
Abstract
As mental health care transitions from facility-based care to community-based services, methods to classify patients in terms of their expected health care resource use are an essential tool to balance the health care needs and equitable allocation of health care resources. This study performed a scoping review to summarize the nature, extent, and range of research on case-mix classifications used to predict mental health care resource use in community settings. This study identified 17 eligible studies with 32 case-mix classification systems published since the 1980s. Most of these studies came from the USA Veterans Affairs and Medicare systems, and the most recent studies came from Australia. There were a wide variety of choices of input variables and measures of resource use. However, much of the variance in observed resource use was not accounted for by these case-mix systems. The research activity specific to case-mix classification for community mental health care was modest. More consideration should be given to the appropriateness of the input variables, resource use measure, and evaluation of predictive performance. Future research should take advantage of testing case-mix systems developed in other settings for community mental health care settings, if possible.
Introduction
Globally, the burden of mental illness accounts for 32% of years lived with disability, 1 costing about US$2.5 trillion in 2010. 2 As in other health care sectors, funding for mental health care is limited. The challenge is how to match resources to the needs of the population.2,3 Methods to classify patients in terms of their expected resource use is an important pre-requisite in addressing this challenge.
Although each person in the population is unique, there are shared characteristics that determine the types of treatments or services that individuals receive from the health care system. 4 In other words, there are groups of people with similar characteristics, which will consume similar amount health care resources and, by extension, incur similar costs of care. These groups represent the mix of cases that are observed in a health care system, or a “case-mix,” 5 which can be viewed as a proxy for the types of health care needs of the population.
Case-mix classification is commonly used in payment systems to reimburse health care providers based on the type of patient, 6 also known as activity-based funding. Other applications of case-mix classification include risk adjustment models for health outcomes or other quality measures, staffing, program evaluation, and long-term planning and budgeting tools for policy makers. 6
Case-mix classification systems can be of two types: grouping or index systems. 5 Grouping systems assign cases into relatively homogeneous groups in terms of their expected resource use. 5 Each group has a weight associated to represent its expected resource use relative to the average case in the population, also known as “case-mix index.” 5 For example, the Resource Utilization Group Version III (RUG-III) is commonly used in the United States and Canada for nursing homes reimbursement. 7 Index systems, instead, combine different characteristics of a case to produce a numerical value for each case that represents the expected level of resource use, which can then be mapped it to a “case-mix index” value to represent expected level of resource use relative to the average case in the population. 5 For example, the Outcome and Assessment Information Set (OASIS) is used by Medicare to reimburse home care services. 8 A previous study also provided further discussion of these two types of systems. 9
It is worth noting that a funding formula is distinct from a case-mix classification system. A funding formula may work by assigning a monetary amount to the case-mix index and further adjusted based on numerous factors external to the case-mix classification system, such as available funding, inflation, geographic and provider characteristics, or negotiations between health system administrators and the providers. On the other hand, the case-mix index values are expected to remain constant because the health care needs of one group relative to another should not change drastically from year to year. Case-mix index values can change in rare occasions, such as changes in technologies or clinical practices, which may affect only one or a few groups by making them either more or less expensive to care for compared to the rest of the population. In addition, a funding formula may not be composed solely of case-mix classification, other designs are possible, such as a blend of case-mix and global budget. 10
For mental health, the delivery of care can take place in multiple settings as de-institutionalization has shifted mental health services from facility-based inpatient care to community-based care.11,12 Facility-based inpatient care provides intensive observation, diagnosis, and treatment typically in times of crisis, 13 and usually requires a hospital admission with one or more overnight stays. 14 Community-based care typically employs a care team that provides a wider range of services, including both urgent and ongoing care, such as assertive treatment services, crisis management, outreach, recovery, housing, occupation training, and day programs. 13
Previously, Jones et al 15 reviewed 16 studies between 1990 and 2005 studying predictors of mental health service utilization and costs. Hermann et al 16 reviewed 36 studies between 1980 and 2002 focusing on risk adjustment models of psychiatric health outcomes and costs, which included some case-mix systems. Mason and Goddard reviewed 5 international examples of activity-based funding systems for mental health between 2006 and 2008. 17 Harris et al 18 reviewed 13 case-mix classification systems for all mental health care settings, but only in some Western countries published between 1995 and 2012.
To date, most mental health case-mix classification systems have predominantly focused on care in acute or inpatient settings. However, case-mix classification systems for community settings have received little attention. Therefore, this review summarized the nature, extent, and range of the up-to-date research on mental health care resource prediction using case-mix specifically in community settings, and identified the gaps in the current research.
Methods
In alignment with scoping review methods by Arksey and O’Malley, 19 and PRISMA, 20 four academic literature databases were searched: PubMed, Web of Science, PsychInfo, and SCOPUS. Keywords were used to search the title and abstract for the presence of mental health, case-mix, and community settings concepts: (“mental health” OR “mental ill*” OR “mental disorder?” OR “psychiatr*” OR “behavio* care” OR “behavio* health”) AND (“casemix” OR “case mix” OR “case-mix” OR “case type?” OR “diagnosis related group*” OR “patient mix” OR “patient? group*” OR “patient? classification?” OR “patient? cluster*” OR “case? cluster*” OR “risk adjust*” OR “case adjust*”) AND (“communit*” OR “outpatient?” OR “out-patient?” OR “ambulatory”). Searches were done in October 2018 and included all date ranges. Duplicates and non-English full-text articles were removed. Database searches were also supplemented by scanning references of the eligible articles, consulting with experts and co-authors.
Articles’ titles and abstracts were then screened for relevance, followed by a screen of the full-text by the lead author and a review by the co-authors. Articles were included if a case-mix classification system was used to predict resource use of community mental health care or health care resource use of people with mental health disorders in community settings. This review used the World Health Organization’s definition of health care resources as the three main inputs of a health care systems as human resources, physical capital, or consumable resources. 21 As in similar reviews,18,22,23 this review considered studies that predict resource use using case-mix classification, rather than to simply describe the differences in resource use among sub-groups of the study sample, or to explain the variation in resource use by adjusting for different variables. In addition, a predictive study should provide a quantitative assessment of how well the predicted resource use explained the observed resource consumption, such as the R2 value. 15 The community settings were defined as care settings that do not require an overnight stay at the facility, 14 which may include outpatient treatments or day programs.
To capture the scope of the case-mix classification systems presented, we collected key characteristics from each eligible article. Specifically, we collected information regarding the bibliography (authors, year of publication), sample data (geographic jurisdiction, care settings, age groups, sample size), case-mix system (name, input variables, type), resource use measure (definition of measure), and predictive performance (type, reported value). Data were then recorded and reviewed with the co-authors.
Results
This study identified 17 articles matching the criteria (Figure 1), which presented 32 case-mix classification models (Table 1). Most were from academic sources, except for the technical reports of the case-mix systems developed in Australia and New Zealand.14,46,50 Most studies (11 out of 17) focused only on adult population.

Search procedures for relevant articles.
Eligible studies, ordered by year of publication.

Abbreviations: ACG, Ambulatory Care Groups; ADG, Ambulatory Diagnostic Groups; AMHCC, Australia Mental Health Care Classification; CAMHS, Child and Adolescent Mental Health Services; CCI, Conditional Comorbidity Indices; CDPS, Chronic Illness and Disability Payment System; CGAS, Children’s Global Assessment Scale; DCG, Diagnostic Cost Group; DRG, Diagnosis Related Groups; FIHS, Factors Influencing Health Status; GAF, Global Assessment of Functioning; HCC, Hierarchical Condition Category; HoNOS, Health of the Nation Outcome Scales; LONCA, Level of Need-Care Assessment; LSP, Life Skills Profile; MCAS, Multnomah Community Ability Scale; MCI, Mental Comorbidity Indices; MH-CASC, Mental Health Classification and Service Costs; NICE, National Institute for Health Care Excellence; NZ-CAOS, New Zealand Mental Health Classification and Outcomes Study; PCI, Physical Comorbidity Indices; SMI, Serious Mental Illness; URG, Utilization Risk Groups.
Most of the research came from the United States, and the largest studies came from the USA Veterans Affairs and Medicare systems.42,45,48,53 However, it is worth noting that the samples from the Veteran Affairs system were mostly adult males, and samples from the Medicare system were adults aged 65 or older, which were not representative of the US population. The most recent major effort came from Australia with their Australian Mental Health Care Classification (AMHCC), 50 which was developed to predict resource use for both inpatient and community settings, and all age groups.
The input variables for the case-mix classification systems were varied. Most common variables were diagnosis, demographics, variables related to severity, comorbidity, or functional status. Most case-mix systems were grouping system, and index systems were less common.
There were also a wide range of measures of resource use from the studies identified. These measures can be roughly classified into 2 types: proxy measures (such as number of visits) (Table 2) and direct measures (such as claims data or wage-weighted staff time) (Table 3).
Empirical results of case-mix systems predicting proxy measures of resource use, ordered by name of the case-mix system and year.
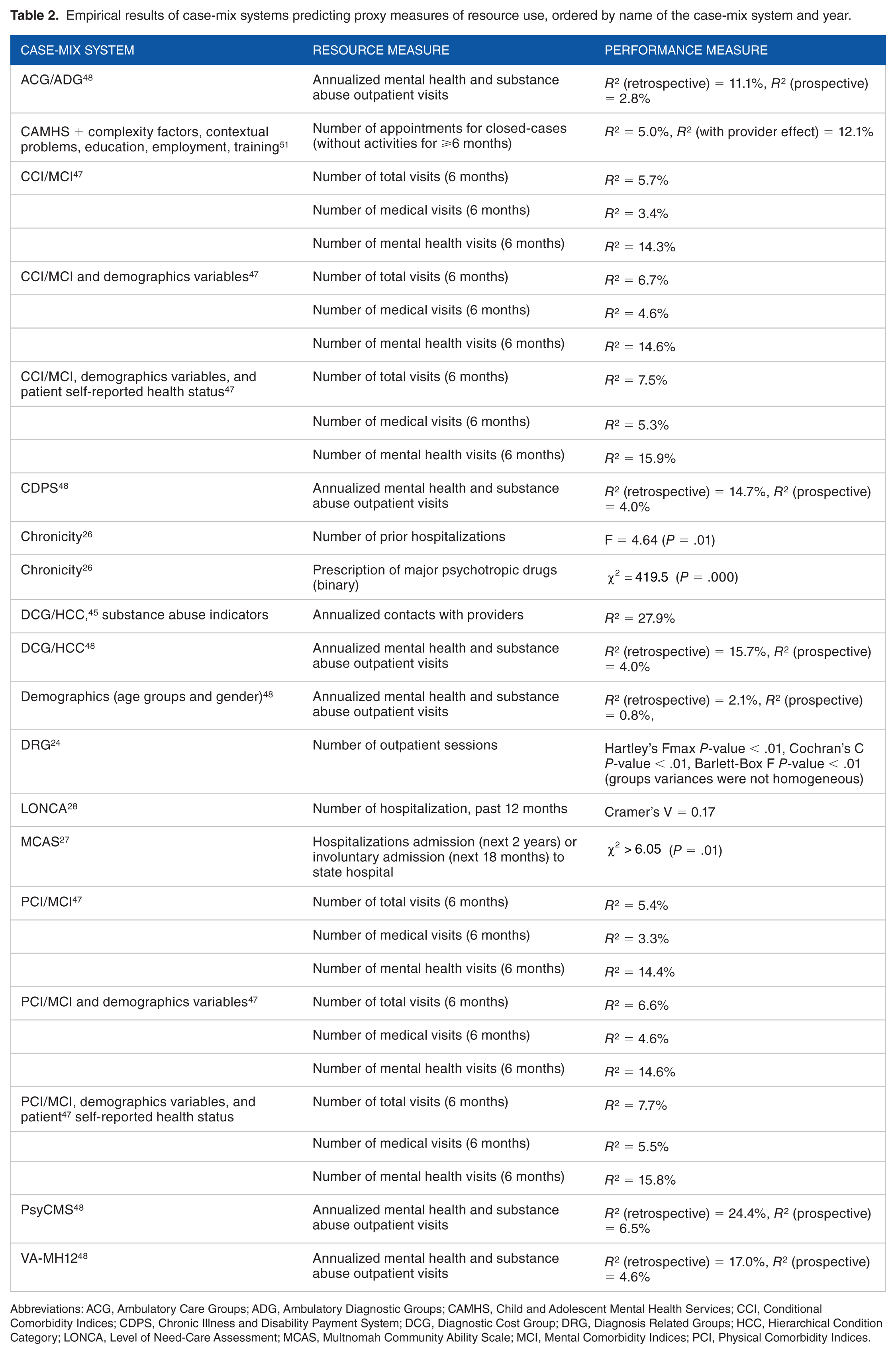
Abbreviations: ACG, Ambulatory Care Groups; ADG, Ambulatory Diagnostic Groups; CAMHS, Child and Adolescent Mental Health Services; CCI, Conditional Comorbidity Indices; CDPS, Chronic Illness and Disability Payment System; DCG, Diagnostic Cost Group; DRG, Diagnosis Related Groups; HCC, Hierarchical Condition Category; LONCA, Level of Need-Care Assessment; MCAS, Multnomah Community Ability Scale; MCI, Mental Comorbidity Indices; PCI, Physical Comorbidity Indices.
Empirical results of case-mix systems predicting direct measures of resource use, ordered by name of the case-mix system and year.
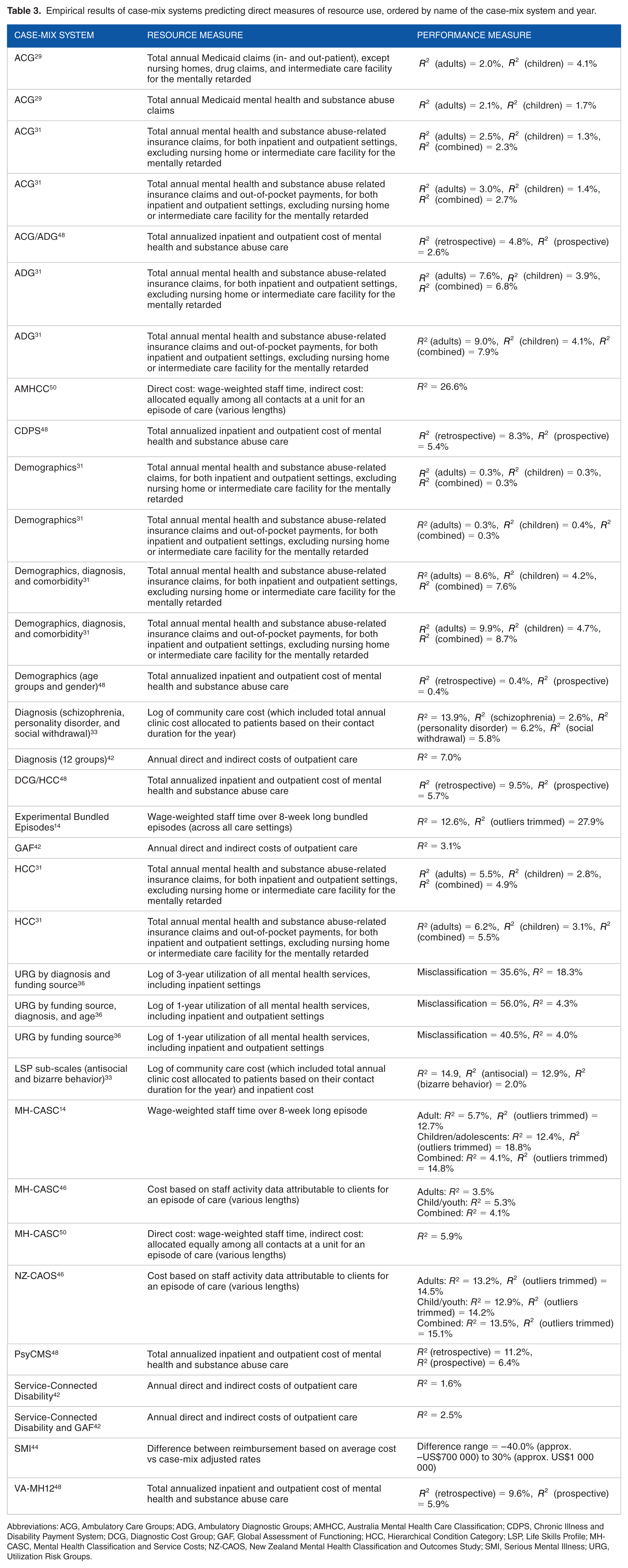
Abbreviations: ACG, Ambulatory Care Groups; ADG, Ambulatory Diagnostic Groups; AMHCC, Australia Mental Health Care Classification; CDPS, Chronic Illness and Disability Payment System; DCG, Diagnostic Cost Group; GAF, Global Assessment of Functioning; HCC, Hierarchical Condition Category; LSP, Life Skills Profile; MH-CASC, Mental Health Classification and Service Costs; NZ-CAOS, New Zealand Mental Health Classification and Outcomes Study; SMI, Serious Mental Illness; URG, Utilization Risk Groups.
For the direct measures, all studies used episodic basis for their resource use measures, which summed all the relevant costs over an episode of care. Only two studies attempted to define episodes of care that were variable based on the group or case,46,50 while the others pre-defined a fixed episode length for the entire sample. There were also a wide range of follow-up times used for measuring resource use (Tables 2 and 3), ranging from a few weeks to up to 3 years. Alternatively, another option is to calculate a direct resource use measure on a per-diem basis, which predicts resource use per day or per visit, 5 such as the System for Classification of In-Patient Psychiatry (SCIPP) developed in Canada. 54
The measures of resource use could also be expressed as a continuous variable or a categorical variable. As a result, there were also various performance metrics used to evaluate the case-mix classification systems, but most common was the coefficient of determination (R2) for the measures of resource use expressed as a continuous variable (Tables 2 and 3). The R2 was sometimes referred to as the reduction in variance (RIV), or the amount of variance in resource use explained by the case-mix classification system. Although the R2 was commonly reported, the differences in the measures of resource use and follow-up duration did not allow for a meaningful comparison.
Since the distribution of the resource use was often positively skewed, some studies attempted to approximate a symmetric distribution with a log transformation33,36 (Table 3). Some studies also trimmed the outliers to improve their predictive performance14,46 (Table 3).
There were also other notable case-mix classification systems currently being used, where activity-based funding has been implemented, such as the Netherland’s Zorgzwaartepakketten (ZZP) and the UK’s Mental Health Clustering Tool (MHCT) but, to our knowledge, these did not have empirical results regarding their predictive performance. The ZZP has 38 psychosocial care packages which classifies all ages based on psychosocial or cognitive functioning, social skills, mobility, activities of daily living, and behavioral problems. 17 The MHCT has 21 groups which used the Health of the Nation Outcome Scales (HoNOS) 37 as input, then classifies adults using diagnosis, severity, chronicity, and cognitive impairment. 55 An earlier version of the MHCT with 13 groups reported an R2 = 10.9%. 56
Discussion
Principal results
A modest number of studies examined case-mix classification systems to predict mental health care resource use in the community settings. A direct comparison in terms of predictive performance was not possible due to the variation in the measures of resource use, the follow-up duration, and performance metrics. In general, it can be said that the large majority of the variation in community mental health resource use was still not accounted for by these case-mix classification systems.
Although most research on this topic came from the Unites States, the Australian system (AMHCC) was most comprehensive, covering all ages and care settings (inpatient and community settings). 50 The most recent refinement was the addition of five phases of care (assessment only, acute, functional gain, intensive extended, and consolidating gain) which reflects the goal of care. 50 These phases of care are intended to serve as a proxy for a person’s health care needs and, by extension, a person’s expected resource use driven by health care needs.
Input variables
It is worth acknowledging that when a case-mix classification system is used in a funding formula, it must ensure that resources are allocated equitably. Therefore, whether a variable should be a case-mix input variable is an important consideration. In the literature, the variables used for classification were often grouped into only a few categories such as demographics, diagnosis, clinical status, or treatment variables. Discussions regarding their appropriateness as case-mix variables were also rare. Using an alternative classification of these variables, this study summarized the scope of case-mix variables used in the literature and discussed how case-mix variables can influence funding allocation (Table 4).
Input variables and their alternative case-mix classifications.

Needs Variables
Variables that indicate the level of health care needs are those that not only have high explained variance of the resource use, but should also be variables that directly drive the resource use. For example, ethnicity 46 and gender29,31,48 may have high correlation with resource use, but such correlation may be confounded by other factors such as systematic marginalization in the society that can make someone more vulnerable to mental health disorders and, by extension, to have higher expected level of resource use. Therefore, future research should consider variables that directly drive resource use, such as diagnosis, functional status or severity of illness, instead of those that simply correlate with resource use.
Individual vs Provider Variables
Provider variables, in essence, describe why it costs more in one facility compared with another, regardless of the person’s health care needs. For example, these can be care setting, facility type, regional characteristics, staff qualifications, or teaching status. Using these variables as case-mix variables essentially reinforces the systematic inequalities that exist among the providers. Therefore, using variables related to the individuals, whenever possible, may help avoid this reinforcement. However, in some cases, reinforcing systematic inequalities may be desirable, such as adjusting for facilities located in rural areas where resources and supplies may cost more to be delivered. As mentioned, these may also be adjusted for in a funding formula as external factors, so that the case-mix system maintains its focus on the health care needs. Only the case-mix classification systems from Australia and New Zealand used care setting as a case-mix variable, but they were used as the first split to essentially join 2 separate case-mix systems for inpatient settings and community settings together.14,46,50
Process Variables
Process variables are those that describe treatments or services given to a person.14,46,50,51 When using treatments or services as case-mix variables, they may encourage providers to do more of them for financial gain if they are under the control of the providers. Similar to provider variables, consideration should be given to whether variables that describe the needs of the individuals should be used as much as possible, or if there is a valid rationale for reinforcing differences in such variables (eg, to incentivize certain practices).
Historical Variables
Variables that describe historical use of services or treatments provided can be viewed as proxies for historical needs, such as prior hospitalization, 26 or usage in a prior year. 36 The shortcoming of these variables is that they have limited ability to be modifiable and change with current needs. On the other hand, there are historical variables that are continued to be relevant to current needs, eg, past history of abuse or violence. 14 Historical variables therefore should not be entirely discounted, but the important consideration is whether historical variables have long-term relevance in describing a person’s current health care needs, or whether another variable that is more dynamic and could change with a person’s health care needs may be more appropriate.
Ambiguity of Variables
Ambiguity may arise if the variables chosen to describe the patient type result in more than one way to classify an individual. This ambiguity may give providers an incentive to choose the classification that maximizes the reimbursement, especially if the differences in the expected resource use or reimbursement of the possible classifications are significant. Given the same input, a good case-mix system should be able to consistently classify a person to only one group.
Studies in this review primarily obtained their input data from administrative sources or clinical assessment data. While administrative datasets offered convenience, they may only contain a few variables of health care needs, such as diagnosis codes. Instead, it may be more advantageous to use clinical assessment data designed to measure needs as part of the care plan creation. However, not all clinical assessments are created equal. Future research should consider the assessment that appropriately matches the clinical context (eg, mental health specific vs general medical assessment, inpatient vs community, children vs adults), and as comprehensive as possible to capture: needs, individual, provider, process, and historical variables describing an individual.
Output variables
The use of proxy measures of resource use was common in this review, such as the number of visits or appointments (Table 2). In fact, one of the first case-mix classification systems, DRG, used length of stay as a proxy for an inpatient episode’s cost. 25 This approach assumed that costs of care do not vary day-to-day during the hospitalization. 54
Similarly, for direct measures of resource use, when assuming that the costs of care do not vary day-to-day or visit-to-visit, it is also possible to calculate the costs of care for a particular case on a per-diem basis by multiplying the number of days/visits with expected cost per day/visit. However, the studies using direct measures of resource use found in this review all calculated costs of care on an episodic basis with a pre-defined follow-up length (Table 3). In an analysis from Australia, the preferred method of predicting resource use in community settings was a pre-defined episode with fixed length, due to the chronic nature of mental health care and intermittent provision of community-based services. 14 This differs from the continuous service consumption of inpatient settings.
The class of direct measures of resource use can be further divided into billed costs (eg, claims data) or observed costs (eg, staff time study). Billed costs have three main limitations. 54 First, they often include non-clinical administrative costs (such as management, claims department), which could reduce the variance in the resource use measure if the administrative costs are high relative to costs of clinical care. 54 Second, sometimes billed costs are derived by averaging over a large number of patients rather than the actual amount an individual patient consumed, 54 which could also reduce the variance in the resource use measure. Third, additional variance can be added if there is a lot of variation in accounting practice across different organizations. 54 On the other hand, observed costs like staff time activities are more likely to closely match the actual resource consumption by individual patients and potentially more responsive to patients’ characteristics, 54 but these may be harder to obtain than available administrative data.
Gaps in current research
There are many available case-mix systems that were developed for inpatient settings but were not tested for community settings. Creating a case-mix system is not a trivial process; however, considerable progress can be made by experimenting with existing case-mix systems developed for use in another setting. For example, Canada’s SCIPP is a good candidate for testing in community settings. This system was able to explain 26.3% of variance in inpatient psychiatry cost, which is higher than most of the identified case-mix systems. 54
It has been shown that children and adolescents also have unmet mental health care needs. 57 Most of the studies only focused on adult populations (Table 1). Therefore, future case-mix classification systems should also consider children and adolescent populations in the development of new case-mix systems.
Only three of the studies cross-validated the predictive performance of their systems on a different data set than the one used for model derivation.45,48,51 Cross-validation can serve two purposes: to evaluate the generalizability of the model on unseen observations or future users of the health care system, and to compare competing models. 58 Future research should consider using cross-validation when evaluating the predictive performance because the uncross-validated performance metric may give an overestimation.
Finally, it was not always clear if there exists a process or mechanism for updating the case-mix systems and exchanging knowledge. The pattern of health care resource consumption could potentially change between pre- and post-implementation of case-mix funding. Therefore, it is important to have a robust feedback loop by conducting more replication studies to validate case-mix systems under different conditions, as new data become available if using administrative data, or with more participating sites and over different time periods if using staff time activity data. For example, Australia has an organization dedicated to continuous improvement of case-mix classification systems with more replication studies planned. 50
Limitations
This study was not without limitations. First, this study only examined articles written in English, which also limited our review to only English-speaking jurisdictions. Second, the future of case mix classification systems within funding formulas was not clear from this review. This study did not consider the implementation outcomes and policy impacts of the identified case-mix systems, which deserves a separate review in the future.
Conclusions
This study provided a summary of the scope of research in community mental health care case-mix classification. The research activity was modest, while the transition from institutionalization to community care continues to evolve. Consideration should be given to appropriateness and assumptions of the case-mix variables, resource use measure, and evaluation of predictive performance. More research, especially of replication type, is needed in community mental health to ensure resources are meeting the needs of the population as new data become available and as the health care system evolves overtime. The introduction of standardized assessment systems into community mental health services should be considered as a foundational step toward establishing a pervasive common data source for clinical variables to be used in community-based case-mix systems.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NT was supported by the Ontario Trillium Scholarship by the Government of Ontario, Canada. This research was also partially supported by interRAI Canada. The opinions expressed were only of the authors.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NT and JWP created the search criteria. NT, CP, and JPH contributed to the literature search. NT performed the primary screening. All authors contributed to the writing of the manscript and approved the final manuscript.