
Abstract
Childhood stunting is a global public health concern that affects millions of children worldwide. This study assessed the association between household latrine access type and childhood stunting in the Bolgatanga Municipality of Northern Ghana. A cross-sectional study was carried out in health facilities in the study area. Data collection consisted of mother-child pairs with children aged 0 to 59 months. The outcome variable was stunting, while the main exposure variable was household sanitation facility type and other covariates. Bivariable and Multivariable analyses were used to determine factors associated with stunting. Key findings of the study included, 40.5% having access to improved toilet facilities, 16.4% using unimproved facilities, and 43.1% practicing open defecation. Prevalence of stunting was 28.5% (95% CI: 23.9-33.1). Children from households practicing open defecation had more than twice the odds of being stunted compared to those with access to improved sanitation (adjusted odds ratio [AOR] = 2.26; 95% CI: 1.21-4.02). Male sex, low birth weight, and lower maternal education also emerged as significant risk factors. Our findings highlight the need for integrated public health strategies that address poor sanitation, promote maternal education, and support the nutritional needs of vulnerable children to reduce stunting in similar settings.
Introduction
Childhood stunting is a significant global public health challenge, affecting millions of children worldwide. 1 The World Health Organisation (WHO) describes stunting as a condition whereby a child’s height-for-age is more than 2 standard deviations below the WHO child growth standards median for children of the same age and sex who are well-nourished. 2 In 2020, globally, stunting affected about 149.2 million children under 5 (U5) years, with the burden disproportionately high in Africa, where prevalence rate reached nearly 30% above the global average of 22.3%.3,4 In Ghana, stunting is the most prevalent form of undernutrition among children U5, with rates ranging from 14.7% to 28.2% across different regions and a national average of 17%.5 -8 The Upper East Region (UER) of Ghana has consistently recorded higher prevalence rates of 21%, as compared to 10% and 11% in the Eastern and Greater Accra regions respectively. 8
Stunting reflects the prolonged consequences of persistent inadequate nutrition, especially during the initial 1000 days of life. It has been associated with both short- and long-term consequences on children, including impaired cognition, poor educational outcomes and quality of life, as well as mortality. 9
Among the key contributing factors is inadequate sanitation, which has been associated with stunting through diarrhoeal diseases, helminth infections, and environmental enteric dysfunction (EED). 10 These conditions impair nutrient absorption and growth, particularly in contexts where access to improved sanitation is limited. Beyond sanitation, multiple child-, maternal-, and household-level factors contribute to stunting, and these include child’s age, sex, birth weight, vaccination status, birth spacing, maternal education and nutritional status, antenatal care (ANC) utilisation, household wealth, family size, and structure.7,11,12
Globally, 60% of people in low-and middle-income countries (LMICs) lack access to safely improved sanitation services, with open defecation remaining prevalent in many settings thereby making the Sustainable Development Goal (SDG) targets of 6.1 and 6.2 which aims at ensuring availability and sustainable management of water and sanitation for all by 2030 a mirage. 13 In Ghana, initiatives such as the Community-Led Total Sanitation (CLTS) programme have sought to improve sanitation coverage. Nevertheless, progress has been uneven, particularly in rural and peri-urban areas. In the UER, it is estimated that about 18% of households still practice open defecation, and up to 95% lack access to basic sanitation services.8,14
Although the association between poor sanitation and child health is well recognised, there is limited empirical research specifically examining this relationship within northern Ghana and particularly the UER. Considering the region’s sanitation challenges and elevated stunting rates, environmental conditions likely contribute to child growth faltering. However, this link remains underexplored in the local context.
This study, therefore, investigates the association between household sanitation access and childhood stunting in the UER, with the aim of generating evidence to inform targeted, context-specific interventions to improve child nutrition and health outcomes.
Materials and Methods
Study Setting and Design
The study was conducted in the Bolgatanga Municipality, the regional capital of the Upper East Region. The municipality covers a land area of 729 sq. km and shares borders with the Bongo District to the North, South and East by Talensi, and Kassena-Nankana District to the West. It has an estimated total population of 130 890, with 26 179 (20%) being children aged 11 to 59 months, and 31 414 (24%) being women in their fertile age (WIFA).
The municipality has 2 types of erratic water supply systems–a rural system comprising rivers; dams; ponds and dugouts; precipitation; hand-dug wells; and other natural water sources which easily dry up during the dry season and an inconsistent urban water supply system by the Ghana water company limited comprising of a network of piped systems that supply water to mainly urban dwellers. Waste disposal is generally a challenge in the municipality, with only about 15% of the overall waste being properly collected and disposed of.
Administratively, the municipality is divided into 9 sub-municipalities by the health authorities and has a total of 47 health facilities. These include 1 regional hospital (secondary level), 1 hospital and 1 clinic (primary level), 6 health centres (sub-municipality level) and 38 community- based health planning and services compounds (CHPS; community level), all of which offer free postnatal care (PNC) services. 15
A cross-sectional design was employed, and the study was conducted in selected health facilities within the municipality.
Study Population, Sample Size, and Sampling Procedures
Our study population consisted of mothers and children under 5 who attended postnatal care sessions at selected health facilities in the Bolgatanga municipality. Post natal care attendance in the municipality is reported to be over 80%.
15
The sample size was calculated using Cochrane’s formula for determining proportions for a single population:
We used multiple sampling techniques to select health facilities and respondents. The regional hospital, which is the only secondary-level and referral facility, was chosen on purpose to represent the secondary level of care. The lottery method was used to select 1 primary level health facility and 9 CHPS compounds from each of the 9 sub-districts. All 6 sub-districts with health centres had their centres included. In the 3 sub-districts without a health centre, the highest-level CHPS compound was selected to ensure complete representation of all sub-districts and levels of healthcare delivery.
Using the previous year’s PNC attendance data from the District Health Information Management System 2 (DHIMS2), a proportion-to-population size approach was employed to allocate participants to each selected health facility. At each facility, participants were selected using simple random sampling via the lottery method, with slips labelled ‘YES’ or ‘NO’. Recruitment continued until the desired sample size was achieved. Informed consent was obtained from all participants.
Data Collection Procedures
Data were collected from 1st to 31st August 2023 using a semi-structured questionnaire administered electronically through face-to-face interviews. Trained research assistants conducted interviews using tablets, with the questionnaire programmed in Open Data Kit (ODK). The questionnaire consisted of questions related to child, maternal, and household socio-demographic characteristics. Information on household toilet facilities was also collected. Additionally, data, which included birth weight, birth order number, mother’s height, number of ANC visits, and mother’s weight before 12 weeks, were extracted from the maternal and child health record books. Maternal body mass index (BMI) was calculated by dividing the maternal weight in kilograms (kg) by the height in metres (m) squared (kg/m2).
Anthropometric measurements included height and mid-upper arm circumference (MUAC) of children, were collected. For children under 24 months, length was measured in a recumbent position using an infantometer. For those older than 24 months, height was measured standing using a stadiometer. All measurements were recorded to the nearest 0.1 cm. Child’s age was verified from health records and recorded in completed months.
Study Variables and Definitions
Outcome Variable
The outcome variable was stunting, analysed in binary form (1 = stunted, 0 = not stunted). Stunting was defined using height-for-age Z-scores (HAZ), calculated in ENA software. A child was classified as stunted if the HAZ was below −2 standard deviations (SD) from the median of the WHO reference population. 2
Description of Main Exposure Measures
The main exposure variable was household toilet facility type. This was categorised as ‘Improved’, ‘Unimproved’, and ‘Open defecation’. Improved facilities included: flush/pour-flush toilets to piped sewer systems, septic tanks and pit latrines; ventilated improved pit (VIP) latrines; pit latrines with slabs; and composting toilets. Unimproved facilities included: flush/pour-flush to elsewhere; pit latrine without a slab or open pit; bucket; hanging toilet on latrine. Other facilities, including households with no facility or use of bush/field, were considered open defecation. 13
Covariables
Considering the plethora of causes of child stunting in Ghana, covariables were grouped into 3 domains as child-, mother- and household-related covariables. Child-related covariables included age, sex, birth weight, and birth order. Mother-related covariables were age, education status, marital status, employment status, parity, number of ANC visits, and BMI. Household-related covariables included place of residence, gender of household head, education status of household head, employment status of household head, and household size. These factors have been shown to influence stunting in children U5 years from prior studies.7,12,16,17
Statistical Analysis
Data analysis was performed using Stata 17/IC (StataCorp LLC, Texas). Descriptive statistics were used to summarise the distribution of household sanitation facility types, child, maternal, and household characteristics, as well as child stunting. Categorical variables are presented as frequencies and percentages. Chi-square tests were used to determine whether there were statistically significant differences in the prevalence of stunting across categories of variables such as sanitation facility type, maternal education, household wealth, and other relevant covariables. Binary regression models were used to quantify the association between stunting and household toilet facility type, and covariables. Multivariable analysis examined the association between stunting and toilet facility type, while adjusting for all covariables such as child’s age, child’s sex, child’s birth weight child’s birth order, maternal age maternal level of education, maternal employment status, marital status of mother, maternal body mass index, number of ANC visits before delivery, parity, household head education level, household size, sex of household head, place of residence, household head employment status, household size, place of residence and sex of household head.
Multicollinearity was assessed using Variance Inflation Factors (VIF), and no indication of collinearity was detected before conducting the multivariable analysis. Results were reported as adjusted odds ratios (AOR) with 95% confidence intervals (CI), and statistical significance was set at P < .05.
Ethical Consideration
The study protocol was reviewed and approved by the Navrongo Health Research Centre Institutional Review Board
Results
Background Characteristics of the Studied Population
A total of 390 mother-child pairs (92.4% response rate) participated in this health facility-based survey. Maternal and child background characteristics are presented in Table 1. Most mothers (72.3%) were aged 20 to 34 years, with 83.1% currently married. Slightly more than half (54.9%) completed Junior or Senior High School, and 68.5% were employed. Around 70.8% had 2 or fewer children, and 69.5% had normal body weight. Approximately 74.4% had attended at least 8 ANC visits. Over half of the children (55.6%) were female, and 52.3% were within the age group of 12 to 23 months. The majority (90.8%) had birth weight greater than 2.5 kg, and 44.6% were first-order births.
Maternal and Child Background Characteristics (

Household Characteristics
Table 2 presents the household characteristics of the study population. Majority (62.1%) of respondents were from households located in the urban areas of the municipality with males dominating (87.7%) as the household heads. Most (83.1%) household heads were employed with 37.4% haven received junior or senior high school (JHS/SHS) education. Half (50.4%) of the households had 5 to 9 members. Prevalence of open defecation was found to be high at 43.1% whilst 40.5% used improved toilet facilities.
Household Characteristics of Studied Participants (N = 390).

Prevalence and Distribution of Childhood Stunting by Background Characteristics
Table 3 presents the prevalence and distribution of childhood stunting according to participants background characteristics. The overall prevalence of stunting was 28.5% (95% CI: 23.9-33.1). Stunting was significantly more prevalent among children from households with no access to sanitation facilities (practicing open defecation) as compared to those with access to improved sanitation facilities (36.3% vs 19.6%, P = .004). It was also significantly higher (34.1%, P = .027) among male children and those aged 24 to 35 months (46.2%, P = .010) compared to female children and other age groups respectively. Additionally, children born with a low birth weight had a higher prevalence of stunting than those with normal weight (52.8% vs 26.0%, P = .001). Stunting prevalence also varied significantly by birth order, with children of fourth birth order having the highest rate (40.0%). Furthermore, stunting was significantly higher in children with unemployed mothers compared to those with employed mothers (38.2% vs 24.0%, P = .004). Similarly, households with unemployed household heads had significantly higher prevalence of stunting compared to household heads who were employed (40.9% vs 25.9%, P = .014).
Prevalence and Distribution of Childhood Stunting by Child, Maternal, and Household Characteristics of the Studied Participants (N = 390).

Factors Associated With Childhood Stunting From Logistic Regression Analysis
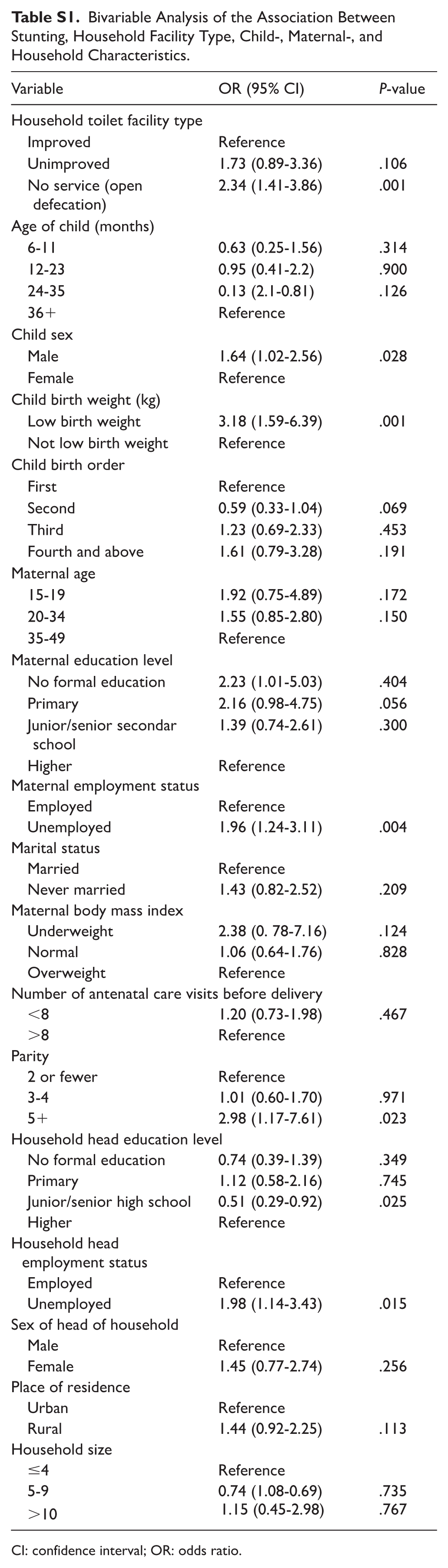
In bivariable regression analysis (Appendix S1, Additional File 2), household toilet facility type was significantly associated with stunting, with children from households practicing open defecation having higher odds of being stunted compared to those with improved sanitation facilities (OR = 2.26, 95% CI: 1.41-3.86, P = .001). Stunting was significantly associated withchild-related factors such as sex and birth weight; maternal factors including employment status and parity; and household characteristics such as the educational level and employment status of the household head.
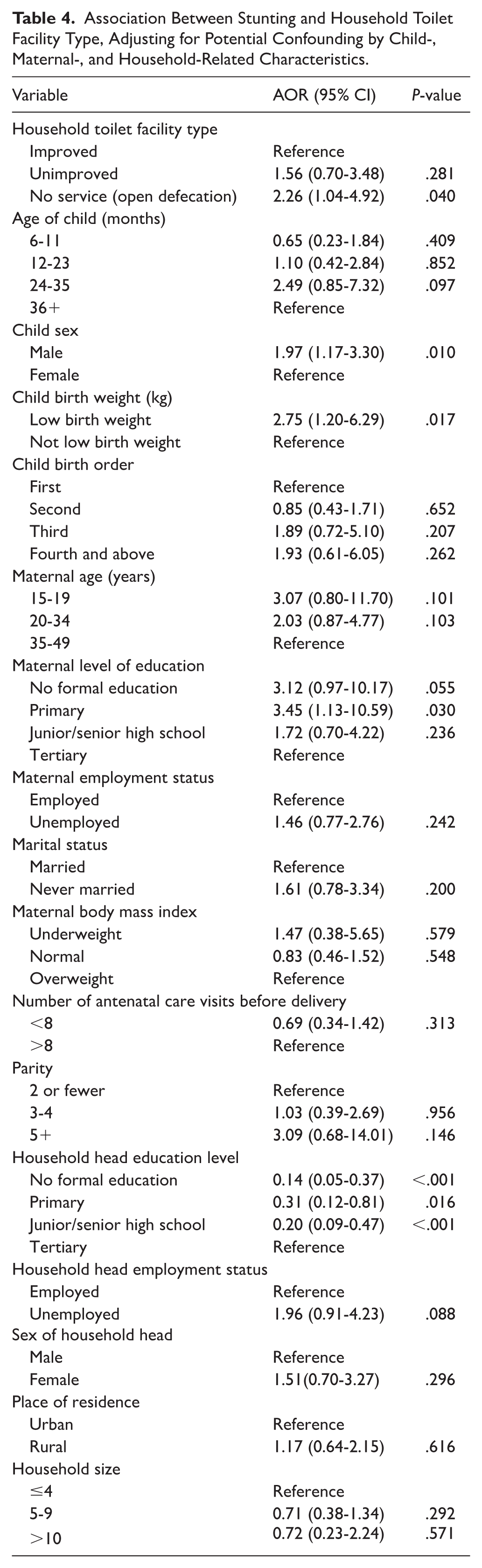
The results of the multivariable analysis are presented in Table 4. After adjusting for potential confounders, children living in households that practiced open defecation had more than twice the odds of being stunted compared to those in households with improved sanitation facilities (AOR = 2.26, 95% CI: 1.04-4.92, P = .040). Several other significant associations were identified among the covariables. Male children were significantly more likely to be stunted than females (AOR = 1.97, 95% CI: 1.17-3.30, P = .010). Children born with low birth weight had approximately 3 times the odds of being stunted compared to those who were not born with low birth weight (AOR = 2.75, 95% CI: 1.20-6.29, P = .017). Maternal education was also associated with stunting, with children whose mothers attained primary education having over 3 times the odds of being stunted than those whose mothers attained tertiary education (AOR = 3.45, 95% CI: 1.13-10.59, P = .030). Interestingly, the odds of stunting were significantly lower among children from households where the head had no formal education (AOR = 0.14, 95% CI: 0.05-0.37, P < .001), primary education (AOR = 0.31, 95% CI: 0.12-0.81, P = .016), or junior/senior high school education (AOR = 0.20, 95% CI: 0.09-0.47, P < .001) compared to children from households with heads who had tertiary education.
Association Between Stunting and Household Toilet Facility Type, Adjusting for Potential Confounding by Child-, Maternal-, and Household-Related Characteristics.
Discussion
This study investigated the association between stunting and household toilet facility type in the Bolgatanga Municipality of the Upper East Region of Ghana. The prevalence of stunting in our study was 28.5%, which is higher than what (21%) was previously reported in the studied area 8 and the global average of 22.3%. 4 Our finding was however lower than estimates from some African countries, such as Rwanda (37.7%), 11 Ethiopia (50.2%) 18 and Tanzania (31.6%). 19 The widespread occurrence of undernutrition observed in the study area points to a serious public health concern, with many children likely suffering from long-term nutritional deprivation. Such chronic deficiencies can hinder normal growth and development, leading to delayed cognitive function, poor academic achievement, and impaired physical growth. 20 These children are also more vulnerable to common childhood illnesses, particularly pneumonia and diarrhoea, as their bodies struggle to absorb essential nutrients and maintain a robust immune response. 21 Over time, the effects of early stunting may extend into adulthood, increasing the likelihood of developing chronic conditions such as hypertension, diabetes, dyslipidaemia and obesity. 22
Our study revealed that fewer than half of the respondents (40.5%) lived in households with access to improved toilet facilities with a notable proportion (43.1%) having no toilet facility at all, indicating widespread open defecation in the study population. In addition, we found a significant association between the type of toilet facility and child stunting. Children from households practicing open defecation had more than twice the odds of being stunted compared to those with improved sanitation facilities, and even after adjusting for potential confounders, underscoring the contribution of sanitation in childhood nutritional outcomes in the study setting. This finding aligns with evidence from multiple studies conducted in different contexts. In Benin for example, children from households lacking sanitation services had higher odds of stunting compared to those with basic sanitation. 23 Likewise, in Ethiopia, children exposed to open defecation were found to have 1.29 times greater odds of stunting than those from households with improved latrines. 24 However, not all studies have reported consistent significant findings of the association between stunting and sanitation, with others finding no significant associations at all.25,26 We believe that contextual or methodological differences may influence the observed associations.
Although the primary focus of this study was on the association between stunting and toilet facility type, several covariables also showed significant associations with childhood stunting, including sex of child (male), birth weight (low birth weight), maternal education level (low levels of education), and education level of head of household. These factors have been widely acknowledged by the literature from other LMICs,12,27 -29 and reflect biological and social mechanisms that contribute to childhood stunting. Male children are biologically more susceptible to early-life infections and tend to grow more rapidly than females, which increases their nutritional demands. 30 In resource-constrained settings, this heightened requirement may not be met, increasing their vulnerability to growth faltering Low birth weight sets the stage for stunting through impaired physical development, increased disease vulnerability, and inadequate nutritional support in early life, especially in low resource settings. 31 Maternal education influences child nutrition through multiple pathways, including health literacy, feeding practices, and healthcare utilisation.32,33 However, an unexpected result was that lower educational levels among household heads were associated with lower odds of stunting, contrary to existing literature. 34 This finding may reflect unmeasured confounders such as household wealth, caregiving roles, decision-making dynamics within households, or access to resources that were not fully captured in this study. Nevertheless, collectively, our findings reinforce the multifactorial nature of stunting and the need for integrated interventions addressing both environmental and socio-demographic determinants.
Strengths and Limitations
A key limitation of this study is its cross-sectional design, which limits the ability to draw causal inferences. Additionally, the data were not nationally representative, and the study was not community-based, which may restrict the generalisability of the findings beyond the study area. Furthermore, although health-facility attendance in the study area exceeds 80%, children who do not attend health facilities may differ systematically in nutritional status, introducing the possibility of selection bias associated with health-facility–based data collection. Another limitation lies in the reliance on self-reported data without observational verification, for example, the type of toilet facility used, which may be subject to reporting bias, especially given that participants were recruited from health facilities. Moreover, not all relevant exposure variables were included; in particular, socio-economic status (SES), a key determinant of undernutrition, was not adjusted for in the analysis. Another limitation of the study is that no morbidity data were collected for the children as child morbidity could affect nutritional growth outcomes. Despite these limitations, a major strength of the study is that anthropometric measurements were conducted by trained health personnel, and data missing from maternal and child health record books were cross-checked with facility registers, ensuring accuracy and completeness.
Conclusion
This study reveals a high burden of childhood stunting alongside widespread open defecation in the study area. In addition, there was a significant association between toilet facility type and childhood stunting, with children from households practicing open defecation being at increased risk. Our findings underscore the multifactorial nature of childhood undernutrition and emphasise the need for integrated interventions that improve household sanitation, promote maternal education, and support vulnerable infants, particularly those born with low birth weight.
Footnotes
Appendix
Bivariable Analysis of the Association Between Stunting, Household Facility Type, Child-, Maternal-, and Household Characteristics.
| Variable | OR (95% CI) | P-value |
|---|---|---|
| Household toilet facility type | ||
| Improved | Reference | |
| Unimproved | 1.73 (0.89-3.36) | .106 |
| No service (open defecation) | 2.34 (1.41-3.86) | .001 |
| Age of child (months) | ||
| 6-11 | 0.63 (0.25-1.56) | .314 |
| 12-23 | 0.95 (0.41-2.2) | .900 |
| 24-35 | 0.13 (2.1-0.81) | .126 |
| 36+ | Reference | |
| Child sex | ||
| Male | 1.64 (1.02-2.56) | .028 |
| Female | Reference | |
| Child birth weight (kg) | ||
| Low birth weight | 3.18 (1.59-6.39) | .001 |
| Not low birth weight | Reference | |
| Child birth order | ||
| First | Reference | |
| Second | 0.59 (0.33-1.04) | .069 |
| Third | 1.23 (0.69-2.33) | .453 |
| Fourth and above | 1.61 (0.79-3.28) | .191 |
| Maternal age | ||
| 15-19 | 1.92 (0.75-4.89) | .172 |
| 20-34 | 1.55 (0.85-2.80) | .150 |
| 35-49 | Reference | |
| Maternal education level | ||
| No formal education | 2.23 (1.01-5.03) | .404 |
| Primary | 2.16 (0.98-4.75) | .056 |
| Junior/senior secondar school | 1.39 (0.74-2.61) | .300 |
| Higher | Reference | |
| Maternal employment status | ||
| Employed | Reference | |
| Unemployed | 1.96 (1.24-3.11) | .004 |
| Marital status | ||
| Married | Reference | |
| Never married | 1.43 (0.82-2.52) | .209 |
| Maternal body mass index | ||
| Underweight | 2.38 (0. 78-7.16) | .124 |
| Normal | 1.06 (0.64-1.76) | .828 |
| Overweight | Reference | |
| Number of antenatal care visits before delivery | ||
| <8 | 1.20 (0.73-1.98) | .467 |
| >8 | Reference | |
| Parity | ||
| 2 or fewer | Reference | |
| 3-4 | 1.01 (0.60-1.70) | .971 |
| 5+ | 2.98 (1.17-7.61) | .023 |
| Household head education level | ||
| No formal education | 0.74 (0.39-1.39) | .349 |
| Primary | 1.12 (0.58-2.16) | .745 |
| Junior/senior high school | 0.51 (0.29-0.92) | .025 |
| Higher | Reference | |
| Household head employment status | ||
| Employed | Reference | |
| Unemployed | 1.98 (1.14-3.43) | .015 |
| Sex of head of household | ||
| Male | Reference | |
| Female | 1.45 (0.77-2.74) | .256 |
| Place of residence | ||
| Urban | Reference | |
| Rural | 1.44 (0.92-2.25) | .113 |
| Household size | ||
| ≤4 | Reference | |
| 5-9 | 0.74 (1.08-0.69) | .735 |
| >10 | 1.15 (0.45-2.98) | .767 |
CI: confidence interval; OR: odds ratio.
Acknowledgements
The authors acknowledge the immense support they got from the Upper East Regional Health Directorate, the Bolgatanga Metropolitan Health Directorate and the heads of all selected health facilities. Our profound gratitude goes to all the staff of the various postnatal clinics of selected health facilities.
Abbreviations
AOR: Adjusted Odds Ratio; ANC: Antenatal Care; BMI: Body Mass Index; CHPS: CWC: Child Welfare Clinic; Community-based Health Planning and Services; 95% CI: 95% Confidence Intervals; DHIMS2: District Health Information Management System 2; GSS: Ghana statistical service; HAZ: Height-for-Age Z-score; JMP: Joint Monitoring Programme; MICS: Multiple Indicator Cluster Survey; OR: unadjusted Odds Ratio; ODK: Open Data Kit; PNC: Post Natal Care; SES: Socioeconomic status; SSA: Sub-Saharan Africa; SDGs: Sustainable Development Goals; UNICEF: United Nations Children’s Fund; WASH: Water, Sanitation and Hygiene; UER: Upper East Region; WIFA: Women In their Fertility Age; WHO: World Health Organisation.
Author Contributions
JBKD conceived, designed, analyzed the data and drafted the initial manuscript. DC drafted the initial and final manuscripts. MB designed, drafted the initial and final manuscripts. SA designed, analyzed the data, and drafted the initial and final manuscripts. All authors read and approved the manuscript for submission for consideration for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data and information based on which conclusions are made can be found within the manuscript. The raw de-identified data may be made available upon reasonable request from the corresponding author.