informant from MOH shows that there are no criteria and process to include or exclude a service in Circular 35/50, and this poor quality of policy development may lead to undesirable effect of Circular 35/50: ‘we drafted the circular based on the list of services that are belived to be overused, provided by the VSS. We have no information on the burden of related disease or cost-effectiveness or cost of the services. The conditions were developed based on meeting with expert from central hospitals. . .’ (IDI, male, MOH)
Besides, there are also many comments that health facilities have not paid attention to comment on the draft version of Circular 35/50 before regulating/amending: ‘The health facilities feedback very slowly when being consulted on the draft document. It is nearly impossible to get responses of over 50% (more than half of the health facilities across the country). Often the documents have been sent 2-3 times to get sufficient required comments to be revised’ (IDI, female, MOH)
Lack of mechanism to monitor the implementation of Circular 35/50
According to key informants, the MOH and DOH do not have enough information in monitoring the implementation of SHI policies in general and Circular 35/50 in particular: ‘We (the health sector) have no detailed information on reimbursement as the VSS. When the MOH ask for results and problems in implementing Circular 35/50, we sent dispatchs to hospitals and wait for response to document and report to the MOH’ (FDG, general – provincial 2)
Besides, the lack of accountability and transparency in the reimbursement process is also a challenge to monitor the implementation of Circular 35/50: ‘The health insurance does not reimburse to our hospital (VND 5.7 billion), does not answer what is wrong to be added, but requests the hospital to search the mistakes by themselves, so it is very time consuming, and sometimes the hospital does not know how to do it, and it happens repeatedly’ (IDI, health staff, general – provincial hospital 2)
Challenges relating service delivery
Although Circular 35/50 aims at mitigating the use of high-technology services, it is difficult to achieve this goal due to the fact that the higher-level of hospitals, that is, central and provincial-level ones tend to provide more high-technology services to commensurate with their reputation, thus it also leads to the increase in OOP: ‘It is difficult to control high-level hospitals to not use the high-technology and expensive services because providing those services help them to confirm their reputation, to improve treatment quality, to increase their revenue by providing those services upon request, updated with the latest inovation in the word. . .’ (FGD, provincial 2) ‘the more expensive services they provide, the more contribution from the patients’ (FGD, provincial 5)
According to FDGs and IDIs, Circular 30/50 has some detailed conditions for reimbursement based on the level of healthcare providers. For example, a service, namely, therapeutic hypothermia, is only reimbursed if performed in a special level hospital or other hospitals approved by the MOH; other service, namely joint injection, must be done by provincial-level or higher-level hospitals to be reimbursed. Key informants discussed that the way of requirment might tighten the service provision in lower-level hospitals and continue to increase the provision in higher-level hospitals.
Challenges relating health workforce
Key informants discussed the challenges relating healthcare workforce in lower-level hospitals to meet the requirement of Circular 35/50. Although Circular 35/50 aims at improving quality of healthcare services, it led to the challenges that the lower-level health facilities are not able to provide the services: ‘Circular 35/50 regulates many conditions relating the healthcare workers that deliver the services which are commonly providing in district and commune health centers. Circular 35/50 greatly affect the lower-level hospitals in the way that they could not reimburse the services because we do not have the doctors that are qualified with the requirements. It takes time for healthcare workers in district hospitals and commune health center to satisfy the condtions listed in Circular 35/50’ (IDIs, female, MOH)
Challenges relating health information system
Qualitative results suggested that limitation of the health information system at country-level as well as at facility-level lead to the fact that the MOH could not have enough information to monitor the policy implementation: ‘Only VSS has detailed information on reimbursement for the whole countries, the health sector do not have access to the data. Even we could use the VSS database to evaluate the results of cicular 35/50, it is still not enough because VSS does not have data on OOP. Actually, the MOH also does not have any mechanism to record the information on OOP’ (IDI, female, MOH)
Besides, key informants pointed out the challenges with the information on burden of disease, costs, and cost-effectiveness of medical services in order to develop a good benefit package: ‘There is no information on the cost-effectiveness of the medical services in supporting us to develop or to amend Circular 35/50. When developing detailed reimbursement conditions for each medical service, we consulted a professional advisory board which includes mainly the healthcare professionals, but rarely the health economists’ (IDI, male, MOH)
Discussion
The list of medical services in Circular 35/50 could be considered as a negative list – meaning a list of services that will not be covered or covered under specific circumstances by SHI scheme. The development of Circular 35/50 is inevitable to develop a SHI benefit package of medical services in a more explicit approach. This is aligned with the trend in developing benefit package in other countries9,15 as well as suggestions of experts for Vietnam context. 16 By explicitly regulating the list of uncovered or conditionally covered by SHI, it helps to identify whether SHI fund is being spent ‘value-for-money’ on services that create maximum benefit for society; support adherence to budget limits; develop a precondition for reducing variations in care and outcome by specifying the services to be delivered, etc. 17 In Vietnam, Circular 35/50 was developed and implemented with the initial purpose of ‘controlling the reimbursement expenditure of medical services that are expensive and tend to be overused’ and ‘improving quality of delivering healthcare services’. However, the results from this study show that Circular 35/50 migh have undesirable results.
Firstly, we observed that many expensive services regulated in Category 1 of Circular 35/50 (e.g., positron emission tomography – computed tomography (PET-CT), CT, phacoemulsification, etc) and in Category 2 (e.g., pulse contour cardiac output (PiCCO), hemodiafiltration (HDF), etc.) are commonly delivered more often in higher-level hospitals. However the qualitative results from this study showed it is challenging for Circular 35/50 in mitigating the use of regulated expensive services in higher-level hospitals. Indeed, the policy environment including the hospital autonomy policy, the current provider payment method of FFS, the preference of higher-level hospitals in providing high-technology and expensive services to ‘confirm their reputation’ are believed to be the main reasons why higher-level hospitals continue to increase the use of high-technology and expensive service in general and the regulated services in Circular 35/50 for particular.
Secondly, examining OOP expenses in 2 higher-level hospitals shows the trend of increasing OOP expenses for services defined in Category 1 and Category 2 compared to services not regulated in Circular 35/50. This observation was confirmed by key informants that Circular 35/50 causes health facilities to ‘claim unreimbursed services through user fees from patients’. In this case study, the providers seem to have stronger incentives to claim the cost of services listed in Circular 35/50 through OOP payments since it is difficult to satisfy all reimbursement conditions regulated in Circular 35/50. Other authors discussed about this issue in the way that under the current financing system, providers have faced strong incentives to provide the most profitable services covered by SHI or provide services not covered by SHI through user fees from patients.18,19 Most updated publication by Lee et al, 20 employing a health system community survey collected between 2015 and 2017 in 2 districts in Vietnam, also pointed out the weak role of SHI in decreasing the impact of utilizing higher-level facilities. The authors discussed that patients’ preference for higher-level facilities under the context of hospital autonomy policy, FFS payment mechanism have been resulting in high OOP expenditure. 20 To be effectively implemented, policy on SHI benefit package in general and Circular 35/50 for particular need to be carefully design to address the potential impact of broader policy environment.
Thirdly, data on 100 medical services with the highest amount requested for reimbursement across the country as well as in visited provinces have shown that Circular 35/50 have a greater influence on the lower-level providers, that is, commune healthcare centers in term of the total amount requested for reimbursement. Moreover, Circular 30/50 has some detailed conditions for reimbursement which is in favour of the higher-level hospital rather than the lower-level hospital (e.g. joint injection must be done by provincial hospitals or higher-level hospitals to be reimbursed). Besides, in order to improving the services delivery, Circular 35/50 have many requirements on the healthcare workforce. However, it is believed to be very challenging for the lower-level providers to imediately satisfy all of these requirements. In the short run, both of the issues might lead to the reduction in services delivery in lower-level hospitals rather than improvement of services delivery.
Moreover, applying WHO’s 6 building blocks of a health system, 14 we also found other challenges to the implementation of Circular 35/50. One of the profound challenges is that Circular 35/50 might be conflict with other policy documents. The detailed instruction of Circular 35/50 is also belived to be confict with other available policy documents as well as available guideline of medical procedure. The conflict is easy to understand because of the existence of a large number of different regulatory documents from MOH and VSS related to the SHI reimbursement as presented in the result. Other example is that 41 out of 100 services having the highest amount requested for reimbursement are defined in Category 2 are mainly rehabilitation services and acupuncture services. These services are mostly overlapped with the basic package of healthcare services for grassroot level in Circular 39/2017/TT-BYT dated October 18, 2017. This fragmentation and inconsistence problems might caused by the design failure and institutional fragmentation discussed by World Bank. 19 In the short run, this issue needs to be solved as suggestion by the World Bank by regularly review the body of laws and regulations (decrees, circulars) and analyzing their consistency, validity, and possible contradictions, then, to revise, consolidate and harmonize HI regulations. 19 In the long run, promoting a coherent decision making condition is fundamental for good SHI governance. 19
Other challenge relating controversy instructions of Circular 35/50 that mentioned in the results may stem from the quality of policy development. The development of Circular 35/50 was lack of formal process to develop the benefit package, lack of agreed criteria to include or exclude a service in benefit package, lack of throughout pilot assessment to consider the potential impact of the policy as well as lack of the engagement of stakeholders, that is, health care providers. This might be the main reasons lead to the controversial debate around the detailed instructions of Circular 35/50. In the near future, it is important to have agreed process of developing and revising the benefit package in general and the negative list of medical services, that is, Circular 35/50 for particular. The development and revision process have been well discussed in literature.17,21 Evidence on cost-effectiveness of medical servies, information on burden of disease is urgently required to aid this kind of process.
Finaly, without closely monitoring the implementation’s results, a policy could not meet desirable goals as in the case of Circular 35/50. The limitations of current health information system on reimbursement data make it more difficult to build up a good monitoring process. Thus, urgently improving the health information system is prerequisite to ensure the production, analysis, dissemination and use of reliable and timely information on reimbursement and service utilities to aid the monitoring and policy implementation.
Strengths and Limitations
This is one of the rare and detailed reviews on the results of a SHI-related circular as suggested by World Bank. 19 Due to the limited time, resources and availability of data, we only focused on analyzing the implementation results of Circular 35/50 – which regulates the list of uncovered and conditionally covered medical services by the SHI scheme (negative list) – from an economical perspective, but not reviewing and evaluating the whole SHI benefit package from a broader perspective. Along with the health financing system reform in Vietnam in the future, it is necessary to further study on the possibility to apply the well-known framework in developing benefit packages in Vietnamese context.
The process of evaluating the results of Circular 35/50 implementation shows certain limitations on searching and generating information based on reimbursement database. Especially, due to the lack of reimbursement data before the introduction of Circular 35/50, it is impossible to fully understand the implementation results of Circular 35/50. Ensuring the ability to explore reimbursement data in a synchronous manner across the country over time, ensuring the accuracy of technical service coding, the accuracy of disease diagnostic coding, etc. play an important role to support further policy review and policy making process.
Conclusion
The introduction of a list of unreimbursed and conditional reimbursed services by SHI (regulated by Circular 35/50) in Vietnam is inevitable in order to develop a benefit package in a more explicit approach. However, it is challenging to mitigate the reimbursement of high-technology and expensive services in higher-level providers. There is also a sign of increasing OOP for those conditional reimbursed services regulated in Circular 35/50 from 2 observed central and provincial-level hospitals. Moreover, Circular 35/50 seems to have greater influence on the lower-level providers (in terms of the proportion of amount reimbursement requested for services regulated in Circular 35/50 to the total amount reimbursement requested for all services) rather than to higher-level hospitals. It also poses great challenges to lower-level providers in terms of fulfilling the human resources related requirements regulated in Circular 35/50. It is necessary to have an agreed process of developing and revising the health benefit package in general and the negative list of medical services, i.e. Circular 35/50 for particular, in which carefully considering the potential impact of broader policy environment. Health information system also needs to be improved to aid the process as well as to closely monitor the policy implementation.
Footnotes
Funding:
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was financially supported by Asian Development Bank (ADB) under the Project on Strengthening the Policy and Institutional Framework of Social Health Insurance.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NTH and NTHg contributed to the design and implementation of the research. All authors contributed to the analysis of the results and to the writing of the manuscript.