
Abstract
Home care is an important service for persons with neurological conditions, but little is known about factors affecting health care costs in this setting. Using administrative data collected with the Resident Assessment Instrument for Home Care (RAI-HC), this study identified factors associated with home care costs for recipients of home care services with Alzheimer disease or related dementias, multiple sclerosis, and/or amyotrophic lateral sclerosis. As part of this study, the effectiveness of the Resource Utilization Groups for Home Care (RUG-III/HC), a case-mix classification system developed for the RAI-HC, in predicting care costs for this population, was also tested. Clinical characteristics indicative of greater disease severity had high levels of significance in predicting home care costs. In particular, the RUG-III/HC was highly predictive of home care costs for 3 neurological conditions, indicating the validity of this case-mix system for this population. With the increasing prevalence of neurological conditions and demand for home care services, future studies should continue to focus on identifying specific predictors care costs for those with neurological conditions in this care setting.
Introduction
Neurological conditions account for 11% of the global burden of disease in developed countries 1 The disease burden is substantial due to the chronic and progressive nature of these conditions, which can result in loss of function, debilitating pain, and reduced quality of life.1-4 In Canada, an estimated US$9 billion is spent annually on drugs, hospitalisation, and physician care for neurological conditions. 2 The costs associated with these conditions are expected to increase in coming years as their prevalence rates continue to grow. 1 Therefore, it will be increasingly important to understand and manage factors affecting costs of care for these conditions.
Non-acute forms of care (eg, home care) are required for many neurological conditions due to functional loss over the course of disease.5,6 Publicly funded home care in Ontario is universally available at no cost to those with care needs that can be met to support remaining in the community. Care coordinators determine service eligibility and perform clinical assessments on those expected to require services for greater than 60 days using the Resident Assessment Instrument for Home Care (RAI-HC). Reassessments are conducted every 6 to 12 months, or sooner if there is a non–self-limiting change in health status requiring an adjustment to the care plan. Community-based services are provided through contracted agencies including nursing, physiotherapy, occupational therapy, speech-language therapy, social work, nutrition, and personal support.
Estimates of the prevalence in home care of neurological conditions such as Alzheimer disease and related dementias (ADRD) and multiple sclerosis (MS) are much higher than in general settings, at 25.6% and 1.8%, respectively. 7 In comparison, the prevalence of ADRD in the general population is estimated at 0.6% and 0.3% for MS. 8
Despite the sizable proportion of home care clients with neurological conditions, relatively little is known about the costs of services they receive and factors affecting their costs of care. Health care needs can be understood using the Andersen-Newman 9 framework, which categorises factors contributing to health service use as predisposing factors (eg, age, sex), enabling factors (eg, income, access to health care), and need factors (eg, disease diagnoses, symptoms). Outside of home care, need factors such as disease severity and progression of illness over time have been found to affect care costs for those with neurological conditions.10,11 Similar factors have also been identified in the home care setting for persons with other conditions such as colorectal and breast cancers.12,13 A previous study using the Andersen-Newman framework for health care utilisation found that need and enabling factors had the greatest significance in predicting service use in home care. 14
The purpose of this study was to determine specific clinical and demographic characteristics affecting home care costs in Ontario home care clients with ADRD, MS, and amyotrophic lateral sclerosis (ALS). These conditions were identified as priority conditions for research as part of the National Population Health Study of Neurological Conditions in Canada (NPHSNC). 15 In addition, the conditions vary in their prevalence, etiology, and impact on the individual and their caregivers. Alzheimer disease and related dementias is among the most common of neurological conditions, with the potential of serious impairment in both cognitive and physical functioning over time, but with a typically later onset in the life course. 16 Amyotrophic lateral sclerosis is one of the most severe neurological conditions, affecting physical functioning rapidly and resulting in a relatively short life expectancy.17,18 Multiple sclerosis is associated with substantial disease burden due to its relatively young age of onset combined with long-term increasing physical impairment, but less cognitive impairment than ADRD typically. 19 As in prior studies, it was expected that need factors indicative of disease severity and progression of illness would be associated with home care costs for neurological conditions. This study was funded by the Public Health Agency of Canada as part of the NPHSNC.
Methods
Setting and data source
The present study involved a secondary analysis of home care assessment data collected as part of the Canadian Staff Time Resource Intensity Verification (CAN-STRIVE) project. Costing was done using both societal and payer perspectives. Data were obtained from a centralised Ontario repository representing all public home care, and included RAI-HC assessments and standardised administrative records. In total, the analytic data set included 435 141 assessments of home care clients between April 2005 and June 2008 with assessment records linked to billing data for home care services. Multiple assessments for individuals were included as part of these data to capture a more continuous mix of characteristics and costs over time. These linked data included only assessments administered in home settings, and excluded assessments for individuals living in congregate care settings where formal care provided outside of home care was expected. At the time these data were collected, home care was organised into 14 Community Care Access Centres (CCACs), which were single point entry agencies in which care coordinators were responsible for assessing client needs and contracting appropriate home care services from provider agencies in response to those assessments. Ethics approval for this study was obtained through from the Office of Research Ethics at the University of Waterloo (Project #18599).
Study Population
Home care clients with a diagnosis of ADRD, ALS, or MS were included in this study. Diagnosis of ADRD and MS was identified from a pick list in the disease diagnoses section of the RAI-HC. Persons with an ALS diagnosis were found using the ALS ICD-10 code (G12.2) in a write-in section that is also found in the disease diagnoses section of the RAI-HC. The validity of these diagnostic codes has been confirmed elsewhere. 20 A comparison group was also created for the descriptive portion of this study that included persons with other neurological conditions, including cerebral palsy, epilepsy, Huntington disease, muscular dystrophy, Parkinson disease, stroke, spinal cord injury, and traumatic brain injury. This group was identified using a combination of pick list items and ICD-10 (International Classification of Diseases, Tenth Revision) codes using the approach described by Foebel et al. 20
Measures
The selection and operationalisation of variables used in the analysis was based on a review of the case-mix literature as well as publications related to the Andersen-Newman model. In both cases, the number of publications related to costs in home care is very limited, so identification of potential variables was also informed by clinical feedback obtained from stakeholder consultations done as part of the larger National Population Health Study of Neurological Conditions.
Cost variable
Weekly formal care costs were calculated by aggregating service episodes from the day of the RAI-HC assessment until discharge, RAI-HC reassessment, or 13 weeks, whichever occurred first. Services had to be provided in at least 3 of those weeks. Formal care costs included billings for nursing, personal support, physical therapy, occupational therapy, speech-language therapy, social work, dietetics, and respite services. Some costs such were excluded because they were unavailable (eg, care coordinator time), not incurred by the CCAC (eg, medications are covered by the province), minor expenditures (eg, equipment rental), or unrelated to client characteristics (eg, travel time). Of these exclusions, the lack of data on care coordinator is probably the most substantively important limitation of the measure used. Median wage rates for each service at the time of the study were applied to visits or hours of service to determine formal direct costs. Informal direct care costs were calculated by applying an hourly rate equivalent to half the median wage rate of personal support services to the hours of activities of daily living (ADL) and instrumental activities of daily living (IADL) support reported by informal caregivers in the RAI-HC over a 7-day period, as has been done in similar studies.21,22 The total average weekly service costs were the sum of formal and informal care costs.
Predictor variables
Characteristics of clients with ADRD, ALS, and MS that could reasonably be assumed to have an impact on care costs for that condition were considered as predictors of care costs. A list of these variables can be found in Table 1. These characteristics were categorised as predisposing, enabling, and need variables based on the Andersen-Newman model of health care utilisation. Most of the variables included in this study were need factors comprising clinical characteristics or functional limitations associated with ADRD, ALS, and MS. Only characteristics thought to have an impact on care costs present in the RAI-HC assessments were considered for this study.
Variables of interest identified for inclusion into multivariate models.

Abbreviations: ADL: activities of daily living; IADL: instrumental activities of daily living.
Predisposing and enabling factors were drawn from RAI-HC assessments. Predisposing factors are those pre-existing traits that could increase or decrease the person’s service utilisation independent of need. The 2 predisposing variables considered here were age at the time of assessment (years) and the client’s sex. Enabling factors are those that can act as barriers or facilitators to access to needed services. Cohabitation with a support person and the geographic region of the client’s resident were used as enabling variables.
Need factors include both objectively and subjectively defined indicators of the persons illness level, health status, or disability that would be the basis for requiring health services. The models reported here used a combination of widely used interRAI scales as well as individual items from the RAI-HC. The scales that were used included the Cognitive Performance Scale with values from 0 to 6 measuring cognitive function,23,24 ADL Hierarchy Scale with values from 0 to 6 measuring physical disability, 25 Depression Rating Scale with values from 0 to 14 measuring depressive symptoms,26,27 Pain Scale with values from 0 to 3 measuring the frequency and intensity of pain, 28 IADL Capacity Scale with values from 0 to 6 measuring capacity to perform IADL, 29 and the Health Status Index (HSI) with values ranging from −0.03 to 1.00 measuring preference weighted health-related quality of life.30,31 In all cases except the HSI, higher scores indicate more severe impairment.
The Resource Utilization Groups for Home Care (RUG-III/HC) case-mix classification system developed for the RAI-HC21,22 is a need measure of particular interest because it is a composite measure of clinical characteristics expected to predict costs of home care. The RUG-III/HC classifies patients into 23 groups more than 7 clinical categories with similar combined formal and informal resource use and clinical descriptions.21,22 Each of the 23 groups have corresponding ratio-level case-mix index (CMI) values that describe mean resource utilisation for a group relative to the mean resource utilisation for the entire population. For this study, CMI values based on the combined costs of formal and informal care were used. The validity of the RUG-III/HC for classifying Canadian home care clients into relatively homogeneous clinical and resource intensity groups has been confirmed. 21
Statistical Analyses
Statistical analyses were conducted using SAS version 9.2 (SAS Inc., Cary, NC, USA). Care costs, CMI values, and sample characteristics were described using means and frequency procedures. Multivariate linear regression was used to identify factors affecting care costs for the 3 conditions. The regressions were performed independently for each of the 3 conditions using manual backwards elimination as well as manual specification of final models to control potential order of deletion effects related to collinearity. The models were assumed to be robust as analyses were conducted on large population-level data. However, as cost distributions are heavily left-skewed, the multivariate regression models were also tested using log-transformed costs. Once the final models were established, separate multivariate regression analyses were done to measure the independent explained variance for predisposing, enabling, and need factors. In addition, a model that used only RUG-III/HC CMI values was run to provide a baseline comparison of how much variance is explained by that case-mix system alone.
Most of the individual items from the RAI-HC that were used as predictor variables were treated as binary variables. The scales that were examined were treated as continuous measures in the regression models for convenience of displaying their effects in models with large number of covariates. Some of these scales are ratio-level measures with equal distances between points and meaningful values of 0 (eg, RUG-III/HC, HSI), but other scales are arguably ordinal measures where the distances between points may not be equal. In those cases, it may have been more appropriate to treat the scale as a ‘class’ variable; however, this would probably not have substantively changed the key findings and would have made the tables exceedingly lengthy.
Results
There were 70 061 assessments with an ADRD, MS, or ALS diagnosis on record. Alzheimer disease and related dementia was found in 59 310 assessments representing 25 901 individuals, ALS was present in 991 assessments representing 452 individuals, and MS was present in 9946 assessments representing 3309 individuals. The average age of individuals for ADRD, ALS, and MS was 82, 63, and 58, and the proportion that was female was 63.9%, 53.8%, and 75.5%, respectively. The comparison group comprised 273 202 individuals, of whom 71.7% were female.
Persons with ADRD, ALS, and MS were more complex than persons in the comparison group. Larger proportions of our study population had physical or functional limitations or had greater levels of limitations as compared with the comparison group. Those with ADRD, ALS, or MS were more likely to have at least some cognitive impairment, incontinence, and difficulty with expression, as well as moderate to severe ADL and IADL limitations. Similarly, individuals with the 3 neurological conditions were also more highly concentrated in the 3 highest resource intensity RUG-III/HC categories (Special Rehabilitation, Extensive Services, and Special Care). Additional supplementary information on the distribution of characteristics across groups is available on request.
The mean total weekly cost of home care services for the ADRD population was US$593.32 and the mean CMI was 1.40. The mean cost for those with MS was US$574.92, although the mean CMI was higher than the ADRD value at 1.52. The ALS population had the highest mean cost (US$898.41) and CMI (1.77) of the 3 conditions. The comparison group had a lower mean cost and CMI (US$337.16 and 0.87, respectively).
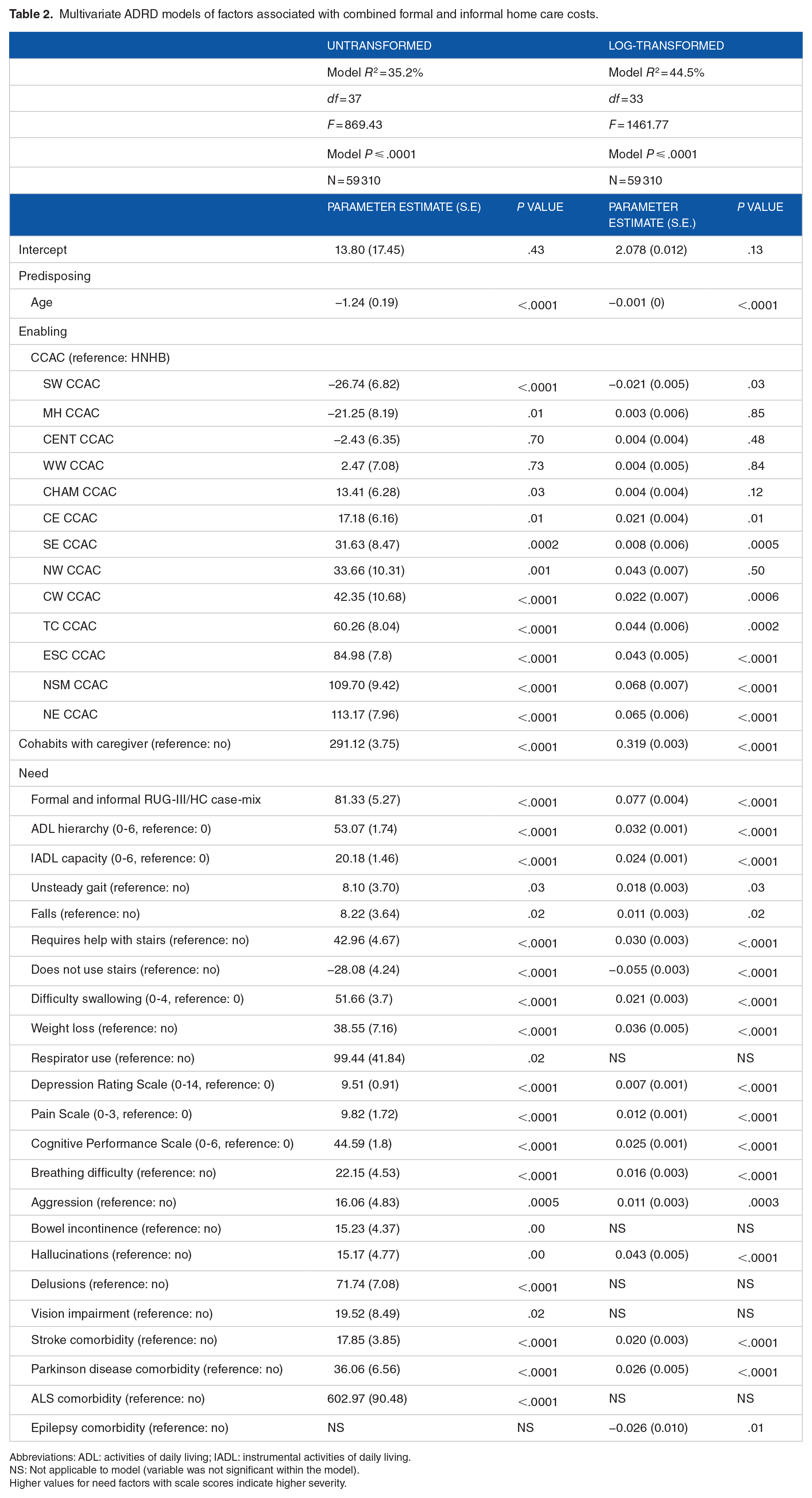
Table 2 shows the results of the untransformed and log-transformed models for ADRD. Results were similar in both models, although the explained variance was considerably higher when cost was log-transformed. Most variables were significant in both models. Many of the need factors identified have been known to complicate care for those with ADRD, and indeed, most covariates were associated with increased care costs. One of the factors most strongly associated with higher cost in both models was cohabitation with a caregiver, an enabling factor.
Multivariate ADRD models of factors associated with combined formal and informal home care costs.
Abbreviations: ADL: activities of daily living; IADL: instrumental activities of daily living.
NS: Not applicable to model (variable was not significant within the model).
Higher values for need factors with scale scores indicate higher severity.
Two untransformed and 2 log-transformed models were identified for those with ALS (Table 3). Using backwards elimination, 2 untransformed and 2 log-transformed models were identified. As each pair of models had virtually identical levels of explained variance, both sets of models were reported here. In some cases, predictor variables were significant in the untransformed models, but not in the log-transformed ones (eg, difficulty swallowing, breathing difficulty, tracheostomy, ADRD comorbidity). In other cases, issues related to multicollinearity may have meant the significance of predictor variables dependent on the other covariates present. For example, in the log-transformed models, the following variables were included in only one of the 2 options: help with stairs, does not use stairs, Cognitive Performance Scale, bowel incontinence, hallucinations. In the non-transformed models, unsteady gait and IADL capacity scale appear in one, but not the other model. As with ADRD, higher levels of explained variance were found in the log-transformed models, although the difference was smaller. Significant enabling and need factors were found across all models, but predisposing characteristics were only significant in the untransformed models. Across models, covariates in the ALS models that were positively associated with costs had larger increases in care costs than found in the ADRD models. Specifically, cohabitation with a caregiver and respirator use were present across all 4 ALS models, and in all 4 models, were strong contributors of cost.
Multivariate ALS models of factors associated with combined formal and informal home care costs.

Abbreviations: ADL: activities of daily living; IADL: instrumental activities of daily living.
NS: Not applicable to model (variable was not significant within the model).
Higher values for need factors with scale scores indicate higher severity.
The results of the MS models can be found in Table 4. No predisposing variables were significant in these models. Again, the explained variance for the log-transformed model was higher than the untransformed model and cohabitation with a caregiver was associated with large increases in care costs. An increase in HSI (indicating better health) also appeared to be associated with very large reductions in care costs. However, it is important to note that valid HSI scores are between −0.03 and 1 so that an increase of 1 on the HSI scale would represent a difference in health-related quality of life from death or worse than death to perfect health. A greater number of variables were negatively associated with care costs in the MS models.
Multivariate MS models of factors associated with combined formal and informal home care costs.

Abbreviations: ADL: activities of daily living; IADL: instrumental activities of daily living.
NS: Not applicable to model (variable was not significant within the model).
Higher values for need factors with scale scores indicate higher severity.
Some similarities were seen across models and conditions. Cohabitation with a caregiver, ADL capacity, and the RUG-III/HC case-mix were consistently positively associated across all models at high significance levels (P ⩽ .01). Regional effects on care costs were also observed across models and conditions. Other significant factors across conditions were difficulty breathing, cognitive performance, bowel incontinence, and unsteady gait. Conversely, characteristics such as sex, social withdrawal, and a number of neurological comorbidities (cerebral palsy, muscular dystrophy, spinal cord injury, traumatic brain injury, and Huntington disease) were consistently nonsignificant across conditions and models.
The log-transformed models produced higher levels of explained variance across all conditions and generally had fewer covariates, both indicating that the left-skewness of the cost distribution had some effect on the models. The total explained variance for each model as well as the explained variances for each of the predisposing, enabling, and need factor groups can be found in Table 5. In the absence of predisposing, enabling, and all other need variables, the RUG-III/HC case-mix system had high levels of explained variance. However, it is also the case that other need variables besides the RUG-III/HC CMIs contributed additional explained variance in both the non-transformed and transformed models. Enabling variables alone also demonstrated high levels of explained variance across conditions and models.
Explained variances (R2) by model and condition.

Discussion
The purpose of this study was primarily to identify characteristics predictive of the total cost (formal public home care cost plus the contribution of unpaid caregivers who are assigned a cost of one-half the hourly rate of a replacement worker) for those with ADRD, ALS, and MS. The identified predictors of these costs are consistent with findings reported in the literature. Like Kempen and Suurmeijer, 14 need and enabling factors had high levels of significance in predicting home care service utilisation. Cohabitation with a caregiver, in particular, was predictive of very large increases in care costs across the 3 conditions. Here, the strong and consistent finding that caregiver cohabitation with the care recipient was positively associated with cost is not surprising given cohabitation status tends to be associated with greater opportunity to provide this care, which is associated with greater informal care hours and thus a higher cost function.
Although this study does not include measures of disease progression or severity like previous studies, this study does support findings in the literature on costs of neurological conditions. For example, difficulties with breathing and mobility and greater symptom severity for depression, cognitive performance, pain, and ADL and IADL limitations are consistent with greater disease severity and progression and were predictive of higher care costs in this study. Considering that co-occurrence of these symptoms is expected for persons with ADRD, ALS, and MS, it was unsurprising to see that the cost of care for these conditions was high.
The cost estimates derived in this study also support previous findings that the costs and service needs of persons with these 3 conditions are substantially greater than the general home care population. Although home care costs have not previously been estimated for ADRD, ALS, and MS, the higher costs of care for these conditions are consistent with prior literature showing that care for neurological conditions is associated with high costs in acute and general settings.32-34 In addition, this study provided the resource intensity of the 3 conditions relative to the general home care population. The overall higher relative resource utilisation for persons with ADRD, ALS, and MS is also consistent with literature describing the greater care needs required for those with functional limitations.11,35
Interestingly, although the cost of care for MS was lower than for ADRD, the relative resource utilisation ratio was higher for those with MS. The lower mean cost and higher resource utilisation ratio would suggest that those with MS likely consume a greater volume of lower cost services than those with ADRD. This finding demonstrates that although estimates of cost can be important for policy planning around funding, cost alone may not be adequate when planning for resource needs and allocation. This implication may be particularly relevant to informal services, which are likely to bring savings to the health care system at the expense of provided by unpaid caregivers.
The fact that regional differences in costs were significant after controlling for need variables has important implications for policy and practice. These differences may reflect practice patterns that mean that access to and amount of services received depends on where one lives in the province. These differences did not always translate to urban-rural differences where concentration of resources or travel distances might have affected costs. There may be differences in contract rates between regions, but those differences are unlikely to be of the magnitude found in our analyses.
Finally, the models for predicting costs within clinical subgroups all demonstrated levels of variance as strong as or stronger than is typically reported in the case-mix literature. This is particularly true for patients with ALS and MS where R2 values were notably higher (55.2% and 46.8%, respectively) than has been reported elsewhere for general home care populations.21,22 The strong performance of the RUG-III/HC in the absence of other explanatory variables demonstrated its ability to measure clinical complexities associated with ADRD, ALS, and MS. In addition, even though the RUG-III/HC was not initially designed for specific use with particular neurological populations, it proved to be an effective predictor of care costs, particularly for the ALS population. Compared with the explained variances achieved in the final models, however, it is clear that the addition of other need characteristics could improve its ability to measure clinical complexity and predict resource use. Nevertheless, it appears that the current RUG-III/HC is an adequate measure of clinical complexity and predictor of cost for the general home care population that includes persons with ADRD, ALS, and MS. Given that the RAI-HC is a pan-Canadian standard assessment used routinely in 9 Canadian provinces and territories, it is useful to have a case-mix classification system that allows for adjusted comparisons of home care clients that take differences in resource intensity into account. Now that the adoption of the RAI-HC is widespread in Canada, it would be worthwhile to re-examine those data linked to cost data to explore options to further enhance the performance of the RUG-III/HC system taking into account the additional covariates that proved informative for the 3 neurological populations examined here.
Limitations
Some limitations of this study must be noted. These include the inability to differentiate subtypes of ADRD, ALS, and MS, or to measure the time since their onset. Because the progression and severity for each of these conditions differ based on subtype, differentiation between these subtypes may have identified other predictors of costs. In addition, the effect of non-neurological comorbidities was not assessed as part of this study because the objective of this study was to identify the effects of characteristics associated with neurological conditions on cost. Also, although this study provides accurate estimates of costs based on HC service utilisation, costs associated with specific service disciplines were not differentiated. Furthermore, case managers play an important role in the provision of home care services to clients, but costs associated with their roles were not included in this study.
Conclusions
Overall, the findings of this study indicate that clinical complexity is the main driver of care costs in these populations, with some characteristics being particularly predictive of high care costs. The ability of this study to identify specific client characteristics and disease symptoms affecting home care costs for these conditions will allow for more targeted care management and policy planning approaches for persons with ADRD, ALS, and MS. Similarly, the estimation of service utilisation as a ratio-level value will be useful for resource management. As utilisation of home care services and the prevalence of neurological conditions are expected to rise in coming years, an understanding of more specific mechanisms affecting care costs in home care will be required. Future studies of costs for the neurological conditions and for home care should continue to explore specific predictors of care costs to produce further actionable findings at the policy level.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the National Population Health Study of Neurological Conditions. We wish to acknowledge the membership of Neurological Health Charities Canada and the Public Health Agency of Canada for their contribution to the success of this initiative. Funding for the study was provided by the Public Health Agency of Canada.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Cheng completed all analyses and drafted the first version of the manuscript. All authors contributed to development of research concept and analytic plan. All authors contributed to revision of manuscript and approved final version.