
Abstract
Background
Globally, approximately 3.5 billion people lack safely managed sanitation services. In Africa, 45% of the population uses either shared or unimproved sanitation facilities. Ethiopia continues to be ranked among the countries with the lowest levels of hygiene and sanitation coverage. Moreover, many villages and kebeles who have latrine practicing open defecation. So the objective of this study is to assess sustainable latrine utilization and associated factors among open defecation free (ODF) declared villages in Ebinat District.
Methods
A community based cross-sectional study triangulated with qualitative data was conducted from January 17 to February 11/2017 in Ebinat District. Multistage sampling was employed to select study subjects. A total of 752 households were selected by using systematic random sampling technique. Four focus group discussion and seven key informant interview participants were selected purposively to collect qualitative data. The Data entered using Epi Info version 7 and exported to SPSS version 20 for analysis. Crude and adjusted odds ratio with 95% CI were computed to identify the predictors of sustainable latrine utilization. Open Code software was used for thematic content analysis.
Results
The overall sustainable latrine utilization was 31.5 % with 95% CI of (28.2, 34.8). Factors associated by households were presence of children 7-18 years old, attending elementary school [AOR:1.63, 95% CI: (1.09-2.45)], HHs ever visited in a year by health extension workers [AOR:3.15, 95% CI: (1.80-5.53)], HHs ever visited in a year by health development armies [AOR:3.23, 95% CI: (1.99-5.26)] and family member attending Community-Lead Total Sanitation and Hygiene triggering [AOR:1.78, 95% CI: (1.16-2.67)] and distance of latrine from dwelling [AOR:3.22, 95% CI: (1.54-6.72)].
Conclusion
In this study, sustainable latrine utilization is lower than expected level. Therefore, program implementers should prioritize behavioral change interventions, and health workers and HDAs should conduct frequent follow-ups after the ODF declaration.
Plain Language Summary
Background
Globally, 2.4 billion people do not have access to improved sanitation facilities. In African, 45% of the population uses either shared or unimproved sanitation facilities. Ethiopia continues to be ranked among the countries with the lowest levels of hygiene and sanitation coverage. So the objective of this study is to assess sustainable latrine utilization and associated factors among open defecation free (ODF) declared villages in Ebinat District, Northwest Ethiopia.
Methods
A community based cross-sectional study triangulated with qualitative data was conducted from January 17 to February 11/2017 in Ebinat District. A total of 752 households (HHs) were selected by using multistage sampling technique. Four focus group discussion and in-depth interview participants were selected purposively to collect qualitative data. Data were collected using structured questionnaire and observational checklist. The Data entered using Epi Info version 7 and exported to SPSS version 20 for analysis. Crude and adjusted odds ratio with 95% CI were computed to identify the predictors of sustainable latrine utilization. Open Code software was used for thematic content analysis.
Results
The overall sustainable latrine utilization was 31.5 % with 95% CI of (28.2, 34.8). Factors associated by households were presence of children 7-18 years old, attending elementary school [AOR:1.63, 95% CI: (1.09-2.45)], HHs ever visited in a year by health extension workers [AOR:3.15, 95% CI: (1.80-5.53)], HHs ever visited in a year by health development armies (HDAs)[AOR:3.23, 95% CI: (1.99-5.26)] and family member attending community lead total sanitation and hygiene (CLTSH) triggering [AOR:1.78, 95% CI: (1.16-2.67)] and distance of latrine from dwelling [AOR:3.22, 95% CI: (1.54-6.72)].
Conclusion
In this study, sustainable latrine utilization is lower than expected level. Therefore, program implementers should prioritize behavioral change interventions.
Background
Sustainable latrine utilization remains a fundamental yet insufficiently addressed component of global sanitation efforts. According to the World Health Organization and UNICEF Joint Monitoring Programme (JMP), approximately 3.5 billion people still lack safely managed sanitation services globally, and hundreds of millions continue to practice open defecation, particularly in rural areas of low- and middle-income countries. 1 Importantly, evidence shows that access to improved sanitation facilities does not necessarily translate into consistent utilization, as behavioral, environmental, and socio-economic factors strongly influence sanitation practices.2,3 This underscores the importance of focusing on sustainable latrine utilization as a critical determinant of sanitation-related health outcomes and progress toward Sustainable Development Goal (SDG) 6.2.
In sub-Saharan Africa, sanitation challenges remain pronounced, with a large proportion of the population lacking access to basic sanitation services and practicing open defecation. 1 Despite increasing efforts to improve sanitation coverage, many communities experience slippage, whereby households revert to open defecation or discontinue latrine use after initial adoption. 2 This highlights a persistent gap between sanitation infrastructure provision and long-term behavioral change. 3 Sustainable latrine utilization in these settings is influenced by multiple interrelated factors, including socio-cultural norms, affordability of construction materials, technical quality and durability of latrines, and the extent of community engagement and follow-up support. 4 Consequently, sanitation interventions that focus solely on infrastructure without addressing behavioral and contextual determinants often fail to achieve lasting impact. 5
Ethiopia has made notable progress in rural sanitation through the implementation of Community-Led Total Sanitation and Hygiene (CLTSH), which has led to the declaration of many villages as Open Defecation Free (ODF).6,7 These efforts have contributed to a significant reduction in open defecation practices over the past decade. 1 Although Ethiopia has decreased the prevalence of OD from 92% in 1990 to 37% in 2014 8 ; the country continues to be ranked among those with the lowest levels of hygiene and sanitation coverage.
Furthermore, sustaining latrine utilization after ODF declaration remains a critical challenge, with evidence indicating that some communities revert to previous sanitation behaviors over time. 2 Factors such as inadequate post-ODF follow-up and an emphasis on achieving ODF status may sometimes prioritize short-term outcomes over long-term sustainability, leading to gaps in continued monitoring and support. 3
Health statistics indicate that much of the disease burden in the country is preventable and that a considerable proportion is directly related to unsafe water, inadequate sanitation and poor hygienic practices. 9 On average, Ethiopian children experience five to twelve diarrhea episodes a year and more than 250,000 children die annually as a result of diseases related to poor environmental sanitation and hygiene. Moreover, acute watery diarrhea continues to be a threat to the social and economic development of the country.8,10 In the study area, most of the kebeles are rural and use traditional pit latrines, carrying high risk of collapse. Additionally, a majority of the people have negative traditional beliefs regarding latrine use. Therefore, the aim of this study was to assess sustainable latrine utilization and associated factors among ODF-declared villages in the Ebinat district.
Methods and Materials
Study Design and Period
A community based cross sectional study design was conducted to assess the sustainable utilization of latrines from January 17to February 11, 2017.In addition, a qualitative study was conducted to explore associated factors among open defecation free (ODF) declared villages.
Study Area
The study was conducted in the Ebinat district, South Gondar Administration Zone, Amhara Regional State, northwest Ethiopia. It is located approximately 687 km from Addis Ababa, the capital city of Ethiopia. Based on population projections from the Ethiopian Statistical Service, the estimated total population of Ebinat district (district) in 2017was approximately 232,700, of which 117,000 were males and 115, 700 were females. The number of households in the district was estimated to be 60,711. The district is divided into 2 urban and 35 rural kebeles. Among the rural kebeles 15 kebeles with 25,861 households have declared ODF.
11
All households in ODF-declared kebeles of Ebinat district was the source population. The study population was all selected households in selected ODF-declared kebeles of Ebinat district (Figure 1). Map of Ebinat disrict in South Gondar Zone Amhara Regional state, Ethiopia, 2017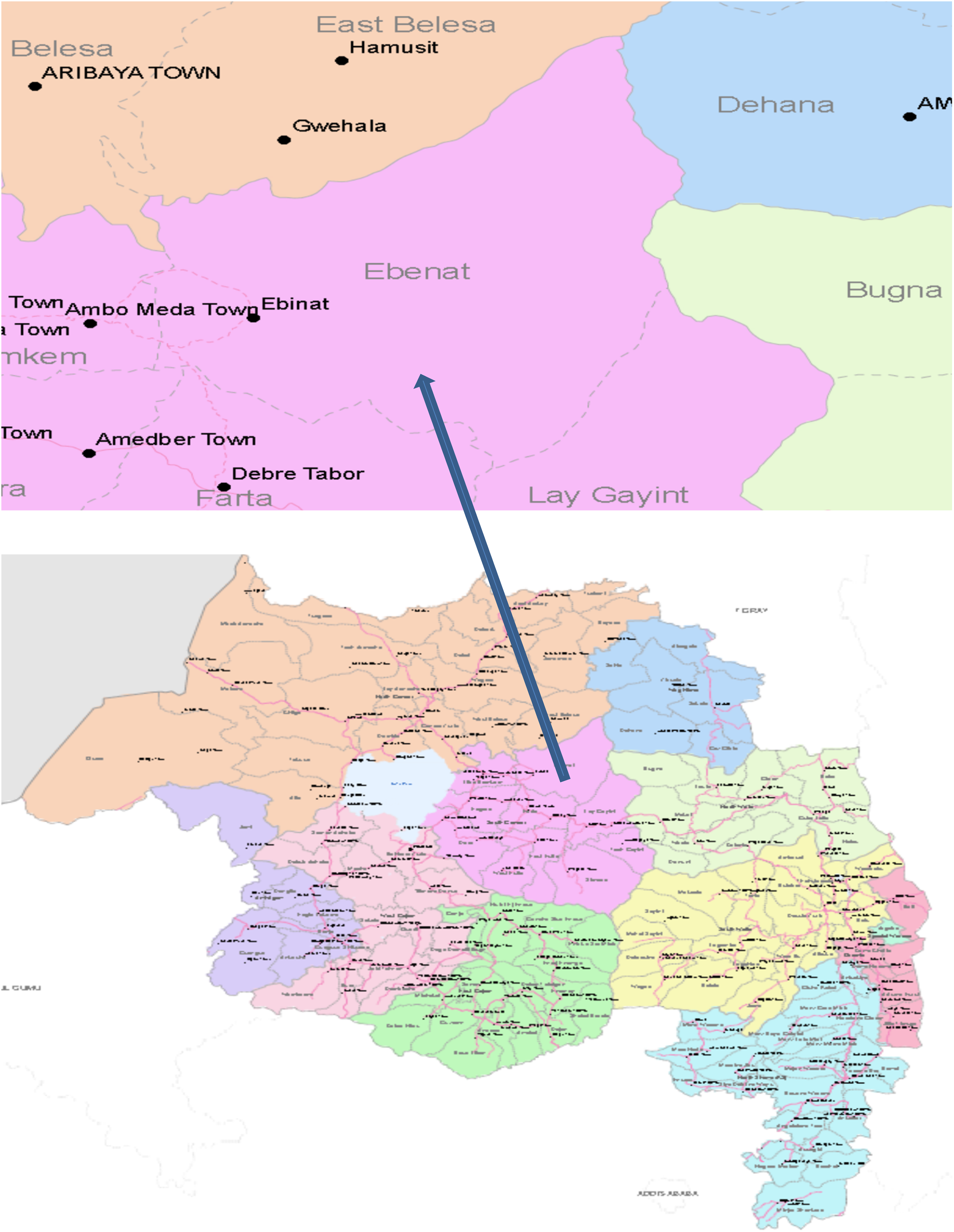
Sample Size Determination
A single population proportion formula was used to determine the sample size based on the following assumptions. A study conducted in rural households of Hawzien district, Tigray, Ethiopia, the proportion of consistent latrine utilization was 37.4%
12
with 95%CI, α-level 5%, and 5% margin of error (d), design effect (D) of 2 and 5% non-response rate was considered. The sample size (n) was calculated as: n=
Participants in qualitative study for key informant interview (KII) and focus group discussion (FGD) were identified through purposive sampling. Four FGD groups, each group containing 8 participants with a total of 32 participants were selected. From this, two women groups (5 participants at Shumgien Sarnko and 11 participants at Wonberoch Woftoma) and two men groups (7 participants at Wonberoch Woftoma and 9 participants at Birkoch)were participated. Participants for key informant interview (KII) were a head of Woreda Health Office (health professional), two HEWs at health post, two religious leaders and two health development armies (HDAs) at communities.
Sampling Technique
Multistage sampling was employed to select study subjects. Five ODF Kebeles which account 33% in the district were selected randomly by using simple random sampling technique. Then the calculated sample size was proportionally allocated to study Kebeles based on their total number of households. The allocated households in Kebeles were selected by using systematic random sampling technique (Figure 2). Purposive sampling technique was employed to recruit participants in qualitative study. Schematic presentation of sampling procedure among ODF declared kebeles of Ebinat disrict, Ethiopia, 2017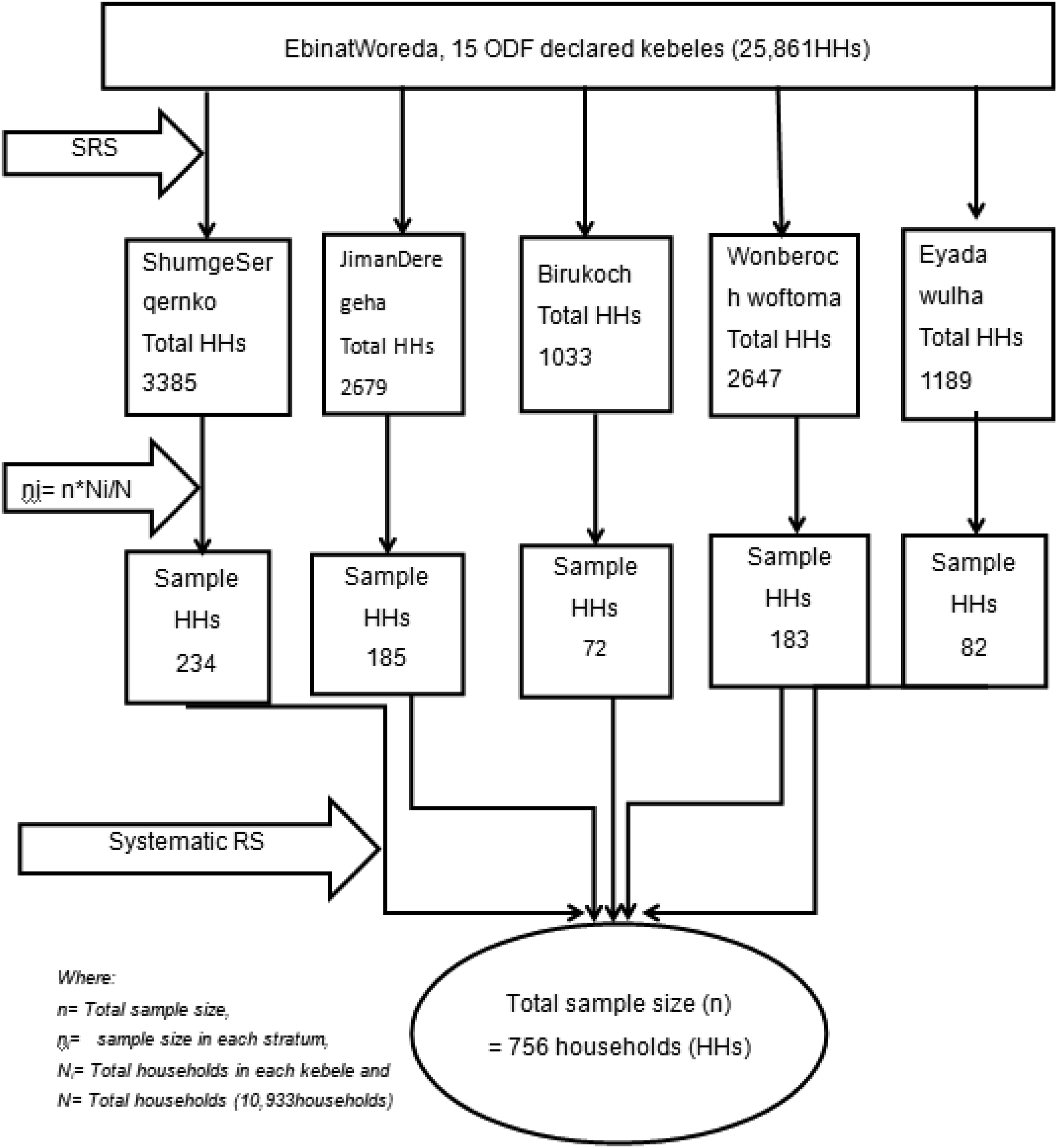
Study Variables
Dependent Variables: Sustainable Latrine Utilization
Independent Variables
Socio-demographic and economic factors: Sex, age, marital status, family size, household income, educational status, occupation, availability of school children, and presence of under five children.
Household and environmental factors: knowledge, availability of latrine construction materials, attributes of latrine construction materials, social norms, and sanction/enforcement.
Behavioral factors: privacy, security, convince, comfort, embarrassment, shame, and humiliation, motivating by follow-up visits, attitudes/beliefs, rewards or incentives, peer pressure/to be like others who utilize latrine.
Operational Definitions and Measurements
Sustainable latrine utilization: measured with 9 questions and the responses coded as 1 for yes and 0 for no. Households which score more than 75% of the questions with positive answer were taken as sustainable latrine utilization. 13
Good Sanitation behaviors: Sanitation behavioral actions include consistent latrine utilization by all family members, fix functional hand washing facility, operation and maintenance (cleaning slab/pit, repairing/re-building) of latrine.14,15Otherwise, poor Sanitation behaviors.
Functional latrine: is a latrine that provided services at the time of data collection even if the latrine required maintenance.
Good status of latrine: a pit latrine having durable and clean slab, superstructure, with a door and the possibility of maintaining privacy during utilization. Otherwise, poor latrine status. 16
Data Collection Tools and Procedures
The data were collected by structured and pre tested questionnaire and supplemented with observational checklists. The Questionnaire is adapted from previously published CLTSH questionnaires and WHO sanitation assessment tool.6,17,18 Then, the tool is initially translated in to local language (Amharic).The reliability of the Amharic version questionnaire was tested using Cronbach’s alpha (Cronbach’s alpha = 0.78). Ten data collectors and four supervisors were involved data collection process after 2days training. The closed houses were registered as non-response when the data collectors revisited the houses at least three times.
Before actual data collection, 5% questionnaires were pre-tested in neighbors’ Kebele, which has similar characteristics in study Kebeles. The findings and experiences from the pre-tested questionnaires were used to amend the final questionnaires.
Semi-structured questionnaire and interview guides were prepared to collect data through FGD and key informant interview techniques and all relevant information that affect the sustainable latrine utilizations. Interviews were conducted by principal investigator and supervisors who served as the moderator and facilitators of the interview. The qualitative data collection tool was comprised open ended questions, which supported with probing questions.
Data Quality Control
The questionnaires were first prepared in English and then translated into local language “Amharic” and back translated into English by different individuals to check consistency and conceptual equivalence. Data were assured by properly designedand pre-tested questionnaires. For data quality improvement, training was given to data collectors and supervisors and the data were collected with close supervision. Every day after data collection, questionnaires were reviewed and checked for completeness by supervisors and principal investigator. Necessary feedback has been offered to data collectors in the next morning. After data entry, data clearance and re-correction was done.
Data Management and Analysis
Data entry, coding and cleaning were done using Epi-Info version 7 and exported to SPSS version 20 for further analysis. Descriptive statistics was used to describe the characteristics of study population in relation to mean, median, standard deviation and frequencies. An association between dependent and independent variables were assessed and its strength was presented using odds ratio with 95% confidence intervals. Both bivariate and multivariable logistic regression model were used to assess the association between outcome and determinant factors. Variables significant in the bivariate analysis (p<0.2) were subsequently entered into a multivariable analysis model. Hosmore and Lemshow test was used for checking model fitness test.
Qualitative information was transcribed and translated into English and analyzed by using Open Code software and analyzed thematically. The data-analysis process was followed a sequence of interrelated steps, such as frequent reading, coding, displaying, reduction, and interpretation. Even during data display and reduction, it has been reviewed earlier steps to refine codes, reread texts, and revised some aspects of the analysis.
Results
Socio-Demographic Characteristics
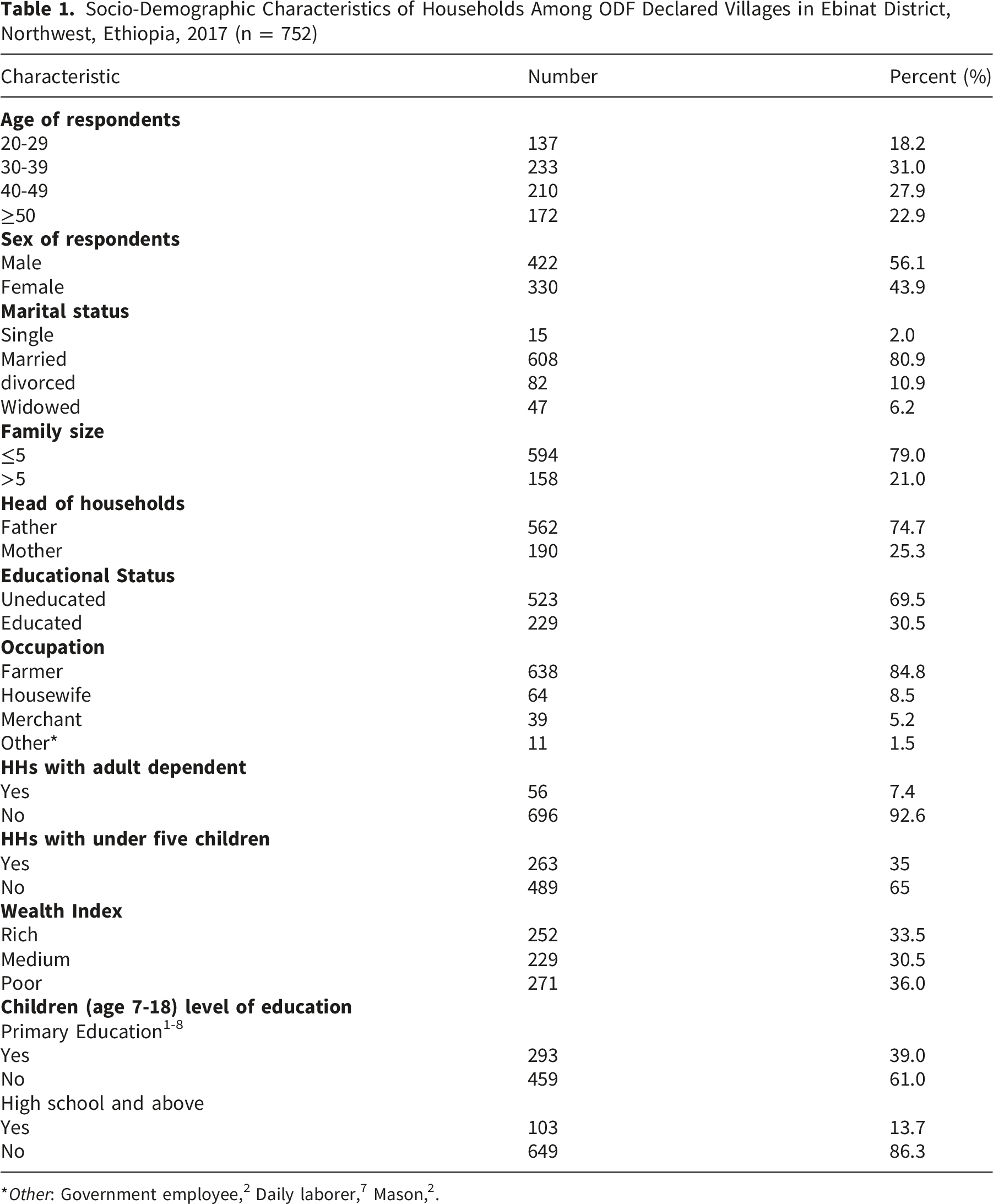
Socio-Demographic Characteristics of Households Among ODF Declared Villages in Ebinat District, Northwest, Ethiopia, 2017 (n = 752)
Latrine Coverage and Sanitation Behaviors
Of the 752 interviewed and observed households, 465 (61.8%) had functional latrines at the time of data collection, of which 461 (99.1%) were simple pit latrines. Among households with functional latrines, 95 (20.4%) shared their latrines with others. Some latrines, 41 (8.8%), were poorly functional due to damaged or absent superstructures. Latrines with wood slabs sealed by mud constituted 385 (82.8%), and 298 (64.1%) of functional latrines had walls that provided privacy. In addition, 341 (73.3%) and 165 (35.5%) latrines had roofs and doors, respectively. Observational findings indicated that 304 (65.4%) functional latrines required maintenance of the floor or superstructure.
Distribution of Latrine Utilization Among ODF Declared Villages in Ebinat District, Northwest Ethiopia, 2017

Sustainable Latrine Utilization
Distribution of Sustainable Latrine Utilization Among ODF Declared Kebeles in Ebinat District Northwest Ethiopia 2017. (n=752)

Analysis of Factors Associated With Sustainable Latrine Utilization
Both bivariate and multivariable analyses were conducted to assess factors associated with sustainable latrine utilization. Variables with a p-value < 0.2 in the bivariate analysis included: presence of children aged 7–18 years attending elementary school, children attending secondary school, household income, household visits by health extension workers (HEWs), household visits by health development armies (HDAs), family member participation in CLTSH triggering, distance of the latrine from the dwelling, and presence of children under five years of age. These variables were subsequently entered into a multivariable logistic regression model to identify independent factors associated with sustainable latrine utilization at the household level.
Facilitators of Sustainable Latrine Utilization
Bivariate and Multivariable Analysis of Factors Associated With Sustainable Latrine Utilization of Households Among ODF Declared Kebele in Ebinat District, Northwest Ethiopia, May 2017 (n =752)
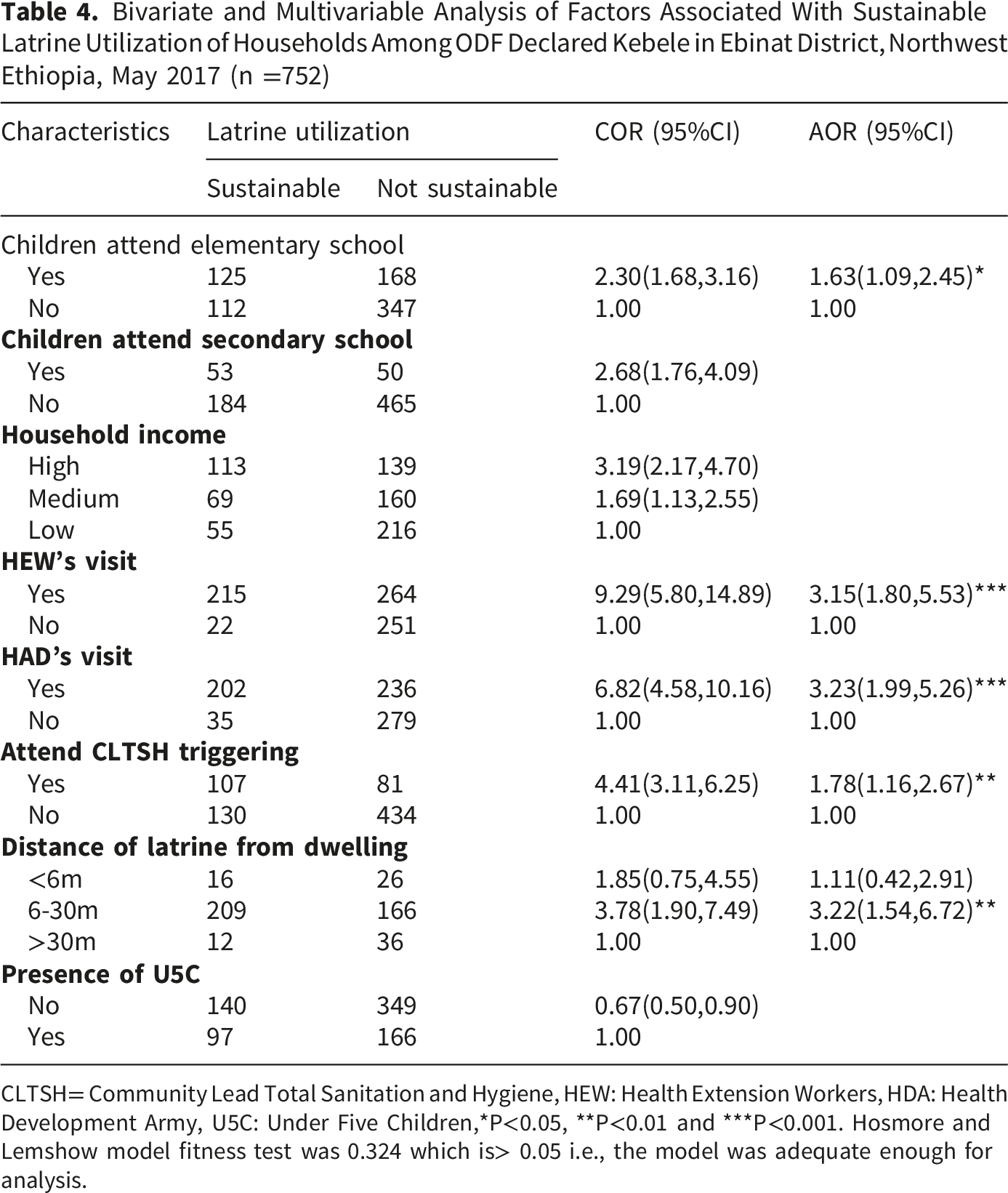
CLTSH= Community Lead Total Sanitation and Hygiene, HEW: Health Extension Workers, HDA: Health Development Army, U5C: Under Five Children,*P<0.05, **P<0.01 and ***P<0.001. Hosmore and Lemshow model fitness test was 0.324 which is> 0.05 i.e., the model was adequate enough for analysis.
Consistent with these findings, qualitative results indicated that support from HDAs, participation in CLTSH triggering, and accessibility of local construction materials (stone, wood, grass, and hand tools) facilitated sustainable latrine utilization.
Participants in FGDs and key informant interviews noted that locally available durable materials, such as olive and “Embiss” wood, which can resist termite damage, were important for latrine construction, maintenance, and rebuilding. They also emphasized the knowledge and skills gained through support from health professionals. A 46-year-old female FGD participant from Wonberoch Woftoma village stated: “….we have an indigenous knowledge of protecting termites damage of our latrine base by covering with plastic sheet the bottom of wood and we are now appreciating it.” In addition to this, the FGD participants also said on social support as when there are peoples, which don’t have a capacity to construct their own latrine volunteers in the village were facilitated by health development armies (HDAs) to construct their latrines.
Behavioral factors were also highlighted as facilitators. Male FGD participants from Wonberoch Woftoma village emphasized that their motivation stemmed from CLTSH triggering, which helped them understand the health risks of feces and the shame and disgust associated with open defecation, particularly when referred to using local offensive terms. Most participants reported that, since CLTSH triggering and ODF declaration, open defecation has been perceived as a bad and unacceptable practice. Some participants also noted that observing proper latrine use during visits to relatives in nearby towns motivated them to sustain latrine utilization.
Barriers for Sustainable Latrine Utilization
FGD and key informant interview participants identified several barriers to sustainable latrine utilization, including lack of awareness, traditional and moral beliefs, absence of integrated promotional activities, limited involvement of respected community members, inconsistent follow-up and support, and a tendency among kebele teams to treat ODF declaration as a symbolic achievement rather than a continuous process. Additional barriers included community frustration due to punitive measures (e.g., restriction of mosquito bed net access for households without latrines), lack of regular post-ODF review meetings at village, kebele, and woreda levels, and limited access to CLTSH implementation guidelines and ODF protocols.
One of the key informant interview participants of 25 year-old HEW stated: “…we we thought we have done awareness creation but still I suppose that the problem is lack of awareness, I think we are not giving it in the right way or we didn’t use the right strategy.” Similarly, a 32-year-old male key informant from the woreda health office explained: “…Currently, open defecations free (ODF) declared villages are going back to open defecations (OD). It is because of at the time of ODF declaration the kebele team was mobilizing the community by emphasizing their ceremony of ODF rather than the importance of latrine utilization. At the end of declaration ceremony, the communities are thought that they have finished their assignment and they follow the previous open defecation practice.”
A 53-year-old male FGD participant from an ODF kebele further stated: “…We received advice to create ODF village; there was a direction what commented us even women not to ashamed with using latrine even at a day time. In spite of that, ODF is stepping back and the situation is worsening right now. The entire area wherever we go there open defecation was become common. I can’t say that it is ODF area now. Unless it is strictly managed for future, we can gate the waste everywhere, every time and we will go to the worst conditions. The people have low awareness about the importance of latrine utilization”
Traditional and moral beliefs remained significant barriers. A 45-year-old female FGD participant from Wonberoch Woftoma noted: “…still some, there is a belief saying that in the past generations of our ancestors, our fathers were grown having open defecation in the field, what was brought to them? Why should we need to keep it as grain in the store?”
Moreover, participants from FGDs and KIIs in Birkoch kebele reported that latrine promotion was not conducted in an integrated manner and that respected community members were insufficiently involved. Although kebele leaders, religious leaders, and community figureheads occasionally advised households, many did not own or consistently use latrines themselves, thereby undermining their role as behavioral role models.
Discussion
This study aimed to assess sustainable latrine use and associated factors among ODF-declared villages in Ebinat district. Out of 752 households interviewed, nearly two-thirds (61.8%) had a functional latrine. However, only 31.5% of all households in ODF-declared kebeles had sustainable latrine utilization (95% CI: 28.2, 34.8).
The current finding was lower than the 36% reported in Ilu Babur Zone, Southwest Ethiopia. 19 It is also much lower than Ethiopia’s national ODF target set at 82% for 2015. 20 However, it is similar to the most recent JMP report from UNICEF and WHO for rural Ethiopia, with a documented 34% rate.8,21Additionally, this finding was lower than the 37.4% consistent latrine use observed in the Hawzein district, Tigray. 12 These differences may be due to varying program strategies. For example, in the study area, campaigns led by HEWs, HDAs, kebele CLTSH teams, and health professionals may not have fully followed protocols or provided complete behavioral change interventions. As a result, sustainability may be compromised compared to regions with structured follow-up and stricter adherence to ODF protocols.
The likelihood of sustainable latrine utilization was 1.63 times higher in households with primary school-aged children compared to those without. The findings of this study were supported by a systematic review and meta-analysis conducted in Ethiopia. 22 It is also consistent with the study conducted in Awabel district, Northwest Ethiopia, 23 and Dirashe district, Southern Ethiopia. 24 This might be due to the fact that students can share their experience with their family because students are exposed to health education about latrine utilization and hygiene information from school clubs, their teachers, and other health professionals.
Close supervision of households with HEWs is relevant to maintain sustainable utilization of latrine. Households that received a visit with HEWs were three times more likely to utilize latrine in sustainable way than households who did not visited by HEWs. This study supports the study finding at Bahir Dar zuria district. 16 This finding also aligns with the study done in the Kewot district of Ethiopia, 25 in Tigray, Ethiopia. 26 Similarly, households that received HDAs visit were 3.23 times more likely than those households that did not receive a visit from HDAs, which supports the finding in Tigray, Northern Ethiopia 27 and in Bangladesh. 28
This study also shows that sustainable latrine utilization among households who attend CLTSH triggering event were 4times more likely than those did not attending CLTSH triggering event. Similarly, the FGD and key informant interview findings indicates that CLTSH triggering event about how feces is disgust, how to use latrines, even facilitators support sustainable latrine utilization. This is consistent with the finding in Laelay Maichew district, North Ethiopia, 29 Diretiyara district, Eastern Ethiopia. 18 This is due to the fact that, CLTSH triggering event attendants have perceived elements of CLTSH approach (shame, disgust and fear of disease).
The study observed that households had a latrine with a distance of 6-30 meter were 3.22 times more likely to sustainably utilize latrine than households with 30 meter and more. This is consistent with the study done in Tigray, Northern Ethiopia. 27 This may be due to the distance was far to be easily accessed by adult dependents (disabled/elder/severely ill) and children less than five years old. This shows that inappropriate location of latrine facility setback sustainable latrine utilization in rural communities of ODF declared kebeles.
The limitation of this study is, even though we have tried to initiate participants to memorize HEWs and HDAs visit specifically on latrine utilization, recall bias was suspected on the purpose and time interval of the visit they received. Furthermore, this study shares the limitations of cross-sectional studies and hence it might suffer from temporal relationship establishment with some variables and might not provide much stronger evidence of causality.
Conclusions
Despite the implementation of the community-led total sanitation and hygiene (CLTSH) strategy and the declaration of open defecation-free (ODF) status, sustainable latrine utilization remains low in several kebeles of the Ebinat district. Factors influencing sustainable utilization include the presence of children aged 7 to 18 years attending elementary school, household visits by health extension workers and health development armies (HDAs), family members’ attendance at CLTSH triggering events, the distance of the latrine from the dwelling, and traditional or moral beliefs. Therefore, program implementers should prioritize behavioral change interventions, and health workers and HDAs should conduct frequent follow-ups after the ODF declaration.
Footnotes
Acknowledgement
We would like to thank the University of Gondar’s College of Medicine and Health Sciences for delivering an ethical clearance for this study. We would like to thank Debre Markos University for every support. We would also like to extend our heartfelt appreciation to the Ebinat district health office for giving us permission to conduct this study. We greatly acknowledge the study participants for their active participation.
Ethical Considerations
Ethical clearance was obtained from Ethical Review Committee (ERC) of Institute of Public Health, University of Gondar. An official letter for permission and support was written to Ebinat district health office and Kebele administrations. Written consent was obtained from study participants prior to commencement of the study. The purpose of the study was clearly explained to study participants and well informed they have a right to withdraw in the study. Permission was also obtained to use sound recorder. Confidentiality was maintained and assured by excluding their names from identification of the study participants. Therefore, the study agreed with the Helsinki Declaration of 1964 and its related amendments in this regard.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this article. The data that support the findings of this study are also available from the corresponding authors.