
Abstract
Due to the remoteness of rural areas, the impact of environmental pollution on residents’ health has not received adequate attention. This study examined the relationship between coal consumption and residents’ health status in rural areas in China between 2005 and 2021. We explored the impact of air pollution caused by coal combustion on the health of rural residents in China and provided associated countermeasures. The annual number of medical visits of rural residents was evaluated via multiple regression, and the Pearson correlation and Granger causality tests were used to evaluate the relationships between coal consumption and the changes in mortality rates of various diseases in rural areas. The results revealed that coal consumption for domestic use had a significant (P < .001) positive effect on the frequency of medical treatment, whereas this effect was not significant at the production end. Significant positive correlations existed between coal consumption in rural areas and increased mortality rates for 7 out of the 10 main diseases. Causal relationships were identified between coal consumption and increased mortality rates due to urogenital system diseases and nervous system diseases. The empirical results of this study suggest that the gradual promotion of clean energy replacement of coal with electricity and natural gas in rural areas should reduce the probability of exposure to gas emitted from coal combustion for rural residents. Related diseases in coal-consuming areas should be screened regularly to effectively protect the health and safety of rural residents.
Introduction
The economic and social development of remote rural areas lags behind that of cities because of insufficient investment in medical resources and a lack of health awareness among rural residents. Scholars in all countries have studied the health status of rural residents.1 -5 In traditional agricultural society, a subsistence lifestyle based on individual households in rural areas spontaneously achieves a natural cycle of material and energy, and the pollution emitted during production and domestic activities can be absorbed by nature. Thus, pollution is minimal in rural areas and has relatively little impact on the health of residents. However, since the Industrial Revolution, waste sourced from large-scale industrial production has spread from cities to the countryside.6,7 In addition to the direct pollution generated during production in rural areas, some energy and chemical products produced by urban factories and used by rural residents also contribute to environmental pollution in rural areas. For example, farmers in China widely use fossil fuels such as oil and coal due to their higher thermal efficiency and the fact that they are smaller in size than firewood; however, they also emit poisonous gases that damage the health of rural residents. 8
A large amount of coal is exploited underground annually in China. As a relatively cheap and abundant source of energy, coal is widely used for production and domestic purposes in China’s rural areas. Insufficient coal combustion emits carbon oxide, sulfur dioxide, fluorine particles, black carbon, and other harmful gases. Volatile organic compounds, sulfates, and black carbon directly sourced from coal-burning emissions can be synthesized into PM2.5, which has a significantly negative health impact on humans.9,10 Previous studies have shown that the waste generated by coal burning has a significantly negative effect on residents’ nervous and respiratory systems11 -13 and can also damage their metabolic and reproductive systems.14,15 Therefore, coal combusted in rural areas may threaten the health of residents, especially in developing countries with slow energy-upgrading processes.
Coal has been the primary energy source in China since the middle of the last century. In 2023, it still accounted for 55.3% of energy, although energy-upgrading activities are being rapidly promoted domestically. The World Health Organization estimates that approximately 400 000 people, mainly women and children, die prematurely each year in rural China because of the use of solid fuels, particularly inferior coal containing fluorine or sulfur. In recent years, to control air pollution from coal, residents in rural China have been encouraged to replace solid fuels such as coal and firewood with electricity and natural gas through measures such as banning the sale of inferior coal, constructing pipe facilities for gas, and promoting the use of clean cookstoves.16 -18 Thus, the proportion of coal consumption to total energy consumption in China’s rural areas has declined significantly.
Furthermore, improvements in mechanization in agricultural production have accelerated the modernization of energy consumption in rural areas. More farmers use electricity or petrol to power agricultural machines to cultivate farms as gas lines, and electricity networks have steadily expanded from cities to rural areas. Many peasants can use natural gas, rather than coal or firewood, as the main energy source for heating houses or cooking. However, the process of clean energy replacement still faces some obstacles; for example, traditional coal-exploited regions exist in China, and people in these places customarily use coal; some rural families in the western and northern regions are still very poor, and people in these places are inclined to rely on inexpensive energy such as coal. Natural gas heating is a cleaner mode in winter; however, it cannot be expanded immediately because of its short supply. Thus, Chinese rural residents have used coal as an important energy source for a relatively long time, and the health effects of coal burning on Chinese rural residents require further studies using specific data and scientific estimation approaches.
The rest of this paper is arranged as follows: In the second section, taking most of the provinces in China as the research object, this paper presents the trends in coal consumption for production and domestic purposes in rural areas from 2005 to 2021 and analyses the situation of rural residents’ medical visits. In the third section, the impact of coal consumption on medical visits in rural areas was verified via multiple regression analysis. The causal relationships between coal consumption and disease fatality rates were subsequently tested on the basis of the classified disease fatality data. The fourth section provides a summary of the study and policy recommendations.
The possible contributions of this study are as follows: First, rural coal consumption is innovatively divided into domestic and production ends to study their health effects, which makes the health effects of coal more precise and informative. Second, by combining the results of the Pearson correlation and Granger causality tests on the mortality rates of various diseases and coal consumption in China’s rural areas, the health impact of harmful gases released by coal combustion could be assessed more accurately. The results of this analysis could help establish guidelines to reduce the health damage associated with coal consumption from the source.
Data and Description
Coal consumption in rural areas in China
China covers a vast area. The northern region is located in temperate and alpine plateau climate zones. Thus, winter in this area is cold and long, and heating houses becomes necessary, especially in regions north of the Yellow River (Figure 1). In the past, the use of coal and firewood for heating and cooking was more common in underdeveloped rural areas, and cleaner energy sources such as natural gas and electricity were underutilized due to a lack of energy infrastructure facilities. In 2016, the entire North China region consumed approximately 400 million tons of standard coal for household warming, half of which was consumed by rural residents. 19 Coal-burning emissions constitute the largest source of air pollution in northern China. Although the proportion of coal consumption has decreased gradually as energy consumption upgrades in rural areas have accelerated, the amount of coal consumption remains relatively high, especially in areas rich in coal resources or less developed.

Coal consumption in production (left) and domestic (right) ends (kg/capita) in 2021.
According to data provided by the Chinese State Statistics Bureau, by 2021, the coal consumption levels per capita in rural areas were 49.9 kg for production and 116.5 kg for domestic use (Figure 2). Production-end coal consumption usually occurs in rural kilns, agricultural greenhouse heating, power generation, and metal smelting, which are scattered throughout rural areas. Domestic coal is used in household or village units for boiler heating and cooking on a coal stove. Most domestic heating boilers and coal furnaces are set indoors, and they consume oxygen and release harmful gases such as carbon monoxide, carbon dioxide, sulfur dioxide, fluorine, arsenic, and mercury.

Domestic and production-end coal consumption in Chinese rural areas from 2005 to 2021.
Thus, since the beginning of the 21st century, reducing coal combustion in rural China has become an important task for governments. Total coal consumption in rural areas has effectively been controlled in recent decades, as national and local governments have introduced policies to ban the burning of small boilers in rural areas to encourage farmers to use clean energy such as natural gas and electricity. In particular, since 2016, total coal consumption has clearly decreased (Figure 2).
In addition to political interventions, other factors impact coal consumption in rural areas. First, in the context of urbanization, the labor force in rural areas is gradually being transferred to cities; however, the quantity of coal consumption for heating houses has not been reduced because households still need to warm the same large spaces. For individual households, owing to the scale effect of energy consumption for heating and cooking, the larger the population scale is, the lower the per capita consumption of household energy. 20 Thus, per capita coal consumption declined more slowly than total consumption in rural areas from 2005 to 2021, and domestic coal consumption per capita even increased after 2019 (Figure 2). Second, many rural families present a lift mode in which older parents stay in the countryside while young people bring their spouses and children to work in the city. Older adults are more inclined to use coal, firewood, and other traditional energy sources, which is a significant obstacle to controlling coal consumption in rural areas.
Medical treatment of rural residents
In recent years, as the income of rural residents in China has increased, health and medical conditions in rural areas have also significantly improved. First, as an emerging developing country, China’s rural residents’ income levels have increased rapidly, from 2282 CNY in 2000 to 20 133 CNY in 2022, with an average annual growth rate of 10.4%. The supply levels of grain, milk, and aquatic products also greatly improved during this period, and fewer people fell ill because of malnutrition than they did in the last century. Moreover, under the guidance of the policy, the 3-tier medical system of counties, towns, and villages was promoted by the Chinese State Council in 2015. This has led to a clearer division and effective cooperation among medical institutions at different levels, especially primary medical care systems in rural areas, which are more regular, and nearly every village has a government-funded clinic and general practitioners. 21 The arrangement of collective purchases of drugs has reduced their prices; under the insurance policy system of China’s new cooperative medical scheme, over 70% of inpatient medical fees and chronic disease treatment fees in rural areas expedited by peasants are paid by the government 22 ; thus, medical systems are more beneficial and inclusive for Chinese rural residents.
However, there is still marked pressure on China’s rural medical systems. First, there is a significant aging trend in rural areas in China; the population over 60 years old in rural areas of China accounted for 19.8% of the total population in 2022, and the incidences of senile chronic diseases (SCDs), such as hypertension, cardiovascular and cerebrovascular diseases, and diabetes, are on the rise.23,24 Families with SCDs had higher hospitalization rates and numbers of outpatient visits than did control families. 25 Thus, the aging trend has increased the number of medical visits per capita in rural China. Second, as industrialization and urbanization have progressed, air, soil, and water pollution has expanded from urban to rural areas, and rural residents face a greater risk of environmental pollution than before. Therefore, the incidence rates of pollution-related diseases, such as cancer, respiratory disorders, and nervous system diseases, are increasing in rural areas.
In Figure 3, “outpatient treatment” means that the patient leaves the hospital immediately after diagnosis and purchases medicine, whereas “inpatient treatment” means that the patient resides in the hospital for a long period. With increasing income, rural Chinese residents’ annual number of outpatient visits per capita remained relatively high during the 2013 to 2017 period (Figure 3). The total number of visits includes the number of inpatient and outpatient visits. The former is only approximately 10% higher than the latter. The main reason is due to rural hospitals’ relatively backward medical conditions compared with urban hospitals; if rural residents develop serious diseases and require hospitalization, they still prefer hospitals in large cities or the nearest county for treatment.

Frequency of Chinese rural residents’ medical visits.
Although rural areas in China face many challenges in residents’ health maintenance, external factors also impact the frequency of rural residents’ visits to local clinics. First, most rural areas in China have achieved 4G or 5G network coverage. Farmers can buy high-quality food from all over the world over the internet, acquire more health-related knowledge, and obtain more advanced disease treatments through online medical institutions. 26 Second, actions to improve village appearance and the environment have also been implemented in villages in China since the 18th National Congress of the Communist Party of China in 2013. 27 Most villages have running tap water, garbage is collected into assigned places and recycled, and an increasing number of residents set up clean latrines for their families, all of which reduce the risk of illness related to sanitary conditions for rural residents.
Third, improving rural residents’ health literacy and encouraging a healthy lifestyle have been the charge of China’s health management departments since the turn of the century. The government has recently promulgated and implemented the “Action Plan for Rural Health Education” and “Guiding Approaches on Promoting the Construction of Healthy Villages.” These policies call for improving rural residents’ health awareness and self-care ability by strengthening health services for key groups, popularizing healthy lifestyles in rural areas and preventing populations from returning to poverty due to illness. 28 Therefore, the medical treatment of rural residents slowly decreased after 2014. As Figure 3 shows, the annual number of visits to local clinics per person decreased from a peak of 3.27 in 2014 to 2.24 in 2021.
Mortality rates for every type of disease in China’s rural areas
Tables 1 and 2 present the main types of diseases and their rankings in terms of mortality rates in China’s rural areas. Although the medical conditions of rural residents have greatly improved, aging is an inviolable trend in China and is currently accompanied by many chronic diseases, such as cardiovascular and cerebrovascular diseases, cancer, diabetes, and rheumatism. Moreover, prolonged poor living habits and relatively weak awareness of health care have led some rural residents to consume excessive amounts of food containing sugar and fat, as well as tobacco, alcohol, and other unhealthy foods, with improved income. Thus, as shown in Table 2, the incidence rates of cardiac and cerebrovascular diseases and malignant tumors are high, making them the 3 deadliest diseases in rural areas. The numbers of deaths per 100 000 people were 188.58, 175.58, and 167.06 in 2021, respectively. Therefore, improved health education and screening or preventive measures in the early stages of the disease are needed.
Mortality rates and ranks of major diseases in 2005.

Mortality rates and ranks of major diseases in 2021.
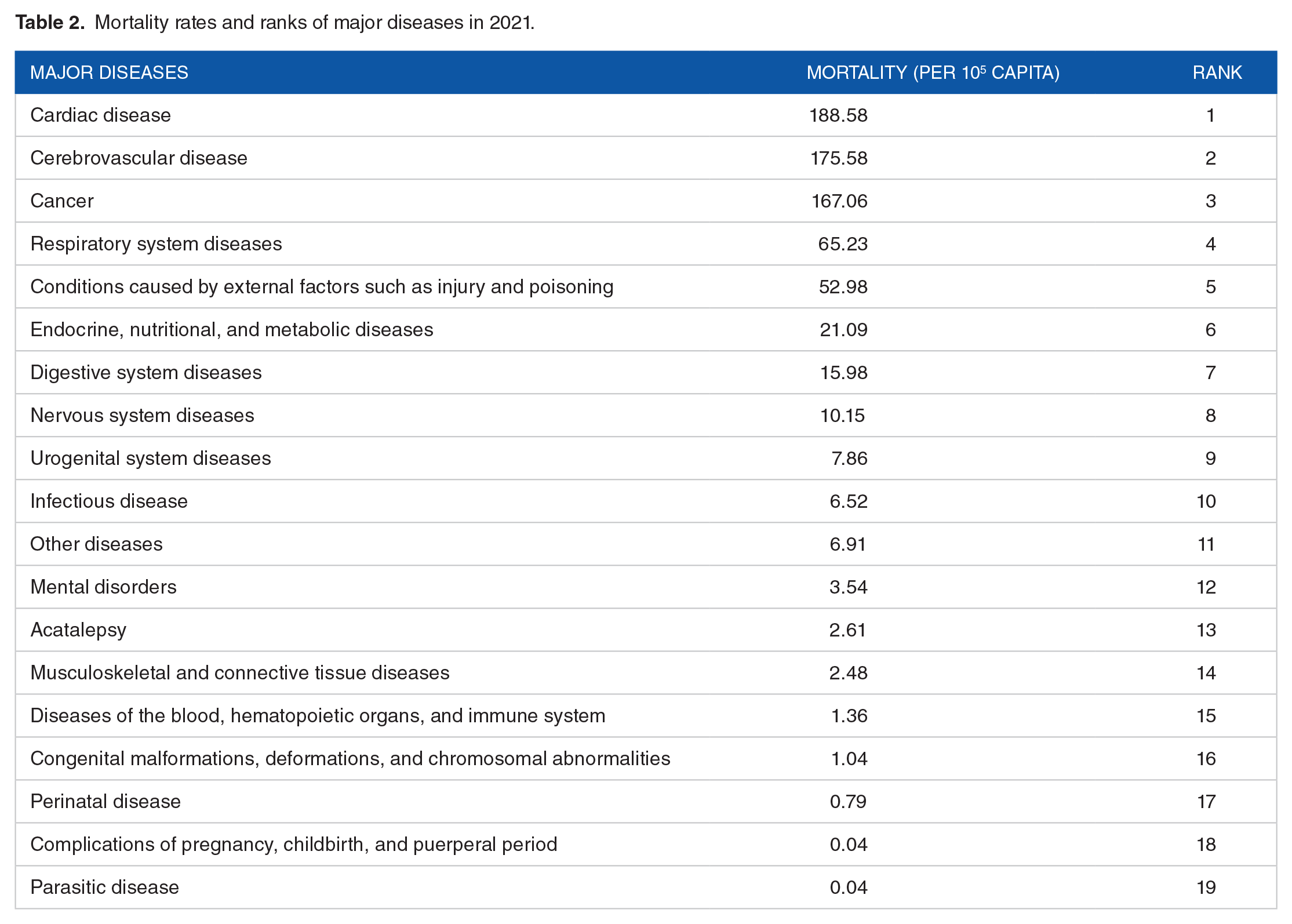
There were also significant variations in the rank order of mortality rates between 2005 and 2021. Owing to strict air pollutant emission control policies, the average concentrations of particulate matter and sulfur dioxide have greatly decreased after the 18th National Congress of the Communist Party of China, and the mortality rate and ranking of respiratory diseases in rural areas have decreased significantly, with the mortality rate per 100 000 people decreasing from 123.79 in 2005 to 65.23 in 2021. Respiratory system diseases and tuberculosis of the respiratory tract emerged as respiratory system diseases in 2021, and the mortality rate of the latter clearly decreased in 2021. The fatality rate associated with respiratory system diseases also decreased from first to fourth among all diseases.
However, it cannot be concluded that the problem of rural residents’ exposure to air pollution has been completely solved. Indoor air pollution resulting from household’s burning coal and straw is still a problem, and the mortality rates of nervous system diseases, cerebrovascular diseases, and urogenital system diseases that are likely related to coal burning emissions are quite high in China’s rural areas. The causal relationships between coal consumption and mortality rates from these diseases should be further examined.
Methods
To research the relationship between coal consumption in rural areas and the frequency of hospital visits more precisely, the following sections of this paper examine the impacts of coal consumption on the frequency of per capita hospital visits of rural residents via multiple regressions. The estimation modes are shown in functions (1) and (2), where the dependent variable pa represents the number of visits per capita during 1 year; pa can be divided into paz and paj, where the former includes the number of both outpatient and inpatient visits and the latter paj indicates the number of outpatient visits. The variables coall and coalp represent the amounts of coal consumed at the domestic and production ends, respectively. Z is the collection of control variables, and i and j represent the province and year, respectively.
Controlling variables include per capita income, the proportion of individual medical expenditure in total expenditure, per capita land area, degree of land mechanization, the number of rural doctors per 1000 people, the number of cases of infectious diseases, the number of individuals in the rural population affected by fluorine pollution, the regional death rate, and variables that reflect the diet of rural residents, for example, grain consumption per capita, edible oil consumption per capita, meat consumption per capita, dairy product consumption per capita, and aquatic product consumption per capita. Table 3 describes the variables used in the study. The panel data include 30 provinces and municipalities from 2010 to 2021. The Tibet Autonomous Region was excluded because some of its data were not accessible from official statistical departments.
Variable descriptions.



This study also assessed the relationships between coal consumption per capita and mortality from diseases in rural areas. However, if the mortality rate of a certain disease is relatively low, the correlation between coal consumption and the mortality rate of this disease may be accidental and not robust. Therefore, the author selected the top 10 diseases with the highest mortality rates and carried out correlation analyses on coal consumption. It is difficult to accurately judge the causal relationships between coal consumption and disease mortality rates using only positive correlations; therefore, this paper also uses the Granger causality test to analyse causal relationships. If the Granger causality test reveals a significant causal relationship and a positive correlation between 2 variables, it can be concluded that coal consumption leads to an increase in the mortality rate of that disease. The results are presented in Section “Pearson correlation and Granger causality tests.”
Results
Impact of coal consumption on residents’ medical visits in rural areas in China
The regression results are shown in Table 4. According to the results of the Hausman test, fixed effect regression analysis was adopted. Total coal consumption per capita and domestic coal consumption per capita had significant positive effects on the density of the total number of medical visits and outpatient visits. Specifically, as shown in Column 1, the coefficient of total coal consumption (coal) is 0.897, P < .001, and the confidence interval is [0.507, 1.287]. As shown in Column 3, the impact of total coal consumption on outpatient visits is also significant at the .1% level. Production-end coal consumption did not have a significant effect on the frequency of medical visits, whereas it was significant for the results of domestic-end coal consumption, as indicated in Columns 2 and 4. The reason for these results is that coal consumption at the domestic end is linked to the lives of rural residents. Residential coal often directly emits pollution, as households lack soot purification facilities; thus, the amount of pollution emitted by domestic coal consumption is greater than that emitted by coal-fired power plants in factories. Moreover, it is difficult to dissipate indoor air pollution over a long period, and the damage to residents’ organ functions is more lasting and significant.
Impact of coal consumption on rural residents’ medical visits.

P < .5. **P < .01. ***P < .001.
Indoor air pollution can directly or indirectly lead to various diseases, particularly diseases due to damage to the respiratory and nervous systems. Previous studies have reported that air pollution often causes respiratory diseases; recently, increasing evidence has suggested that air pollution may contribute to neurodegenerative and Alzheimer’s diseases.29,30 One study reported that air pollution may have significant adverse effects on the immune and nervous systems, which can begin in utero before birth, potentially causing delayed chronic diseases that develop later in life. 31 Indirect diseases refer to the recurrence of diseases due to air pollution, such as aggravated cardiovascular and cerebrovascular diseases caused by indoor hypoxia. 32 These diseases are frequent and chronic, leading rural residents to seek treatment at local clinics.
Most of the coal consumed at the production end is generated during power generation, metal smelting, kiln firing, and heating in agricultural breeding greenhouses. Therefore, the number of victims exposed to poisonous gas is relatively limited compared with that from domestic use because most of them are from factories or farms that burn coal during production. Furthermore, exhaust gases are often emitted outdoors through smokestacks and are more likely to dissipate in the countryside’s wild, sparsely populated areas. Thus, production-end coal burning has a relatively minimal impact on the health of residents in daily life compared with its domestic use.
The other control variables, per capita income (inc) and edible oil consumption (oil), had significant positive impacts on the frequency of medical visits (Table 4). The higher the per capita income was, the more the residents could afford treatment fees; therefore, they were more attentive to their health and were more inclined to visit the village clinic for treatment once they fell ill. The increase in the consumption of edible oil was related to increased dietary fat and could lead to hypertension or hyperlipidaemia. 33 In this case, the probability of rural residents visiting the clinic would also increase. The number of rural doctors per 103 capita (doc) also has a significant positive effect on the frequency of total medical visits, and the results indicate that a greater number of doctors can provide more comprehensive and high-quality medical services, helping to increase the number of visits, both outpatient and inpatient.
The variables that could significantly inhibit the number of medical visits include the proportion of individual medical expenditures in total expenditures (expr) and aquatic product consumption (aqua). The findings suggest that the greater the burden of individual medical expenses, the lower the number of visits to doctors. The overall income level of rural residents is lower than that of urban residents, and medical expenses are an important factor in determining the frequency of farmers’ visits to clinics. The negative impact of per capita aquatic consumption shows that this type of food is beneficial to the health of the population. In rural areas of China with an increased average population age, the consumption of aquatic products has a significant effect on maintaining cardiovascular and cerebrovascular health in older individuals. Although omega-3 fatty acids in fish are generally considered direct factors that promote cardiovascular health, a prior study also concluded that the health effects are caused by the interaction of various nutrients in fish products rather than simply because of the efficacy of the omega-3 fatty acids. 34 This behavior could decrease the frequency of medical visits by people who frequently consume aquatic products.
Finally, the death rate (deathr) is negatively correlated with the average annual number of medical visits by residents (Table 4). The reason is that areas with high mortality rates tend to have a high degree of aging, and older people sometimes cannot be moved easily, making it difficult to visit clinics. Sometimes older adults must be accompanied by their families, reducing the average annual number of visits.
Pearson correlation and Granger causality tests
To increase the interest and importance of the research results, the authors examined the correlations between the top 10 deadliest diseases nationally and per capita coal consumption from 2005 to 2021. According to the regression results shown in Section “Impact of coal consumption on residents’ medical visits in rural areas in China,” the total and domestic coal consumption levels of rural residents in China have a significant positive effect on the annual number of medical visits of residents. In contrast, the effect of production-end coal consumption is not significant. Therefore, this section assessed the correlations between total or domestic coal consumption and disease mortality. Although the positive correlation between coal consumption and the mortality rate of a specific disease does not completely indicate that coal consumption is the cause of death, the significant correlation indicates that the 2 have an inherent connection that cannot be ignored.
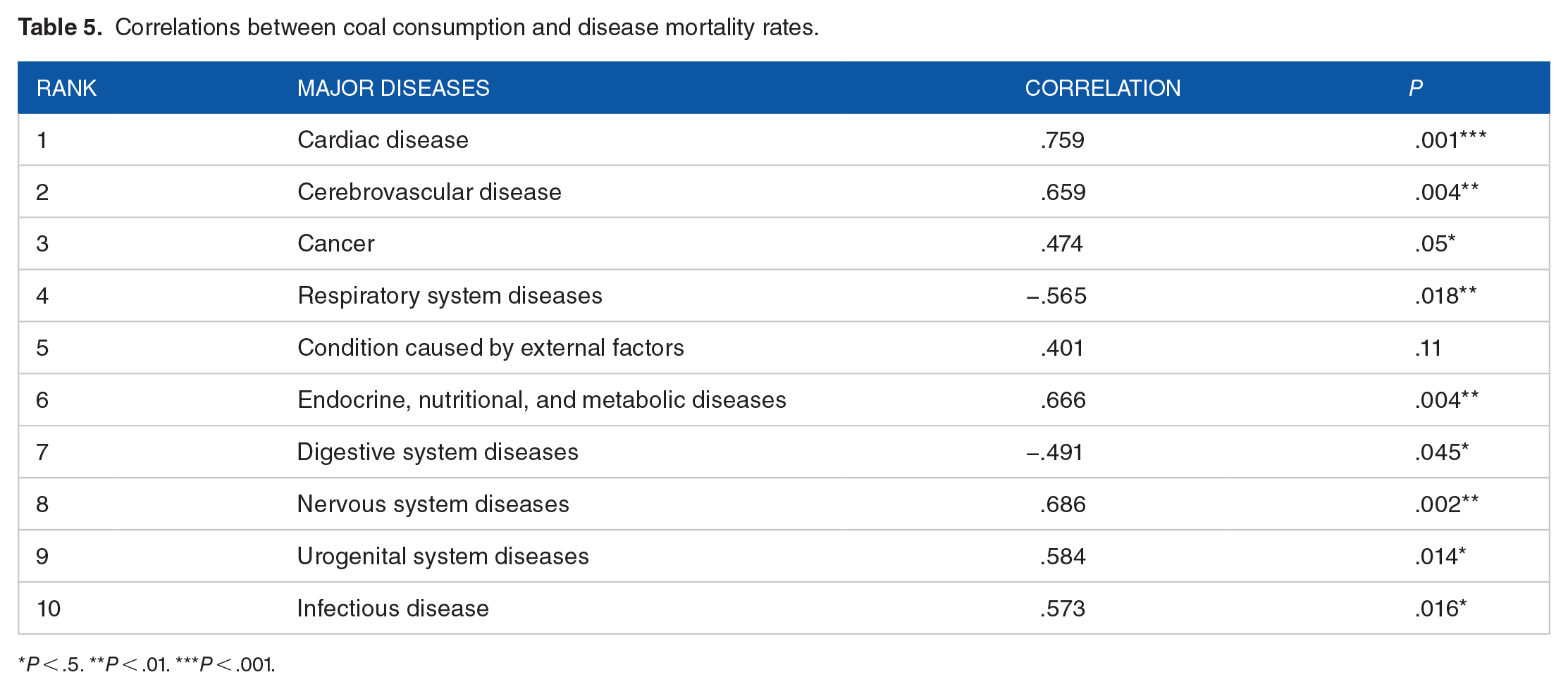
The results are shown in Tables 5 and 6. The mortality rates of 8 out of the 10 diseases were positively correlated with per capita coal consumption; in particular, cerebrovascular disease and cardiac disease were significantly correlated (.768 and .656, respectively) (Table 5). Coal consumption leads to human hypoxia. Soot, carbon monoxide, carbon dioxide, sulfur dioxide, and other waste are also produced during this process, which may damage the heart and blood vessels. For example, a study reported a significant association between domestic coal use and death from ischemic heart disease or stroke in rural Chinese women and recommended that more ventilation stoves be installed in rural households to reduce this risk. 35 Among other diseases, nervous system diseases and genitourinary and circulatory system diseases are also highly related to rural coal consumption.
Correlations between coal consumption and disease mortality rates.
P < .5. **P < .01. ***P < .001.
Correlations between domestic coal consumption and mortality rates.

P < .5. **P < .01. ***P < .001.
There is a negative correlation (P = .018) between coal consumption and the mortality rate of respiratory diseases in rural areas, which is not consistent with expectations. This is because a considerable proportion of rural coal is used for indoor heating in winter, and indoor insulation in winter has a positive preventive effect on respiratory diseases. A prior study reported that temperature discomfort, which is caused mainly by cold, reduces the actual life expectancy of Chinese residents and increases death rates due to pneumonia, chronic obstructive pulmonary disease and other related diseases. These effects are more significant in males and northern residents. 36 Therefore, there is an overall negative correlation between the scale of coal consumption for heating and respiratory disease mortality. However, as coal heating increases overall air pollution levels and damages the respiratory system, the shift from coal to gas or electric heating is still one of the policy directions in rural China. The mortality rate of digestive system diseases is also negatively correlated with coal consumption. Currently, there is an aging trend in China’s rural areas; that is, the proportion of the older population is continually increasing. Cooking with coal can heat food at low temperatures and for a longer time, which has certain benefits for the digestive system of older individuals. 37 The results in Tables 5 and 6 are similar, except for a few diseases for which the correlations between death rates and coal consumption are slightly reduced.
Although the mortality rates of most of the above diseases are positively correlated with per capita coal consumption in Chinese rural areas, it is unclear whether the latter leads to the former; the Granger causality test could be used to verify these relationships. Each variable in the causality test is stable at the second-order level; thus, it meets the prerequisite of the Granger causality test. The results of the Granger causality test are shown in Table 7, which estimates whether coal burning leads to variations in the mortality rate of each disease. The results indicate 2 types of diseases caused by coal burning. Combined with the correlation test results, the results revealed that rural coal consumption leads to increases in mortality rates due to urogenital and nervous system diseases, with the increase in the incidence of urogenital system diseases being more significant (P = .009). The genitourinary system is one of the fastest metabolizing tissues in the human body and is the first to be affected when fluorine-containing toxic particles are discharged from coal burning and enter the human blood circulation.38,39 The accumulation of toxic particles can cause a series of urogenital system diseases, such as kidney failure, uremia, oligospermia, sperm malformation, and prostate hyperplasia.39,40
Granger causality results of coal consumption and mortality rates of major diseases (coal consumption mortality).

P < .10. **P < .05. ***P < .01.
Consistent with the conclusions reported by other scholars, coal exhaust can damage the nervous system. Specifically, the human central nervous system requires a large amount of oxygen to support normal activities, and hypoxia causes irreversible damage to the nervous system. 41 Soot discharged from insufficient coal burning contains a large amount of carbon monoxide, which prevents oxygen from binding to human hemoglobin. Thus, soot inhalation causes hypoxia and damage to the nervous system, which may lead to cognitive decline, memory loss, seizures, and limb disorders. 42 Combined with the results of the above correlation test, rural coal consumption led to a slight decrease in the death rate of patients with respiratory system diseases (P = .073). Although previous studies have shown that soot inhalation can damage the human respiratory tract, the findings of this study indicate that coal burning leads to a decrease in the mortality rate of respiratory diseases. The difference is that coal heating can alleviate respiratory disease-related injuries in winter to a certain extent other than death.
The 3 diseases with the highest mortality rates, that is, heart disease, cerebrovascular disease and malignant tumors, have no clear causal relationships with coal burning (Table 7); however, there are significant positive correlations between these variables (Tables 5 and 6), and previous studies have also indicated that coal combustion is a cause of these diseases.43 -45 The lack of significance in the results can be attributed to the focus of the Granger causality test on statistical outcomes; in fact, there may still be a low degree of internal effect between the 2 variables. China’s rural areas have a greater number of older people in coal-using households, and older people constitute the highest risk group for these 3 diseases. However, although the correlation test results are significant, no causal relationships have been established.
Conclusion
Coal remains an important energy source in rural China because of the difficulty of expanding natural gas lines to all rural areas; moreover, coal is relatively inexpensive and affordable for rural residents with relatively low incomes. Coal consumption in rural domestic areas has a significant positive effect on the average annual number of medical visits of rural residents after illness, whereas production-end coal consumption has no such significant effect. This is because the former affects a wider range of people, and persistent indoor air pollution has a more significant impact on residents’ health. However, coal exhaust emissions from production tend to be intermittent, and the range of damage to the population is often limited to production workers. Significant positive correlations exist between coal burning and 7 of the top 10 deadliest diseases. In fact, coal consumption in China’s rural areas increases the risk of mortality from urogenital and nervous system diseases.
Therefore, upgrading and replacing rural energy sources must be accelerated. Coal should be replaced with clean and renewable energy sources such as natural gas, electricity, and biogas. Specifically, governments and social institutions should make efforts to allow more natural gas pipelines to extend to rural areas and establish power supply facilities for urban‒rural integration to ensure the availability of clean energy supplies in rural areas. More medical personnel and funds should also flow to the rural medical system to provide higher-quality and lower-priced medical services for rural residents and promote the prevention and treatment of related diseases. Clean and efficient coal furnaces can be achieved. The market supervision of coal in rural areas should be strengthened to limit businesses from selling clean, desulfurized, and defluorinated anthracite coal. Farmers should be encouraged to use energy-efficient stoves that can increase coal burning rates, increase the proportion of centralized heating and electric heating in rural areas in winter, reduce dust and carbon monoxide production, and curb indoor air pollution.
The health awareness of rural residents should be improved. Environmental health education should be carried out in rural areas, and more farmers should be made aware of the harm caused by the excessive use of coal as domestic energy through publicity videos, artistic performances and onsite lectures, reducing the market acceptance of inferior coal in rural areas. Households should be encouraged to use more anthracite and ventilation furnaces and encourage more active cooperation in upgrading rural coal to gas, coal to electricity and other facilities. Regular health screenings should also be carried out; for example, in addition to paying attention to the prevention of diseases with high mortality rates, such as cardiovascular and cerebrovascular diseases and malignant tumors, it is necessary to regularly check the nervous system and urogenital functions of residents in coal-consuming rural areas, which would reduce the incidence and mortality rates of these diseases caused by coal burning.
Footnotes
Acknowledgements
We would like to thank the anonymous reviewers and editor for their constructive comments. We are also grateful to all suggestions from professors and committee members (Dong Guo – Columbia University, Hongchuan Wang – Tsinghua University, Beibei Hou and Qian Meng – Henan University).
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We also gratefully acknowledge the support from National Natural Science Foundation of China (Grant number 7227040618) /Henan Provincial Philosophy and Social Science Planning Fundation (2021BJJ027) for conducting this research.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.