
Abstract
Background:
The scarcity of safe drinking water affects individuals living in low income areas, increasing their vulnerability to waterborne diseases. This study aimed to investigate the relationship between socio-economic factors, water handling practices and microbial water quality in Kitwe District, Zambia.
Methods:
A cross-sectional study was conducted among 215 households using a semi-structured questionnaire along with microbiological analysis of water samples during the dry and wet season. A total of 44 water samples (per season) from the point of use and 16 source samples were analyzed for pH, temperature, residual chlorine, total coliforms, and Escherichia coli. Multivariable logistic regression analyzed associations between socio-economic factors, water handling practices, and water quality.
Results:
The prevalence of Escherichia coli contamination was 61.3% during the dry season and 77.3% during the wet season. Key factors associated with household water quality included, household monthly income, education level, family size, season, storage container design, water withdrawal method, covering storage containers, water treatment practices, and hand washing with soap. Notably, households that used narrow-mouthed containers (AOR = 0.090, 0.014-0.580), covered their storage containers (AOR = 0.113, 0.014-0.889), and practiced water treatment (AOR = 0.120, 0.022-0.656) showed significantly reduced risks of E. coli contamination.
Conclusion and recommendations:
The findings highlight the importance of socio-economic factors and proper water handling practices in improving household water quality. To enhance water safety and reduce water-related diseases, targeted interventions should focus on educating communities about the effective handling of water. Furthermore, addressing socio-economic factors and improving access to safe water are essential for mitigating contamination risks in low-income areas.
Introduction
Safe water supply is a fundamental need and a human right that is vital for the health of people in a community. Limited access to clean drinking water, unimproved sanitation facilities and poor water management practices can lead to the emergence of waterborne diseases such as diarrhea, which is responsible for approximately 1.6 million deaths in developing and economically disadvantaged regions1,2 Unsafe water, inadequate sanitation and poor hygiene practices contribute to about 88% of diarrhea associated deaths. 3
In South Asia, studies have shown that poor sanitation, inadequate water handling, and environmental factors contribute to contamination of drinking water. For instance, in Nepal, water quality deteriorates during the rainy season due to poor storage and water distribution issues4,5 while in Bangladesh, human activities related to water, sanitation and hygiene exacerbate water contamination. 6 In Africa, contaminated drinking water remains a major public health concern, as exposure to microbial pollutants can lead to outbreaks of diseases such as diarrhea and cholera.7,8 The sources of contamination often include inadequate sanitation systems, leaks in distribution systems and groundwater contamination, particularly in areas where humans and animals share water sources.9 -11
The unreliable provision of water and sanitation services in developing countries is a key factor contributing to the high prevalence of waterborne diseases, including diarrhea, dysentery, cholera, and typhoid.12,13 In addition, socio-economic factors such as; education, income and occupation may be other potential influential factors associated with the prevalence of waterborne diseases. 14 In a systematic review by Azanaw et al, 15 their study showed a significant association between the level of education and risk of waterborne diseases. Their conclusion was that education is an influential factor in the occurrence of diarrheal diseases in Africa. Similarly, a study conducted in Ghana, Malawi, Mozambique, Niger, Rwanda, Uganda, and Zambia, revealed significant variations in water access and microbial drinking water quality. The findings highlighted education levels to be associated with microbial water quality in Niger and Zambia. 16
At the household level, improper water handling practices during transport and storage can introduce contamination with pathogens of fecal origin, compromising water quality. 17 Studies in Kenya, Ethiopia and Zambia have shown that jerry cans and clay pots are the most commonly used water collection containers.18 -20 However, inadequate cleaning of these containers, coupled with exposure to contaminants, increases the risk of microbial contamination. As a result, stored water can become unsafe before consumption due to bacterial growth.21,22 The deterioration of drinking water quality is often linked to unhygienic storage conditions, lack of proper sanitation facilities and inconsistent household water treatment practices. In many cases, contamination occurs at multiple points, from collection to storage and final use, highlighting the need for improved handling practices to ensure safe drinking water.23,24
Sustainable Development Goal 6 aims to achieve universal and equitable access to safe and affordable drinking water for all by 2030, including Zambian citizens. 25 However, in 2020, over a quarter (26%) of the global population lacked access to improved drinking water, while nearly half (46%) did not have access to improved sanitation. By 2030, billions will still face these challenges unless progress accelerates fourfold. 26 Household water handling practices are crucial in achieving this goal, in addition to the availability and quality of water sources.
The World Health Organization (WHO) recommends employing household water treatment such as chlorination at the point of use, as this can reduce the incidence of water-related diseases such as diarrhea.27,28 In Sub-Saharan African countries, where many people rely on unsafe drinking water, treatment rates remain low, with 29% of the population using unimproved water, only 22% of households treating their water and 18% employing an adequate treatment method. 29 Household water treatment methods, such as boiling, chlorination, filtration, solar disinfection, and slow sand filtration are widely recommended for improving drinking water quality and reducing the risk of waterborne diseases. 30 These methods have been shown to effectively reduce microbial contamination when used consistently. A study in Zambia by Rosa et al 31 found that chlorination was the most commonly used method compared to boiling. Similarly, field trials in Ethiopia demonstrated that chlorine based point of use treatment significantly reduced the incidence of diarrhea. 32 Sikder et al 33 also highlighted the effectiveness of chlorine in reducing E. coli contamination in household water in Bangladesh. However, challenges such as water treatment costs, inadequate knowledge, poor attitudes, and unhygienic practices in households may hinder the effectiveness of household water treatment technologies. 34 As a result, monitoring the quality of water quality has emerged as a critical element in national water, sanitation and hygiene assessments. 35
Evidence suggests that water quality may vary seasonally, highlighting the need for ongoing evaluation of water safety throughout the year.36 -38 Outbreaks of waterborne diseases exhibit both spatial and temporal variations, being more prevalent in peri-urban areas with inadequate planning when compared to urban settings.39,40 These outbreaks are particularly common during the wet season, when contamination risks are heightened, while they tend to be less frequent in dry periods. An epidemiological survey by World Health Organization (WHO) 41 reported that the recent cholera outbreak in Zambia resulted in over 22 000 cases and 719 deaths primarily during the wet season.
Previous studies done in informal settlements of Zambia have found high levels of microbial contamination in drinking water42 -44 but have not evaluated the factors that may led to contamination during transportation, storage and within the household. Against this background, the study aimed to assess the relationship between socio-economic factors, water handling practices, and microbial water quality at the point of use in Kitwe district. It was hypothesized that these factors at the household level significantly contribute to microbial contamination of drinking water.
Methods
Study Area
The study was conducted in the Copperbelt province in Kitwe district in Ipusukilo settlement with latitude 12°45′S and longitude 28°20′E (Figure 1). The area has a population of 31 405 distributed across 3 distinct zones stretching along the Kafue River basin. Kitwe experiences annual average temperatures ranging from 9°C to 31°C. The lowest average temperature of 9°C is recorded in July and the highest average temperature of 31°C is recorded in October. According to the Zambia Meteorological Department, the average annual rainfall for Kitwe is 1258 mm and the majority of precipitation occurs during the months of December to March. The driest month for the city is October. 45
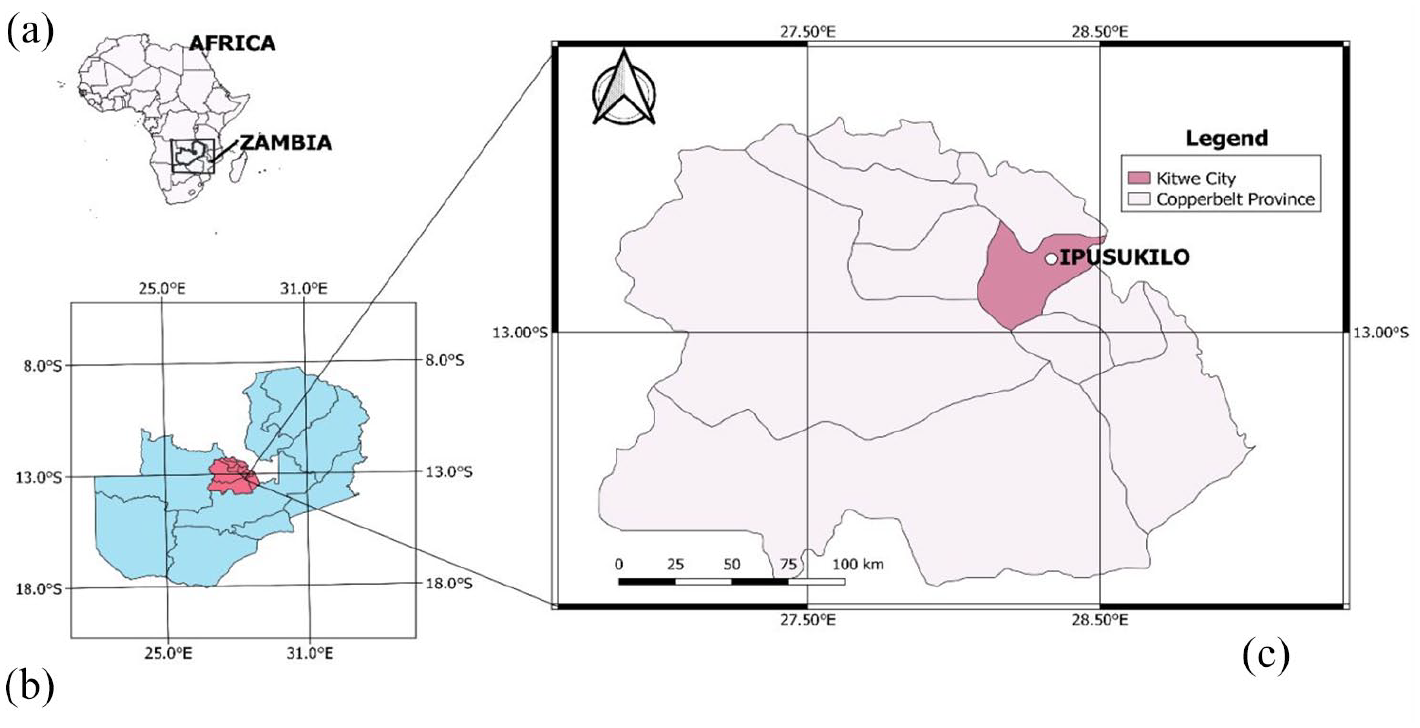
Map showing the African continent (a), the country Zambia (b), the Copperbelt province, and Kitwe city (c).
Study Design
The research study utilized a cross-sectional study design in which qualitative data on the socio-economic and water handling practices was collected using a semi-structured questionnaire. Additionally, microbiological analysis was conducted on water samples from the source and point of use.
Study Variables
Water contamination can arise from numerous sources, however, this study concentrates on Escherichia coli bacteria, a widely recognized microbial indicator of drinking water quality. E. coli serves as a critical parameter for assessing the quality of drinking water, as its presence indicates fecal contamination. Therefore, it was considered the main dependent variable. To identify factors associated with fecal contamination in stored drinking water, a binary coding system was established. The presence of E. coli was coded as 1, indicating contamination, while its absence was coded as 0, signifying no contamination.
The independent variables that could influence the presence of E. coli in drinking water were the socio-economic characteristics (gender of the household head, educational level, household family size, and monthly household income) and water related practices (water collection, storage and hygiene factors).
Sample Size
The decision on the number of households in this study was determined using the Nassiuma formula. 46

Where: n: represents the study sample size, N: represents the total number of households (4800), C: coefficient of variation (30%), e: margin of error (2%). Using Equation 1, the sample size of the study was 215 households.
Sampling Technique and Procedure
The study employed stratified sampling, followed by proportionate sampling, to select households from the 3 administrative zones: Zone 1 (southeast), Zone 2 (southwest), and Zone 3 (northwest). This approach ensured a total sample size of 215 households. The households were selected using simple random sampling. First, a list of blocks and the number of households per block was obtained from the local administration office. Each household in the selected blocks was assigned a number. Households in the block were listed and numbered in a sequence. Houses in each block were identified using administrative codes, specifically IP 1023 (where IP stands for Ipusukilo, 10 indicates the block number, and 23 refers to the household number). Next, a random sample generator, utilizing the RANDBETWEEN function in Excel was then used to select the required number of households from each stratum until the desired sample size was reached.
Water Sample Collection and Microbial Analysis
A sample size ranging from 44 to 100 households is generally considered sufficient to obtain representative data on water quality in areas with a total household population between 4000 and 6000. 47 In this study, water samples were collected in triplicate from 44 household storage containers during the dry and wet seasons, resulting in a total of 132 samples per season. Additionally, 16 water sources (shallow wells), were sampled. All water samples were analyzed for Escherichia coli and total coliforms. Residual chlorine levels were measured using a color comparator with N, N-diethyl-p-phenylenediamine (DPD) as the reagent.
Water sampling, handling, and processing were conducted according to WHO 48 and American Public Health Association (APHA) 49 guidelines on water handling and processing. To ensure that contamination of water samples did not occur during collection, handling, transportation and storage before laboratory analysis, strict aseptic techniques were maintained throughout the process. Sterilized 500 mL high-density polyethylene (HDPE) bottles, known for their durability and non-reactivity, were used for microbial water sampling. To prevent external contamination, bottles were tightly sealed immediately after collection, labeled, and placed in a cooler box stored at 4°C. Disposable gloves were worn, changing them between samples and handled bottles carefully to avoid direct contact. Samples were then transported to the Department of Environmental Engineering Labs at Copperbelt University, Zambia, for microbial analysis within 6 hours of collection. In the laboratory, work surfaces were thoroughly disinfected before and after processing and all analyses were conducted using sterile equipment to further ensure the reliability of results.
Laboratory Analysis
The water samples collected from the point of use were analyzed for total coliforms and E. coli using standard methods of membrane filtration technique. 50 The filtration apparatus was set up, including a filter holder, a membrane filter and a vacuum pump. A sterile membrane filter with a pore size of 0.45 μm was used to target the microbes. A 100 mL volume water sample was poured through a membrane filter using a vacuum to draw the sample through. Coliform bacteria were retained on the surface of the membrane. The membrane filter was then placed on the selective growth medium using a pair of forceps. M-Endo Agar was used for total coliform and incubated at 35°C to 37°C for 24 hours and HiChrome for E. coli was used and incubated at 35°C for 24 hours.
After incubation at the set time, the Petri dishes were removed from the incubator and examined for bacteria colony growth and the colonies that formed on the membrane were counted using a colony counter. Total Coliform colonies typically appeared as red or pink colonies with a metallic sheen on M-Endo Agar and E. coli appeared blue on HiChrome. The total bacterial count in every 100 mL was reported as Colony Forming Units per 100 mL. 50
Data Collection Tools
To evaluate the reliability of the instrument, a Cronbach’s alpha test was conducted on the pre-tested questionnaire, yielding a value of .715. The reliable instrument was then input into Kobo Toolbox for data collection in the field.
Data Analysis
The study used frequencies and cross-tabulations to assess the socio-economic and water handling characteristics in the IBM Statistical Package for Social Science version 27 and the graphics were done in R software. Binary and multivariable logistic regression analysis were conducted to identify factors associated with microbial contamination of drinking water. Crude odds ratios (OR) and adjusted odds ratios (AOR) were used to interpret the results of the logistic regression. The analysis aimed to determine whether any of the independent variables had an influence on microbial water quality. The multicollinearity among independent variables was checked using Variance Inflation Factor values before undertaking the regression analysis. The fitness of the bivariate and multivariable logistic regression model was checked using the Hosmer-Lemeshow statistics and log-likelihood ratio P-value, respectively.
Results and Discussion
Household Socio-Economic Factors
The study included 215 households, with the majority being female-headed (65.1%). Household sizes were mainly 6 to 10 members (49.3%). Nearly half (48.4%) had low monthly incomes (USD 3.80-USD 19.00), while 43.7% earned between USD 22.80 and USD 38. Education levels varied, with 42.8% completing primary school, 29.3% secondary and only 4.2% reaching tertiary education, while 23.7% had no formal education (Table 1).
Summary of household socio-economic factors.

The average exchange rate was 1 USD = 26.269 Zambian Kwacha (ZMW), 2024.
Water Quality Parameters
The physicochemical and biological parameters of the water samples collected at the source and point of use are presented in Table 2.
Physicochemical and biological parameters in point of use and source water samples.
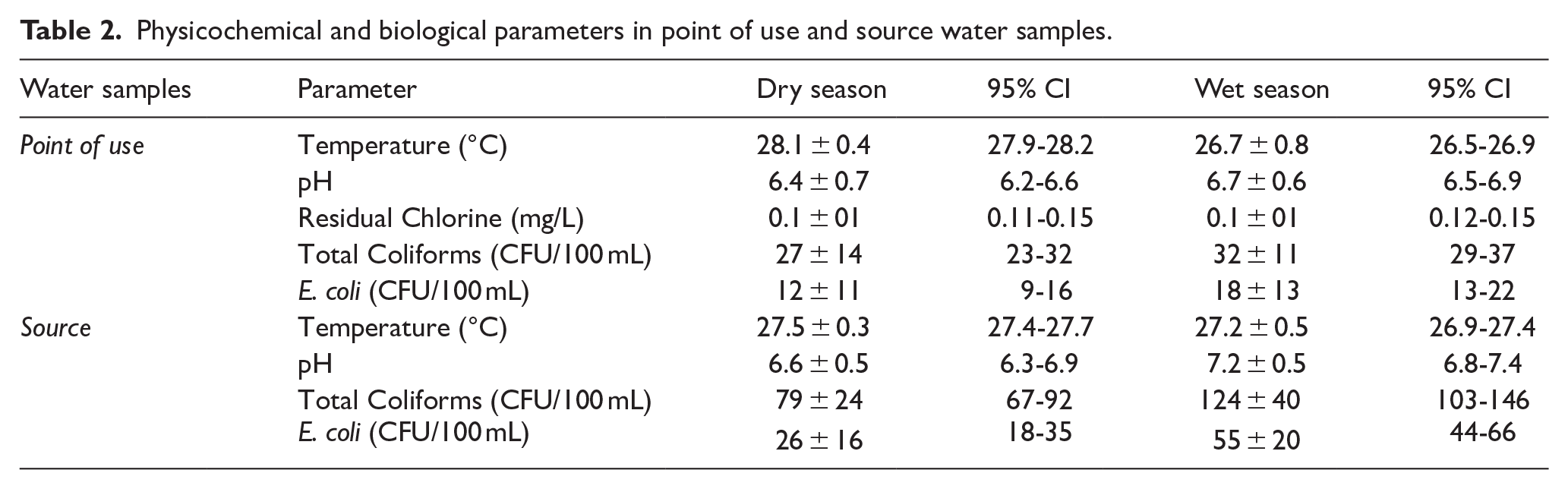
The mean temperature of water samples at the point of use was 28.1°C during the dry season and 26.7°C during the wet season (Table 2). The average pH levels were 6.4 in the dry season and 6.7 in the wet season, both of which fell within the WHO guideline range for drinking water (6.5-8.5). Residual chlorine levels were consistently low across both seasons, with a mean concentration of 0.1 mg/L. In the dry season, 68% of stored water samples had residual free chlorine levels below 0.2 mg/L, while in the wet season, this proportion increased to 75.3%. The WHO recommends a residual chlorine level between 0.2 and 0.5 mg/L. The low levels recorded among households are insufficient to effectively prevent microbial contamination. During the dry season, the mean E. coli counts were 26 CFU/100 mL at the source and 12 CFU/100 mL at the point of use. During the wet season, E. coli levels increased, with 55 CFU/100 mL at the source and 18 CFU/100 mL at the point of use. Both seasonal values exceeded the WHO guideline, which recommends the absence of detectable coliforms or E. coli in drinking water.
Seasonal Variation of Microbial Water Quality at the Point of Use
The results showed that 61.3% of household water samples were contaminated with E. coli during the dry season, increasing to 77.3% in the wet season (Figure 2). A Wilcoxon signed-rank test revealed a significant seasonal variation in microbial contamination, with total coliforms (Z = −8.061, P = .001) and E. coli (Z = −6.582, P = .001) both showing higher levels in the wet season.

Point of use water samples contaminated with E. coli.
Relationship Between Physicochemical Parameters and Microbial Water Quality
Spearman correlation analysis revealed significant relationships between physicochemical characteristics and microbial contamination in household water. During the dry season, water temperature showed a moderate positive correlation with E. coli (r = .52, P = .001) and total coliforms (r = .43, P = .003), suggesting that higher temperatures may favor microbial growth through enhanced metabolic activity and prolonged bacterial survival. In the wet season, temperature showed weak and non-significant correlations with E. coli (r = .22, P = .173) and total coliforms (r = .231, P = .132). Similarly, pH had a strong positive correlation with E. coli in the dry season (r = .69, P = .001). Residual chlorine revealed a moderate and statistically significant negative correlation with E. coli in both seasons (r = −.42, P = .004), underscoring its important role in reducing microbial contamination in household water (Figure 3).

Relationship between physicochemical parameters and E. coli (upper panel (a), (b), (c)) and total coliforms (lower panel (d), (e), (f)) at the point of use during the dry and wet seasons.
Socio-Economic Factors Associated With E. coli Contamination in Stored Drinking Water
The results showed significant associations between household size, monthly income and the education level of the household head with E. coli contamination in household drinking water (Table 3). Household size was significantly associated with microbial water quality (P = .001). Households with 6 to 10 members recorded higher E. coli contamination (70.4%) compared to smaller households with 1 to 5 members (29.6%). Based on the multivariable logistic regression results, smaller family sizes (1-5 members) were associated with lower odds of contamination (AOR 0.076; 95% CI: 0.006-1.001, P = .05) compared to households with 6 to 10 members.
Multivariable analysis of socio-economic factors associated with E. coli in household drinking water.

Abbreviations: 95% CI, 95% confidence interval; AOR, adjusted odds ratio; COR, crude odds ratio; Hosmer and Lemeshow P value = .7 indicating the model fits well; 1, reference category.
Statistically significant.
Education level was another key factor influencing microbial water quality (P = .008). Households with no formal education had the highest E. coli contamination (51.9%), while those with tertiary education recorded the lowest contamination rates (3.7%). The multivariable logistic regression results further reinforced this trend, showing that individuals with tertiary education had significantly lower odds of water contamination (AOR = 0.009; 95% CI: 0.000-0.545, P = .025) compared to those with no formal education. Similarly, household income was found to be associated with E. coli contamination (P = .001). The highest contamination rates (66.7%) were observed among households with incomes between USD 3.8 and USD 19, while those earning above USD 38 had the lowest contamination rate (7.4%). The multivariable logistic regression results showed that households earning over USD 38 showed a significantly lower adjusted odds ratio (AOR = 0.019; 95% CI: 0.001-0.534, P = .020) compared to households with lower incomes of USD 3.8 and USD 19.
Water Handling Practices
Among the 215 households, plastic buckets (59.5%) and plastic containers (40.5%) were the most commonly used methods for storing water. Over half (56.7%) of households cleaned storage containers with water only, while 38.1% used soap and water. Water was mainly accessed by dipping with a cup (59.5%), and 61.9% stored water for more than 24 hours. Regarding sanitation and hygiene, most households (92.1%) relied on pit latrines, while a smaller proportion (7.9%) had access to ventilated pit latrines (Table 4).
Summary of water-related factors.

Water Handling Practices Associated With E. coli Contamination in Stored Drinking Water
Water handling practices were associated with the presence of E. coli in household drinking water (Table 5). The odds of contamination were significantly higher during the wet season, with households having 8.726 times greater odds of E. coli presence compared to the dry season (AOR = 8.726; 95% CI: 1.450-52.515, P = .018). After adjusting for other variables, narrow-mouthed storage containers were associated with significantly lower odds of contamination (AOR = 0.090; 95% CI: 0.014-0.580, P = .011) compared to wide-mouthed storage containers. Covered containers also had reduced odds of contamination compared to uncovered ones (AOR = 0.113; 95% CI: 0.014-0.889, P = .038). The method of water withdrawal was a significant factor, households using the dipping method were over 7 times more likely to have contaminated water compared to those using the pouring method (AOR = 7.245; 95% CI: 1.440-36.447, P = .016). Additionally, the duration of water storage influenced microbial quality, with water stored for more than 24 hours showing higher odds of contamination (AOR = 5.065; CI: 1.850-13.864, P = .002), although this was no longer significant after adjusting for other variables (AOR = 1.375; CI: 0.241-7.855; P = .720). Regarding household water treatment, households that regularly treated their water with chlorine had a significantly lower odds of contamination compared to those who did not (AOR = 0.120; CI: 0.022-0.656; P = .014). Furthermore, maintaining hygiene by hand washing with soap significantly reduced the odds of contamination (AOR = 0.038; CI: 0.005-0.281; P < .001).
Multivariable analysis of water handling practices associated with E. coli in household drinking water during the dry and wet seasons.

Abbreviations: 95% CI, 95% confidence interval; AOR, adjusted odds ratio; COR, crude odds ratio; Hosmer-Lemeshow P-value = .826, indicating a well-fitted model; 1, reference category; HWT, household water treatment; WSC, water storage container.
Statistically significant.
Discussion
Microbial contamination in drinking water at the point of use showed significant deviations from the WHO limit (0 CFU/100 mL). Among the household storage containers sampled, 61.3% and 77.3% were found to be contaminated with E. coli in the dry and wet seasons, respectively. These contamination rates are lower than the 90% reported in Ethiopia 19 but higher than the 56.5% in India. 51
To ensure safe drinking water, WHO recommends water treatment methods that reduce microbial contamination and ensure effective disinfection. 52 Chlorination was the most commonly used water treatment method among households. However, residual chlorine concentrations in household water samples in this study were found to be below the WHO recommended range of 0.2 to 0.5 mg/L. Specifically, 68% of dry season and 75% of wet season water samples had residual chlorine levels below the threshold of 0.2 mg/L, reflecting insufficient disinfection. This proportion was higher than that reported in Panama, where 47% of samples had low chlorine levels 53 but lower than in Ethiopia, where 85% of samples fell below the guideline. 54 Additionally, a negative correlation was observed between residual chlorine levels and E. coli contamination, suggesting that lower chlorine concentrations were associated with higher microbial contamination. This finding aligns with previous studies, which have demonstrated that insufficient residual chlorine levels promote bacterial persistence in stored drinking water.55,56
Temperature was found to be significantly associated with microbial water quality. A moderate positive correlation was observed between temperature and both total coliforms (r = .43) and E. coli (r = .53) during the dry season, suggesting that higher temperatures facilitate bacterial growth and proliferation. This aligns with the findings of Islam et al 57 who reported a similar positive correlation between temperature and E. coli levels in water samples from Bangladesh.
In addition to physicochemical parameters, socio-economic factors and water handling practices were found to be associated with microbial contamination at the point of use. The study revealed that education level was an important predictor of E. coli contamination at the point of use. Household heads with above secondary level education were less likely to have E. coli in their drinking water compared to those with no formal education. This suggests that education plays a critical role in enabling households to adopt better water handling practices or access safer water sources. This is similar to the findings of Mugumya et al 58 and Makokove et al 59 who highlighted that a literate person is more likely to understand health-related issues, including the need to consume safe water and uncontaminated water. Further supporting this, studies by Hasan et al 60 and Yang et al 16 also reported that higher education levels were associated with reduced E. coli contamination in household drinking water. The negative correlation between education and E. coli contamination observed in this study reinforces the notion that enhancing education can lead to improved water quality and safer drinking practices at the household level.
Income was another predictor of E. coli contamination among the studied households, with households earning above USD 38 being associated with a lower odds ratio of E. coli contamination. The results are similar to a study by Hernández-Vásquez et al 61 in Peru who reported that households with higher income were less likely to have E. coli in their drinking water. The role of income in reducing contamination risks can be attributed to improved access to safer water sources and better water handling practices. Previous studies have highlighted the role of income in reducing contamination risks, possibly by enabling access to improved water quality.34,62,63 This trend aligns with broader findings from low and middle-income countries (LMICs), where households in the lowest wealth quintiles are more likely to have E. coli contaminated water compared to the wealthiest households.64,65 The disparities can be attributed to differences in water handling practices and the affordability of safe drinking water.
This study also found that larger household sizes were positively associated with E. coli contamination in drinking water. A family size of 1 to 5 members was 0.076 times less likely to have E. coli in their drinking water compared to a family of 6 to 10 members. This could be due to higher water consumption and handling demands. Larger families may rely more on shared water storage, which can contribute to contamination through handling practices, inadequate storage, or cross-contamination from multiple users. These findings align with those of Ondieki et al 66 who reported a significant influence of household size on the presence of coliforms in household drinking water in Kenya. In contrast, Gebremichael et al 67 found that larger families in Northwest Ethiopia had better access to improved water than smaller families.
The use of wide-mouthed storage containers, such as plastic buckets, was a prevalent practice among the studied households. Wide-mouthed containers increase the risk of contamination due to easier access for dipping utensils and hands into the stored water. In contrast, narrow-mouthed containers help limit contamination by reducing the likelihood of dipping, as they restrict access. Similar observations were reported in a study conducted in Northern India where households utilized wide-mouthed containers for water storage, which provide a large surface area for microbial contamination. 68 Similarly, Ali et al 69 observed comparable results in Ethiopia, highlighting the role of the storage container type in water contamination. In this study, households practicing the dipping method to draw water from the storage container were 7.245 times more likely to have E. coli in their drinking water compared to those using the pouring method. This aligns with findings by Larson et al 70 who reported that the pouring method significantly reduced microbial contamination by minimizing direct contact with the stored water.
Covering water storage containers is generally an important practice that helps reduce the risk of microbial contamination. In this study, households that kept their water storage containers covered showed lower odds of E. coli contamination compared to those that left their containers uncovered. However, this finding contrasts with a study conducted in Thailand, 71 where covered containers were associated with a higher occurrence of E. coli, likely due to contamination introduced during water collection or poor storage hygiene. This suggests that covering alone is not sufficient if other practices are compromised. In addition, household water treatment, particularly chlorination, was found to significantly reduce microbial contamination. Households that consistently treated their water were 0.120 times less likely to have E. coli compared to those that rarely treated it. This is consistent with findings from Nagpur, India 72 where inadequate water treatment left households vulnerable to microbial contamination. Similarly, studies conducted in South Africa, Nigeria and Ethiopia have demonstrated the effectiveness of chlorination in reducing bacterial loads in drinking water.24,38,73
Hand washing with soap was found to be associated with a reduction in E. coli contamination in stored drinking water. Households that regularly washed their hands with soap before handling water showed lower levels of E. coli, which is consistent with previous studies. 74 Proper hand hygiene plays a critical role in preventing the transfer of pathogens, as human hands act as a medium for E. coli contamination, which can then be transferred to drinking water. 75 Studies, such as those by Rifqi et al 76 in Indonesia, have shown that poor handwashing practices in urban slums contribute to high fecal contamination levels on hands, which are then transferred to water storage containers. Similarly, Agensi et al 21 reported that improper handwashing, especially after using the toilet, led to increased bacterial contamination in drinking water in Uganda.
Conclusions and Recommendations
Socio-economic factors and water handling practices are significantly associated with microbial water quality at the household level. In this study, lower income and educational levels were associated with higher contamination levels, indicating that vulnerable populations are at a greater risk. Proper water handling methods, such as using narrow-mouthed containers, covering storage containers, treating water with chlorine and regularly washing hands with soap, were shown to reduce the presence of E. coli. These findings highlight the importance of safe water handling practices in mitigating contamination risks. Additionally, underscores the need for comprehensive public health strategies that promote awareness of proper water handling, effective storage practices, and hygiene. Given these findings, we recommend implementing interventions to promote safer water handling practices and address socio-economic disparities. Community-based education programs should focus on raising awareness about effective water treatment, proper storage methods and hygiene practices. By improving both behavioral practices and structural support, communities can achieve better water quality and public health outcomes.
Limitations of the Study
The microbes chosen for evaluating microbial contamination in household water are essential for understanding microbial contamination. However, this approach does not encompass all potential pathogens that may pose significant health threats. This limitation highlights the need for a broader range of microorganisms to improve the thoroughness of the study. Additionally, as a cross-sectional study, this research establishes associations between socio-economic factors, water handling practices, and microbial contamination but does not determine causation. Longitudinal studies could offer more insight into causal relationships over time. Future studies may also consider factors such as distance to water sources and local environmental conditions to provide a more comprehensive understanding of microbial contamination.
Footnotes
Acknowledgements
The authors acknowledge the Tropical Disease Research Centre for granting ethical clearance. Special thanks are due to Egerton University, the Copperbelt University and the Zambia National Health Research Authority for their institutional support throughout the study. We are deeply grateful to all the study participants for their cooperation and kindness during data collection. Finally, we thank the reviewers for their valuable feedback and insights.
Ethical Consideration
The questionnaire and the study protocol were approved by the Ethics Committee of Egerton University EUISERC/APP/364/2024 and the Ethics Committee of the Tropical Diseases Research Centre TDREC237/10/24. Authorization to conduct the study was granted by the Zambia National Health Research Council NHRA-1612/05/10/2024 and the Zambia Provincial District Health Office.
Consent to Participate
Before participation, consent was obtained from all respondents, who were fully informed about the purpose of the study.
Author Contributions
SN, GMO, EM, and JN collaboratively conceived and designed the experiments. Data collection was conducted by SN and JN, while supervision was provided by GMO, EM, and JN. All authors contributed to data interpretation, manuscript drafting, and revisions. The final version of the manuscript was developed through a collective effort, with all authors actively participating in the revision process and reaching a mutual agreement on its submission.
Funding
The author(s) disclose receipt of financial support for the research, authorship, and/or publication of this article: This research was funded by the Inter-University Council for East Africa (IUCEA).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in the study are available upon request from the corresponding author.