
Abstract
Exposure to polycyclic aromatic hydrocarbons (PAHs) is a major threat to public health and economic stability, particularly in Sub-Saharan African countries such as Ghana. However, limited consolidated evidence exists on the extent of exposure, associated health outcomes, and economic impacts. This systematic review aimed to summarize available studies on health effects of PAH exposure in Ghana and assess potential economic implications. A comprehensive search of PubMed, Scopus, Google Scholar, and African Journals Online was conducted for studies published between January 2014 and January 2025. Sixteen studies met the eligibility criteria. Considerable heterogeneity was observed regarding study designs, target populations, matrices assessed, and PAH analytes measured. Most studies were ecological, limiting comparability and economic estimation. Nonetheless, findings indicate significant exposure to PAHs through environmental (soil, street dust, particulate matter) and occupational (fish smoking, urban living) sources. Urinary PAH metabolite levels among exposed groups were substantially elevated, and over 70% of studies reported carcinogenic risk indices exceeding WHO and USEPA thresholds of 1 × 10⁻⁶. Health effects such as persistent cough, chronic headaches, tachycardia, and dyspnea were reported. Although no Ghanaian study directly evaluated the economic burden, the evidence suggests increased healthcare costs, productivity losses, and environmental remediation expenses. This review identifies critical gaps, including the need for personal exposure measurements, longitudinal health assessments, and economic evaluations. Addressing these gaps is essential for informed policy development and resource allocation to reduce the health and economic impacts of PAH pollution in Ghana.
Keywords
Introduction
Polycyclic aromatic hydrocarbons (PAHs) are a group of chemically stable and environmentally persistent organic compounds generated largely through the incomplete combustion of organic matter, including fossil fuels, biomass, and waste materials.1 -3 Because of their lipophilic nature and environmental persistence, PAHs accumulate in various environmental media such as air, water, soil, and food chains. 4 Human exposure occurs through inhalation of polluted air, ingestion of contaminated food and water, and dermal contact with PAH-contaminated surfaces, particularly in occupational and residential settings. 5
Globally, PAHs are of serious public health concern due to their toxic, mutagenic, and carcinogenic properties. The International Agency for Research on Cancer (IARC) classifies several PAHs, most notably benzo[a]pyrene, as Group 1 carcinogens. 6 Chronic exposure is associated with a range of non-communicable diseases, including lung and bladder cancers, respiratory illnesses, and cardiovascular complications.7 -10 Consequently, PAHs are also recognized for their potential economic burden, contributing to healthcare expenditures, reduced workforce productivity, and the need for costly environmental remediation.
In Ghana, some studies have investigated environmental levels of PAHs in specific media such as air, soil, food (particularly smoked and singed meat), and water, often in urban centers, industrial zones, and abattoirs.3 -5,7,8 These investigations have identified high contamination levels, attributing sources to biomass burning, vehicular emissions, industrial activities, and the use of scrap tires in animal carcass processing. However, these studies have largely remained compartmentalized, focusing on individual exposure routes or media without linking findings to measurable public health outcomes or assessing the wider socio-economic burden.
To date, no comprehensive synthesis exists that integrates multi-pathway environmental exposures, associated health outcomes, and their potential economic implications in Ghana. Moreover, existing reviews, both locally and in other low- and middle-income countries, tend to focus either on environmental contamination or on health effects in isolation, rarely examining the intersection of exposure science, epidemiology, and economic burden in a single framework. This review is therefore novel in its approach to holistically assess PAH exposure in Ghana across multiple environmental media, and to relate these exposures to both public health impacts and the potential financial burden on individuals and the national economy.
By drawing on a decade of research, this work contributes the first integrative review of its kind for Ghana, offering an evidence base that is not only essential for domestic policy and public health programing but also serves as a model for environmental health assessments in similar contexts globally. The findings are particularly relevant to low- and middle-income countries experiencing rapid urbanization and industrialization without parallel investments in environmental monitoring and public health infrastructure.
Methods
Study Search Strategy and Selection
A systematic literature review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The review aimed to synthesize evidence on the public health impacts and economic burden of PAH exposure in Ghana, drawing from peer-reviewed studies published between January 2014 and January 2025.
The search was limited to studies from January 2014 onward to capture a decade marked by advancements in industrial practices, public health systems, and environmental monitoring in Ghana. Earlier studies were few and lacked robust methods or comprehensive health data, making the post-2014 period more suitable for drawing relevant and reliable conclusions.
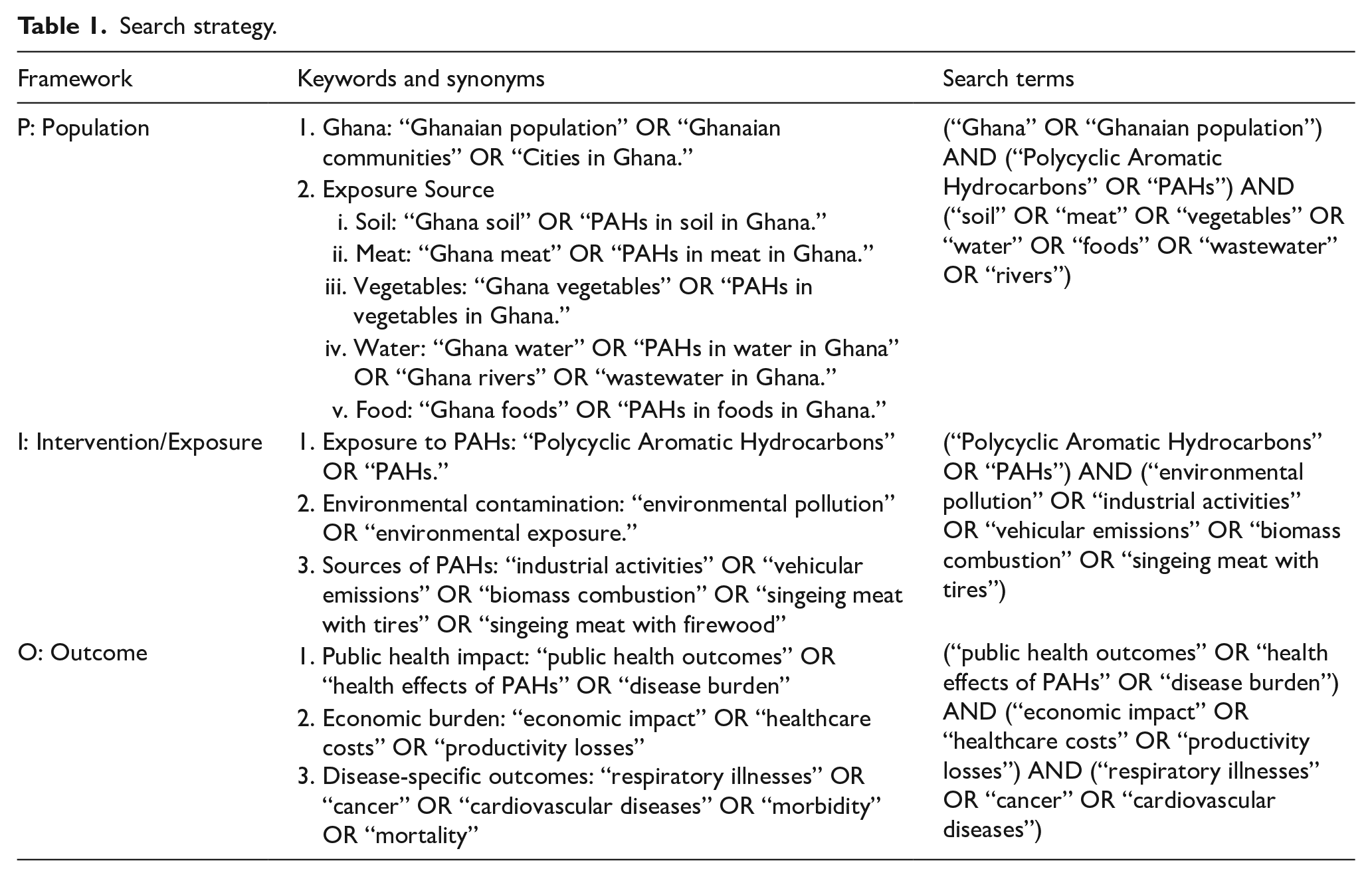
Searches were independently carried out using PubMed, SCOPUS, Google Scholar, and African Journals Online (AJOL), to ensure comprehensive coverage of both international and African-centered literature. The PICO (Population, Intervention/Exposure, Comparison, and Outcomes) framework guided the construction of the search terms and was also used to steer data extraction (summarized in Table 1). To enhance the completeness of the literature base, the reference lists of all included articles were manually screened for additional relevant studies. The review considered only peer-reviewed articles written in English.
Search strategy.
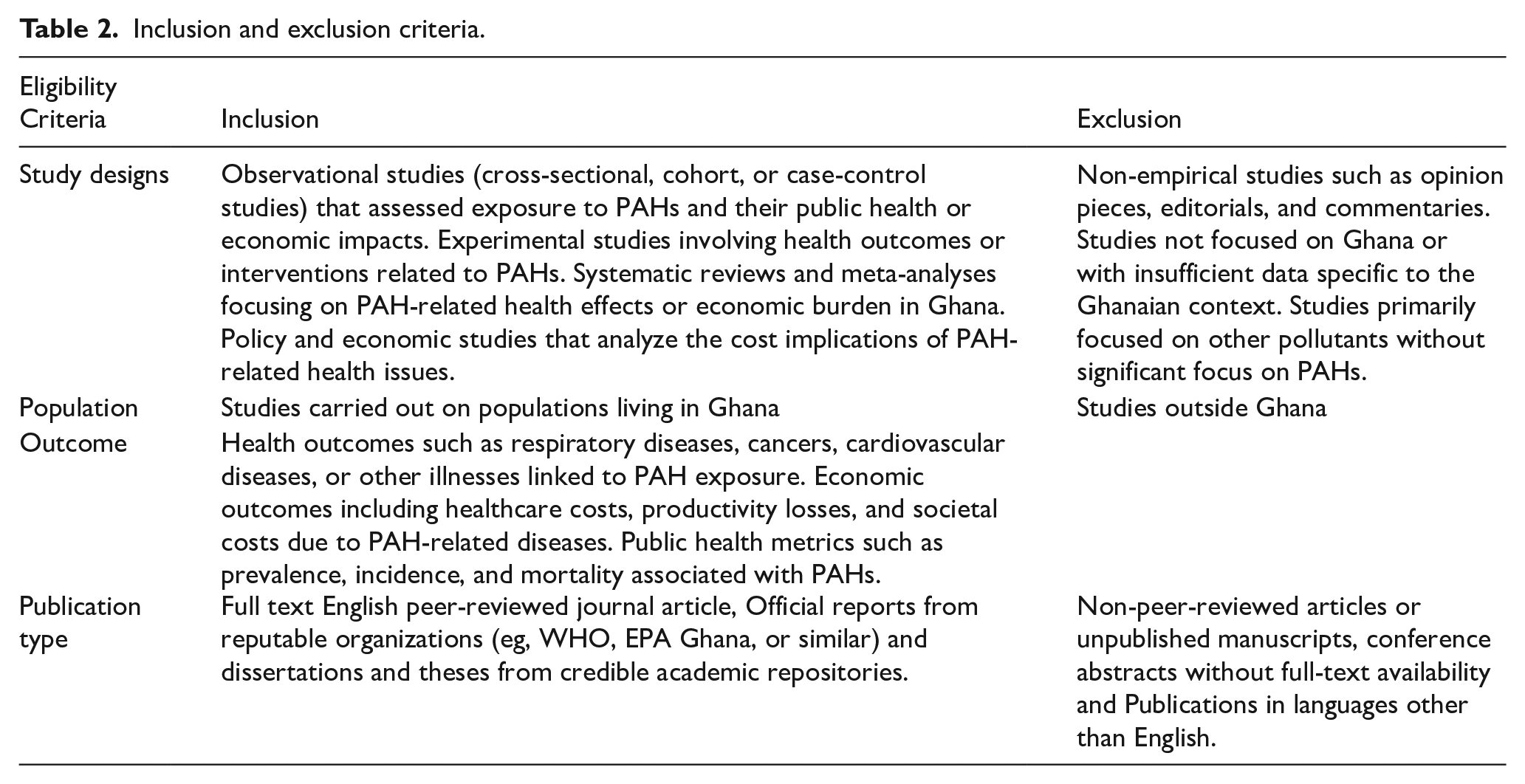
From an initial pool of 142 articles, duplicates were removed and predefined eligibility criteria were applied, resulting in a final selection of 16 studies that were included for synthesis. The full screening and selection process is illustrated in the PRISMA flow diagram (Figure 1), and the summary of the inclusion and exclusion criteria is shown in Table 2.
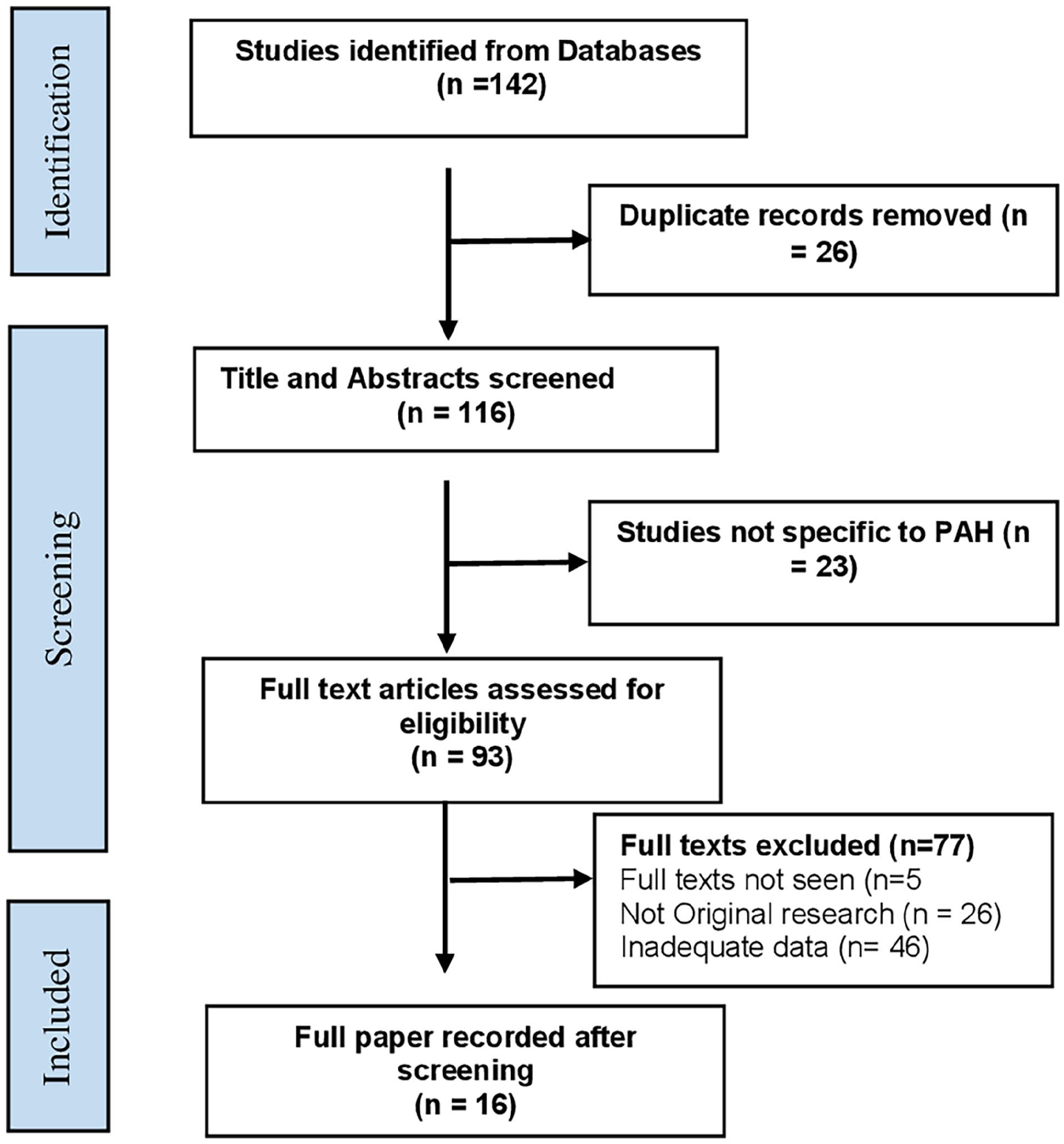
PRISMA flow diagram of study search and selection process.
Inclusion and exclusion criteria.
Public health outcomes were linked specifically to PAH exposure in Ghana to provide a focused, context-specific analysis that reflects the country’s unique environmental practices, regulatory landscape, and health data availability—thereby offering evidence tailored to inform national policy, while also serving as a case study for similarly structured low- and middle-income settings. This study provides a comprehensive analysis of PAH exposure, health outcomes, and economic impacts in Ghana, offering a model for other low- and middle-income countries facing similar environmental health challenges. Its findings contribute to global discussions on environmental contamination, public health, and economic burden, providing valuable insights for policy makers and researchers worldwide.
Data Extraction
Extracted data were categorized into
Data Analysis
Descriptive synthesis was used to summarize study characteristics and identify associations between PAH exposure and health outcomes across Ghana. Narrative synthesis integrated findings on public health and economic impacts, such as healthcare costs and productivity losses.
Results
General Study Characteristics
This systematic review synthesized data from studies conducted across various regions in Ghana, examining the public health impacts of PAH exposure. Characteristics of the included studies are shown in Table 3.
Health effects of polycyclic aromatic hydrocarbon exposure in Ghana.
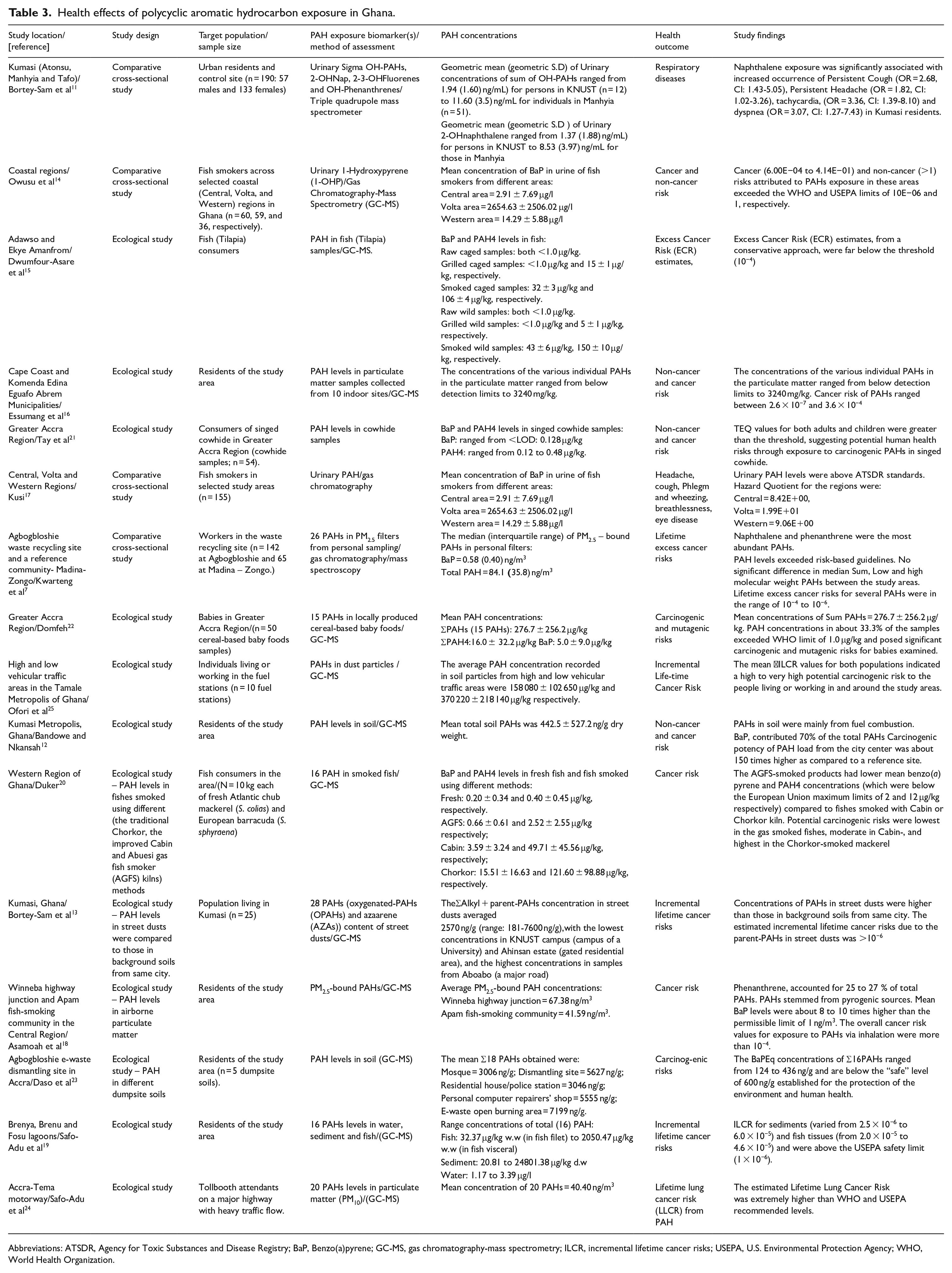
Abbreviations: ATSDR, Agency for Toxic Substances and Disease Registry; BaP, Benzo(a)pyrene; GC-MS, gas chromatography-mass spectrometry; ILCR, incremental lifetime cancer risks; USEPA, U.S. Environmental Protection Agency; WHO, World Health Organization.
The studies spanned major regions in Ghana, including Ashanti,11 -13 Central,14 -20 Volta,17,18 Western, 17 Greater Accra (including Agbogbloshie),7,18,21 -24 and Northern, 25 highlighting widespread PAH contamination across diverse urban, coastal, and industrial settings.
Twelve of the 16 reviewed studies had ecological study design. These studies measured PAH levels in environmental samples including fish,15,18 particulate matter,7,17,19,23 cowhide, 21 locally produced cereal-based baby foods, 22 street dusts,12,24 soil,11,23 water, and sediment. 20 Four studies had comparative cross-sectional design. These studies measured PAH levels in urine samples collected from fish smokers,14,17 urban residents 13 as well as personal PM2.5 filters of workers in a waste recycling site. 7
Diverse population groups were targeted in the studies. These included residents of urban areas,11 -13 e-waste dismantling areas,7,23 coastal areas, and lagoons,14,18 -20 fish smokers,14,17 and fish smoking communities,14,17 -20 e-waste workers,7,23 children, 19 fuel station workers, 25 and tollbooth attendants on major highway. 24
Urban residents may be exposed to PAHs via inhalation of polluted air,11 -13 while fish smokers,14,15,17,18,20 fuel station, e-waste workers, and tollbooth attendants7,23 -25 may face occupational exposure through inhalation of PAH laden air. Children, particularly those consuming locally produced cereal-based foods may be at risk of dietary exposure to PAH. 22
Sources of PAH Exposure in Ghana
The reported sources of environmental exposure to PAH included consumption of fresh and smoked fish,15,19,20 singed cowhide, 21 and cereal-based baby foods 22 ; inhalation of indoor/ambient particulate matter16,19; as well as contact with urban soil/dust,11 -13,23,25 water. 20 Occupational exposures to PAH were reported in 5 studies. These included fish smoking,14,17 working in waste recycling site, 7 fuel stations, 25 and in major highway tollbooths. 24
Health Effects of PAH Exposure in Ghana
Most of the studies measured PAH in environmental samples and conducted a cancer risk assessment of PAH exposure in this population. Different cancer risk indices including overall cancer risk,12,14,16,18,20 -23 excess cancer risk, 15 lifetime excess cancer risk, 7 lifetime lung cancer risk, 24 incremental lifetime cancer risks,13,19,25 mutagenic risk 22 were used to determine the likelihood of developing cancers following exposure to PAH through the different environmental media studied in this population. The reported estimates of cancer risk in most of the studies exceeded the USEPA/WHO acceptable thresholds of 10−6.7,12 -14,16,18,19,21,24,25
Asamoah et al 18 investigated PAH concentrations in fishes smoked using different methods (the traditional Chorkor, the improved Cabin and Abuesi gas fish smoker (AGFS) kilns). Their reports show that AGFS-smoked fishes had lower mean benzo(a) pyrene and PAH4 concentrations (which were below the European Union maximum limits of 2 and 12 μg/kg respectively) compared to those smoked with Cabin or Chorkor kiln and that potential carcinogenic risks were lowest in the gas smoked fishes, moderate in Cabin-, and highest in the Chorkor-smoked mackerel. 18
In the report by Domfeh, 22 PAH concentrations exceeded WHO limit of 1.0 μg/kg in about 33.3% of locally produced cereals food samples, with mean concentrations of Sum PAHs of 276.7 ± 256.2 μg/kg. The estimated carcinogenic and mutagenic risks for babies exposed to PAH through contaminated cereal foods exceeded the acceptable thresholds. 22
Reported cancer risk estimates in 2 of the studies15,23 were however, within acceptable thresholds: Dwumfour-Asare et al 15 assessed PAHs levels in O. niloticus (Nile tilapia) sampled from an aquaculture cage and a wild catch. Their reports indicated that fresh fish samples from an aquaculture cage had higher PAH levels than those from a wild catch. The study also reported that fish smoking significantly increased the levels of carcinogenic PAH such as Benzo [a] pyrene and PAH4 (Benzo [a] anthracene, Chrysene, Benzo [b] fluoranthene, and Benzo [a] pyrene. However, the reported Excess Cancer Risk estimates, were below the acceptable threshold. 15 In another study, the reported BaPeq concentrations of Σ16 PAHs in soil samples collected form Agbogbloshie e-waste dismantling site in Accra, ranged from 124 to 436 ng/g, which are below the “safe” level of 600 ng/g established for the protection of the environment and human health. 23
Other health outcomes associated with PAH exposure were respiratory illnesses such as persistent cough, headache, and dyspnea, which were common among urban residents 13 and fish smokers. 17
Economic Effects of PAH Exposure in Ghana
Direct and Indirect Healthcare Costs Due to PAH-Associated Diseases
Estimation of healthcare costs due to PAH exposure and associated illness could not be done due to lack of data on the Population attributable fraction (PAF), which is a measure widely used to assess the public health impact of exposures in populations. 26 The population attributable fraction is defined as the fraction of all cases of a particular disease or adverse condition in a population that is attributable to a specific exposure. To estimate the PAF of the increase in healthcare costs attributable to PAH, data on the relative risks of developing these diseases due to PAH exposure is needed. In the absence of these data as well as studies directly evaluating the cost of illnesses attributable to PAH, reports from some cost of PAH-related illnesses across Ghana was used to help shed some light on the economic burden of PAH exposure in this population. Table 4 shows the economic burden of PAHs exposure in Ghana.
Economic burden of PAH exposure in Ghana.

The reviewed studies highlight a substantial, though variably quantified, economic burden associated with exposure to PAHs in Ghana. Healthcare expenditures due to PAH-related illnesses, particularly non-communicable diseases such as cancers, cardiovascular conditions, and respiratory diseases, were considered.
A retrospective study at Komfo Anokye Teaching Hospital 27 involving 1975 patients found that the median cost of cardiovascular disease (CVD) treatment was USD 195.29, with stroke-related admissions costing USD 211.19. Stroke was the most prevalent condition, with a case fatality rate of 28.9%. The same study reported a median hospital stay of 5 days.
Using a cost-of-illness framework, the lifetime cost of managing hypertension, an outcome linked to chronic PAH exposure, was estimated at GHS 869 106 (USD 119,056), with the cost of treating related complications such as myocardial infarction (GHS 14,971.46), chronic kidney disease (GHS 23,431.20), and heart failure (GHS 6947.67) contributing significantly to the overall financial burden. 28
In the neonatal population, a prospective study at the Korle Bu Teaching Hospital Neonatal Intensive Care Unit in 2017 estimated an annual expenditure of USD 2.48 million for managing conditions such as bloodstream infections and low birth weight, both of which have been associated with prenatal PAH exposure. The cost per neonate with bloodstream infection was USD 749 compared to USD 494 for those without infection. 29
The economic burden of neurodegenerative diseases potentially linked to long-term PAH exposure is also projected to rise. Estimates for Alzheimer’s disease suggest a national cost of USD 525.4 million by 2030, increasing to USD 3.13 billion by 2050. 30 A separate analysis showed the total cost of dementia in Ghana rising from USD 16.2 billion in 2010 to USD 44.3 billion in 2019, comprising USD 4.8 billion in direct medical costs, USD 5.8 billion in direct social sector costs, and USD 33.6 billion in informal care costs. 31
Lost Hours and Productivity Due to PAH Exposure Effect
Managing complications from PAH-caused morbidities incurs significant costs and necessitates prolonged absences from work for both the patients and sometimes the family caregivers. These health conditions often result in substantial absenteeism, as affected individuals require time away from work for treatment and recovery. Family members who assume care giving roles also miss work, compounding the lost hours. The impact of these lost hours extends beyond individual workplaces, contributing to reduced productivity at the national level. Fisher et al 33 reported that in 2019, diseases linked to air pollution, including those caused by PAHs, resulted in productivity losses amounting to USD 1.63 billion, equivalent to 0.95% of Ghana’s GDP. The reported lost economic output due to air-pollution-related deaths in Ghana, in 2019 was USD 1379 (941–1959) million while lost economic output due to years lost due to disability attributable to air pollution in Ghana was USD 249 (183–325) million. 33 The study also reported that air pollution was responsible for an estimated loss of 43.7 million PIQ points in Ghana. 33
Remediation and Regulatory Costs
No studies reported quantified costs for the environmental remediation of PAH-contaminated sites in Ghana. Ghana lacks published data on the cost of PAH remediation due to several challenges, including the absence of a national inventory of contaminated sites, limited technical capacity and funding, and weak enforcement of environmental regulations. Additionally, PAH contamination is deprioritized in favor of more visible environmental issues, and public awareness remains low. Addressing this gap requires identifying contamination hot spots, conducting baseline assessments, estimating remediation costs, and fostering collaboration among government, academia, and international partners.
Discussion
Main Findings
This systematic review aimed to summarize available evidence on the public health effects of PAH exposure in Ghana. The results suggest that the population living in Ghana could be exposed to PAH through diverse environmental sources including ambient air, street dusts, soil, and consumption of smoked fish, cowhide and local cereal-based baby foods. Occupational sources of PAH exposure in this population included fish smoking, working in waste recycling sites, fuel station, and as tollbooth attendant. The studies reported high concentrations of PAH in different environmental media, suggesting that this population may be exposed to significant levels of PAH. The cancer and non-cancer risk estimates suggest that PAH exposure may contribute significantly to the burden of cancer and other diseases in this area. However, most of the included studies are ecological in design and did not measure PAH exposure in humans, limiting our conclusions on the associations between PAH exposure and human health in this population.
Sources of Exposure to PAH in Ghana
The geographical location investigated in the studies included urban, coastal, and industrial regions, highlighting the widespread nature of PAH contamination. The studies also reported both environmental and occupational exposures to PAH, reflecting diverse exposure sources. As reported in the studies,7,14,18,20,21 1 major source of PAH exposure in Ghana, as seen in other African nations, 34 is the use of smoke from biomass fuel for food processing, and preservation. Both individuals occupationally involved in food smoking, consumers of smoked food products as well as those living in close proximity to food-smoking environment are all at high risk of PAH exposure. People living in urban areas,11 -13 coastal areas,14,16,19 highways,24,25 e-waste dismantling areas7,23 are also at risk of exposure to PAH. Similar urban-industrial exposure patterns have been reported in Portugal, 35 Italy, 36 and Argentina, 37 where residents near industrial sites exhibited elevated PAH exposure through ambient air pollution. Similarly, cities with rapid industrialization and vehicular emissions have been identified as hotspots for PAH contamination.38,39 While studies in Ghana have linked PAH exposure to artisanal activities like fish smoking and cowhide singeing, studies from Europe and Asia predominantly link PAH exposure to vehicular emissions and large-scale industrial activities. This divergence underscores the need for region-specific interventions to address PAH exposure.
Concentrations of PAHs in Different Environmental Matrices
PAH in Food
The concentrations of PAH in potential food samples such as fish,15,18,20 singed cowhide, 21 and locally produced cereal-based baby foods 22 were investigated in different studies. Studies on PAH concentration in smoked fish and cowhide revealed that smoking is a significant source of carcinogenic PAHs such as BaP and PAH4 in smoked fish15,18 and cowhide 21 in this area. Typically, BaP and PAH4 levels in smoked fish samples exceeded the European Commission maximum permissible limits of 2 and 12 μg/kg, respectively.15,18 The study by Asamoah et al 18 further revealed that fish smoking using an improved gas method (Abuesi gas fish smoker), which ensure minimal exposure of the smoked fish products as well as the processors to smoke and heat, may significantly reduce the levels of carcinogenic PAHs in smoked fish. 18
Cereals and cereal based products have been reported as main source of human dietary exposure to PAHs.40,41 This has been attributed to high quantity of these products consumed per individual. 41 In Ghana, as well as other African population, cereal-based foods are staple foods. 22 PAH contamination of cereal-based foods such as bread may be caused by both contamination of raw materials, primarily (flour), as well as the baking process. 41 The reported average BaP concentration of 5.0 ± 9.0 μg/kg in locally produced cereal-based baby foods greatly exceeded the maximum permissible limits of 1 μg/kg set by the European commission. 22 Overall, these studies suggest that consumption of PAH contaminated food may be an important source of PAH exposure among Ghanaian population. These reports are corroborated by other studies of PAH levels in food.42,43 More studies are needed to identify other dietary sources of PAH exposure in Ghana.
PAH in Soil
The mean concentrations of PAH in soil samples investigated in different studies differed according to sites of sample collection. For example, mean concentrations of PAH in soil samples collected from residential areas12,13 were below the allowable levels of 1.0 mg/kg set by the Agency for Toxic Substances and Disease Registry and significantly lower than those collected from major roads and traffic areas, which were above the allowable levels.13,25 In another study, 23 the ΣAlkyl + parent-PAH levels in soil samples collected from around mosques (3006 ng/g) and residential areas (3046 ng/g), although higher than the permissible levels, were significantly lower than those collected from dismantling site (5627 ng/g), personal computer repairers’ shop (5555 ng/g), and e-waste open burning area (7199 ng/g). Comparing PAH levels in soil particle collected around fuel stations in high and low vehicular traffic areas, Ofori et al 3 reported significantly higher PAH levels in soil samples from high vehicular traffic areas than those in low traffic areas. These reports suggest that vehicular emissions (petrogenic) and burning of e-wastes (pyrogenic) may be major sources of PAH contamination in soil in this area. This observation is in line with several previous reports from other countries44 -46 and underscores the need for tight regulation of these emissions in this area.
Particulate Matter-bound PAH Levels
Particulate matter is an important source of PAH contamination in any environment. Indoor air pollution through the use of biomass fuel (wood, dung or charcoal) for cooking, heating and lighting purposes is a serious source of pollution, mostly in Sub-Saharan African countries including Ghana 47 and a major environmental source of PAH exposure in this population. The contribution of this to PAH exposure in Ghana has not received adequate research attention, as only 1 of the reviewed studies investigated PAH levels in particulate matter samples collected from 10 indoor sites. 16 Another important source of particulate matter bound PAH include vehicular emission and smoke processing of certain foods such as fish, meat. The reported levels of Particulate matter-bound PAH levels in the reviewed studies19,24 were higher than the permissible limit of 0.2 mg/m3 set by OSHA for work place exposure and signifies a health risk for workers and residents in these areas.
Health Effects of PAH Exposure
The reported health effects of PAH exposure in this population include cancer and respiratory diseases. However, of the 16 studies reviewed, 13 examined PAH levels in environmental matrices and this was used to estimate cancer and non-cancer risks in the population. Only 3 studies13,14,17 measured PAH biomarkers in body fluid, (urine), limiting our conclusions on the causal associations between PAH exposure and reported human health effects in this population.
Several individual PAHs have been grouped as either carcinogens, probable carcinogens or possible carcinogens to humans.6,46 Epidemiological studies in other populations have linked exposure to PAH with some cancers including lung, breast, skin, bladder cancer48 -50 as well as some childhood cancers including brain tumors, 51 leukemia, 52 nephroblastoma. 53 Several mechanisms for PAH-induced carcinogenesis have been proposed. Polycyclic aromatic hydrocarbons are lipophilic in nature, and therefore able to diffuse across the plasma membrane of cells. The metabolism of most PAHs involve 3 major enzymatic pathways, each involving different enzymes. One of these major pathways is the CYP1A1/CYP1B1 and epoxide hydrolase pathway, which has been implicated in DNA adduct formation. For example, Benzo (a) Pyrene is metabolized and activated by cytochrome P450 enzymes (CYP1A1/1B1), to form reactive metabolites such as Bap-7,8-epoxide, which is further metabolized by epoxide-hydrolase to form 7, 8-diol, and by CYP1A1/CYP1B1 to form 7, 8-diol-9, 10-epoxide (BPDE), the ultimate carcinogenic metabolite of BaP responsible for genotoxic effects. 54 BPDE is capable of reacting with DNA at the N 2 -position of guanine to produce BPDE-N 2 -Dg adduct.55,56 BPDE also induces oxidative stress, inflammation,57,58 which are all critical in carcinogenesis, and tumor progression.
Lung cancer was ranked as the 14th cause of cancer death, accounting for 237 deaths in Ghana in the year 2020. 59 Lung cancer burden disproportionately affects people with lower socioeconomic status, 60 posing a huge burden on families and health system. 59 Although more than 80% of the lung cancer deaths were attributed to cigarette smoking, 59 the role of environmental exposure to PAH in burden of lung cancer is yet to be determined in this population.
A retrospective study on the incidence of childhood cancer in Ghana had reported an age-standardized rate (ASR) of 9.36 per 100,000 person-years based on 1073 cases observed in 2 tertiary hospitals from 2015 to 2019. 61 In their report, the most prevalent cancers were lymphomas and leukemia and the ASR was higher in children living in the Greater Accra region and Ashanti regions, 61 which are largely urbanized areas. The higher prevalence of childhood cancers in urban areas were attributed to availability of pediatric oncology units and relative ease of access to care in the regions. 61 However, these urban regions also record high vehicular traffic and emissions from old, poorly maintained vehicles. The role of vehicular traffic and emissions and its associated PAH exposure in the burden of these childhood cancers has not been studied
Exposure to PAH have also been associated with other non-cancers respiratory diseases including respiratory diseases such as chronic obstructive pulmonary disease (COPD) and asthma. Reviewed studies also suggest that PAH exposure may play a role in other respiratory diseases in this population. For example, odds ratios for persistent cough in urban residents 13 were as high as 2.68 (95% CI, 1.43-5.05). The significant positive correlation observed between MDA and PAH markers measured in that study indicated possible lipid peroxidation/cell damage or degenerative disease in these participants. 13 A recent report on COPD in Sub-Saharan African countries indicated that the percentage change of age standardized YLDs due to COPD among Ghanaian males increased by 46.8% between 1990 and 2019. 62 Reports across Ghana also suggest an increasing prevalence of asthma63 -65 in the population. In one of these, 66 use of electricity as domestic fuel, (which reduces household exposure to PAH) was a protective factor for asthma (OR, 0.34; 95% CI, 0.12-0.97), while inner-city residence (which on the other hand increases exposure to PAH through vehicular and industrial emissions) was an independent risk factor for asthma (OR, 4.8; 95% CI, 1.5-5.2). These observations may suggest that exposure to PAH may have significant role in these diseases.
The respiratory effects of PAHs has been linked to oxidative stress and formation of reactive electrophilic metabolites and/or activation and specific binding of parent compounds to cellular receptors such as aryl hydrocarbon receptor (AhR), the β2-adrenergic receptor (β2-AR) and G protein-coupled receptors.67 -69
Exposure to PAH have also been associated with other non-respiratory diseases including cardiovascular diseases such as ischemia, myocardial infarction and stroke70 -73; impaired cognitive function in adults74,75 and children.74,76 Well-designed studies are needed to unravel the role of PAH exposure in these diseases.
Possible Economic Burden of PAH Pollution and Human Exposure in Ghana
Ghana is one of the rapidly industrializing African countries, undergoing a transition from traditional to modern sources of pollution. 33 Given the pervasive nature of PAH pollution and exposure in Ghana, the resultant economic burden may be substantial. These may include increased direct and indirect healthcare costs due to PAH-associated diseases, reductions in human capital and loss of productivity years due to associated health effects and premature death, as well as remediation expenses.
Direct and Indirect Healthcare Costs Due to PAH-Associated Diseases
In Ghana, treating PAH-linked conditions such as cardiovascular diseases, respiratory and neurodegenerative disorders, and neonatal complications imposes significant financial burdens. Stroke admissions cost USD 211.19 per patient, hypertension care is estimated at USD 119,056 per lifetime, neonatal complications at USD 2.48 million annually, and Alzheimer’s may cost USD 3.13 billion by 2050. 27 In comparison, Germany’s healthcare costs from air pollution (including PAHs) range from €15 to 45 billion annually 77 ; the UK forecasts over £5.3 billion by 2035,78,79 and the USA estimates costs around USD 150 billion per year 80 with that of Utah, a state in the USA recording a median estimate of the direct economic costs of air pollution of USD 1.0 billion per year (USD 0.35 to USD 1.65 billion per year). 81 Barwick et al 82 reported of a $42 billion added healthcare spending each year in China due to exposure to air contaminants, including PAH. South Africa’s annual burden is USD 4.9 million. 83 However, data from many African nations remains sparse.
Ghana’s direct and indirect healthcare costs are lower in absolute terms compared to high-income countries like the USA, UK, and Germany, but they are comparable or relatively higher per capita than other African countries due to limited healthcare infrastructure and a rising prevalence of diseases.
Lost Hours and Productivity Due to PAH Exposure Effect
Ghana lost USD 1.63 billion in economic output in 2019 due to PAH-related diseases, equivalent to 0.95% of GDP. This includes USD 1.38 billion from premature deaths and USD 249 million from disability. Caregiver absenteeism further contributes to these losses. In the USA, productivity losses from air pollution reach USD 20 billion annually, 84 while the EU estimates €100 billion in lost labor income.85,86 Kenya’s informal recyclers experience reduced income due to chronic illnesses linked to PAH exposure. 87
While Ghana’s absolute productivity losses are lower than those in developed economies, the relative economic impact (as a percentage of GDP) is significant, indicating a higher burden proportionally on the national economy.
Remediation and Regulatory Costs, and Broader Economic and Social Impacts
Efforts to address PAH-contaminated soil and water in Ghana require substantial resources, though these initiatives are underfunded, and sporadic. Studies from other African countries also indicated that remediation of PAH-contaminated sites, particularly those affected by industrial waste, is very costly.88 -90 Most African countries do not estimate or report the cost of PAH remediation due to limited technical capacity, insufficient environmental monitoring systems, and a lack of prioritization in national budgets.
In developed nations, environmental remediation costs for PAHs in tar sands and industrial regions may cost up to $1.8 billion annually. 91
In Nigeria, the United Nations Environment Program (UNEP) conducted an environmental assessment of the Ogoniland region, which has been severely affected by petroleum hydrocarbon pollution, including PAHs. The report estimated that full-scale remediation would require over USD 1 billion and could span up to 30 years, illustrating the considerable economic burden of remediating PAH-contaminated environments. 92
Similarly, in Egypt, remediation costs for agricultural and urban soils using techniques such as soil washing and phytoremediation have been estimated to range from USD 5000 to USD 30 000 per hectare. These interventions are often supported by international development organizations. 93 Moreover, remediation costs for short-, medium-, and long-term technologies typically range between USD 39 to 331 per tonne, USD 22 to 131 per tonne, and USD 8 to 131 per tonne, respectively. However, total costs vary significantly based on factors such as site location, capital investment, and permitting requirements. 94
The cost implications of implementing PAH regulations in Ghana, including expenditures for monitoring systems and legal frameworks, may also be enormous. Ghana’s remediation spending may seem lower, but this is largely due to insufficient capacity and lack of action, not a lower pollution burden. In contrast, developed countries allocate substantially more resources for environmental remediation.
The economic impacts of PAH exposure extend beyond financial costs, deepening social inequalities as affected communities face additional economic pressures to address contamination and its consequences.95,96 Soil contamination with PAHs compounds is also capable of affecting soil fertility and crop growth, destroying soil micro-flora, and thereby reducing crop yield, which may adversely affect a nation’s economy.97,98 PAH exposure in Ghana disproportionately affects low-income communities near pollution hotspots, similar to marginalized groups in the U.S. and Eastern Europe.99 -101
Soil contamination, particularly from abattoirs and open waste burning, may threaten Ghana’s agriculture. In China, a 15% to 20% drop in rice yield was linked to PAH-contaminated soil, 102 raising similar concerns for Ghana’s food security. The social and economic inequities in Ghana mirror global patterns, but the impact is more severe due to higher dependence on agriculture and lower resilience of affected communities.
Future Perspectives, Strength, and Limitations of the Review
Future research should focus on personal PAH exposure measurements, longitudinal studies linking exposure to specific health outcomes, and economic modeling of disease burdens attributable to PAHs.
Strengths of this review include its comprehensive coverage of environmental PAH contamination in Ghana and its novel integration of public health and economic perspectives. Limitations include the ecological nature of most studies reviewed, limited direct cost assessments, and heterogeneity in study methodologies. Despite these limitations, this review provides critical baseline evidence for policymakers, researchers, and public health advocates seeking to mitigate the health and economic impacts of PAH pollution in Ghana.
Conclusion
This systematic review identified multiple environmental matrices in Ghana, including air, soil, water, and food, that are significantly contaminated with PAHs. The widespread presence of PAHs across these matrices poses a serious public health threat, with potential links to increased incidence of cancers, respiratory diseases, adverse neonatal outcomes, and other chronic illnesses.
The health risks associated with PAH exposure could impose a substantial economic burden on the Ghanaian economy. The costs may arise from increased healthcare expenditures, reduced worker productivity, environmental remediation efforts, and loss of human capital. However, the current literature lacks sufficient personal exposure assessments and robust epidemiological studies to fully quantify these impacts, highlighting a major research gap.
Addressing these challenges will require an integrated approach involving policy interventions, public education, promotion of cleaner technologies, investment in sustainable practices, and the strengthening of environmental monitoring and regulatory frameworks.
Footnotes
Author Contributions
All authors contributed equally.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.