
Abstract
Background:
Healthcare workers’ (HCWs’) knowledge in delivering medical services is significantly influenced by their understanding of zoonotic diseases and the One Health (OH) concept. This study investigates the extent of HCWs’ knowledge and experience regarding zoonosis and the One Health approach in Ghana.
Methods:
This cross-sectional study involved 182 HCWs at the Tamale Teaching Hospital who completed questionnaires. Logistic regression was conducted to assess associations between socio-demographic factors and knowledge of zoonoses and OH. The correlation between knowledge and self-reported experience with zoonoses was assessed using Spearman’s correlation.
Results:
While 79.7% of HCWs correctly defined zoonoses, only 18.7% could sufficiently identify zoonotic diseases, and 59.3% were familiar with OH. The most commonly identified zoonotic disease was Ebola (75.3%), while brucellosis (12.1%) was the least recognized. Medical doctors were more likely to report previous encounters with zoonoses. Compared to medical doctors (reference HCWs), knowledge of OH was significantly higher among biomedical scientists (OR = 2.25, 95% CI: 0.72-7.37) and lower among nurses (OR = 0.92, 95% CI: 0.33-2.60). Professional experience of more than 5 years was associated with greater knowledge of rabies and tuberculosis. There was no significant correlation between knowledge of zoonoses and self-reported experience with any of the assessed diseases, except for a weak negative correlation with trypanosomiasis (Spearman’s r = –0.206, P = .005).
Conclusions:
The majority of HCWs have inadequate knowledge of zoonosis. Although most HCWs are aware of OH, they have limited experience with zoonosis and OH. Curricula for training HCWs should include more courses on zoonosis and arrange refresher training programs for HCWs. Enhancing HCWs’ expertise in zoonotic disease surveillance and detection is crucial for early identification and control of zoonoses, aiding in the prevention of future outbreaks.
Introduction
Zoonoses are diseases that can be transmitted between animals and humans. Approximately 60% to 75% of human infectious diseases, and about 75% of emerging and re-emerging infectious diseases, are zoonotic. 1 The emergence of zoonotic diseases in Africa is associated with factors such as urbanization, armed conflict, deforestation, poverty, and limited agricultural intensification and input usage. Additional contributors include the consumption of bushmeat, the practice of keeping livestock near or within homes, and the presence of abundant mammalian reservoir hosts and disease vectors. Furthermore, corruption, and an overreliance on natural resources significantly deplete biological resources, increasing the population’s vulnerability to zoonosis.2 -5 Annually, it is estimated that around 2 billion human infections are zoonotic, resulting in approximately 2 million deaths. 6 With most zoonoses considered underreported and neglected, 7 the actual numbers could be higher.
The One Health (OH) approach is an integrated, collaborative approach that combines multiple sectors and disciplines at local, regional, national, and global scales. It aims to achieve optimal health outcomes by acknowledging the integration of humans, animals, plants, and their shared environment. 8 The OH approach enhances disease surveillance, data sharing among stakeholders, diagnostic laboratory systems, and networks for the early detection and response to zoonotic diseases by fostering robust collaboration across relevant sectors. 9 The OH approach helps prevent zoonotic disease outbreaks, enhances food safety and security, mitigates antimicrobial resistance, safeguards global health security, and supports biodiversity and conservation efforts. 8 Ghana, like several African countries, strives to institutionalize and implement OH-based approaches5,10 including acceptance of membership to Global Health Security Agenda (GHSA) 11 and successful organization of One Health Zoonotic Disease Prioritization (OHZDP) workshop leading to the prioritization of 6 zoonoses: anthrax, rabies, zoonotic avian influenza, zoonotic tuberculosis, viral haemorrhagic fevers and trypanosomiasis. 12
The Northern region of Ghana contribute to the highest livestock populations in the country.13,14 The high population of livestock in the region is attributed to the abundance of diverse forage sources, the high demand for livestock and their products, and the availability of labor for livestock husbandry.13,15 With most of the livestock reared under extensive and free-range management systems, 16 the Northern region is a hotspot for zoonoses due to increasing human-animal interfaces. It is imperative to determine the knowledge of healthcare workers (HCWs) on zoonoses and the OH approach to assess their preparedness for disease outbreaks and to help regulatory bodies design specific programs to address identified deficiencies. To the best of the researchers’ knowledge, this study is one of the first in West Africa, particularly Ghana, to assess HCWs’ knowledge of various zoonotic diseases, as well as their understanding and experience with zoonoses and the OH approach. The study’s specific objective was to determine the knowledge and experience of HCWs in northern Ghana regarding zoonoses and the OH approach.
Materials and Methods
Study Design
This cross-sectional study, conducted between June and September 2023 at the Tamale Teaching Hospital (TTH) in Tamale,d the capital of the Northern Region of Ghana, used both closed and open-ended questions to assess the knowledge and experiences of HCWs on zoonoses and the OH approach. Purposive sampling was used. There were 2371 HCWs in total when the study was conducted but we targeted primary health workers (n = 1040). Primary HCWs were chosen because they represent the first point of contact for individuals seeking medical care at TTH. Using Morgan and Krejcie’s sample size table, a sample size of 285 was determined. We therefore invited randomly selected 285 HCWs to this study. Of these, 182 participants agreed to take part in the study, resulting in a response rate of 64%. TTH currently serves as the only referral hospital in the Northern region of Ghana, and ranks as the third-largest teaching hospital in Ghana, following Korle Bu and Komfo Anokye Teaching Hospitals. The hospital trains health professionals at both the graduate and undergraduate levels.
Data Collection
Before the questionnaires were admiministered, the significance and the objective of the study were clearly explained to all participants to ensure informed participation. The questionnaire was self-administered and distributed daily from June to September 2023, with participants allotted 30 minutes to complete it. To ensure comprehensive participation, we targeted HCWs on both night and day shifts to avoid excluding any eligible respondents. To enhance data accuracy and minimize response bias, trained data collectors were present throughout the process to provide necessary clarifications and address any concerns raised by participants. Additionally, to protect participants’ privacy and maintain confidentiality, no personal identifiers, such as names or staff identification numbers were collected. Upon completion, each questionnaire was carefully reviewed for completeness before being recorded for data entry and analysis.
Questionnaire Development
The multi-section questionnaire (Supplemental File 1) collected data on demographics (including sex, age group, profession and professional experience referring to the length of time in years respondents have spent in their current professional position), the ability to identify 25 zoonotic diseases from a list of 27 diseases, and knowledge of 4 aspects (etiology, transmission, diagnosis, and clinical signs) of 5 selected zoonoses by the HCWs. The 25 zoonotic diseases included in the list were those that had been previously reported in Ghana 17 The 5 zoonoses were prioritized anthrax, rabies, African trypanosomiasis, zoonotic tuberculosis 12 and brucellosis which, albeit not prioritized, is considered relevant and endemic in the region. Additionally, all 5 diseases are notifiable in Ghana, with annual reports in the study area. The questionnaire also assessed the knowledge of HCWs on OH, as well as their experiences and training in handling zoonoses. To assess validity, face and content validity were evaluated by 3 veterinarians trained in zoonotic diseases and public health, along with a statistician. These professionals reviewed the questionnaire for clarity, relevance, and comprehensiveness. The evaluation process involved multiple rounds, during which they assessed each item’s alignment with the intended construct, language appropriateness, and coverage of key concepts. Based on their feedback, several items were refined to improve clarity and ensure coherence. Their recommendations were incorporated to enhance the overall quality of the questionnaire. Additionally, the authors further moderated the questions to ensure consistency. To test clarity, the questionnaire was pretested with 10 HCWs at the Nyankpala Health Centre. The reliability of the questionnaire was evaluated using Cronbach’s alpha, which produced a score of .899 across 69 items, demonstrating a good level of reliability. The time to complete the questionnaire was set at 30 minutes, and respondents were supervised to prevent any form of answer-sharing, internet searches, or discussion between participants.
Data Management and Analyses
All completed questionnaires were coded and entered into the IBM Statistical Package for the Social Sciences (SPSS) version 25 (Chicago, IL, USA). Descriptive statistics were performed, and the data were presented as frequency distributions and graphs. The expectation was that all the listed diseases in the second part of the questionnaire would have been identified as zoonotic, except for malaria 18 and HIV/AIDS. 19 In assessing HCWs’ ability to identify zoonotic diseases, each correct identification in this section was assigned a score of 1, while each incorrect answer was assigned a score of 0, resulting in the highest possible score of 27. HCWs’ ability to identify zoonotic diseases was categorized into 2 groups: those with a total score equal to or greater than 50% of the maximum possible score (ie, 13.5 marks, rounded up to 14, ⩾14) and those with a total score below 50% of the maximum possible score (<14). Thus, HCWs were considered to have sufficient recognition of zoonoses if they scored ⩾50% of the total score and insufficient recognition if they scored <50%. This scoring criterion has been previously used in a related study in Ghana. 20
Concerning the knowledge scoring on the 5 zoonotic diseases, a HCW was considered to have adequate knowledge of a particular disease if he/she correctly identified all aspects of each of the 5 zoonotic diseases. This scoring criterion was based on the fact that a lack of knowledge on any aspect of a zoonotic disease could potentially lead to misdiagnosis and underreporting.21,22 Associations between the level of training of HCWs and knowledge of the 27 listed diseases, as their familiarity with and expertise in zoonoses and OH were determined by the Chi-square test. The association between socio-demographic factors and participants’ level of knowledge of these zoonoses and OH is performed with the logistic regression and presented as odds ratios (OR) with 95% confidence intervals (CI), adjusted for gender and professional experience. It was not adjusted for age due to an insufficient number of study subjects in 2 out of the 3 age groups. The association between the level of knowledge of the selected zoonoses and self-reported experience (encountered cases) of those diseases was assessed by Spearman’s correlation, with a P-value < .05 considered statistically significant. There was no missing data in our dataset since our participants were encouraged to complete the questionnaires.
Ethical Consideration
Permission was sought and obtained from the Research and Development Department of TTH. The permission notice had a reference number of TTH/R&D/SR/140. The study was approved by the University for Development Studies Institutional Review Board (IRB No. 2023/003–023) and conformed to the ethical guidelines of the Declaration of Helsinki. All written consents were signed voluntarily by study participants. Respondents were assured that a lack of accurate knowledge would not impact their practice and that all information provided would be used solely for research purposes as anonymized data.
Results
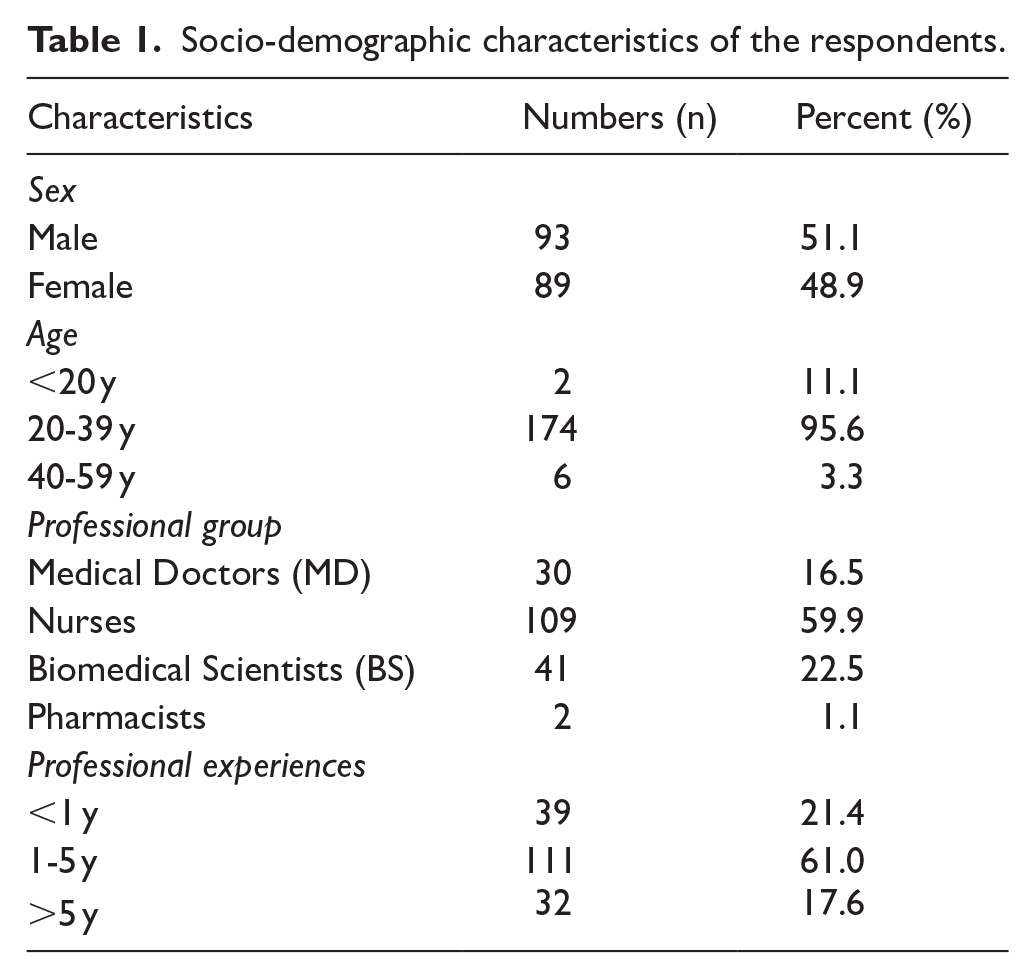
Socio-Demographic Characteristics of the Respondents
The majority of HCWs in the study were males (51.1%), with 95.6% of them falling within the age range of 20 to 39 years. Most HCWs were nurses (59.9%), and 61% had been employed for 1 to 5 years (Table 1)
Socio-demographic characteristics of the respondents.
Hcws’ Accurate Knowledge of the Definition of Zoonosis and Correct Identification of Zoonotic or Non-zoonotic Diseases
A majority (79.7%) of the HCWs knew that zoonotic diseases are shared between humans and animals (Supplemental Table 1). The most accurately identified zoonotic diseases were Ebola (75.3%), monkeypox (69.2%), and Newcastle disease (50.5%). The least accurately identified were hepatitis E (14.8%), fasciolosis (13.7%), and myiasis (13.7%). There were statistically significant differences in the ability of the various HCWs to correctly identify the listed zoonotic diseases, except for Ebola virus (P = .074). Biomedical scientists demonstrated the highest level of expertise in identifying zoonotic diseases compared to other HCWs, making them the most knowledgeable respondents. The majority of respondents knew that malaria (81.3%) and HIV/AIDS (89.6%) were not zoonotic, and there were no significant differences in the knowledge of these diseases as non-zoonotic among HCWs (P = .163 and P = .130, respectively).
Ability of HCWs to Identify Zoonotic Diseases
About a fifth (P < .001) of HCWs demonstrated a total score of the ability to identify zoonotic diseases that was equal to or greater than 50% (Figure 1). Biomedical scientists demonstrated the highest proficiency in identifying zoonotic diseases (63.4%).
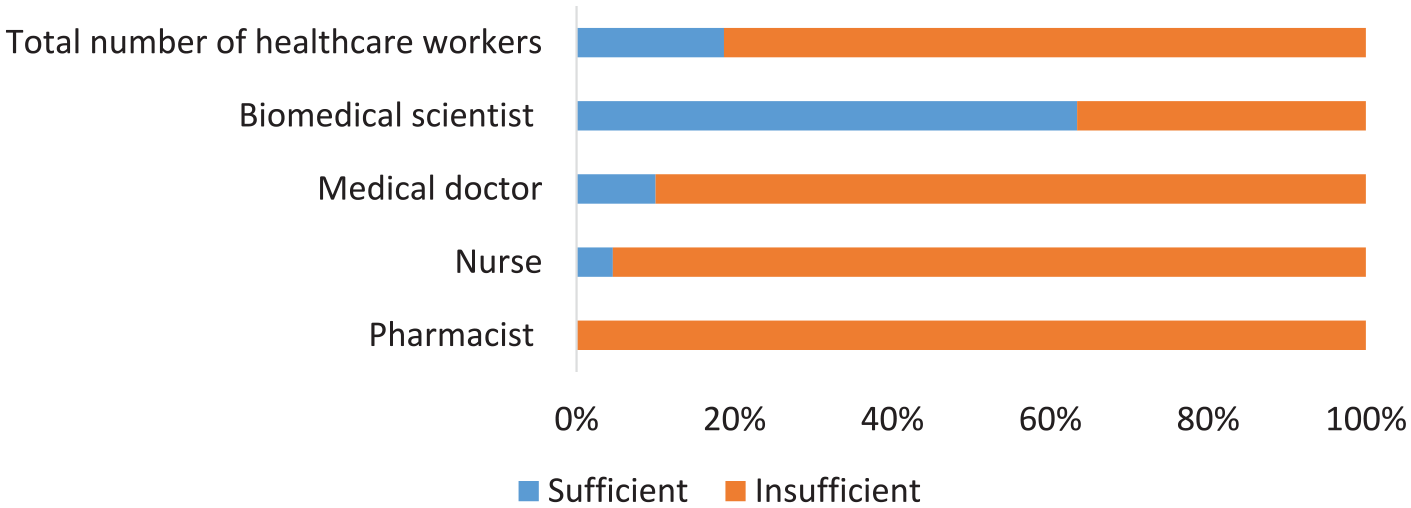
Ability of healthcare workers (HCWs) to recognize zoonoses. HCWs sufficiently recognize zoonoses if they score ⩾50% of the total score and insufficient if they score ⩽ 50% of the total score.
Correct Knowledge of the Four Aspects of Anthrax, Rabies, Brucellosis, African Trypanosomiasis, and Zoonotic Tuberculosis
Generally, most of the HCWs knew more about the etiology and mode of transmission and the least of the diagnoses of the 5 diseases (Figure 2A-E, Supplemental Table 2). The HCWs had inadequate knowledge of all the diseases: brucellosis (98.4%), rabies (94.0%), anthrax (90.1%), trypanosomiasis (88.5%) and zoonotic tuberculosis (84.6%; Figure 2F, Supplemental Table 3). However, biomedical scientists exhibited a robust understanding of the diseases followed by medical doctors and nurses.

Level of correct knowledge of healthcare workers (HCW = 182). (A-E) shows their correct knowledge on various aspects of each of the 5 zoonotic diseases. (F) is the overall correct knowledge on each zoonosis. [Medical Doctors (MD) = 30, Nurses = 109, Biomedical Scientists (BS) = 41 and Pharmacists = 2] ’The colors in the legend for section E also apply to sections (A-D).
Knowledge, Experience and Training Needs of HCWs Regarding Zoonosis and OH
Most HCWs had never encountered any zoonotic disease in their career (76.9%), never had any form of public health education (92.9%), or were involved in a workshop or training (97.3%) regarding zoonotic diseases before this study (Table 2). The zoonoses encountered by the few HCWs (23.1%) were rabies (69.0%), tuberculosis (31%), anthrax (23.8%), dengue (4.8%), brucellosis (4.8%), salmonellosis (2.4%), toxoplasmosis (2.4%), cysticercosis (2.4%), Ebola (2.4%), and trypanosomiasis (2.4%; Figure 3; Supplemental Table 4). A greater proportion of HCWs who discussed zoonoses with veterinarians (12/182,6.6%) were confident to do so (8/12,66.7%). The OH concept was known by 59.3% of the HCWs; mostly the biomedical scientists (66.7%) and doctors (66.7%). In all, the HCWs appreciated the relevance of refresher courses on zoonoses in their profession (74.7%). A post hoc analysis adjusted by the Bonferroni method showed a statistically significant difference between medical doctors and biomedical scientists (adjP = 0.039) in their encounter with a zoonotic disease in their line of practice/work, and a statistically significant difference between nurses and biomedical scientists (adjP = 0.002) in their knowledge of OH
Healthcare workers’ knowledge of OH experience with zoonosis, and training needs.

Abbreviations: BS, biomedical scientist; HCW, healthcare workers; MD, medical doctor; Ph, pharmacists.
P ⩽ .05.

Zoonotic diseases encountered by healthcare workers. Total healthcare workers (HCW = 42), medical doctor (MD = 12), Biomedical Scientists (BS = 4), Pharmacists = 2, Nurses = 26.
The Association Between Sociodemographic Factors and Participants’ Level of Knowledge of Zoonosis and OH
In adjusted (Table 3) and not adjusted (Supplemental Table 5) logistic regression analysis, the level of knowledge of selected zoonoses and the knowledge on OH was generally lower in males than females (except for Rabies, OR = 1.34, 95% CI: 0.35-5.65), higher in medical doctors than other professional groups (except for Trypanosomiasis and Anthrax), and was not associated with professional experience, as it was higher only for HCWs with 1 to 5 years of experience regarding Brucellosis (OR = 2.39, 95% CI: 0.20-58.00) and for those with >5 years of experience regarding Rabies (OR = 2.62, 95% CI: 0.21-31.38).
The association between sociodemographic factors and participants’ level of knowledge of 5 zoonoses and knowledge of OH, presented as OR with 95% CI and adjusted for sex and professional experience.

Reference, NA – not applicable due to lack of variable; BS, biomedical scientist; CI, confidence interval; OH, one health; OR, odds ratio; Ph, pharmacists.
The Association Between the Level of Knowledge of Zoonosis and Self-Experience
In Spearman correlation (Table 4), there was a significant weak negative correlation between the level of knowledge of trypanosomiasis and self-experience (encountered cases of trypanosomiasis).
The association between the level of knowledge of zoonoses and self-experience (encountered cases) of the diseases assessed by Spearman correlation.

P ⩽ .05.
The significant P-value (P=0.005) for trypanosomiasis indicates statistically significance, albeit weak negative correlation(-0.206) between knowledge of trypanosomiasis and self-experience(encountered cases) of the disease. This suggests that HCWs who reported encountering cases of trypanosomiasis tended to have lower knowledge levels about the disease, or vice versa.
Discussion
Our study shows that most of the HCWs were familiar with the definition of zoonosis. Our findings are comparable to the findings of studies in Tanzania. 23 This contrasts with observations made in Uganda 22 where primary caregivers, albeit aware of zoonoses, thought disease transmission was only from animals to humans. The correct identification of malaria and HIV/AIDS as non-zoonotic by most HCWs in this study is comparable to observations made in Uganda. 22 This could be attributable to adequate education of HCWs on these diseases in response to their hyperendemicity in these locations. Except for Newcastle disease, the top 3 identified zoonoses (Ebola, monkeypox, and avian influenza) are diseases that have recently gained global notoriety due to persistent outbreaks and have warranted intense public education and governmental interventions to prevent or manage these outbreaks. Biomedical scientists demonstrated the highest level of expertise in identifying zoonotic diseases compared to other HCWs, making them the most knowledgeable respondents. One possible explanation for the higher proficiency among biomedical scientists in identifying zoonotic diseases is their educational background and training, which often includes more in-depth coursework in microbiology, infectious diseases, and disease transmission. Additionally, their professional roles frequently involve laboratory work and diagnostics related to pathogens, which may enhance their familiarity with zoonoses.
Similarly, a negative correlation between knowledge and the encounter of Trypanosoma cases was observed among biomedical professionals. This can be explained by the fact that their knowledge of trypanosomiasis likely stems from academic and laboratory training rather than direct clinical exposure. As a result, these professionals, despite having strong theoretical knowledge, may encounter fewer clinical cases due to their limited involvement in frontline diagnosis and treatment. Thus, their theoretical expertise does not necessarily translate into practical case encounters, resulting in an inverse relationship.
Although the HCWs were able to define zoonoses, they were generally unable to identify most zoonotic diseases and had lower knowledge of the 5 selected diseases. These findings compare with the findings of a previous study, which also reported similar knowledge gaps among HCWs regarding zoonotic diseases. 22 Their level of knowledge of zoonoses was independent of years of professional experience and profession, although doctors appeared to know more than other HCWs. This finding challenges the assumption that experience equates to expertise in zoonotic disease management. The least recognized aspect of a zoonotic disease was the diagnosis, a pattern identical to observations made in Uganda 22 and Tanzania, 21 reflecting the barriers to disease diagnosis in some African countries. These variations in HCWs’ knowledge regarding different aspects of zoonoses (such as knowledge of the disease agent, transmission, clinical signs, and diagnoses) can be attributed to differences in professional training, clinical exposure, and scope of practice. For instance, biomedical scientists may demonstrate superior knowledge of pathogens (bacteria, viruses, parasites) due to their intensive training in laboratory diagnostics. In contrast, medical doctors and nurses are likely to be more proficient in identifying disease transmission and clinical signs due to their direct patient care responsibilities. However, in Kenya, the least known aspects of a zoonotic disease were the etiological agent and transmission. 21 There is evidence that healthcare professionals’ knowledge of a disease increases with its local occurrence, the inability to diagnose a disease might affect the prevalence or incidence of the disease. The low occurrence of the selected zoonoses in humans might directly affect the willingness of HCWs to learn about most zoonotic diseases. 23
The effectiveness of the OH concept has been observed in the successful management of several epidemics including sleeping sickness in Uganda’s Busoga Region (1976-1983)24,25, H5N1 highly pathogenic avian influenza virus in chickens in Kaduna state in northern Nigeria (2006)26 -28and rabies in Namibia (2015). 29 We argue that the awareness of HCWs of the OH definition, was not reflected in their practices. For instance, nearly all the HCWs had not discussed any zoonoses with their animal health colleagues. While this observation could be attributed to the low encounter with zoonoses in the careers of HCWs, the inadequacy of public health education, training, and the neglect of most zoonoses might also play a role in the reduced and potentially ineffective collaboration between animal and human healthcare providers. By contrast, in Kenya, 85% of public health workers reported having discussed zoonoses with their veterinary colleagues, and 98% were involved in public health education on zoonotic diseases. This lack of collaboration in Ghana may be attributed to limited encounters with zoonotic diseases during HCWs’ careers, insufficient training, and the broader neglect of zoonoses in public health education. Additionally, the structural separation of human and animal health systems creates significant barriers to interdisciplinary communication.
To address these challenges, we propose a multi-tiered strategy to enhance the knowledge, collaboration, and practice of zoonotic disease management in Ghana. We propose institutional reforms that will bridge the gap between animal and human health in Ghana. For instance, the 2 health sectors in Ghana could be unified under one ministry instead of 2 (ie, Animal health under the Ministry of Food and Agriculture, and Human health under the Ministry of Health). This could help eliminate inherent barriers resulting from governmental bureaucracies and open channels for the easy implementation and application of OH principles and approaches. Such reforms could trickle down to tertiary institutions to ensure the familiarization of health professionals across various sectors during their formative years. Early exposure to collaborative practices would encourage stronger professional relationships, enabling seamless cooperation in practice. In addition, we suggest the implemention of refresher courses and continuing education programs. Regular, mandatory training sessions on zoonotic diseases for HCWs across disciplines are essential. These courses should cover disease recognition, diagnosis, and management while emphasizing the OH approach to disease prevention and control. Additionally, digital platforms, such as webinars and online modules, can ensure widespread access to updated knowledge for HCWs in remote areas.
In the interim, the country can adopt other measures, such as promoting community engagement through public health education programs and OH collaborations, as part of its efforts to mitigate zoonotic diseases on the continent. Addressing zoonoses effectively involves integrating health education into popular media, such as cartoons, newspapers, TV and radio programs, and including the OH approach in school curricula. 30 For example, cartoons, advertisements or dramas in different local dialects, depicting zoonotic disease prevention can resonate with diverse audiences. Finally, Ghana can draw inspiration from Kenya’s collaborative approach, which has successfully fostered communication between human and animal health professionals. Similar frameworks could be adapted to the Ghanaian context, with pilot programs in high-risk regions.
Strengths and Limitations
This study has several strengths. It provides novel insights into the knowledge and experiences of HCWs in Ghana regarding zoonotic diseases and the OH approach. The study site is a representative hospital in the Northern Region of Ghana.
The study is particularly relevant as zoonotic diseases continue to pose a major public health threat, requiring an interdisciplinary approach for effective management. The use of a structured questionnaire allowed for systematic data collection. Additionally, the study highlights gaps in knowledge and the lack of interaction between HCWs and veterinary professionals, which could inform future training and policy reforms.
However, this study also has limitations. The response frequency was 64%, and the target sample size was not fully achieved due to a combination of factors, including the reluctance of some HCWs to participate, likely attributable to their demanding work schedules. Additionally, staff absences during the data collection period may have contributed to the reduced participation rate, as the same individuals were often encountered during repeated visits. Despite the lower-than-anticipated response rate, statistical analyses, Cronbach’s alpha, which produced a score of .899 across 69 items, demonstrated a good level of reliability and confirmed that the obtained sample was representative and retained sufficient power to detect significant associations, ensuring the reliability of the study findings. Also, the very small sample of pharmacists (n = 2) may have led to extreme or non-representative outcomes. While we retained these observations in primary analyses for completeness, readers should interpret pharmacist-specific findings with caution and can not be generalizable. Future studies should intentionally oversample pharmacists to allow for robust subgroup analyses. Moreover, Ghana’s healthcare system features a dynamic and continuously evolving workforce, with many professionals shifting between roles,seeking greener pastures in first world countries or advancing their education. This fluidity may account for the relatively shorter work experiences observed.
Conclusion
Generally, HCWs at the TTH have inadequate knowledge of several zoonoses. However, the majority of HCWs are aware of the OH concept but have little experience with zoonoses and OH. Promoting collaborative efforts under the OH framework is of paramount importance in Ghana. This could be achieved by merging animal and human health under a single ministry and creating avenues for increased interactions between human health workers and veterinarians. Refresher training programs for healthcare professionals focusing on zoonoses and OH approaches could also be organized. Due to the increasing frequency of zoonotic outbreaks globally (such as COVID-19, Ebola, and monkeypox), there is a growing need to strengthen health systems, enhance surveillance and diagnostic capacities, and improve the knowledge and preparedness of healthcare workers to effectively prevent, detect, and respond to such emerging threats. Addressing these challenges requires bold, systemic reforms that bridge the divide between human and animal health sectors. Public health education, institutional integration, and proactive collaboration are key to safeguarding human and animal health against future zoonotic threats. The study is especially relevant for countries in sub-Saharan Africa where zoonotic spillover risks are high due to close human-animal-environment interactions and under-resourced health systems.
Supplemental Material
sj-docx-1-ehi-10.1177_11786302251339881 – Supplemental material for Assessing the Knowledge and Experience of Healthcare Workers in Zoonoses and the One Health Approach: A Cross-Sectional Study in Ghana
Supplemental material, sj-docx-1-ehi-10.1177_11786302251339881 for Assessing the Knowledge and Experience of Healthcare Workers in Zoonoses and the One Health Approach: A Cross-Sectional Study in Ghana by Godwin Dogbey, Brigid Unim, Abbiw Richard Kwamena, Godwin Clinton Ahiabor, Marta A. Kisiel, Xingwu Zhou, Apollo O. Maima, Amidu Abdul-Aziz, Ben Enyetornye, Robert Niayele, Anthony Amison Agbolosu and Kweku Asare-Dompreh in Environmental Health Insights
Footnotes
Acknowledgements
We would like to thank the management of the TTH for permitting us to conduct this study at their facility. We also thank all HCWs who participated in the study.
ORCID iDs
Authors’ Contributions
GD, RN, BE, AAA, AA and GCA conceptualized the study. GD, RN, AAA, BU, ARK, GCA, KAD, AOM, MAK, AA, BE, elaborated the research methodology. RN, AAA, GD and GCA conducted the survey. GD, BU, MAK, XZ, ARK and KAD performed data analysis and data interpretation/visualization. GD and BU drafted the manuscript. BU, MAK, AOM, XZ, ARK and KAD critically reviewed and improved the manuscript. All authors substantially contributed to the study and approved the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available upon request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.