
Abstract
Background:
Use of opiates, including synthetic opioids, is associated with a number of negative consequences, including increased risk of opioid use disorders and other mental health conditions. However, studies are limited in examining patterns of opiate use among persons in inpatient psychiatry, particularly those that consider the relationship between pain and opiate use.
Objective:
This study examined the prevalence in the prior 12 months to admission and patterns of opiate use and pain in a population-based study of persons admitted to inpatient psychiatry in Ontario, Canada.
Methods:
We conducted retrospective cross-sectional study of 165 434 persons admitted to inpatient psychiatry between January 1, 2006 and December 31, 2017. Using data from the Resident Assessment Instrument for Mental Health, we examined prevalence and factors associated with opiate use in the prior 12 months by a number of patient characteristics, including demographics, mental and physical health status, concurrent substance use, pain severity and frequency, and health region of residence.
Results:
The prevalence of opiate use within 12 months of admission was 7.5%, between 17% and 22% among those experiencing daily pain, and 27% among persons with a primary substance use disorder. Multivariable analyses revealed strong associations among demographic and clinical variables with opiate use (c = 0.91), including being of younger age, use of other substances, greater frequency and severity of pain, and health region of residence.
Conclusion:
The strong relationship between pain and opiate use in this population, and the regional variation in this pattern, supports the need for integrated care for mental illness and substance use, and therapeutic approaches to pain management that reduce risks of problems associated with substance use for persons with mental health conditions.
Background
Canada and the United States have the highest prescription opioid consumption in the world, and its use continues to increase dramatically. In the United States, the number of deaths due to opioids increased by more than 300% between 2001 and 2016. 1 This trend was similar in Ontario, Canada, between 2000 and 2015, particularly deaths among persons aged 25 to 34. 2 The College of Physicians and Surgeons of Ontario has suggested that opioids are overprescribed, resulted from an overreliance of pharmaceutical treatments for long-term pain and a lack of nonpharmaceutical pain management resources within the health system. 3 There is a strong association between daily dose of opioids and opioid-related mortality, particularly when dose exceeds recommended threshold. 4 Furthermore, negative outcomes associated with opioid use are more common among persons of lower-income status in Ontario. 5 Yet, between April 1, 2015, and March 31, 2016, there were more than 600 000 persons provided with a new opioid prescription in Ontario, with dental pain accounting for the most common clinical indication for opioid initiation and postsurgical pain accounting for the highest dosages and longest duration of use. 6 Canadian clinical guidelines for opioid prescribing for pain 7 have not been effective in reducing the rate of opioid-related hospitalizations, the prevalence of high-dose opioid use, and significant interprovincial variation in the dispensing of high-dose opioid formulations in Canada.8-10 All of this has resulted in an increasing rate of opioid-related deaths in Ontario, particularly from nonmedical or use of illicitly obtained opioids. 11
Substance use, including opioid use, is associated with a number of mental health conditions, including personality and posttraumatic stress disorders. 12 Persons who have an opioid use disorder may experience psychotic symptoms 13 and engage in use of additional substances, including alcohol. 14 While patients with opioid use disorders can be effectively treated with interventions like methadone maintenance treatment (MMT), 15 monitoring for mental health conditions remains important. For instance, the prevalence of depression and suicidal ideation among persons receiving MMT has been estimated to be 43% and 15%, respectively, well above population norms. 16 Substance use disorders can complicate the management of long-term noncancer pain, making routine monitoring and assessment for substance use disorders an important aspect of long-term opioid prescribing. 15
Pain has contributed to off-label use of opioids, with persons receiving opioid prescriptions for cancer or long-term noncancer pain being at increased risk of opioid abuse and dependence.17-19 Opioid prescribing in emergency medicine is of particular concern, particularly given the substantial use of emergency departments for pain. 20 Opioid misuse among patients with long-term pain has been linked to low pain acceptance, which is unresolved pain despite increasing opiate dosing, as well as increased pain perception due to opiate tolerance, increased risk of opioid use disorder and other psychiatric conditions, and risk of overdose.18,21 Pain is a complex physiological and emotional response to real or perceived damage to the body. Pain manifests as behavioral, affect, and cognitive responses from patients and is highly subjective. Within inpatient mental health settings, the assessment and treatment of pain is highly complex. Pain and psychiatric conditions are highly comorbid, 22 with historical estimates of up to 38% of inpatient psychiatric patients reporting pain symptoms.23,24 Pain is particularly common among persons receiving treatment for substance abuse, with 1 year and lifetime prevalence estimates of substance use disorders ranges from 3% to 48% and 16% to 74%, respectively, among patients with long-term pain. 18
The relationship between pain and mental health is variable and nuanced. Pain is more prevalent among persons with anxiety and depression than those with psychotic disorders. 22 For instance, the prevalence of pain among adults with major depressive disorder is estimated to be 47%. 25 It may be that long-term physical distress precipitates depressive symptoms, yielding a depressive disorder as a secondary diagnosis, 26 or that a primary depression manifests as pain response.27,28 However, it is also possible for the 2 conditions to exist independently from one another.29,30 Regardless of the cause, the result is that persons with psychiatric conditions tend to report greater pain intensity and pain-related disability compared with the general population.25,31 Co-occurrence of pain and psychiatric conditions is associated with disability, impaired physical and mental well-being, poor quality of life, and increased burden on the health care system. 25 Taken together, these trends suggest that persons affected by pain admitted for psychiatric care are a highly vulnerable population. Comorbid psychiatric conditions may complicate pain treatment, elevating the risk of dependence on opiates.
While patterns of opioid use have been examined in the general population, no studies exist examining the extent of opioid use among a population of persons admitted to inpatient psychiatry. Therefore, the purpose of this study is to estimate the prevalence of opiate use within the year prior to admission to inpatient psychiatry in Ontario, Canada. We also examine factors associated with opiate use, including physical pain.
Methods
We used a retrospective cross-sectional study of 165 434 persons admitted to inpatient psychiatry between January 1, 2006, and December 31, 2017. The data were available from the Ontario Mental Health Reporting System (OMHRS) of the Canadian Institute for Health Information (CIHI). The OMHRS includes data from the Resident Assessment Instrument for Mental Health (RAI-MH) at admission, at 90 days (if still in hospital), and at discharge for every person admitted to mental health beds across 71 hospitals in Ontario, Canada. The RAI-MH includes more than 400 items grouped under 24 broad categories including: sociodemographic variables, clinical and functional status, harm to self and others, provisional psychiatric diagnosis, substance use, control interventions, health service utilization, social relationships, and vocational factors. 12 Persons overseeing the care of the person complete the RAI-MH using all sources of information, including interview with the person and the person’s family (where appropriate) as well as discussions with other clinical team members and review of the person’s clinical record. In Canada, the CIHI oversees all training for the completion of the instrument as well as data quality (https://www.cihi.ca/en/mental-health-and-addictions). The instrument and its care planning applications are also supported by detailed manuals available to assessors.32,33 The instrument has good interrater reliability, with an average agreement of 83% and average weighted kappa of 0.70 for all its items. 34 In Ontario, the RAI-MH is licensed free of charge to the Ontario Ministry of Health and Long-Term Care for use among all hospitals providing inpatient mental health services. Further information about copyright and licensing can be found at www.interrai.org.
Dependent variable: opiate use
The main outcome variable was opiate use within the year prior to admission to hospital. The RAI-MH includes a section on substance use, where assessors rate the most recent instance a person reported using a given substance, including opiates, cannabis, cocaine, stimulants, inhalants, and hallucinogens. Assessors are trained to include natural and synthetic forms of opiates including heroin and synthetic preparations of methadone. Use is coded if the person used the substance in the 3 days, 7 days, 30 days, 90 days, and 12 months prior to admission. While our primary variable of interest is any use within the 12 months prior to admission (including 3, 7, 30, and 90 days), we also report the more granular results for the patterns of pain and opiate use that occurred within 30 days (including 3 and 7 days).
Independent variables
The demographic variables included approximate age by birth year, having a confidant, marital status, being homeless, living alone, highest level of education, employment status, and health region of residence. In Ontario, there are 14 health regions called Local Health Integration Networks (LHIN) that oversee the distribution of health funding, organization, and accountability of health services within their region. Gender on the RAI-MH is coded as “female,” “male,” and “other.” Given the small number of persons coded as “other,” we created 2 gender categories, coded as male and female. For those employed or attending school, risk of employment or disruption of education was identified based on increased lateness or absenteeism, poor productivity, intention to quit, persistent unemployment, or fluctuating work/school.
Admission characteristics were identified based on the reason for admission, whether the person was involuntarily admitted to hospital, and the person’s insight into their mental health or substance use condition. A number of substance-related variables were examined, including: Patterns of use of other substances within the prior 12 months, the number of alcohol drinks in a single sitting in the prior 2 weeks, daily tobacco use, and intentional misuse of over-the-counter or prescription medications. The RAI-MH includes a scale ranging from 0 to 4 measuring problematic substance use (PSU) using the “CAGE” domains: whether the person feels the need to cut down, others have criticized the persons use of substances, the person feels urge to drink or use substances first thing in the morning, and whether the person feels guilt related to alcohol or substance use. These items have been found to be reliable and valid indicators in predicting problematic use 35 and are recommended as screening items in the Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-Cancer Pain. 36 A number of other clinical scales are embedded in the RAI-MH, including the Cognitive Performance Scale (CPS; ranges from 0 (cognitively intact) to 6 (very severe cognitive impairment) 37 ; the Aggressive Behavior Scale (ABS; ranges from 0, no behavior to 12, daily behavior across 4 indicators) 38 ; the Depressive Severity Index (DSI; ranges from 0 to 15, with higher scores indicating higher frequency of depressive symptoms observed in the last 3 days) 39 ; Activities of Daily Living Hierarchy (ADLH) Scale, which measures the level of dependence on others for personal hygiene, mobility, toilet use, and eating, with a high score being a more dependent patient.
The RAI-MH also includes a Pain Scale which combines the frequency and intensity of pain into a score that ranges from 0 (no pain) to 4 (excruciating daily pain), with scores greater than 1 indicating daily pain differentiated on intensity. The intensity measure of this scale is similar to other validated measures of pain, such as the Visual Analog Scale (VAS), Numerical Rating Scale (NRS), and Simple Descriptive Scale (SDS). 40 The RAI-MH codes pain intensity via a 0 to 4 scale similar to the SDS: 0 (no pain), 1 (mild), 2 (moderate), 3 (severe), and 4 (excruciating). Frequency is coded based on daily or nondaily pain is experienced nondaily or daily. This interRAI pain scale was highly correlated with VAS scores. 41
The primary Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), Fourth Edition (2006-2014) and DSM-V (2015-2017) category coded at discharge was included. For ease of interpretation, we recoded DSM-V categories into the prior DSM-IV category. For instance, DSM-V introduced a unique category for disorders related to trauma that were previously included within the DSM-IV category for anxiety disorders. We included the 6 most common diagnostic categories: neurocognitive disorders, substance-related and addictive disorders, schizophrenia spectrum and other psychotic disorders, mood disorders, anxiety disorders, and personality disorders. All other diagnostic categories were assigned to a category labeled “Other” due to low count and negligible prevalence in the sample. These include mental disorders due to general medical conditions, somatoform disorders, factitious disorders, dissociative disorders, sexual and gender identity disorders, eating disorders, sleep disorders, adjustment disorders, and impulse-control disorders not elsewhere classified. Concurrent substance use disorder was identified based on the presence of any DSM diagnoses in conjunction with a secondary or tertiary substance use disorder. Using International Classification of Diseases, Tenth Revision, Canada (ICD-10-CA) codes, we also identified certain medical and neurological illnesses that are commonly associated with pain, including cancers, HIV/AIDS, diabetes, hepatitis C, multiple sclerosis, rheumatoid arthritis, traumatic brain injury, stroke, and epilepsy. Given the low prevalence in the sample, the following medical conditions were grouped as “other medical diagnoses”: diabetes, chronic obstructive pulmonary disease (COPD), heart failure, renal disease, rheumatoid arthritis, metastatic cancer, lymphoma and tumor without metastasis.
Analytic approach
Bivariable relationships between the independent variables and opiate use were examined using chi-square analyses. Independent variables with significant bivariable associations were considered in multivariable logistic regression model. We entered variables into the model in blocks (eg, demographics, clinical symptoms, diagnoses, year, and LHIN), keeping variables with significant associations at P < .0001. The LHIN 7 (Toronto Central) was used as the reference group, as this LHIN represents the highest population density and concentration of psychiatric services among all LHINs. The Pain Scale was entered into the model last to determine the strength of the association between pain and opiate use after holding all other variables constant. All analyses were performed using SAS, version 9.4.
Results
The total prevalence of reported opiate use within 12 months of admission to psychiatric hospital was 7.5% (n = 12 409). Table 1 provides a description of the characteristics of persons admitted to inpatient psychiatry in Ontario, and the prevalence of opiate use by each characteristic. Approximately 50% of the sample were under the age of 44. Opiate use was more common among the younger age groups, with between 8% and 11% of those between age 18 and 44 reporting opioid use in the prior year. Notably, those aged 18 to 24 have higher prevalence of past-year opiate use (8.4%) compared to those aged 45 to 64 (6.5%). Among the 51% of the total sample who were male, the prevalence of opiate use was 9% among males compared to 6% among females. Opiate use was almost twice as common among those whose employment or education was at risk (10.5%) compared to those not at risk (5.8%). Use was less common among the 54% of patients who reported having or having had a partner at some prior point in their life. Patterns of opiate use did not differ by homelessness or living alone.
Sample characteristics, proportion of persons reporting opiate use within the year prior to admission to hospital by each characteristic, and chi-square statistics examining the differences in proportion reporting opiate use by levels of each characteristic.

Abbreviation: DSM, Diagnostic and Statistical Manual of Mental Disorders.
indicates lived with spouse, children, others (not spouse or children), group setting with non-relatives.
The most common psychiatric diagnoses were mood disorders (41.5%), with 58% of the sample exhibited moderate to severe depressive symptoms. About a quarter of inpatients had schizophrenia and other psychotic disorders (23.6%), with 33% of the sample exhibiting moderate to severe positive symptoms of psychosis. Primary substance use disorders were prevalent among 16% of the sample, with opiate use being most prevalent among persons with a primary and concurrent substance use disorder compared to other diagnoses.
Variable patterns of opiate use were noted across symptom, functional, and medical conditions. For most symptoms and functional scales, the prevalence of opiate use within the prior year was similar to or lower among persons scoring higher on each scale. For instance, 7.7% of persons with moderate to severe depressive symptoms reported opiate use compared to 7.2% of those with no or mild symptoms. The notable exception is persons reporting pain. Of the 24% of patients who reported pain, about 14% reported experiencing daily pain (a Pain Scale score greater than 1). The prevalence of opiate use within the prior year increased from 10% among persons reporting nondaily pain to 17% among persons reporting daily severe pain and 21% among persons reporting daily excruciating pain. The prevalence of opiate use was 15.5% among the 0.4% of patients with HIV, 33.5% among the 0.9% of patients with hepatitis C, 9% among the 0.2% of persons with multiple sclerosis, and 8.3% among the 0.2% of persons with traumatic brain injury.
There was substantial variation in the prevalence of opiate use across regions in Ontario. About 14% of the total provincial admissions were from LHIN 3, with 14% using opiates in the prior 12 months. While LHIN 14 accounted for only 2% of the provincial admissions, about 16% within that LHIN reported opiate use in the last 1 year.
Table 2 shows the prevalence of opiate use in the 12 months preceding psychiatric hospital admission by indicators of substance use and addictions. More than a quarter of psychiatric admissions in Ontario were for substance use (27%), and of these, 20% had used opiates in the 12 months prior to admission. Opiate use was most prevalent among patients also having used stimulants (41%), inhalants (35%), and cocaine (33%). About a quarter of patients reporting intentional misuse of either over-the-counter or prescription medication reported using opiates in the prior 12 months.
Prevalence of opiate use within 12 months of admission among persons who have used other substances within the prior year, alcohol use in prior 14 days, and intentional misuse of over-the-counter or prescription medications.

Additional substances included inhalants, stimulants, cocaine/crack, cannabis, and hallucinogens.
Factors associated with opiate use
Table 3 shows the results of the final multivariable logistic regression model that includes pain. The models without pain and with pain (model 2) had very strong fit in discriminating between those using and not using opiates, with c-statistics of 0.90 and 0.91, respectively. In the final model, persons who were aged 25 to 44 were 33% more likely to use opiates than those aged 18 to 24. Having a high school education, or greater, and being employed decreased the odds of opiate use. Persons with a substance use disorder were about 2.5 times more likely to use opiates compared to other primary diagnoses. Interestingly, holding all variables in the model constant, concurrent substance use disorder was not significantly associated with opiate use (odds ratio [OR] = 0.99; 95% confidence interval [CI], 0.88-1.12). Other than primary substance use disorders and hepatitis C, persons with all other psychiatric, medical, and neurological diagnoses in the model were found to have lower odds of opiate use. Indicators of additional substance use were all strongly associated with opiate use. Persons with a score greater than 2 on the PSU scale were 75% more likely to use opiates, while persons using cocaine/crack, simulants, or inhalants were all more than twice as likely to use opiates. Patients who reported having intentionally misused over-the-counter or prescription medications in the prior 90 days were 3.61 times more likely to use opiates. Interestingly, patients who had reporting having a 5 or more drinks in a single sitting the prior 2 weeks were about 45% less likely to use opiates. Year of admission was also associated with opiate use, with the odds of opiate use increasing by 1.03 for each year after 2006. The odds of opiate use also varied across LHINs, where the odds of opiate use were higher for patients in LHINs 1, 13, and 14 compared to patients in LHIN 7.
Logistic regression results examining the relationship between individual characteristics and opiate use within 12 months prior admission to hospital (AUC = 0.91).
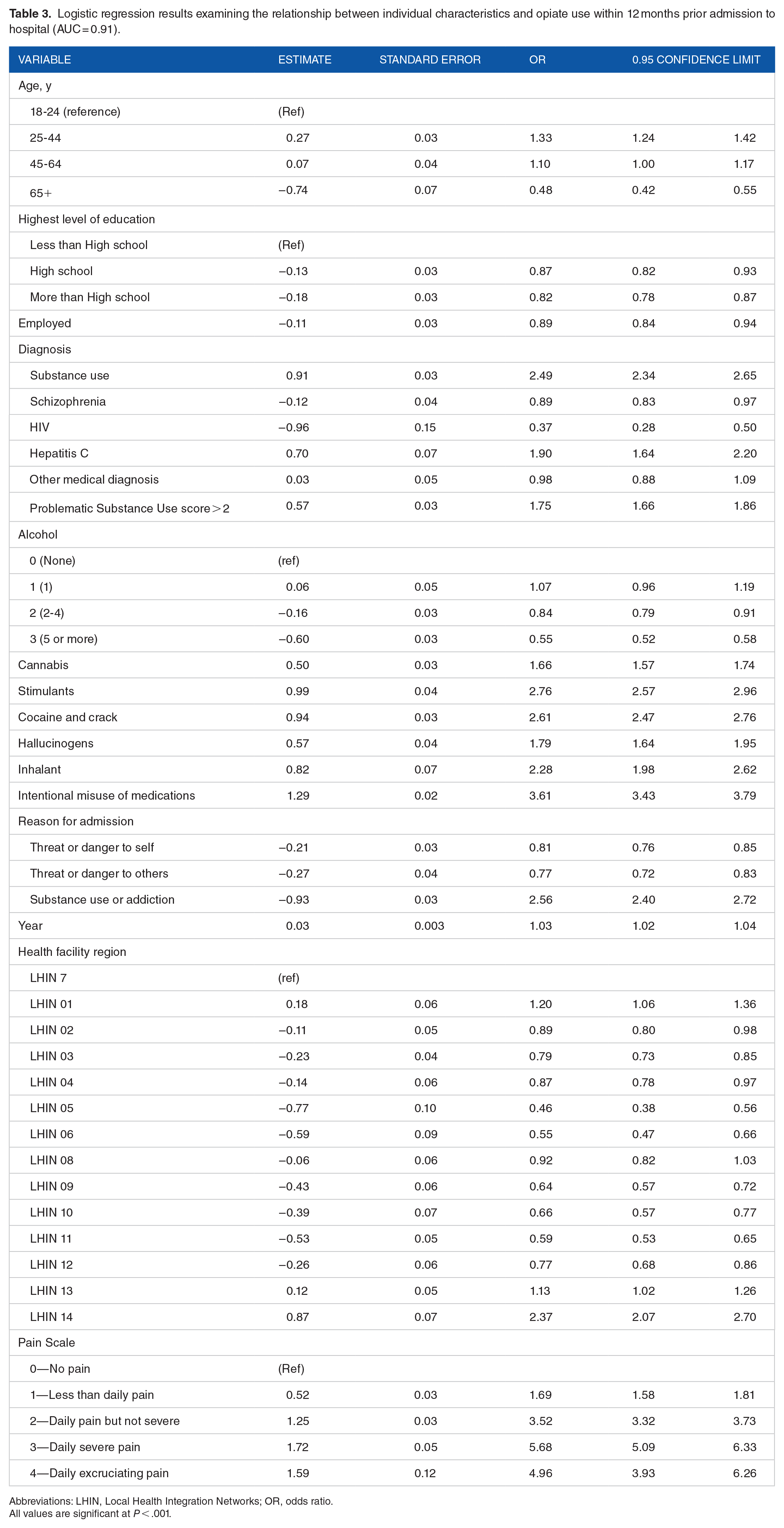
Abbreviations: LHIN, Local Health Integration Networks; OR, odds ratio.
All values are significant at P < .001.
Pain was strongly associated with opiate use in the multivariable model. Patients experiencing nondaily pain were 3.5 times more likely to use opiates, while those with daily severe pain were 5.68 times more likely to use opiates compared to those with no pain. Since there are no data on whether the person was using opiates in some supervised fashion (eg, opioid maintenance therapy), we examined the misuse of over-the-counter or prescription medications, as well as use of opiates in the 30 days and 1 year prior to admission, by level of pain (Figure 1). The results clearly indicate the positive association where the prevalence of opiate use within 30 days (χ2 = 5736.17, P < .0001) and 12 months (χ2 = 4346.67, P < .0001) prior to admission increases as pain increases. For those with no pain, the prevalence of opiate use within 30 days of being admitted was 5%, whereas 15% or more for those experiencing daily pain (a Pain Scale score of 2 or more) reported opiate use within 30 days of admission. The trend is also shown for misuse of over-the-counter or prescription medications, with 22% to 28% persons experiencing daily pain having misused medications in the prior 90 days.

Percentage of person reporting opiate use in the 12 months and 30 days prior to admission, and misuse of over-the-counter or prescription medications within 90 days prior to admission by Pain Scale score for persons admitted to inpatient psychiatry in Ontario, Canada.
Discussion
This study examined the patterns of opiate use among persons admitted to inpatient psychiatry in Ontario, Canada. The findings show that opiate use within the 12 months prior to admission was prevalent for about 7% of the total sample and varied substantially across patient characteristics. The prevalence did increase slightly over time. The overall prevalence did increase by about 2% between 2006 and 2008 but then remained relatively stable, dropping slightly after 2013. The reasons for the slight decrease after 2013 are not clear, perhaps relating to local changes in policy and practice related to opiate use, a diversion of persons who use opiates to other service settings, or loss to follow (eg, death). Looking at results for 2015, the prevalence of opiate use in this study was lower than the prevalence of use of opioid pain relievers in 2015, 13%, among the Canadian population. 42 However, if we consider that a large proportion of opiate use reported in this sample may have been nonmedical, such as through intentional misuse of medications, the prevalence is greater than the 2% of the general Canadian population reporting nonmedical use in 2015. 42 The strong relationships between substance use disorders and opiate use found in this study further emphasize the extent to which opiate use may be associated with negative outcomes, rather than therapeutic benefit, within this population.
We also found significant variation in those that reported opiate use across health regions in Ontario. The regional variations in odds of opiate use require further examination. After adjusting for demographic and clinical characteristics, the odds of opiate use varied substantially in comparison to the most densely populated region in Ontario, LHIN 7 (Toronto Central). Further research is needed to examine whether this variation is related to factors such as population densities and compositions, health service resources, or other public policies. For instance, the general variation observed in this study is consistent with variations in patterns of opioid prescribing across Ontario.8-10 In Ontario, health services administered by the LHINs do not include local and provincial public health agencies, and until recently, the LHINs did not have oversight over primary care providers. As such, variations in opiate use across regions may relate to variations in prescribing practices, health system organization, public health policy, illicit supply, population characteristics, and other systems issues. This is an important area for further research to understand whether variations in health system and public health policies contribute to the variations in opiate use in mental health contexts.
Pain was reported among almost a quarter of persons in inpatient psychiatry in Ontario, Canada, between 2006 and 2017. The odds of opiate use more than tripled among persons reporting daily pain. What is concerning about these findings is that the prevalence of substance-related issues, such as misuse of medications, also increased as pain severity and frequency increased. This relationship was more pronounced among persons in pain who were using opiates. The prevalence of substance use disorders among persons using opiates also varied by level of pain. The lower prevalence of substance use disorder among those who used opiates and reported higher levels of daily pain may have reflected a subset of persons using opiates under medical supervision for severe pain, but may also have been an artifact of the small sample of persons reporting severe or excruciating daily pain.
The patterns of opiate use among persons in pain exemplify the complexity in assessing and managing pain in psychiatry. An advantage of the RAI-MH is that, in addition to intensity, it also codes for frequency (how often pain is experienced over time), which do provide a more complete picture of a patient’s pain over time, rather than a single snapshot. That said, the pain scale is meant to be a screening measure and not an in-depth assessment of all facets of pain. Comprehensive measurement of pain intensity includes the affective, cognitive, and behavioral presentation of the patient in response to real or perceived stimuli. 22 However, as each of these measures is a neural process, a patient’s pain can be complicated by and intertwined with comorbid psychiatric and physical conditions. For instance, there exists a reciprocal relationship between pain and psychiatric symptoms such as anxiety and depression, with pain exacerbating low mood and anxiety, while these symptoms may sensitize a person to pain from an underlying physical condition, or even present as symptoms of psychiatric disorders. 22 Our findings emphasize the need to include holistic and comprehensive assessment of pain following brief screening that may be based on unidimensional, subjective reports of pain.43,44 Unlike acute medical care settings the source of pain may not be visible or clearly diagnosed among persons in mental health contexts; the source of pain as well as the treatment plan is often complex, unclear, and malleable. The psychiatric care team must consider the person’s social context, mental and physical health conditions, and risk of addiction when collaborating with the patient to achieve pain control. 45 Comprehensive assessments such as the RAI-MH would support this process by considering the interplay between physical, mental, functional, and substance-related issues. Of course, addressing the context of opiate use and pain among persons with mental health conditions relies on the availability of integrated systems of support for pain and substance use.
It is also important to recognize that persons not reporting pain also reported use of opiates in the prior year. Over the course of the observation period of this study, there have been many changes related to the use of opioids across Canada, with opioid use having emerged as major public health crisis.1,2,10 Numerous studies in Ontario have reported an increase in problems associated with opiate use, including substance use disorders and mortality.4,8 Indeed, our findings indicate that the majority of those using opiates prior to admission to inpatient psychiatry have other indicators of problematic substance use, including substance use disorders and use of other high-risk substances like stimulants and cocaine/crack. Furthermore, the increased prevalence of opiate use from 2006 to 2008, and beyond, may further reflect this population issue. However, it was surprising to find that, contrary to other literature, 13 persons with serious mental health symptoms such as psychosis were less likely to report opiate use. It may be that persons using opiates were still be intoxicated or experiencing withdrawal at admission, masking other mental health symptoms. While the prevalence of medical conditions was generally low in this study, the increased prevalence of opiate use among persons hepatitis C may be representative of problems associated with nonmedical use of opiates, such as the use of intravenous delivery methods. Together, these findings are important for creating awareness on the risks associated with polysubstance use that includes opioids and other drugs. Further research is needed, perhaps using cluster analyses, to examine combinations of substances being used in relation to or in the absence of pain, and their associations with clinical outcomes, hospital readmissions, and other outcomes.
Finally, our findings emphasize the importance of comprehensive assessment systems for conducting a holistic assessment of the person’s mental and physical health status, functioning and supports, and substance use. It important to recognize that such systems are not meant to simply administratively record observations of a person’s status. The assessment should be used within the clinical context to inform ongoing plans of care, 32 while at the same time yielding aggregate data that can be used for program and policy planning and evaluation.
Limitations
This is a descriptive study and cannot make causal inferences about the associations between the variables assessed at admission to psychiatric care and the use of opiates in the year prior to admission. As such, due to limitations in data available at the time when a person may have used opiates, it is important to note that factors other than those examined in this study may have been associated with the person’s use of opiates. Furthermore, given that the data used in this study represent a specific subset of the mental health services and do not represent primary care, emergency departments, community mental health or substance use services it is likely that our study underestimates the prevalence of opiate use among persons with mental health conditions. Thus, the characteristics of persons using opiates in this study cannot be generalized to those within the general population. It is possible that most persons using opiates never come into contact with inpatient mental health settings. This possibility comes from the fact that mental health and addiction services in Ontario continue to be fragmented, with the emergence of services providing concurrent disorders services being a recent and rare phenomenon. 46
We were not able to distinguish opiate use under medical supervision and nonmedical use of opiates. Specifically, there was no way to determine the type or opiate being used, whether there was a prescription for the opiate, and whether the person was using an opiate for maintenance purposes. For those who may have had a prescription, data on the common clinical indications for opiate use (dental, postsurgical, musculoskeletal, trauma, and cancer/palliative care) was not available. This information would be helpful for teasing out problematic opiate use from supervised use, and whether supervised use of opiates may have been helpful.
Conclusions
A large proportion of persons reporting use of opiates in the 12 months prior to admission to inpatient psychiatry have substance use challenges and addiction. A substantial proportion of persons using opiates were admitted for substance use or addiction, had a substance use disorder, engaged in misuse of over-the-counter or prescription medications, and used other substances. Furthermore, increasing severity and frequency of pain is strongly associated with opiate use and PSU. These findings support the movement toward integrated care for mental illness and substance use, and therapeutic approaches to pain management that reduce risks of problems associated with substance use for persons with mental health conditions.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
OA contributed to the background literature review, study design, conducted data analyses, and writing of the manuscript. AR contributed to study design, supported interpretation of data analysis, and contributed to the manuscript drafting and editing. CP provided study design, supported data analysis and interpretation, and supported the writing and editing of the manuscript.