
Abstract
Background:
The public health risk of microbial contamination of fomites is evident from the numerous fomite-associated outbreaks that have occurred in several countries. Despite the high-touch nature of door handles across various settings, no comprehensive synthesis of contamination rates and microbial profiles has been performed.
Aim:
The aim of this work was to assess the prevalence and types of microbial contamination on door handles in public and healthcare settings.
Methods:
We systematically searched PubMed, Web of Science, and Scopus for studies published up to July 2024. A systematic review and meta-analysis were conducted according to the PRISMA guidelines. Pooled prevalence estimates were calculated via a random-effects model, and subgroup analyses were performed to assess differences on the basis of pathogen type, handle location, and setting.
Results:
A total of 27 studies met the eligibility criteria. The overall estimation of microbial contamination of door handles revealed a prevalence of 9.96% (95% CI: 5.87‒14.11). Compared with viral contamination which was observed to be 17.73% (95% CI: 9.24‒27.81), bacterial contamination was less common at 6.20% (95% CI: 2.90‒10.42). The most predominant bacterial agent was Bacillus spp. (55.74%), followed by Acinetobacter baumannii (25.00%); the most prevalent virus was rotavirus (62.50%). The rate of contamination was higher for toilet door handles (23.04%) than for other public and healthcare handles (7.75%). Hospitals presented slightly higher contamination rates (10.82%) than did public settings (8.97%).
Conclusion:
This systematic review highlights the widespread microbial contamination of door handles, particularly in public and healthcare environments. While bacterial contamination is predominant, the finding of viruses such as rotavirus, norovirus and even SARS-CoV-2 highlights the stringency of cleaning that has to be applied. These findings emphasise the need for targeted hygiene interventions to reduce the risk of pathogen transmission via door handles, particularly in high-traffic areas.
Introduction
The risk of contracting infectious diseases from microbial contamination of high-touch surfaces such as door handles is a significant public health concern because of the numerous fomite-associated outbreaks, including human parainfluenza virus 1 (HPIV1) and norovirus that have occurred in several countries.1,2 Fomites, also known as fomes, were first understood to be “seeds of disease,” carried by diseased people and disseminated by indirect human contact over great distances. 3 This idea dates back to 1500s. Currently, a fomite is essentially any inanimate object that might spread disease-causing agents to a new human host when it becomes contaminated with infectious organisms. 4 Since most people in industrialised nations spend 90% of their time indoors, the built environment and objects that people commonly come into direct contact with, such as doorknobs, tend to be the most significant sources of contamination and transmission. 5 Door handles, especially those in public places and healthcare settings, are particularly susceptible to contamination because of their frequent use and the diversity of microorganisms introduced by users.6,7 This presents a serious challenge for infection control, particularly in hospitals where nosocomial infections (NIs) pose life-threatening risks to patients and healthcare workers, 6 as they account for approximately 7% and 10% of all infections, 2 in developed and developing countries, respectively. 8 In developed countries such as the United States, approximately 2 million patients acquire nosocomial infections every year, and at least 90 000 of them die. 9
Hospital-acquired infections can be caused by bacteria, viruses, or fungi; however, 90% of the time, bacteria are the primary cause. 10 The most well-known bacteria are Gram-negative bacilli and Gram-positive cocci, while the main fungal causes of NIs include Aspergillus spp., Candida albicans, and Cryptococcus neoformans. The rate at which fomites become contaminated is influenced by various factors, such as moisture content, contact frequency, the ability of pathogens to form biofilms and environmental cleanliness.2,11 -13 This is particularly true in healthcare environments where routine cleaning practices may be insufficient and where the presence of pathogens such as Clostridium difficile, Acinetobacter baumannii, and vancomycin-resistant enterococci (VREs) can result in severe health outcomes for immunocompromised individuals. 14 In healthcare facilities, door handles in toilets and other rooms have been identified as major sources of microbial contamination, facilitating the transmission of pathogens such as Staphylococcus aureus, Escherichia coli, and even viruses such as SARS-CoV-2.15 -17 These surfaces act as reservoirs for pathogens that may be deposited by individuals who carry microbial flora from various locations or from contact with other contaminated surfaces. The contamination of door handles thus serves as a critical point of contact for the spread of hospital-acquired infections (HAIs), which continue to be a major concern worldwide.
Fomites are also a recognised pathway for community-acquired infections. Public areas such as schools, offices, restaurants, and transportation hubs experience large volumes of human traffic, which increases the likelihood of microbial contamination of door handles and other frequently touched surfaces.18,19 Studies have also shown that bacteria and viruses can persist on surfaces for varying lengths of time, increasing the risk of transmission. 20
Despite an improved appreciation of the role that fomites play in disease transmission, the microbial ecology of door handles is not well defined across different setting. Although existing studies report a range of contamination rates and microbial species, no systematic review has synthesised these findings into a cohesive analysis. This review, therefore, aimed to assess the prevalence and types of microbial contamination on door handles in public and healthcare settings.
Methodology
Search Strategy
The systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 21 The search process, conducted between September 22nd and 27th, 2024, involved an extensive exploration of electronic databases, including PubMed, Web of Science, and Scopus, covering studies published up to July 2024. To ensure a comprehensive search, we used a combination of terms related to microbial contamination, including “microbial contamination,” “bacterial contamination,” “viral contamination,” and “fungal contamination,” paired with terms associated with fomites such as “door handle,” “door knob,” “door latch,” and “fomites.” The search strategy was constructed as follows: (“microbial contamination” OR “bacterial contamination” OR “viral contamination” OR “fungal contamination”) AND (“door handle” OR “door knob” OR “door latch” OR “fomites”). Only studies published in English were included. No restrictions were applied on the basis of the study design, allowing for the inclusion of observational studies, experimental studies, and case reports. Citations of relevant studies and similar articles suggested by PubMed were also screened to ensure completeness. Gray literature was not included. The selection process was documented and illustrated via a PRISMA-P flow diagram.
Study Selection
All records obtained from searches were imported into Rayyan software. 22 Two reviewers independently screened the records according to predefined eligibility criteria. On the basis of the research keywords, we included studies that provided both qualitative and quantitative data on microbial contamination of door handles and other fomites. The studies included were cross-sectional, longitudinal, prospective, and outbreak studies. For the outbreak studies, we considered only those in which samples were collected from door handles and reported on the organisms recovered from these surfaces. In these cases, only the data related to fomite (door handle) contamination were included in the review. We included only articles that were accessible to us in full text and published in English. Studies were also included if they reported contamination of door handles by specific groups of microorganisms, such as bacteria, viruses, or fungi. The publications excluded from the review included reports, case-control studies, commentaries, letters to editors, and review articles. Textbooks were also excluded. Additionally, studies that did not specify the sample size for the door handles swabbed or did not report the number of positive samples were excluded. Preprints were also excluded from the review. Additionally, studies focusing on pathogens not associated with fomites or those not specifically related to door handle contamination were excluded to maintain relevance to the research focus. The Zotero reference management tool (Version 6.0.30, Corporate for Digital Scholarship) was used to organise and download full-text articles. Any discrepancies between the 2 reviewers were referred to 2 senior authors (E.S.D and P.B.T.Q) for resolution.
Data Extraction
Data extraction was carried out independently by 2 reviewers, P.O.A and A.O, via a standardised form created in Microsoft Excel 2013 software. The key data points extracted from each study included citation, fomite type, site of study, methods of organism isolation, number samples of collected and number of isolates, sampling method, organism identification method, dilution factor, genes targeted, media and broth used, incubation conditions, country, biofilm phenotype, and median viral load or colony-forming units (CFUs). The percentages were converted to whole numbers for consistency. For studies reporting multiple bacterial isolates, data from individual isolates were extracted. This allowed us to aggregate data across studies, regardless of whether they focused on a single pathogen or multiple isolates within a group of microorganisms, to provide a comprehensive assessment of microbial contamination. Any discrepancies during extraction were resolved through discussion or consultation with senior authors (E.S.D and P.B.T.Q). All the data were systematically stored in a central database for analysis.
Quality Assessment
The quality of the included studies was evaluated via the 18-item Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist. 23 This assessment was conducted independently by 2 researchers (E.S.D and F.C.N.K), and any disagreements were resolved through discussion. The key criteria from the STROBE checklist used for the quality assessment included the following: title and abstract (clarity in the introduction, background/rationale, and stated objectives), methods (study design, setting, participants, variables, data sources/measurement, potential biases, study size, and statistical methods used), results: (descriptive data, outcome data, and how they were presented), discussion (key results, interpretation, limitations, and generalisability of findings), and other information (funding). The quality scores of the studies ranged from 8 to 14, with most studies demonstrating solid methodological rigor in areas such as study design and data reporting (Supplemental Table S2). Discrepancies in scoring were resolved by consensus between the reviewers.
Statistical Analyses
Statistical analyses were performed using R version 4.3.3 and relevant packages, including “meta” and “metafor,” to generate plots and conduct random effects meta-regression for subgroups. Statistical significance was set at P < .05. A meta-analysis was conducted using data at Supplemental Table 3 to pool contamination data from the eligible studies. A random effects model was used to calculate pooled prevalence estimates along with 95% confidence intervals (CIs). Heterogeneity between studies was assessed via the I2 statistic, with values greater than 50% indicating significant heterogeneity. Subgroup analyses stratified the pooled estimates according to the location of sampling (public vs healthcare settings). Publication bias was determined through funnel plot inspection for asymmetry and Egger’s regression test. Sensitivity analysis was used to evaluate the robustness of the results through the sequential omission of single studies.
Results
Search Result
The initial literature search of all 3 databases yielded a total of 2098 different studies. After removing duplicates, 1399 unique articles were screened for eligibility. A total of 1207 studies were excluded at this stage because they did not meet the inclusion criteria on the basis of their title and abstracts. Following the title and abstract screening, the full texts of the remaining 192 studies were retrieved, of which 141 studies were excluded for the following reasons: 8 were conference abstracts, 31 had poor representativeness of outcomes, 50 were not specific to the topic, 23 provided inadequate information relevant to the study’s objectives, and 29 did not specify the sample size for the door handles swabbed or did not report the number of positive samples. After a thorough evaluation of the complete texts from the databases, 16 studies met the eligibility criteria and were included in the systematic review and meta-analysis. Twenty-five similar articles suggested by PubMed through the “similar articles” feature were selected and screened, among which 25 were assessed for eligibility, and 22 were excluded because they provided inadequate information.3 studies were subsequently added to the 16 studies included from the database search, resulting in a total of 19 studies included in this review. These 3 studies were included as they provided specific quantitative data on microbial contamination of door handles, which aligned with the inclusion criteria. This process, from the initial identification of studies to the final selection, is detailed in the PRISMA flow diagram (Figure 1).

A flow diagram of our systematic review process (PRISMA guide).
Study Characteristics
A total of 19 studies were included in this review (Table 1). Twelve of the studies focused specifically on viruses, 6 studies focused on bacteria and 1 study on focused on both bacteria and fungi. Nine of the included studies involved outbreak or post outbreak studies.19,24 -32 All the studies on viruses were conducted during or after the outbreak, with the exceptions of Refs.2,33 which were conducted in office buildings during seasons conducive to respiratory and enteric infection and low (healthcare-associated infections in patients in intensive care units) HIPI incidence years, respectively, to determine the role of fomites in the transmission of respiratory viruses. Most studies focused on bacterial contamination relying on biochemical tests, Gram staining, and colony morphology for organism identification. Notably, Ababneh et al 14 exclusively used PCR to identify Acinetobacter baumannii in hospital door samples. In contrast, viral studies predominantly utilise PCR-based methods, with reverse transcription PCR (RT-PCR) being the most common technique used among the studies. The biochemical tests in one study were conducted via API20 strips according to the manufacturer’s instructions (BioMerieux). 34 Two studies focused specifically on Staphylococcus aureus.18,35 A total of 8 different location types were included, with the majority being from hospitals, 2 from offices and 1 each from a tourist university campus, car, ship or residential building. One study included yeast. 34 None of the studies assessed the longevity or persistence of the pathogens on the dour handle. Only 1 study has determined the viability of viruses. 28
A summary of characteristic features of included studies.
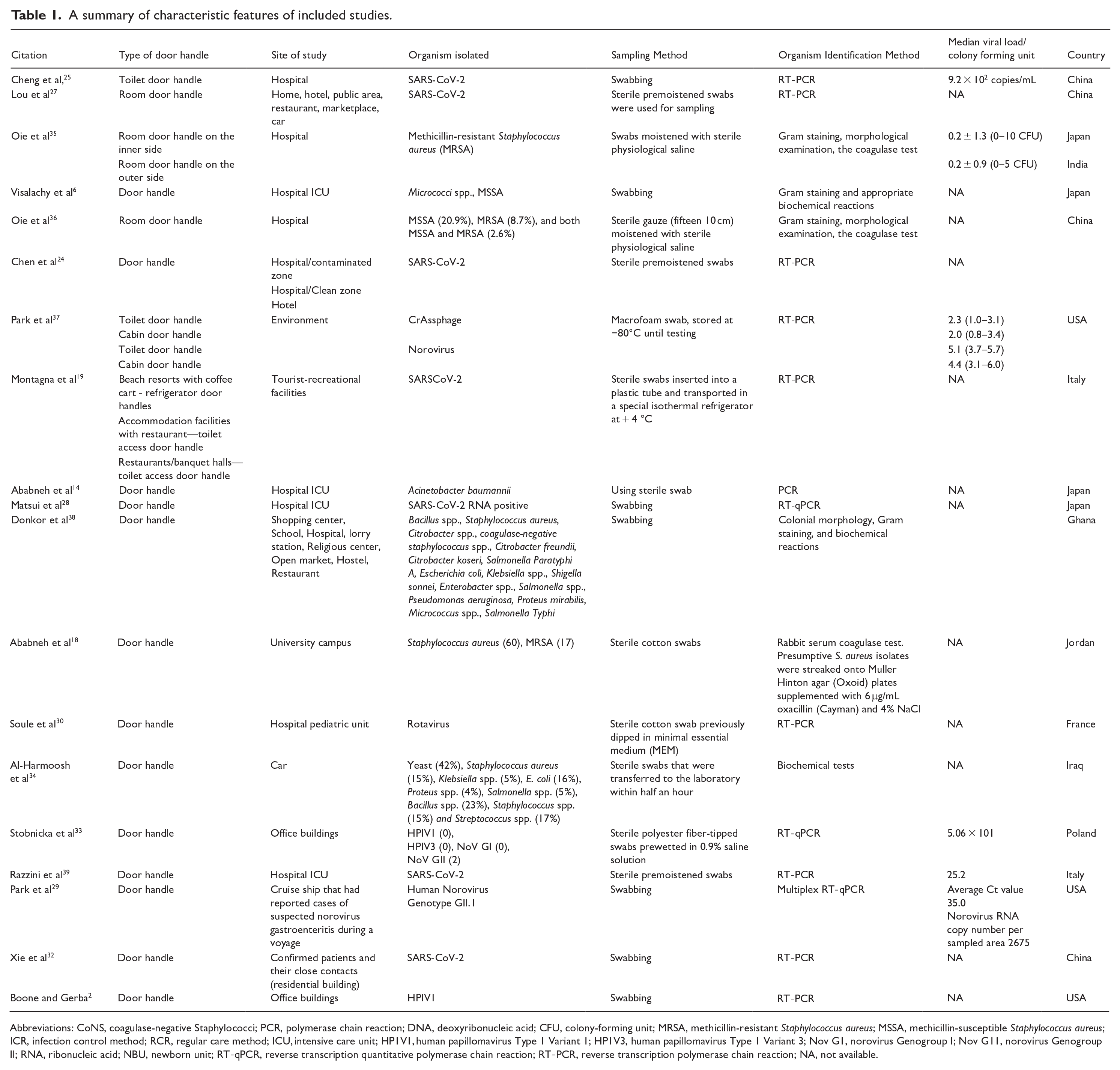
Abbreviations: CoNS, coagulase-negative Staphylococci; PCR, polymerase chain reaction; DNA, deoxyribonucleic acid; CFU, colony-forming unit; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible Staphylococcus aureus; ICR, infection control method; RCR, regular care method; ICU, intensive care unit; HP1V1, human papillomavirus Type 1 Variant 1; HP1V3, human papillomavirus Type 1 Variant 3; Nov G1, norovirus Genogroup I; Nov G11, norovirus Genogroup II; RNA, ribonucleic acid; NBU, newborn unit; RT-qPCR, reverse transcription quantitative polymerase chain reaction; RT-PCR, reverse transcription polymerase chain reaction; NA, not available.
The studies reviewed employed various methodologies to isolate and identify microorganisms from door handles across 14 different countries (Supplemental Table S1). Swabbing was the primary sample collection method used across all studies. Following swab collection, bacterial samples were analysed using culture-based techniques and viral samples were predominantly analysed using molecular method (PCR). The incubation conditions for bacterial cultures typically range from 35°C to 37°C over 18 to 48 hours, whereas viral samples are often stored at −80°C before PCR analysis. Most viral studies, particularly during the COVID-19 pandemic, have been conducted in developed countries, with a focus on target genes such as RNA-dependent RNA polymerase and nucleocapsid protein for SARS-CoV-2. Bacterial studies have shown broader geographical representation and often targeted genes linked to antimicrobial resistance, such as blaOXA in Acinetobacter baumannii.
Meta-analysis
Prevalence of Door Handle Contamination
The pooled analysis revealed that the overall prevalence of microbial contamination on door handles was 9.66% (95% CI: 5.87-14.1; Figure 2). The prevalence of toilet door handle contamination was 23% (95% CI: 7.37-43.72), which was higher than the microbial contamination of other door handles in commercial buildings and restaurant settings, with a contamination rate of 7.75% (95% CI: 4.23-12.0; Figure 3). Further analysis of the setting revealed that the prevalence of microbial contamination of door handles in hospitals was 10.82% (95% CI: 5.60-17.22), whereas that in public facilities was 8.97% (95% CI: 4.36-14.73; Figure 4).

Pooled prevalence of microbial (bacteria, fungi, and virus) contamination of door handle.
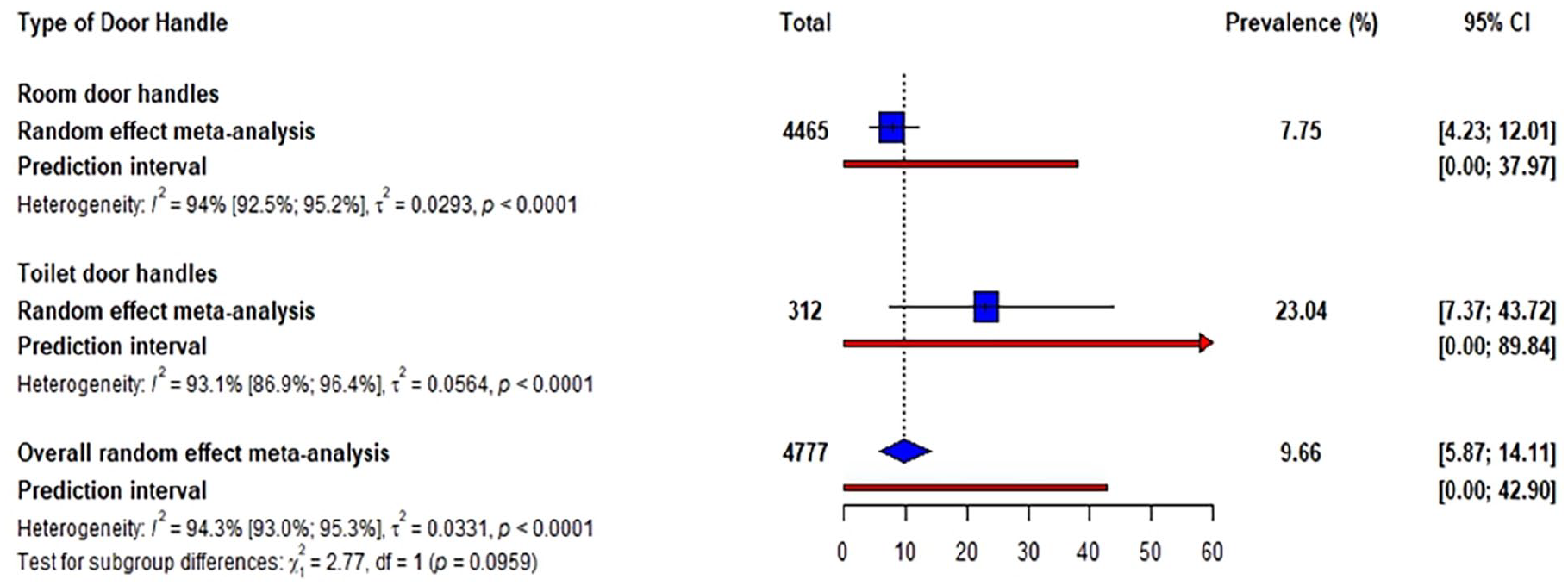
Pooled prevalence of microbial contamination based on the type of door handle (toilet of room door handle).
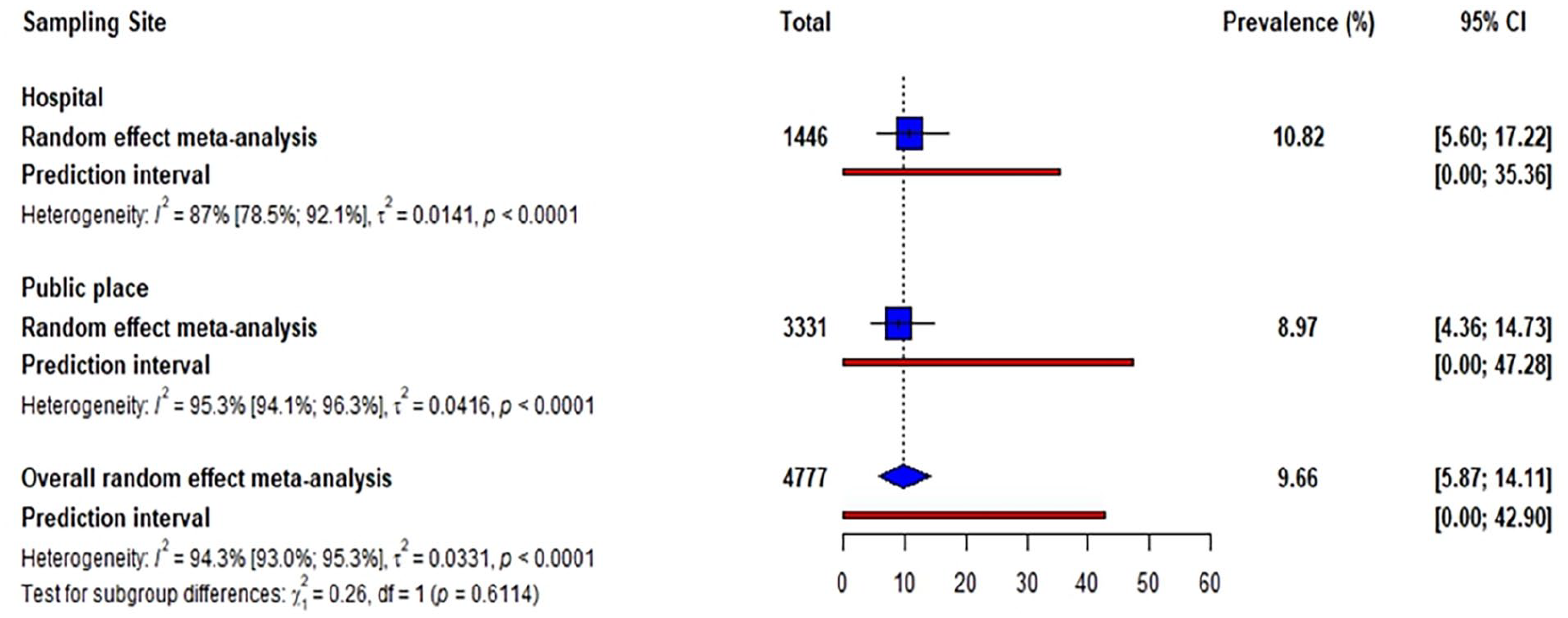
Pooled prevalence of microbial contamination base on location type (Hospital and other public places).
Microbial Contamination Profile
The identified studies reported the isolation of various bacteria and viruses from contaminated door handles (Supplemental Table S3). Pooled data indicated that the prevalence of bacterial contamination was 6.20% (95% CI: 2.90-10.42), which was lower than the prevalence of viral contamination at 17.73% (95% CI: 9.24-27.81; Figure 5). Yeast contamination of door handle of 42% was found in a single study. Subgroup analysis of bacteria revealed that Bacillus had the highest prevalence at 55.74% (48.48-62.88), followed by Acinetobacter baumannii (25%), at (0.00-79.25). Among viruses, rotavirus was the most prevalent, causing 62.50% (25.89-93.28) of viral handle contamination, whereas SARS-CoV-2 was found in 6.75% (3.80-10.29) of door handles (Figure 5).
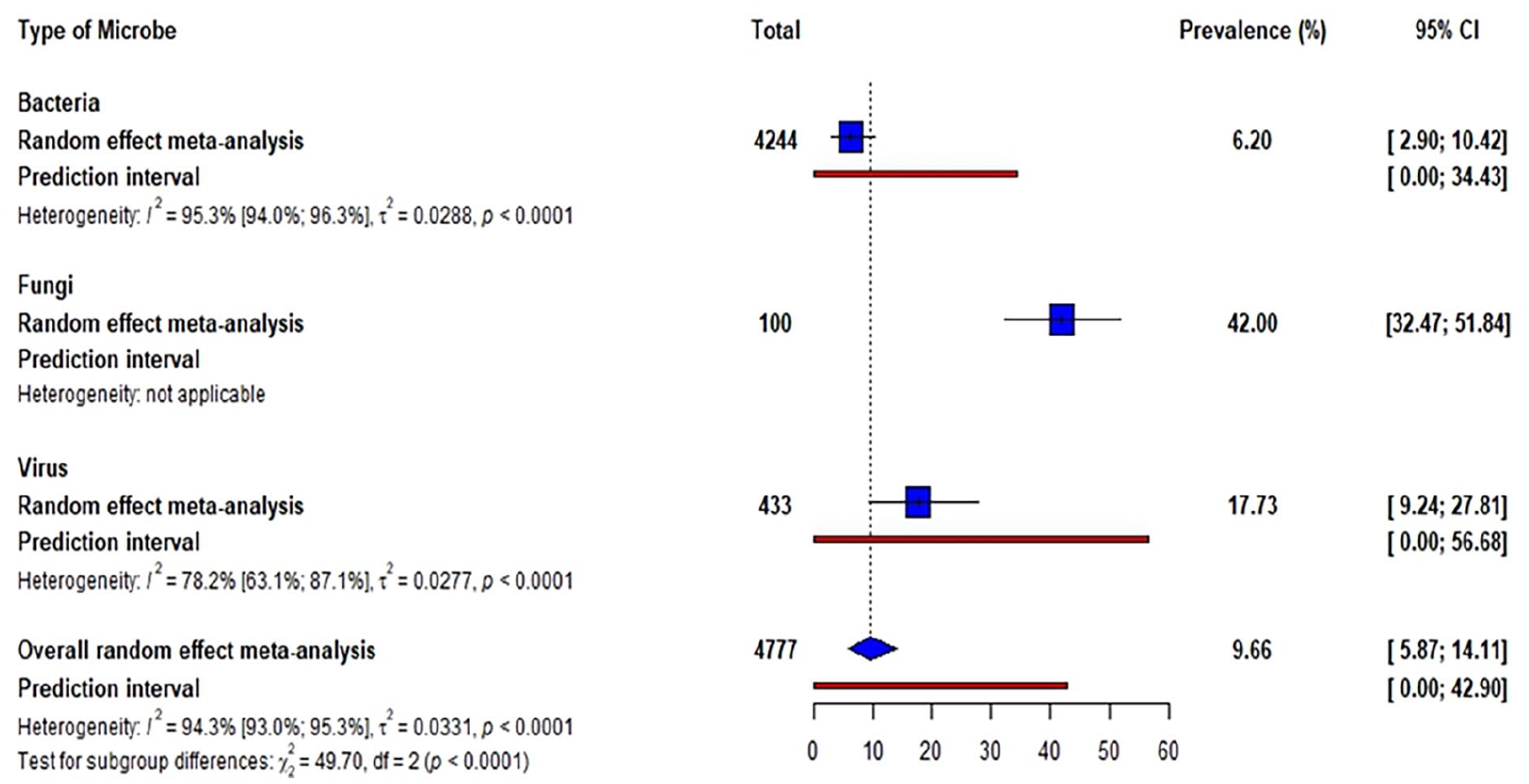
Pooled prevalence of microbial contamination based on the type of microbe (bacteria, fungi, and virus).
Publication Bias
Based on the forest plot (Figure 6), we observed variability in the transformed proportions and standard errors across the studies. The spread of data points and the position of the point estimates relative to the reference line indicate heterogeneity among the results.

Forest plot of studies included in the meta-analysis.
Discussion
Our findings revealed substantial contamination of door handles, with microbial contamination rate of 10.82% in hospitals and 8.97% in public settings; hence, the mean microbial contamination rate was slightly higher in hospital settings than in public spaces. The hospitals are high-contact zones, and the frequent touching of surfaces by healthcare workers, patients, and visitors allows for microbial transfer.40,41 In addition, the presence of susceptible and immunocompromised individuals enables a supportive environment for microbial persistence and transmission.20,42 Although rigorous disinfection is being practiced in hospitals, the presence of multidrug-resistant organisms mostly complicates the efforts to maintain aseptic conditions. These microorganisms have shown to survive on surfaces for extended periods of time, making their contribution to the burden of contamination despite routine cleaning. 10 Lower contamination rates in public settings could reflect differences in the frequency and intensity of surface interactions, as well as environmental conditions such as airflow and ambient temperature, which can contribute to limiting microbial survival.2,43 However, public door handles act as significant reservoirs for community-acquired pathogens and have been related in some instances to inconsistent sanitation practices with hand hygiene.2,44,45
We have observed that toilet door handles consistently exhibit higher contamination rates (23%) in contrast to other door handles (7.75%). According to a study from Baze University, 42.9% of isolates from toilet door handles were identified as Staphylococcus aureus, as well as Escherichia coli and Salmonella typhimurium, indicating significant fecal contamination. 46 This is likely due to their proximity to sources of fecal matter, which increases the likelihood of pathogens such as Escherichia coli and Salmonella spp. being transferred to surfaces. In contrast, other door handles, such as those found in offices or residential areas, tend to be contaminated with environmental or respiratory pathogens. The higher contamination rates on toilet door handles can also be attributed to inconsistent hand hygiene practices post restroom use, highlighting the critical role of effective handwashing and frequent cleaning of high-contact surfaces in mitigating the spread of gastrointestinal pathogens. Hygiene awareness and interventions that specifically target restrooms in public spaces and healthcare settings, where the potential for cross-contamination is especially high, are needed to prevent infection in these settings.
Our meta-analysis result revealed notable differences in contamination rates across various pathogens, providing important insights into the dynamics of microbial contamination on door handles. The relatively low contamination rate of SARS-CoV-2 (6.75%) aligns with the understanding that respiratory viruses such as SARS-CoV-2 may rely more on airborne transmission than on fomite transmission,47,48 although the persistence of viral particles on surfaces still poses some risk, as they can persist and survive on infected surfaces for up to 9 days. 49 On the other hand, rotavirus, crAssphage, and norovirus exhibited a much higher contamination rate on door handles. This may imply that these viruses may have the ability to persist on surfaces ranging from several days to several weeks and cause outbreaks through indirect transmission. For example, norovirus can endure freezing temperatures and resist many common disinfectants, which contributes to its persistence in various environments. 50 This is a significant finding given Norovirus’s role in viral gastroenteritis outbreaks, as norovirus is responsible for almost 90% of viral gastroenteritis cases and almost 50% of all outbreaks worldwide, 51 emphasising the importance of surface cleaning in public and healthcare environments, especially in high-contact areas. Regarding bacteria, the high contamination rates for Bacillus (55.7%), Acinetobacter buamannii (25%), Staphylococcus aureus (17.54%), MSSA (19.2%), MRSA (5.33%), and CoNS (7.10%) are concerning, particularly in hospital settings where these bacteria, especially MRSA, are common causes of healthcare-associated infections.52 -54 This finding is consistent with other studies by Osman et al, 55 highlighting the prevalence of Staphylococcus on high-touch surfaces in hospitals, where the combination of high-traffic and vulnerable patients creates a high-risk environment. In contrast, the relatively lower contamination rates for Gram-negative bacteria such as Salmonella Paratyphi A (3.83), E. coli (2.73%), Klebsiella pneumoniae (2.73%), Shigella sonnei (1.64%), and Salmonella typhi (0.55%)may reflect the fact that these organisms are more frequently associated with fecal contamination,56,57 potentially indicating better hand hygiene practices in certain settings, although the presence of these pathogens still points to lapses in sanitation.
The fact that only 1 study included fungi with a prevalence of 42% in their analysis highlights a significant gap. While fungal pathogens are less prevalent on fomites, they may have grave consequences for immunocompromised individuals, such as hospital patients. Given the severe clinical outcome of fungal infection by fungi such as Candida, which leads to a high mortality rate following infection of vulnerable populations, the rarity of this investigation is surprising. For example, candidaemia is the most common nosocomial bloodstream infection in U.S. hospitals.42,58 It is associated with high morbidity and 25% to 40% all-cause in-hospital mortality. 59 This would therefore indicate that the perceived imbalance in the attention given to bacteria, viruses, and fungi is that bacterial contamination may be more overtly perceived to have a more direct linkage with common infections, whereas insidious infections of viruses and fungi on surfaces might be underestimated.
In fact, the detection of microbial contaminants, particularly antibiotic-resistant contaminants, on door handles in all public and health-related premises requires immediate, effective intervention strategies. Antimicrobial coatings, such as copper-silver alloys, on highly touched surfaces, such as door handles, might reduce the risk of microbial transmission.60 -62 These materials are bactericidal in nature and hence can reduce the possibility of contamination, particularly for those premises that receive unusually high volumes of traffic. The adoption of touchless door mechanisms automatic doors and/or foot-operated handles should also be promoted in the wake of growing acceptance as a useful tool in infection prevention and control.63,64 The frequent cleaning of high-touch surfaces is imperative with the use of EPA-approved disinfectants that are effective against a wide array of pathogens, including norovirus and MRSA.46,65,66 While the use of disinfectants is increasing, their effectiveness depends upon parameters such as pathogen load, concentration, and cleaning frequency. Advanced innovations, including UV irradiation and phage therapy, have been equally effective in removing recalcitrant and resistant pathogens and hence may present good alternatives in addition to the traditional use of disinfectants. 67 Increasing awareness and education on proper hand-washing procedures among staff and the general public are recommended. Hand hygiene stations must be conveniently located at all entrances and exits.
First, the variation in study designs, sampling periods, and targeted organisms could be limitations because different approaches may introduce bias in the performance of the review. For example, studies that were carried out during or after an outbreak overrepresented some pathogens, whereas other works may have focused on a few key microorganisms and excluded other more significant pathogens. The range of pathogen identification methods used in various studies ranges from highly sensitive molecular techniques to traditional, less sensitive methods and influences the rates of detection and range of pathogens identified. Considering these limitations, this review provides relevant information about the prevalence of microbial contamination on door handles and highlights the need for standardised protocols that improve surveillance with a view toward reducing risks associated with high-touch surfaces. Future research should focus on developing universal guidelines for fomite disinfection and pathogen detection to ensure consistent and effective hygiene practices across various settings.
Conclusion
This systematic review and meta-analysis revealed that public and healthcare-associated door handles might serve as key reservoirs of microbial contamination, with a pooled contamination rate of 9.66%. The predominant bacterial pathogens were Bacillus spp. and Acinetobacter baumannii, whereas rotavirus was the most common viral contaminant identified. There is high contamination of toilet door handles; hence, targeting disinfection actions to such high-risk outlets will be paramount. Therefore, routine cleaning, coupled with targeted disinfection and effective hygiene interventions, is essential to reducing the transmission of pathogens via fomites, especially in settings with high human traffic and vulnerable populations.
Supplemental Material
sj-docx-1-ehi-10.1177_11786302251328550 – Supplemental material for Microbial Contamination of Door Handles: A Global Systematic Review and Meta-Analysis of Public and Healthcare Settings
Supplemental material, sj-docx-1-ehi-10.1177_11786302251328550 for Microbial Contamination of Door Handles: A Global Systematic Review and Meta-Analysis of Public and Healthcare Settings by Peter Ofori Appiah, Alex Odoom, Patience B. Tetteh-Quarcoo, Fleischer C. N. Kotey and Eric S. Donkor in Environmental Health Insights
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.