
Abstract
Carrying out health research with schools can be both challenging and highly rewarding. Here we describe lessons learned from a research partnership lasting over 5 years, initially with 84 primary schools in London and Luton, and extended to 35 secondary schools, during our children health cohort study. This period included school closures and societal disruption during the COVID-19 pandemic, creating additional challenges to ongoing school participation. Our study involved annual health assessment visits to schools to test over 3000 participants and parental self-report questionnaires, to assess the potential benefits of air quality improvements arising from London Ultra Low Emission Zone (introduced in April 2019) on children’s lung development and health. Measures included height, weight, pre- and post- bronchodilator spirometry, physical activity monitoring, cognitive assessment, epigenetic markers of disease risk, SARS-CoV-2 IgE and IgM antibody testing, and heavy metals testing. The average annual participant attrition for our study was 11.6%. The acceptable threshold outlined in the initial protocol was 20%. All schools continued to participate in the study for 5 years. Central to the study success have been: shared agreement on the importance of the research topic; early preparatory work with stakeholders, a parallel engaging and innovative air pollution learning and outreach programme, incentivising school/teacher co-operation and parental questionnaire completion to boost response rates and mitigate non-response bias; and continuity of contact with the accessible and flexible research team. These successes form a template for other health research studies planning long-term engagement with schools.
Keywords
Introduction
Meaningful engagement and involvement with participants in public health focused research is widely recognised as being necessary to ensure that research remains relevant, useful and trusted by individuals and communities. 1 Schools are popular settings for conducting health research involving young people, providing both practical and contextual benefit for health investigators. Working with children in schools is socially significant because findings can have both immediate and long-term benefits in the lives of developing children 2 and local communities.3,4
Schools provide large and often diverse groups of children and young people, conveniently stratified by age, who can be easily approached when successful and trusting relationships have been developed between schools and researchers. 5 Schools are a safe place for children, where the majority of parents have trust in the organisation and governance. However, trust between community and researchers cannot always be assumed as “one of the major challenges in conducting health research is the understandable lack of trust that often exists between community members and researchers, based on the long history of research that has had no direct benefit. . .and no feedback of the results to the participants involved.” 6
Furthermore, due to the large number of studies and projects competing for time on a school’s busy schedule, and schools’ overriding priority being the education of their students, many researchers have found it difficult to encourage schools to participate in research projects. 7 Problems are often related to building relationships and communicating, including ensuring that school partners in research feel heard and valued, managing expectations about project progress, and maintaining continuous participation over time, within the highly dynamic school environment. 8
It is therefore important for research teams to build positive and effective relationships with school staff and parents to conduct successful research.5,9 Research considerations need to be combined with a careful examination of the needs of each individual school in order to build a successful recruitment and retention strategy. 7 Furthermore, conducting health research with children in schools can be challenging due to: gaining access from gatekeepers, logistics and planning of successful field days, co-operation of school staff, parental consent and maintaining contact and positive relationships, particularly over extended periods.10,11 Ongoing engagement is vital for success where studies use designs that require repeated measurements over time, particularly cohort studies.
We describe our approach and insights from our research - a 5-year parallel natural experiment cohort study (initially 4 years but extended by 1 year due the COVID-19 pandemic), working with primary and secondary schools in London and Luton from 2018 to 2023 to test if the introduction of the Ultra Low Emission Zone (ULEZ) in London would produce improved lung growth in children. Sub-studies addressed secondary hypotheses on impacts of the ULEZ on physical exercise, obesity and travel behaviours, and cognitive function development. The study is described in detail elsewhere. 12
By adopting a school-centred research approach, our research team were able to initially partner with 84 primary schools across the 2 study sites and through these partnerships acquired individual parental consent for participation of 3414 children from school years 2, 3, and 4 (aged 6-9 years) to take part in the study. With a 1-year extension to the data collection period to compensate for school closures during the COVID pandemic, we extended recruitment to 35 secondary schools to which the older children among our cohort transitioned. Our partnerships allowed us to schedule and carry out over 500 visits to schools to collect annual health data from participating children, including: height and weight measurements, spirometry assessments, physical activity and travel behaviours, and in subsets of children: measurements of cognitive function and mental health, capillary blood sampling for COVID antibodies and heavy metals, and saliva sampling for DNA and epigenetic analyses.
School closures and social distancing restrictions during the COVID-19 pandemic, and especially the 3 national lockdowns that took place between March 2020 and March 2021, presented particular challenges in terms of continuing engagement and retention of schools and undertaking data collection. Carrying out research activities in the form in which they were originally planned became impossible, hence the investigators had to find alternative ways in which to continue engaging children, teachers and parents, to continue data collection, and to prevent schools from dropping out.
The aim of this article is to share the experiences and lessons learnt from conducting public health research with children in school settings from our research study before, during and after the COVID-19 pandemic. Our reflections might be beneficial for teams conducting school-based research with children and young people, and for researchers who are exploring paths to broadening research impacts and enhancing outreach to diverse communities. Building and maintaining positive, flexible and effective relationships with school staff and parents, even during challenging times, is vital. 9
Methodology
Research Planning
Researchers naturally think their research topic is sufficient of itself to lead to a school’s participation, but our experience shows that schools had a range of different considerations as seen in Figure 1.
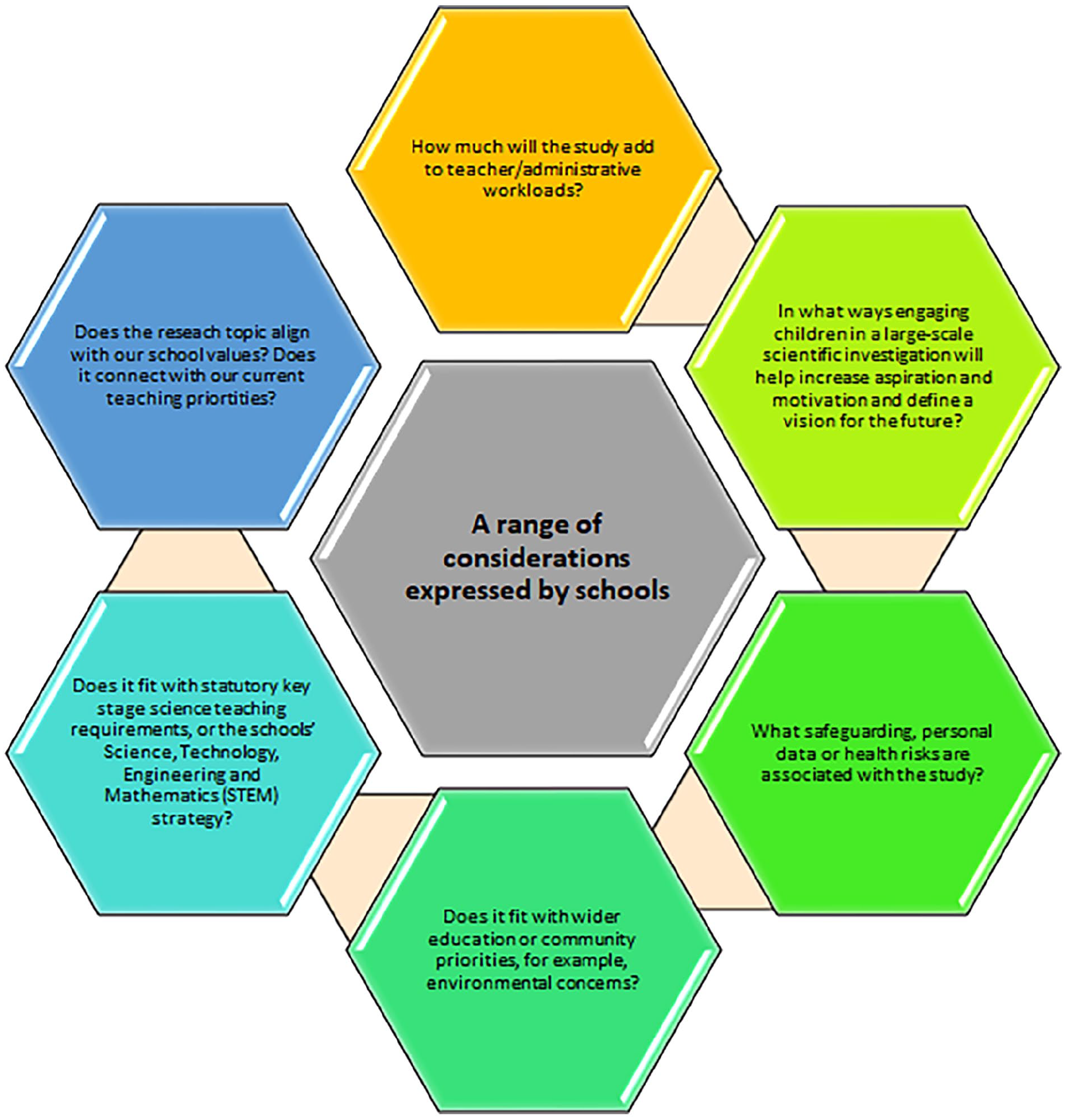
School considerations.
Failure to address these fundamental questions, risks recruitment failure at the outset.
In order to mitigate such risk, our team invested time in preparatory work with head teachers, teachers, parents, and children attending schools in the study target area in central London and Luton. We used an informal approach, obtaining permission from head teachers to speak to parents at the school gates of schools eligible for the study, as they collected their children from school. Recent research provided evidence that air pollution levels in Luton was associated with stunted lung growth in primary school children. 13 . We discussed with teachers the optimal means of giving parents information and securing written informed consent (see Attachment 1) for participation – in this case by sending information sheets and consent forms home in the children’s school bags. Every consent form covered all aspects of the study and was signed by the parent and the child.

Consent form.
By involving them in the research planning phase, where the research topics and agendas are set, research questions and aims are agreed, and study design and materials are designed, our research study team were able to facilitate their needs. 14 The stakeholders reflected on their own experiences with air pollution and brought innovative ideas and logistical support to our research study.
Recruitment of Schools and Children
Considerable data on schools is publicly available on the websites of local authorities and individual schools themselves, enabling researchers to build a picture of the likely numbers of schools and children eligible for a research study.
The 2 pools of schools eligible for recruitment to the study were clearly defined by the study eligibility criteria, in this case state primary schools situated or with catchment areas within the central area of the ULEZ in London (intervention cohort), or within the Borough of Luton (comparison cohort). Schools meeting these criteria were contacted and invited to participate, and meetings arranged with head teachers or their delegates to discuss the study and answer any questions. 12
Appendix 1 provides an example of our study school Participants Information Sheet.
The results of this school-centred approach enabled us to recruit 84 primary schools and 35 secondary schools’ representative of the range of socioeconomic and ethnic profiles of school-aged children across London and Luton.
Recruitment of the school was the first stage in a partnership, the second stage was recruiting children as participants for the research. Parental consent was sought for each child to participate.
In addition to parent information sheet (Appendix 2) and children information sheet (Appendix 3), the team worked with a professional video company to provide a short engaging YouTube video, involving child actors role-playing the elements of the research. A video was easily accessed via links embedded in emails or QR code scanning and easily watched by parents and children together on mobile phones.
Some of the most useful and practical approaches were found to be school assemblies, playground visits at home time, classroom visits, using the schools’ communication systems and social media.
Figure 2 illustrates the approaches that worked for our team during the recruitment process.

Approaches in Recruitment.
Importance of Public Engagement in Recruitment and Retention
Recruitment of schools and children can also be enhanced through the use of public engagement. 11 Using local and national media or local radio to increase publicity and the profile of the research can play a vital role in accessing a broader range of families within the local area; this could also include those families who speak English as an additional language, thus increasing interest and subsequently participation in the research Schools and their communities often work very closely together in various aspects of school life - from knowledge and teaching to parental support and empowerment. Therefore, discussions between these communities plays a role in promoting the study and enabling the study to be recognised.
The team organised a high-profile launch for the study and worked closely with contacts in the Public Health units of local authorities to arrange simultaneous school visits. The mayors of London and Luton were present at the launching of the project. These provided ready images and copy for local print, regional and national TV, and social media, leading to widespread dissemination of the study, further promoting the study to other schools in the study areas.
Ethical and Safe School Visits
Prior to data collection visits, the team ensures an ethical and safe environment for the researchers and the schools involved. Proof of enhanced Disclosure and Barring Service (DBS) checks (as required by the Office for Standards in Education, Children’s Services and Skills (OFSTED) for all study team members visiting schools is a prerequisite for school participation. DBS certificates and work photo IDs were presented upon entry.
Incentives and Science Outreach
Partnering with schools for research is not only beneficial for the research team, but also for the children involved and their schools. Offering incentives for the school plays an important role in collaboration. Based on feedback from participating schools, the incentives were used to purchase sports equipment, build outdoor learning spaces and fund extra-curricular activities.
Giving the children who participated a small stationery item such as a pen, badge or certificate as a “thank you” is very well-received (Appendix 4), making the children feel valued as part of the research and encourages them to participate again in the future. Parents were also incentivised to return their questionnaires annually. They got a £5 supermarket voucher for returning the health questionnaires.
Offering science educational workshops is a useful way to reach children within the school beyond those consenting to the study. Engaging children in disadvantaged areas in science, especially those under-represented in science, technology and Medicine (STEM) professions including women and those from minoritised ethnic groups is especially important. Children readily understand that their environment is polluted and under threat. Engaging them in interactive informative play readily allows them to understand and begin to articulate views and advocate on this topic.
The team partnered with an award-winning public engagement science group to develop and deliver interactive learning and outreach sessions over the course of the study. These were delivered by a Learning and Outreach Officers. They were STEM subject university graduates who were responsible for the delivery of our interactive learning experiences and building community partnerships. They co-ordinated outreach activities that align with educational standards.
The outreach activities were supported by additional leveraged funding. Topics reflected the additional sub-study elements during the course of the study are outlined in Appendix 5.
These outreach sessions were highly attractive to schools and had an important additional effect: retaining schools and children in the study. Comments were almost invariably positive, including for example, from a teacher: “I’ve never seen my children so engaged in a topic.”
Our learning and outreach extended to the wider community and beyond, for example we delivered sessions at local festivals, national initiatives (MRC event, New Scientist LIVE), and leading science bodies.
The School Visits
Figure 3 illustrates the data collection in 3 simple steps:
Step 1. Scheduling Health Assessment Visits
Step 2. Conducting Health Assessment Visits
Step 3. Maintaining Contact with Schools

Data collection in 3 steps.
Sustaining Relationships With Schools and Parents During COVID-19 Pandemic
The COVID-19 pandemic brought unprecedented challenges for society and families. Sudden changes in resources, daily routines and relationships as a result of restrictions on physical interaction resulted in major impacts on families with children. In the absence of school, childcare, extra-curricular activities and family gatherings, children’s social and support networks were severely disrupted. This was particularly evident in families with low levels of social support. 15
The pandemic presented very specific challenges for our research study. Spirometry (blowing into a machine to measure lung function) is a procedure that can generate an aerosol, presenting a potential cross-infection risk. The team had the double challenge of finding a way of visiting schools in a way that was safe for schools and the study team, but also carrying out spirometry safely.
We identified and worked with 4 “pathfinding” schools who helped us to remain in touch with our participants and research partners. Parents, school staff and children were invited to online meetings that helped the team to identify concerns and priorities by listening to honest, helpful and practical suggestions. They were given the opportunity to raise concerns and voice their questions as active contributors to our revised research strategies. These contacts helped to expand the dialogue and acknowledge lived experience. As research on covid transmission dynamics and risk developed, we found ways of minimising risk by carrying out spirometry assessments outdoors under gazebos, and later, in well-ventilated large rooms, using CO2 monitors to give a proxy of fresh air exchange. These approaches were formally co-designed and risk-assessed with stakeholders and respiratory health experts from European Respiratory Society and Public Health England. The team also created interactive science workshop activities that could be accessed by our study participants in their own time. Questionnaires were sent to participants who we could not visit and without a deadline for completion, thus giving families room and time to adjust to their new routines and roles during lockdown.
Retention
Various cohort retention and implementation strategies were adopted. Participating schools were given an annual incentive of £250 for each stage of data collection. Staff members with responsibility for participant contact were provided intensive training and support on study protocols, including retention techniques. In recruiting research staff for our study team applicants were screened for experience, communication skills, cultural-competence, and specialised knowledge of the population (ie, in Luton where a large part of the cohort was of Asian/Asian British origin, researchers with similar ethnic backgrounds were employed. A number of different contact details for participants were recorded and these updated at every participant contact.
20 secondary schools in London with small numbers (<5 children per school) of our cohort participants were identified; The team did not have the resources to visit these schools to carry out health assessments. To retain and gather data on these participants, we ran a health assessment event in central London on 2 consecutive study years (Y4 and Y5). These combined health assessments with science engagement sessions. Centralised testing flyers were sent to participants (Appendix 6). These proved popular and successful and were attended by over 70 children.
Cohort retention issues were discussed through meetings involving research assistants, project managers and principal investigators. During these meetings, the study team examined the latest recruitment and retention rates and discussed strategies and ideas for participants who were difficult to contact.
Table 1 illustrates the challenges encountered by the research team and the measures taken to resolve them.
Research tasks and challenges, measures and outcomes.

Discussion
Recruiting and retaining participants in health research is often challenging, especially in ethnically and culturally diverse populations living in disadvantaged communities. These communities face unique challenges, adversities and inequalities. 16 We presented practical solutions that have helped to recruit and retain schools and participants over a 5-year period, as an exemplar for future longitudinal studies in school-aged children.
Engaging everyone involved in the research (school staff, parents, children, local council members etc.) at the earliest possible opportunity, helped the research team to make informed decisions about the research process and make some practical changes. Benefits included getting input on research activities, developing culturally sensitive approaches and enhancing the recruitment and retention of research participants. 17 Stakeholder engagement is a powerful vehicle for effectuating changes that can improve health. 18 . Engaging community health stakeholders in the research process is often the missing link to improving the quality and outcomes of health promotion activities, disease prevention initiatives, and research studies. 19
Maintaining stakeholder engagement for the full duration of the study is a long-term process that requires time and effort from all sides. It builds trust, values all stakeholders’ contributions, and generates a collaborative framework. 20
Children and young people are viewed as active contributors in the project, rather than objects of research. 21 Adopting involvement strategies such as learning and outreach sessions, that play to children’s competencies and strengths is vital. Engagement of children and young people requires the use of creative, participatory methods, tools and involvement techniques to reveal children’s abilities. Participating children learned about lung function by exploring lung props, making slime, building green walls with plants, drawing with charcoal and performing breathing exercises with straws and feathers. Attachment 2 is an excerpt of our workshop brochures. Research is often planned and described in emotionally “neutral” terms, although participatory research necessarily relies on building relationships and engaging emotionally in a research process with others. 22 Embedding the enjoyment of interactive learning about the main topic of the study within the participatory research process, was an essential part of the project. Learning and outreach sessions for the children on the study health assessment days were a major component of our recruitment and retention strategy, reinforcing the positive relationships between researchers, children, and the schools. Although many funders do not see this as a fundamental part of research which often results less financial support, it plays a key role in the study experience. Children are inquisitive by nature, therefore introducing research and workshop-based activities into their typical school day is exciting for them and makes full use of their inquisitive nature. Curiosity is a powerful driver of learning. 23 Additionally, in educational settings, curiosity for scientific knowledge is a major motivation for long-term involvement in STEM subjects and predicts academic performance.24,25 Furthermore, science education policy documents worldwide highlight the importance of scientific literacy and suggest it is essential that pupils develop their understanding about the processes of science and the type of knowledge science produces and have the ability to apply this in everyday contexts. 26

“Pollution solution” workshop activity.
One of the often-cited criticisms of health research is its lack of pragmatism, frequently addressing questions and outcomes of limited relevance to the end-users. This means a significant proportion of health research is potentially wasted from the outset, because researchers have not consulted with end users when prioritising an area of research or selecting a specific research question. 27 Building trust between investigators and community members is vital and could enhance protocol development and implementation.28,29 Engaging the community can improve the quality, validity, and relevance of research findings, and it can empower community members to advocate for programme and policy changes that may be indicated as a result of the research. 17
Implications for Practice
The lessons learned from our research team during the 5-year study period appear to have enabled us to maintain 84 primary schools’ interests, expand successfully into 35 secondary schools and keep all schools on board for the whole study, including during the pandemic. The team’s tailored approach, flexibility and engagement have been vital to secure their continuous engagement with the project. Our learning journey could enable more clinical researchers to study children’s health in school settings. The combination of recruitment and retention strategies outlined in this manuscript form a working template for other health studies planning long-term engagement with schools.
Implications for Policy
The tangible benefits from this study include: (A) Creating valuable educational and health promotion opportunities in areas of high deprivation where fewer resources and opportunities are available, (B) Inform policy discussion and improve decisions leading to better air quality, health, and wellbeing. Our efforts align with the Framework for Action developed by WHO that aims to enhance the ongoing work in the health and education sectors and to contribute to the achievement of other global commitments for child health. Successful partnerships in health research offer schools, parents, teachers, communities, and other stakeholders opportunities to build healthier lives and add to the creation of global standards for health promoting schools.
Supplemental Material
sj-docx-1-ehi-10.1177_11786302251328831 – Supplemental material for Collaborating With Schools for Public Health Research in England: Lessons Learned for Successful Partnerships
Supplemental material, sj-docx-1-ehi-10.1177_11786302251328831 for Collaborating With Schools for Public Health Research in England: Lessons Learned for Successful Partnerships by Ivelina Tsocheva, Jasmine Chavda, James Scales, Rosamund Dove, Harpal Kalsi, Helen E Wood, Grainne Colligan, Louise Cross, Luke Sartori, Jessica Moon, Aisling Murray, Sarah Van Den Berg, Alice Hirst, Jessica Mitchell, Jason Le, Frances Balkwill, Kristian Petrovic, Esther Lie, Mia Keating, Britzer Vincent Paul Raj, Pavani Kotala, Gurch Randhawa, Ian S Mudway and Chris Griffiths in Environmental Health Insights
Footnotes
Appendix
Acknowledgements
We are expressing our gratitude to all participating schools, parents and children for their enthusiasm and continued support.
Author Contribution
Ivelina Tsocheva, Jasmine Chavda, James Scales, Rosamund Dove, Harpal Kalsi, Louise Cross, and Helen E. Wood contributed to the manuscript equally. All authors reviewed the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CHILL study was supported by the National Institute of Health Research Public Health Research (grant number 16/139/09) with additional funding by the Medical Research Council (grant number MC UU 00006/5).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.