
Abstract
Background:
Open defecation (OD) is the act of disposing human feces in open spaces and is a known risk factor for transmission of pathogens through environmental pollution, hence causing fecal oral diseases. Approximately 419 million people globally are practicing OD and 5.6 million people in Kenya. The study investigated the influence of socioeconomic factors on open defecation and fecal oral diseases.
Methods:
Stratified random sampling was used to select 204 participants from 8 administrative units (strata). Quantitative data was collected using a standardized semi-structured questionnaire and qualitative data through conducting Key Informants Interviews and Focus Group Discussions.
Results:
53% and 30% of respondents attributed OD to lack of education on WASH and low monthly income respectively. Pearson Chi-square tests showed a significant association between family size and OD (P < .05) and a strong association between occupation, monthly income and education (P < .001). Endemic fecal oral diseases include amoebiasis, diarrhea and typhoid with an occurrence of 64%, 35%, and 1% respectively. Diarrhea had a prevalence of 222 per 10 000 persons, amoebiasis at 399 per 10 000 persons and typhoid at 5 per 10 000 persons. These results are consistent with those from related studies that link OD to prevalence of fecal-oral diseases.
Conclusion and Recommendations:
Socioeconomic factors influence practice of OD which in turn increases the prevalence of fecal oral diseases. In order to end OD, public health stakeholders should intensify health education and promotion on the negative health impacts of OD and also employ Community Led Total Sanitation interventions.
Introduction
Open defecation refers to the disposal of human feces in open spaces such as fields, open bodies of water, forests, beaches, or with solid waste. 1 In the year 2022, 419 million people were reported practicing OD. Rural areas accounted for 9 out of 10 people practicing open defecation. 2 Only 30% of Kenya’s population can access basic sanitation systems at home 3 and OD is practiced by approximately 7.4% of the population, largely in rural areas. 4
Studies have shown that, peoples’ sanitary preferences influence their defecation practices 5 cultural practices, resources, availability of materials, and habits, 6 and different social and environmental factors. 7 Household head’s level of education has an influence on open defecation whereby households whose household heads are educated have a higher likelihood of owning a sanitary facility as compared to those whose heads are less or not educated. This is because households whose heads are educated can understand health effects of open defecation and the importance of owning a toilet facility in their households.8,9 A higher education level translates to a higher monthly income of a household, meaning that they are in a better position to construct a sanitary facility and may even opt for a better technology. In a study carried out in India, participants who were illiterate had poor knowledge about sanitary latrines while, those who were literate had a better attitude toward latrine utilization. 10
Some studies have also shown that OD is influenced by household size whereby, a household with a smaller family size is less likely to practice open defecation than a household with a larger size. 11 Household heads with a large family size may not have financial capability to construct a toilet at home because they are overwhelmed by the responsibility of providing for the basic needs of all members. Despite the fact that they may know the health and environmental benefits of latrine ownership and are willing to construct one, they may not be able to do so. Such households where the family size is large will decide to defecate in the open. 8
A study carried out in Ghana showed that there exists a relationship between occupation and OD. O’Reilly et al reported that wealthier farming villages in Uttarakhand, India, which could afford to construct latrines, practiced OD because it was more convenient than going back home to defecate. 12 Similarly, a study carried out in Haiti showed that much time was spent by agricultural households’ members outdoors away from home, hence they considered building a toilet was not important since it could not be used. 13 One’s occupation also influences one’s source of income; hence, when a household head has a higher monthly income level, there is a lesser likelihood of his/her household members practicing open defecation. 8
Monthly income levels in a household also influence OD. Among the poorest households, the most common form of sanitation is open defecation. 14 A report by WHO/UNICEF JMP showed that there exist inequalities in Kenya when it comes to open defecation, where 0% is reported in the richest household compared to 47% amongst the poor households. 1 Appiah-Effah et al observed in rural Ghana that women in the poorest quintile were more inclined to practice OD than women in the richest quintile. 15
OD perpetuates a vicious cycle of disease; hence, countries with high levels of open defecation have the highest number of under-5 deaths as well as the highest levels of malnutrition due to diarrheal diseases. 16 Diarrhea is among the main leading causes of under-five deaths, and Sub-Saharan Africa records the highest under-five mortality rate globally, whereby in every 1000 live births, there are 74 deaths. 17 According to WHO, poor sanitation accounts for 10% of the global disease burden of diarrheal diseases, and those countries which have higher proportions of people practicing open defecation report higher under-five mortality and malnutrition rates. 1 Fecal-oral transmitted diseases are caused by exposure, through ingestion, of disease-causing microorganisms that are present in human or animal excreta. These diseases are a major cause of illness especially in sub-Saharan Africa, and lack of adequate sanitation, safe water, and awareness contributes to the prevalence of these diseases. 18 Mara observed that most water-related disease outbreaks like trachoma, cholera, and typhoid have been highly associated with poor sanitation practices such as OD. 19 The negative impacts on the environment and human beings show that open defecation should be eradicated.
Various studies on OD in Kenya have been conducted in Arid and Semi-arid Lands (ASAL).20 -22 In Kericho County, which is not ASAL, limited research has been done linking OD, socioeconomic factors, and prevalence of fecal-oral diseases. This background formed the basis upon which this article on assessment of the impact of OD and socioeconomic factors on prevalence of endemic fecal-oral diseases in Soin Ward was carried out.
Methods
Study Area
The research was conducted in Soin Ward, Sigowet/Soin Constituency, Kericho County. Soin ward lies between latitude of 0° 25′12.47″S and longitude of 35° 17′45.16″ E. The rationale for selecting Soin Ward is because a report done by the KNBS and SID showed that Kericho County was among 9 counties where the gap difference between the best and worst performing wards is over 80% in access to improved sanitation, and Soin ward was ranked as the worst in the report. 23
Research Design
A cross-sectional study design was utilized for the selected households in the study area, as the data gathered from household heads or their designated representatives was intended to be generalized to the entire population of Soin Ward.
Target Population
Quantitative study target population comprised households within the study area. Interviews were conducted with adult household heads or their appointed representatives above the age of 18 who provided accurate and reliable information. Further, qualitative information was obtained through key informant interviews and 10 Focused Group Discussions.
Sampling Technique and Sample Size
Proportionate sampling technique was employed to select the number of households that were interviewed from 8 sub-locations. Simple random sampling was used to select households from each stratum. Sample size was done as guided by Kothari formula for finite population 24 and a size of 204 was obtained.
Data Collection Tools
A semi-structured questionnaire was utilized to collect primary data from households essential to achieving the study’s objectives. A Focus Group Discussion (FGD) and Key Informant Interview (KII) schedule were used to collect qualitative data. A template was developed using WHO household sanitary survey guidelines to collect data from Ministry of Health registered health facilities on endemic fecal oral diseases in the study area.
Data Analysis
Descriptive data was analyzed using frequencies and percentages. Data on socioeconomic characteristics associated to OD practice was analyzed using Pearson Chi-Square tests, and quantitative data was illustrated using tables and charts. Statistical significance was assessed using P-values ⩽ .05. Data obtained from Focus Group Discussions (FGDs) and Key Informant Interviews (KIIs) were coded based on keywords or key concepts using in vivo techniques and analyzed to identify recurring themes.
Ethical Considerations
As part of ethical and data protection considerations, clearance was obtained from the Research and Ethics Committee of Egerton University, and research permit from National Council of Science, Technology, and Innovation (NACOSTI/P/23/28163) was secured before commencement of the study. Further approvals were sought from the local authorities including the County Public Health Department before commencement of data collection.
Results and Discussion
Socio-Demographic Characteristics of the Respondents
In this paper, 204 respondents were contacted, and all agreed to take part, achieving a 100% response rate. The largest proportion of the respondents was farmers (52%) and those employed accounted for 16.7%. Additionally, female accounted for 67.2% of the respondents while 32.8% were male. A total of 110 (53.9%) respondents’ level of education was primary school, whereas those who attained tertiary colleges and university were 8.8% and 6.9% respectively. It was also noted that 72% of the respondents earned KES 10 000 and below monthly and 8.3% earned above KES 50 000 a month.
Relationship Between Open Defecation and Socio-Economic Factors and Fecal Oral Diseases
The relationship between OD, socioeconomic factors and fecal oral diseases was determined using Pearson’s Chi-square tests. Table 1 indicates that no significant association existed between OD and gender (P = .660), between OD and age (P = .707), a significant association between OD and household’s family size (P = .018), between OD and fecal oral diseases, and a strong association between OD and occupation (P = .000), average monthly income (P = .000) and household’s head level of education (P = .000).
Pearson Chi-Square Test of Association Between OD and Socioeconomic Factors and Fecal Oral Diseases.

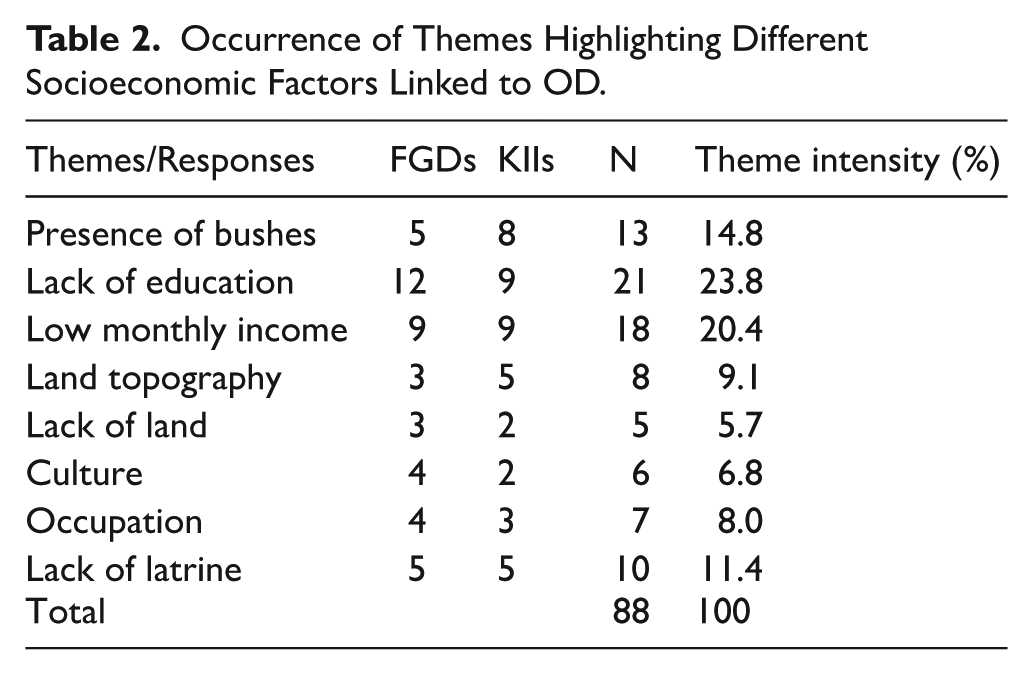
Data obtained from the FGDs and KII guides was analyzed using in vivo and descriptive coding for common themes on the socioeconomic factors influencing the practice of OD. As illustrated in Table 2, the 2 major themes identified by the respondents on the socioeconomic factors influencing OD include; lack of education and low monthly income at 23.8% and 20.4% respectively.
Occurrence of Themes Highlighting Different Socioeconomic Factors Linked to OD.
Kipsitet sub-location accounted for 38% cases of the reported fecal oral diseases while Kapchebwai and Kejiriet sub-locations accounted for the lowest reported cases at 2% and 1% respectively (Figure 1).
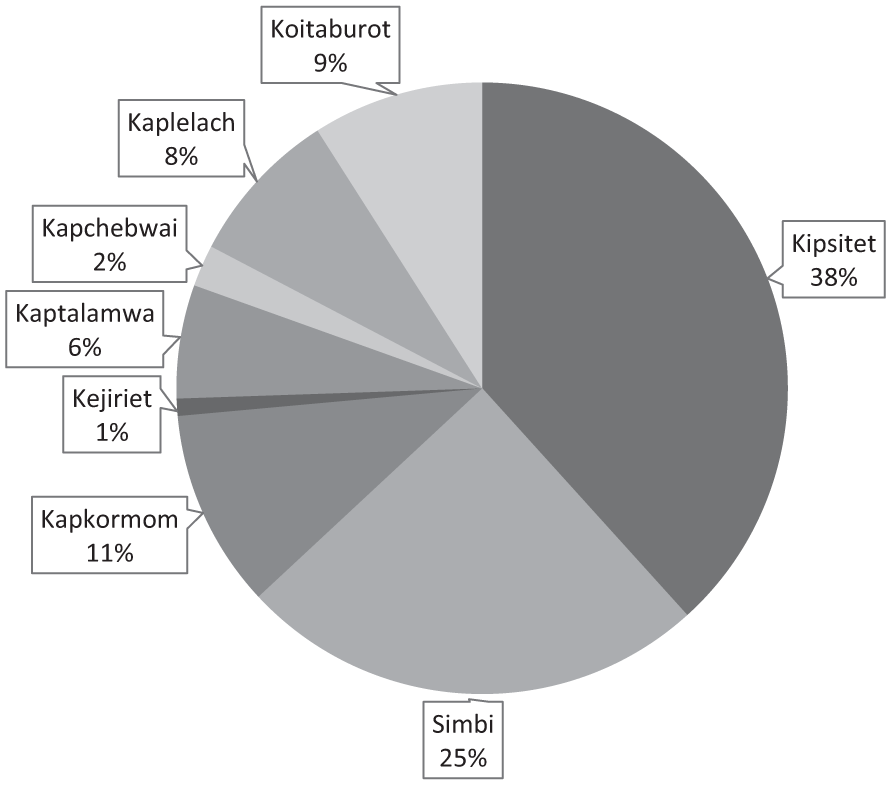
Hospital data showing spatial distribution of fecal oral diseases.
Results from the study showed that amoebiasis was the most prevalent fecal oral disease and was common among individuals aged between 25 and 59 years. Additionally, diarrhea was particularly common amongst children under the age of 5, accounting for 83.5% of all diarrheal reported cases (Table 3).
Distribution of Fecal Oral Diseases Across Different Age Cohorts in Soin Ward.

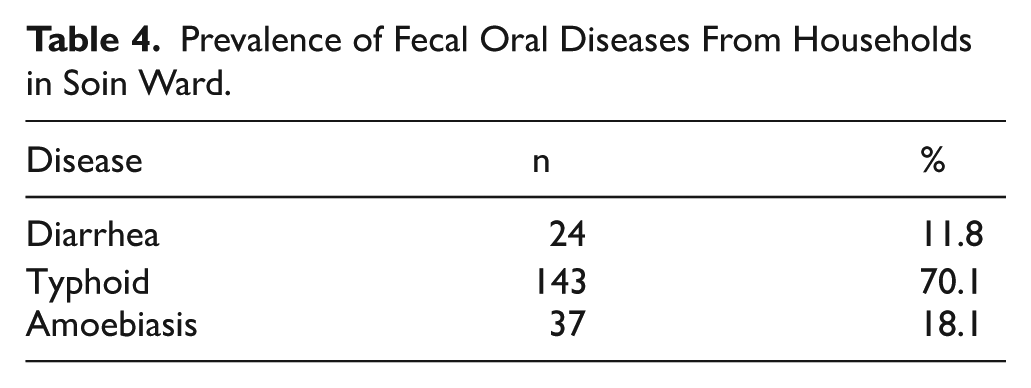
Table 4 shows that data obtained on fecal oral diseases from the household level indicated that the most prevalent fecal oral disease reported at was typhoid (70.1%), followed by amoebiasis (18.1%) and diarrhea (11.8%).
Prevalence of Fecal Oral Diseases From Households in Soin Ward.
Socio-Economic Factors Influencing Open Defecation and Associated Endemic Fecal Oral Diseases
In this article, age and gender, which were some of the selected socio-economic determinants, did not statistically have any significance in influencing OD. Similar studies done in Ghana on OD gave similar results. 26
Education is essential in order for people to recognize the significance and necessity of environmental sanitation. Lack of education was a factor deemed to contribute to open defection in qualitative data findings with a theme intensity of 13.6%. Poor level of schooling or lack of education implies limited understanding of disease transmission through the fecal oral route. Therefore, such households will not view the open defecation as a bad practice and a behavior detrimental to their health 15 . Households with educated heads owned latrines since they comprehend the impacts of open defecation and the significance of owning and using a latrine. Similar studies carried out on factors influencing open defecation show that household with low level of education have a higher likelihood of practicing open defecation.8,22,27
Households with a higher monthly income are less likely to practice open defecation because they can afford to build a latrine. They have the financial capability to build a toilet facility, even utilizing improved technology. 28 In Soin ward households whose average monthly income was 50 000 shillings and above had 100% latrine coverage compared to households with a monthly average income of less than 5000 shillings which had 57% practicing open defecation. Busienei et al also established that in Lodwar, latrine coverage was minimal in low-income households compared to those with higher incomes. 22 Families with limited financial resources tend to prioritize sanitation less.29,30 In rural Ghana, it was noted that women in the poorest income group were more likely to engage in open defecation compared to women in the wealthiest income group. 15
Occupation also contributes significantly to open defecation. Findings from the study indicated that 89% of casual laborers earned less than 10 000 shillings per month, this limits their ability to build a latrine, consequently, practicing open defecation. Farmers, casual laborers and bodaboda operators in the FGDs asserted that when they go to work, they cannot go back to their homes to access the latrines because they are far and might consume most of their time hence, they defecate anywhere they find some privacy. O’Reilly et al reported that wealthier farming villages in Uttarakhand, India, which were in a position to build latrines, practiced OD because it was more convenient than going back home to defecate. 12 A study in Haiti showed that much time was spent by agricultural households’ members outdoors away from home hence considered building a toilet was not important since it could not be used. 13 A similar study in Uganda showed that villagers go to farmlands in the morning and return in the evening hence resorting to open defecation because of absence of sanitary facilities in the farming and grazing areas. 31 When one is employed, it means they have a constant, reliable source of income and can budget their earnings to accommodate provision of a sanitary facility.
Another key predictor of open defecation was household size. Among households with over 10 members, 60% practiced OD, compared to 33.8% of families with fewer than 5 members. These results align with a study carried out in Ethiopia, which reported that households with more than 5 members were highly likely to engage in OD than those with 5 or fewer members. 11 Smaller families may experience an improved standard of living, encouraging better latrine usage. In contrast, larger households might face challenges like waiting times, leading to missed opportunities to use toilet facilities. 32 Overcrowding, particularly in the mornings, may compel members of large families to defecate in the open. 33 Household heads with a large family size claimed that owning a latrine was not a priority investment because the cost of constructing one was high and they focused on providing food, shelter and clothing first. Therefore, although they may know the health and environmental benefits of having a sanitary facility in their households, their willingness to build one will decrease thus opting to defecate in the open.
Prevalence of Fecal Oral Diseases The health hazards related to infectious diseases that are linked to human feces and the danger of exposure to these organisms can cause serious health concerns such as viral infections, diarrhea, typhoid, and cholera, also rises as a result of open defecation. 34 Diarrhea is a leading cause of death in children under the age of 5 17 and a major cause of mortality and morbidity in children in many developing countries. A study done on the global burden of disease showed that Kenya is still among the top 5 sub-Saharan countries with the highest number of disability-adjusted life-years (DALYs), equivalent to 794 310. 35
The study recorded a higher percentage of diarrheal cases from children under the age of 5 compared to persons above 5 years of age. This can be explained by the fact that, as children start crawling and teething they are predisposed to frequent diarrheal infections as they wander into unhygienic environments. 36 Whereas majority of caregivers practice unsafe disposal of children’s feces since it is believed to be free of contaminants, unsafe disposal of children’s feces poses significant threats of childhood diarrhea. The young children can come in contact with the contaminated environments making them susceptible to diarrhea pathogens. A study on Disease burden and risk factors of diarrhea in children under 5 years across Kenya showed that contaminated environments mean children are more susceptible to frequent bouts of diarrhea owing to their weak immune status. 37
While amoebiasis occurs worldwide, it is largely an infection of impoverished communities, particularly when sanitation is poor. 38 In areas where there is inadequate access of sanitation infrastructure and open defecation is practiced like Soin, amoebiasis is a public health problem. Amoebiasis is caused by Entamoebiasis histolytica which is the second leading cause of parasitic diseases globally. 39 Although there was equal exposure to men and women to the pathogen Entamoebiasis hystolytica, the study shows that more women are reported to have contracted amoebiasis as compared to their male counterparts. A similar study done in Uttarakhand hills in India on prevalence of parasitic infection also observed that the infection was more prevalent in female population than men. 40 This might be explained by the health seeking behavior of women compared to men.
From the study, typhoid cases are low. This observation is corroborated by prior research done on the Global Typhoid Fever Incidence whereby Africa recorded low typhoid cases and was attributed to lower typhoid incidence. 41 Kenya is among the 44 countries and freely associated states with high or very high incidence of typhoid fever, according to Global Burden of Disease 2019 estimates and was among the countries that have introduced typhoid conjugate vaccines into their routine immunization schedule as a preventive measure amongst children. Although the number of typhoid cases recorded in health facility registers was low, a higher number of cases were reported at the household level. This discrepancy may be due to the fact that data were collected only from 2 Ministry of Health (MoH)-registered facilities, while many individuals may have sought treatment at other facilities not registered with the MoH. Another possible explanation is that unregistered clinics often use the Widal test for typhoid diagnosis, which the MoH phased out in 2017 due to its low diagnostic accuracy. 42 In contrast, MoH-registered facilities use the Enzyme-Linked Immunosorbent Assay (ELISA) test, which provides higher diagnostic accuracy. 43
Conclusion and Recommendations
In this study, there exists an association between socioeconomic factors, open defecation and prevalence of fecal oral diseases. Lower educational levels and monthly income of the household head increase the likelihood of practicing OD. Households with employed heads are more likely to own sanitary facilities because they can afford the construction cost compared to those headed by casual laborers who have meager income. Additionally, larger family sizes are associated with a higher tendency to practice OD due to challenges like waiting times may compel members to defecate in the open. OD in turn contributes to the prevalence of the endemic fecal oral diseases through ingestion of contaminated water and food. Food is contaminated by flies which bring fecal pathogens from the feces disposed in the open to the food while water surfaces are contaminated when fecal matter is carried by storm water to the rivers.
Public health officers together with the community health assistants and community health promoters should employ Community Led Total Sanitation (CLTS) interventions to accelerate end of OD practice. Additionally, health education should target at raising awareness on the health and environmental effects of OD.
Limitations of the Study
The study focused on the influence of the influence of socioeconomic factors on open defecation and fecal oral diseases. There are other factors like environmental factors, water handling techniques and household hygiene that can influence fecal oral diseases. This limitations highlights the need for further studies on other factors that contribute to prevalence of fecal oral diseases.
Footnotes
Author Contributions
KC, GMO, and DOO collaboratively conceptualized and designed the study. KC carried out data collection with supervision by GMO, and DOO. All authors contributed to data interpretation, manuscript drafting, and critical revisions. The final manuscript was developed collaboratively, with all authors approving the submitted version.
Consent to Participate
Prior to participation, all respondents provided informed consent after being briefed on the study’s objectives.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in the study are available upon request from the corresponding author.