
Abstract
In Norway, approximately 50% of older people die in nursing homes (NH). Holistic care and pharmacological management are key factors in quality at the end of life. The purpose of this longitudinal study was to describe the use of opioids in an NH during a 5-year period. We focused on palliative care, symptoms, and suffering during the last 3 days before death. Data were collected from spring 2013 to spring 2018. We used the interRAI assessment instrument annually and when the resident died. We conducted a semi-structured interview with nurses on duty at the deathbed. At the time of death, the residents had an average age of 88.9 years and an average stay of 2.9 years (N = 100). At the first assessment, 19% of the residents used 1 or more type of opioids. On the day of death, 55% had an active prescription for opioids, mainly as subcutaneous injections. The results illustrate the different uses of opioids, including managing pain, dyspnoea, sedation, for comfort, as a prophylaxis, or a combination of reasons. Cancer- and cardiovascular diagnoses were the strongest predictor for using morphine (P < 0.05). Identification of the residents’ needs for opioids is a challenge for palliative care nurses, both ethically and legally.
Background
The international modern hospice movement started in England with Dame Cicely Mary Saunders in the 1970s. She worked to improve care and treatment for cancer patients at the end of life. In Norway, health politicians have shown little interest in the hospice movement 1 with only a few hospices founded by devoted nurses and physicians. At the end of the 1990s, a group of health care professionals wanted to transform ideas from the hospice movement in England to other types of care institutions. Consequently, the Liverpool Care Pathway (LCP) for Care of the Dying Patient and their next of kin was developed for use in hospitals and nursing homes (NHs). 2 In 2017, The LCP documents were rewritten and adapted to Norwegian health care, although the name was changed to the Last Days of Life.
To date, this plan has been implemented in 328 (33%) of the NHs in Norway, with support from the health department. Notably, in Norway, the physician writes an ‘advanced directive’ in the medical records when nurses observe a significant clinical change in the residents’ health conditions. The main key for symptom control during the terminal phase in an NH is a standardized medication ‘kit’. 3
The Norwegian welfare political model ranks institutional care as the gold standard for care of older people. Few relatives are able to perform around the clock care due to Norway’s low unemployment rate, which is presently 4.0%. 4 In Norway, approximately half the population dies in an NH with the average length of stay (LOS) being around 730 days. The municipalities own 88% of all NHs. 5 The main reason for admission to an NH is cognitive impairment. In Norway, about 80% of the residents have symptoms of dementia, in spite of relatively few residents having a specific dementia diagnosis according to international classification of diseases 10th revision (ICD-10). 6 Optimal pain management is challenging for health professionals in NHs. The residents have problems expressing their needs and therefore providing optimal treatment for pain is difficult. 7 For example, 1 study registered pain by structured face-to-face interviews. The next of kin thought that the resident experienced pain more frequently than nurses or care assistants did and twice as often as assessed by the residents themselves. 8 In another study, the researcher discussed how various psychiatric disorders, other than dementia, may affect pain assessment and treatment in NHs. 7
Furthermore, in a study of 12 NHs, the staff regularly conducted pain assessment. However, these authors underlined that an assessment tool is needed to indicate the presence or absence of pain in severely cognitively impaired residents. 9 The results of a European study that included 7 European Union (EU) countries plus Israel, known as the SHELTER (Services and Health for Elderly in Long TERm Care) Study, revealed considerable differences in pain management across European countries. Factors positively associated with pharmacological pain management were being female, having cancer, and experiencing moderate or severe pain. 10 The purpose of this study was to describe the use of opioids in an NH during a 5-year period, focusing on their use related to palliative care, symptoms, and suffering during the last 3 days before death. We used the displayed data to follow up the opioid use in the NH:
To document the differences in opioid use at admission and at death;
To document the types of reasons for the use of opioids near death;
To illustrate guidelines for appropriate opioid use; and
To document changes in resident characteristics and opioid use between first assessment and death.
Methods
Setting
This study setting was a non-profit NH in Oslo with 70 beds. The owner and the administrative leader were supportive of the study, defining it as a quality insurance project. Only a few of the next of kin refused participation of their demented relative. Data collection started in the spring of 2013 with 63 residents and new residents were recruited. The researchers assessed the patients annually and at time of death. Ten patients were discharged or removed to another NH and were excluded from the study. Altogether, 100 residents were included in the study. Twelve of the residents were transferred to a hospital for examination or for acute medical treatment and died unexpectedly after a few days in the hospital. The staff in the NH had contact with the hospital staff and received information about the last days of the resident’s life.
We did not meet the residents or have access to the electronic patient records. One of the researchers went through the assessment tool together with the patient’s primary contact nurse. Both were responsible for the quality assurance of the data. The nurses were aware of their responsibilities according to ethical guidelines and national regulations. The study did not require regional ethical committee approval for medical and health professional research.11,12 The project followed ethical guidelines for social sciences, humanities, law, and theology. 13 The resident or the next of kin was informed about the project and signed a written informed consent form.
Quantitative data
At the first assessment, a few of the patients had lived in the NH for several years. The quantitative part of the study considered the patients’ needs for medical treatment and care. We collected data using an assessment tool, the resident assessment instrument for long-term care facilities (RAI-LTCF), known as the interRAI, version 2.0. The instrument has been translated and back-translated, with good content, face validity, and inter-observer reliability. 14 The different variables on the RAI are expressed in several scales generated with the analysis tool RAIsoft (www.raisoft.fi).
The Activity of daily Living scale (ADLH) ranges from 0 to 6 and includes help with personal hygiene, movement, toileting, and nutrition, with a value ⩾3 indicating comprehensive help. 15 The Cognitive Performance Scale (CPS) is a 6-point scale evaluating memory with a value ⩾3 indicating moderate to severe problems. 16 The Communication scale (COMM) ranges from 0 to 8 and encompasses two 4-point items that assess making oneself understood and having the ability to understand others. On this scale, a value ⩾4 indicates moderate to severe cognitive impairment. The Depression Rating Scale (DRS) ranges from 0 to 14, with a value ⩾3 indicating depression. 17 Finally, the 5-level pain scale summarizes pain frequency and intensity with a higher score indicating more intense pain. 18
The analysis tool generated algorithms using the resident assessment instrument software (www.raisoft.fi). Descriptive statistics and statistical analyses were performed using IBM SPSS software, version 25. We used a cross-table calculation to compare characteristics and clinical features like the central diagnosis, functioning status, body mass index (BMI), and central symptoms to document changes between the first and the last assessment (Table 2). Then, we added a forward logistic regression analysis with morphine as the dependent variable.
Qualitative data
The NH office contacted the project leader after a resident died. A soon as possible, we carried out an interview with the nurse who had been on duty during the time of death. In addition to RAI-LTCF, open questions were asked, including the reasons for the resident’s use of opioids and how the nurses perceived the resident’s palliative phase. The nurses brought the nursing notes from the last 3 days of the resident’s life, containing information such as psychosocial support, symptoms, and medication. In addition, we collected special observations and reflections that were documented. The nurses’ descriptions and assessments of the residents’ care were written in the electronic notes section in RAIsoft and we analysed the text. The notes for each resident were read, coded, and discussed to gain information regarding their observations on the use of opioids. We organized the text according to the main reasons for giving opioids. To describe the nurses’ information like this has value in presenting and treating research factors as living entities that resist simple classification. We used a descriptive qualitative design to interpret and discuss the data.19,20
In this NH, the doctor works 16 h/day each week, spread over 4 days, and can be called in during the day or evening. The nurses may start a standard procedure for palliative care after consulting with the physician (Table 1). Otherwise, the staff is dependent on contacting the central emergency service when needed.
The 4 important medications for alleviation of suffering in the terminal phase. 3

Abbreviation: sc, subcutaneous; po, per oral.
Observation: Both Midazolam and Robinul are used here without accepted indications. The enclosed treatment algorithms are developed upon large documentation on the effects of these medications among the terminally ill. The doctor in charge should be aware of their responsibilities when using drugs outside approved indications.
Results
The background data included the number of assessments, sociodemographic data, primary diagnosis, functioning status, nutrition status, and central symptoms (Table 2). The majority of residents were females. Cardiovascular disorders were the most frequent diagnoses along with cognitive decline. Pneumonia was often present at the end of life, whereas cancer and stroke were among the 6 most common diagnoses in this sample.
Characteristics of residents at first assessment and at death (N = 100).
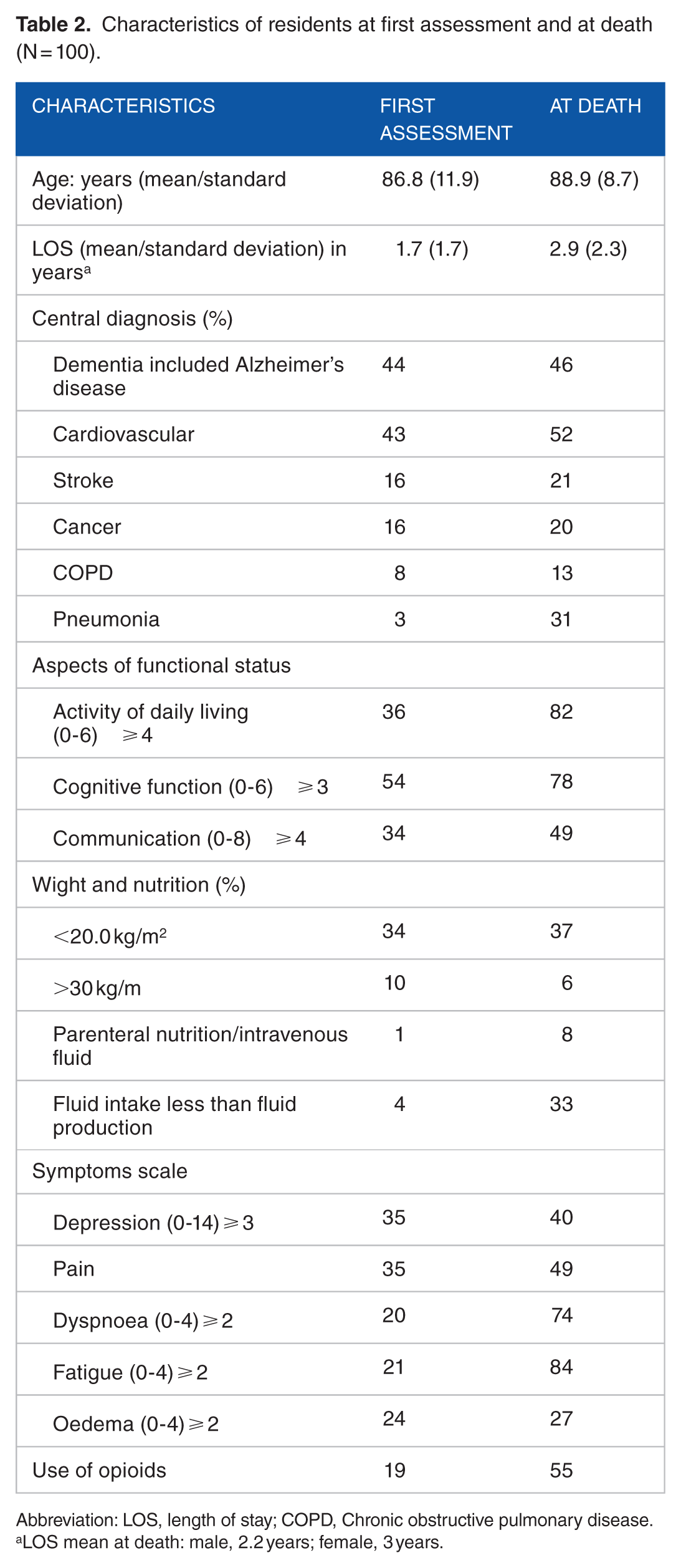
Abbreviation: LOS, length of stay; COPD, Chronic obstructive pulmonary disease.
LOS mean at death: male, 2.2 years; female, 3 years.
Different aspects of the patient’s functional status, such as activities of daily living, cognitive function, and communication, declined before the time of death. A logistic forward regression analysis gave non-significant result. The same test compared the use of opioids at first and last assessment. The characteristics with significantly different values were cancer diagnoses (P = 0.048 and odds ratio [OR] = 3.9), heart/coronary disease (P = 0.023 and OR = 3.49), or suffering from dyspnoea (P = 0.074 and OR = 3.2).
The number of residents receiving the different types of opioids is presented in Figure 1. In this study, 55% of the residents received opioids during their last days. Several of the patients used more than 1 type of opioid, including morphine, buprenorphine, oxycodone, and combinations of oxycodone, naloxone, fentanyl, hydromorphone, or other opioids.

Number of subscripted opioids during the first and the last assessment (at death).
At the first assessment, the majority of the residents (N = 81) did not use any opioids. At the last assessment, 1 type of opioids was most common, 8 residents use 3 or more types of opioids.
What are the factors associated with the use of opioids in NH residents close to death?
The data analysis revealed 6 reasons why the nurses used opioids: pain, sedation, dyspnoea, comfort, prophylaxis, or a combination of reasons (Figure 2).

The reasons for using opioids close to death.
The main reason to give opioids was pain (22%) or a combination of different reasons (22%). Opioids were used as a prophylaxis (18%) or for comfort (13%). In the case descriptions, the main reason for the administration of opioids was dyspnoea (14%) and need of sedation (11%).
For each reason, we have listed examples and cases to illustrate the different types of opioids and mode of administration, together with the most common use of palliative medications in the last days of life. We also present short descriptions from the additional information provided by the nurses.
Pain
(a) Family members complained a patient had not received enough medication and was in pain; as a result, 2 days before she died, she started on morphine (5 mg) subcutaneously (sc) regularly. (b) A patient experienced a lot of pain before the morphine dose was increased in the last days to 5 to 10 mg sc 6×. (c) After some time, a patient made eye contact with another resident showing her pain, so she received morphine. (d) A patient with cancer was followed up by a pain team at another hospital and received a pain pump (CADD-Legacy). (e) A patient made painful face expressions, had difficulty breathing, and seemed to have pain in her whole body. First, she received oxycodone (2.5 mg) with a moderate effect. At 9:50 p.m., she received 2.5 mg of morphine using a butterfly needle.
Dyspnoea
(a) A patient was heaving after each breath and received oxygen, furosemide (40 mg), and glycopyrronium bromide (0.2 mg) at 10:00 p.m. She received morphine (2.5 mg sc) because of intense respiration problems and struggling for breath. (b) A patient had difficulty breathing, was somnolent, and was able to make contact, yet had no pain. The doctor was contacted per telephone and ordered morphine (2.5 mg sc). (c) There was a sudden change in breathing and a patient received morphine-scopolamine (2.5 mg sc). (d) A patient had fast and shallow breathing. The last night she received 0.5 L of oxygen through a nasal catheter throughout the night. The patient had received morphine (2.5 mg) from the night nurse in charge.
Sedation
(a) A patient did not look as if she was in pain when being bathed. The doctor recommended to continue with a pain regime and increased morphine-scopolamine (5 mg sc every 3-4 h). (b) A patient was bedridden with stable respiration but struggling with her body. The pain regime included morphine every 4 h, with an increase if needed.
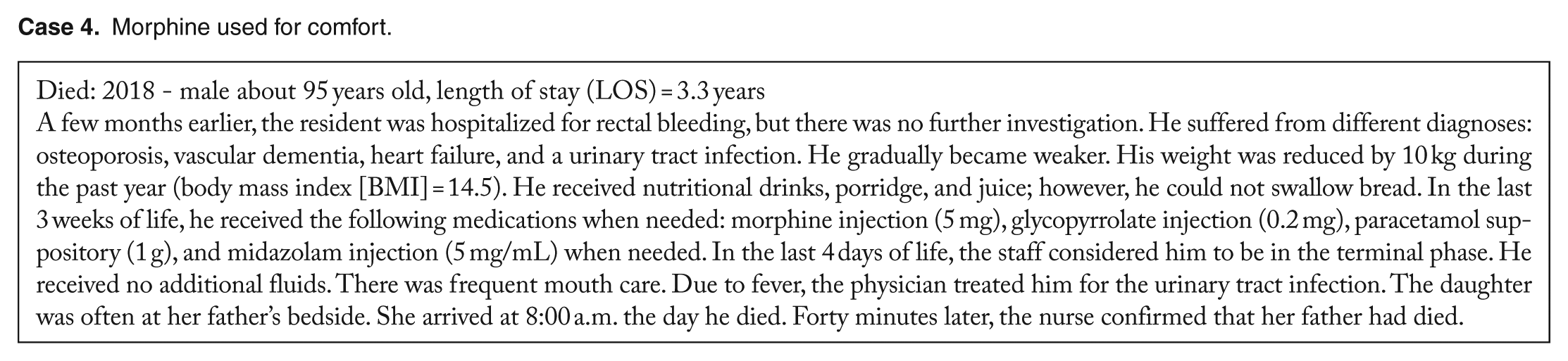
Comfort
(a) A patient suddenly had a high fever 3 days before she died. The family wanted only palliative care with morphine (sc 2.5 mg 3×). The patient died peacefully. (b) When the staff realized that a patient was dying, the doctor was contacted by telephone. Morphine (2.5 mg) was ordered every 4 h. (c) It was difficult to know how much a patient understood the last days as she could not communicate. A paracetamol suppository and morphine sc were started.
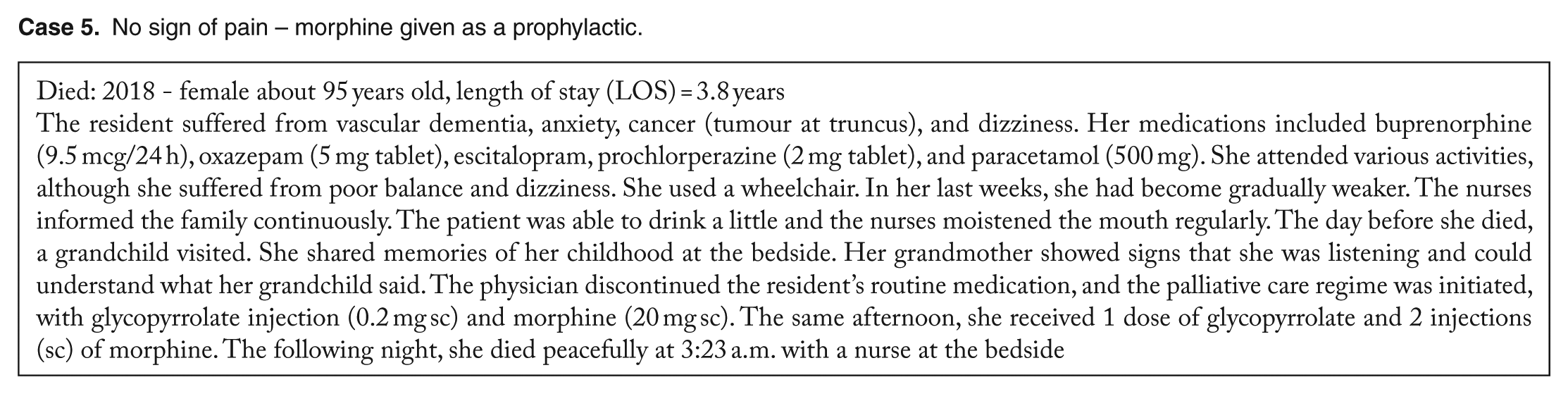
Prophylaxis
(a) Two weeks before a patient died, the nurse contacted the doctor and he prescribed morphine (2.5 mg sc) as needed. On the last days, the nurse gave morphine regularly and there was ‘no sign of pain’. (b) The nurse called the doctor who ordered morphine by injection. (c) A patient became worse during the night and the family was contacted. The patient received morphine (2.5 mg sc), when she became restless, as a prophylactic. (d) A patient died surrounded by others. He had fast and shallow respiration. A butterfly needle was inserted sc in the right arm and the patient was give morphine (2.5 mg) at 1:00 and 6:00 p.m. as a prophylactic. (e) A patient refused all treatment. The last day she was willing to receive medication, a butterfly needle was inserted, and she was administered morphine.
Combination of reasons for opioid treatment
(a) A patient was uneasy and had pain and difficulty sleeping. She received morphine (5 mg sc 3×) using a butterfly needle, together with diazepam (2 mg) with some effect. (b) A patient was sad, depressed, and, at times, confused. She received diazepam (10 mg) as a suppository due to agitation and anxiety, intense pain, and respiratory tract secretion. She received furosemide (20 mg intramuscular [im]) together with morphine (2.5 and 5 mg sc) at 9:45 pm with good effect. (c) A patient knew he was dying, but showed anxiety the closer he became to death. He received diazepam and paracetamol suppositories and morphine (2.5 mg sc) as needed.
Morphine use for pain control.

Morphine use for sedation.

Morphine use for respiration problems (dyspnoea).

Morphine used for comfort.
No sign of pain – morphine given as a prophylactic.
Discussion
In this longitudinal study, we followed an NH population in Norway over a 5-year period. When this study started, the residents had lived in the NH for an average of 1 year. The threshold for admission to an NH is higher today than it was a few years ago. Consequently, the Norwegian coordination reform 21 encouraged municipalities to expand local primary health care and reduce hospital admissions and LOSs. About half of the residents had dementia or an Alzheimer’s disease; this seems to be under diagnosed. Our sociodemographic characteristics show that the majority of the residents were assessed to have moderate to severe problems with cognitive performance. This is similar to data from a Norwegian NH study (N = 2983) with 2 cross-sectional samples and 83% of the participants having mild to severe dementia. 22
The residents’ general conditions were relatively stable until marked changes occurred at the end of life. This is reflected in the number of subscripted opioids during the first assessment and at death. Several of the residents in this current sample suffered from heart disease, dementia, pneumonia, stroke, cancer, and Chronic obstructive pulmonary disease (COPD) as the main causes of death. The SHELTER Study included 500 NH residents from 5 European countries who died within 6 months after their last RAI assessment. Fatigue was reported to be an important factor for predicting a more accurate prognosis. 23 In the current study, fatigue and the residents’ functional status decreased. In this population, the patients used different types of opioid tablets during their stay in the NH. The use of morphine on the day of death was statistically significantly higher than at admission. The oral route of administration was more common at the residents’ first assessments. On the day of death, the nurses used sc injection of morphine, as documented in the presentation of the cases. These data correspond with a study in the Netherlands evaluating the routes of administration of prescribed drugs. Prescribed morphine increased from 21% to 87%, and the oral route of administration changed to sc on the day of death. 24
Decreased appetite could indicate that one has lost an ‘appetite for life’. In this current study, the staff seldom administrated parenteral nutrition or intravenous fluid. As exemplified in case 3, when the resident was not able to eat or drink, the nurses moistened the resident’s mouth regularly. It is important to manage poor nutritional intake to help prevent dehydration and pneumonia. Parenteral hydration might be helpful but can also contribute to discomfort at the end of life. For example, the administration of 1 L of normal saline per day in dying cancer patients did not improve symptoms, quality of life, or survival compared with placebo. 25 The use of opioids reduces the residents’ ability to stay awake. Frequent moistening of the mouth is one of the most important measures to alleviate the sensation of thirst in dying people.
The reasons for the use of opioids varied and seem to have temporary motivation. Pneumonia is a frequent factor triggering the end of life. It can be challenging to assess whether the NH resident has a terminal pneumonia that will lead to death or a pneumonia that could be treated to improve their functional status and general condition. One solution could be to conduct a trial with antibiotics for a period of 3 days. If the resident’s health condition deteriorates further or there are no changes, antibiotics should be discontinued, while treatment should continue if the health condition improves. 26 In this current study, the policy in the NH was to treat residents in their ‘own’ bed. Opioids could have been given due to dyspnoea or for comfort. This is according to the goal of symptom control without life prolongation in advanced dementia. A large proportion of the residents experienced dyspnoea, which is a subjective phenomenon, such as pain. However, respiratory distress, such as the use of auxiliary muscles, cyanosis, increased respiratory rate, and a decrease in oxygen saturation, can be observed by health care professionals and relatives. For some residents, morphine could have been administered to manage dyspnoea instead of pain. Research shows that administration of morphine could be an effective measure to manage dyspnoea and that small doses may suffice. 27 In opioid-naive patients, it is important ‘to start low and go slow’. Careful monitoring and individual dose titration are important. Several of the residents who were transferred to a hospital were struggling with respiratory problems. Neither medication, oxygen, nor a ventilator appeared to reduce their suffering.
The World Health Organization (WHO) is concerned about older people and claims that residents experience pain, which is often not well treated and sometimes not treated at all. 28 In Norway, palliation with the use of opioids has often been associated with cancer patients. In our study, residents with a cancer diagnosis used opioids significantly more often than non-cancer residents.
Early registration of symptoms of pain could improve communication about death and dying with the residents and their next of kin. In an interview study with 50 next of kin in 2 NHs, who had been present immediately prior to and after the death of their family member, results showed that the relatives wanted exact information and better communication. The next of kin recommended that staff should take initiative for both written and oral communication. 29 It is important to ask the next of kin about their assessment of whether their loved ones have pain, because they know the resident well and could assist in identifying subtle, less obvious changes in behaviour that may be indicators of pain presence. 30 In improving communication, the physician should also ensure the family that, in due time, palliative care would be provided in the NH and sufficient analgesics would be given.
Polypharmacy, including opioids, is a common cause of dyspnoea and fatigue, which is easy to observe, yet harder to treat. In the present study, nurses assessed the majority of the patients as having fatigue in the terminal phase. This resulted in the nurse having to assist the resident in their activities of daily living, including using a wheelchair instead of walking. The aim was to conserve energy for visits from significant others and provide an opportunity to share feelings.
If the resident is in pain, morphine tablets usually follow a 4-h rule. 31 In the terminal stage, the residents may have problems with swallowing; consequently, morphine is administered sc. In Norway, there are different guidelines for the use of opioids or other central medicines, but they are not specific for the NH. During the last couple of years, the NH started to use a medication kit known as the ‘Advanced Directive’ for medication in the terminal phase. This kit includes morphine, midazolam, haloperidol, and glycopyrrolate. 3 As described in the ‘Cases’, the residents received morphine as an sc injection at the end of life. The physician has the responsibility to include a prescription in the resident’s electronic record ahead of time as an ‘Advanced Directive’ or when the resident’s situation has changed. The nurse in charge assesses the resident’s condition and gives medication, relying on her professional, ethical, and legal judgement. As the Cases illustrate, the nurses may seek advice from the physician by telephone.
About half of the residents had reduced communication skills. The staff may have difficulties in assessing pain in non-verbal residents. The nurse’s reflections demonstrate how their assessments may appear unsystematic and the wishes from the resident’s next of kin may be essential for prescribing opioids. The staff sometimes seemed unsure how to assess pain. Lack of knowledge and competence may be related to inconsistent pain assessment; in addition, these assessments can be complicated by the residents’ cognitive and sensory impairments. 32 Furthermore, the large proportion of residents with stroke and dementia, together with communication problems, may affect the resident’s ability to report pain and hinder the nurses’ responses. Pain may be interpreted as dementia-related behaviour or as delirium. A systematic literature review and expert opinion related to end of life care proposed that, during the last days of life, it may be the health care professional’s ability to assess pain, and not pain itself, that declines. 33
It is a great challenge to work in an NH. Working with older people is regarded as less attractive than acute care. In Norway, there is a shortage of medical doctors and registered nurses in NHs; unauthorized nurses account for one-third of the nursing staff. 34 In medical departments in acute hospitals, the staff includes mainly licenced nurses (90%). 35 Furthermore, there is a considerable gap in the standards in palliative vs ordinary wards in hospitals and NHs in Norway. 27 However, comorbidities are high among NH residents. These older patients suffer from serious physical deficits, cognitive impairments, and reduced ability to communicate, and this leads to comprehensive challenges, especially when NHs are understaffed and the workers less educated.
In Norway, the proportion of people dying in NHs has increased from 28% to 48% during the last 3 decades. 36 The average LOS is about 2.4 years. The focus on older people and their need for dignity and a peaceful death is gaining increasing attention in Norway. 1 The administration of opioids has increased after the ‘advanced directive’ and medication kit became standardized. The case examples and notes do not convey why the resident is uneasy or what may be affecting their pain. In this study, questions regarding existential pain were not discussed with the nurses. The medication kit did not include a treatment for peace of mind. Notably, in a study of older people exploring their reasons for desiring an end to life, one of the reasons given was ‘the pain of not mattering’. 37 The increased use of opioids at the last days of life, challenge the nurses to learn about their patients’ hopes and visions early in the palliative phase. The residents’ cognitive functioning was seriously reduced in this study and, as the case studies revealed, nurses and care workers should learn the residents’ preferences early in their stay.
To the best of our knowledge, this is the first longitudinal study following a Norwegian NH population over a 5-year period, focusing on death and dying. Some of the residents had resided in the NH for several years before the first assessment; others had lived there a shorter period. Some older people stay in their own homes with extended home care service, while those in this study were in a situation where they had to apply for permanent residency.
A limitation of this study is that the population was a representative sample from only 1 NH from 1 geographical area, reducing the generalizability of our findings. Strengths of this study include the documented diagnoses and use of medications, especially opioids. We also presented the different types of opioids used, along with the frequency and medication dosage. We included residents for whom prescription for opioids were ‘as needed’, not as a regulary description. Information from the nurses shortly after the resident died, included the excat doses of opoids. Finally, we presented 5 cases to illustrate individual needs and the frequency and doses in the terminal phase.
Conclusions
The majority of the NH residents were vulnerable, frail older people. The time span from when they were relatively well functioning to bedridden may seem short. The proportion of residents who suffered from daily pain increased from 35% to 49%, from the first assessment to end of life. The use of opioids in the same period increased from 19% to 55%. This may be interpreted in different ways. The characteristic of pain may be more unbearable close to death or the staff may want to facilitate a peaceful death. When the patient is diagnosed as dying, the doctor and nurse prescribe and administer drugs more often.
Attitudes and beliefs that affect decisions about opioid use among health professionals also need to be investigated in the future. Strategies that target the ordering and monitoring of pharmaceutical care at the end of life can be enhanced by legislation. Advanced directives and the use of a ‘kit’ protocol, similar to the one used in the present study, may be useful. The nurses clinical observations are important as palliative care challenges the nurses’ professional responsibilities, both ethically and legally.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
LWS and OEV were responsible for the data collections. All of the authors (LWS, SAS, MHK and OEV), conceived and designed the paper and analyzed the qualitative data. LWS analyzed the quantitative data. All of the author contributed to the writing of the manuscript and agreed with manuscript results and conclusions. Together they have worked through revisions and approved the final version.