
Abstract
Background:
Arsenic, a widely recognized and highly toxic carcinogen, is regarded as one of the most hazardous metalloids globally. However, the precise assessment of acute and chronic human exposure to arsenic and its contributing factors remains unclear in Ethiopia.
Objective:
The primary goal of this study was to assess the levels of acute and chronic arsenic exposure, as well as the contributing factors, using urine and nail biomarkers.
Methods:
A community-based analytical cross-sectional study design was employed for this study. Agilent 7900 series inductively coupled plasma mass spectrometry was used to measure the concentrations of arsenic in urine and nail samples. We performed a multiple linear regression analysis to assess the relationships between multiple predictors and outcome variables.
Results:
The concentration of arsenic in the urine samples ranged from undetectable (<0.01) to 126.13, with a mean and median concentration of 16.02 and 13.5 μg/L, respectively. However, the mean and median concentration of arsenic in the nails was 1.01, ranging from undetectable (<0.01 μg/g) to 2.54 μg/g. Furthermore, Pearson’s correlation coefficient analysis showed a significant positive correlation between arsenic concentrations in urine and nail samples (r = 0.432, P < .001). Also, a positive correlation was observed between urinary (r = 0.21, P = .007) and nail (r = 0.14, P = .044) arsenic concentrations and the arsenic concentration in groundwater. Groundwater sources and smoking cigarettes were significantly associated with acute arsenic exposure. In contrast, groundwater sources, cigarette smoking, and the frequency of showers were significantly associated with chronic arsenic exposure.
Conclusions:
The study’s findings unveiled the widespread occurrence of both acute and chronic arsenic exposure in the study area. Consequently, it is crucial to prioritize the residents in the study area and take further measures to prevent both acute and chronic arsenic exposure.
Introduction
Arsenic is a widely recognized, highly toxic carcinogen and is regarded as one of the most dangerous metalloids in the world. 1 Also, arsenic is one of the most dangerous endocrine-disrupting chemicals and poses a wide range of health hazards. 2 Arsenic is a highly toxic, effortlessly transportable, widespread contaminant worldwide. 3 Arsenic is widely distributed in the environment and is found in over 200 mineral species. It ranks 20th in the earth’s crust, 14th in seawater, and 12th in the human body.4,5 However, paradoxically, arsenic is not considered an essential element and is extremely hazardous to humans. 6
Arsenic is mostly released into the environment through either human activities or natural processes. 7 Surprisingly, arsenic has remained stable in the environment for several years, as it is not easily transformed from a toxic to a nontoxic form. 8 Arsenic exposure in humans can occur through skin absorption, inhalation, or ingestion. However, ingestion is the predominant route for arsenic intake, followed by inhalation.9 -11 and dermal absorption. 12 Arsenic exposure in humans primarily occurs from consuming drinking water contaminated with arsenic. 13 Arsenic compounds are found in both organic and inorganic forms. Arsenite [As(III)] and arsenate [As(V)] are the predominant inorganic forms of arsenic in the environment and pose a greater risk to human health.14,15 In contrast, organic arsenic (As) compounds are prevalent in seafood but less harmful to human health and rapidly eliminated by the body. 16 Furthermore, most arsenic compounds have no taste, smell, or color and dissolve easily in water, posing a higher health risk. 17
Acute and chronic exposure to inorganic arsenic causes numerous cancers and noncancer health-related outcomes. 18 Acute arsenic poisoning results in 2 distinct clinical manifestations: acute paralytic syndrome and acute gastrointestinal syndrome.19,20 Prolonged exposure to low concentrations of arsenic in drinking water can lead to a wide range of health effects, 21 including skin lesions such as hyperkeratosis and alterations in pigmentation, as well as skin, lung, bladder, liver, kidney, and prostate cancer. Apart from numerous cancers, chronic exposure to arsenic can cause a broad range of non-cancer risks, including cardiovascular disease, hypertension, pulmonary, neurological, hepatic, and kidney diseases, type 2 diabetes mellitus, anemia, fetal loss, premature delivery, and male infertility.9,14,17,21,22,23,24,25,26,27,28,29,30 Likewise, chronic arsenic exposure is known to cause peripheral neuropathy as well as hearing, visual, somatosensory, and other disorders in humans. 31
Assessing human exposure to arsenic is a significant challenge, especially in a population exposed to relatively low concentrations of arsenic. Thus, the cumulative internal dose of an individual offers a biological way to track As exposure in the environment. Human exposure biomonitoring measures an individual’s present body burden and identifies recent and past environmental exposure. 32 Determining the amount of arsenic humans are exposed to by drinking water requires analyzing arsenic in biological samples and water. Exposure of a population to low amounts of arsenic in drinking water, which are possibly cancer-causing, may be better reflected by biological indicators in determining the total exposure dosage. 33 Hence, future studies should pinpoint environmental and human indicators for detecting early exposure, identifying poisoning, and assessing risks. Thus, selecting and developing suitable biomarkers for assessing arsenic exposure status is important for primary prevention and decision-making in public health.
Currently, biomarkers of exposure have received the most attention. The most common approach to understanding recent and chronic human exposure to arsenic is to determine the total arsenic concentration using biomarkers. 34 Concentrations of arsenic in blood, urine, hair, and nails have all been used as exposure indicators.14,33 -35 Among these, urine, hair, and nails are the most commonly employed biomarkers36,37 to identify, quantify, and monitor arsenic exposure. 38 Urinary arsenic has recently been considered a more preferable and reliable biomarker for monitoring recent exposure than blood because most absorbed arsenic is eliminated through urine and is relatively easy to collect.37,39 However, individuals should avoid consuming certain seafood before urine sampling to prevent confounding the estimation of inorganic arsenic exposure. In contrast, arsenic in nails is also a useful indicator and a preferred biomarker for assessing past exposure, while it is less prone to external contamination than hair.40 -42 Urinary arsenic is a biomarker of recent exposure, whereas nail arsenic is a biomarker of long-term (past) exposure.43 -45 Hence, measuring acute and past exposure to arsenic using appropriate biomarkers is essential for understanding the true magnitude of arsenic exposure and assessing its health impacts. However, no study has examined this issue in the study area or country. In addition, there is a lack of knowledge on the magnitude, presence, and impact of arsenic in Ethiopia among academicians, policymakers, research institutes, governments, and nongovernmental sectors, especially those working in water, sanitation, and hygiene interventions.
As a result, this study aimed to assess acute and chronic exposure to arsenic through groundwater consumption among the residents of the study area using urine and nail biomarkers and associated factors.
Materials and Methods
Description of the study area and population
The study was conducted in the Adami Tulu Jido Kombolicha District. Adami Tulu Jido Kombolcha District lies in southern Ethiopia, within the East Shewa Zone of the Oromia Region. The district capital city, known as Batu Town, is located 115 km from the zonal city of Adama and 160 km from the capital city, Addis Ababa. 46 The district is located at an altitude of 1500–2000 meters above sea level, with a latitude of 7°56′N and a longitude of 38°43′E. 47 It is bordered by other districts, zones, and regions within the Central Rift Valley, such as the Arsi Negele district in the south, the Dugda Bora district in the north, the Arsi zone in the east, and Southern Nations and Nationalities People in the west. 46 The district’s topography varies, encompassing highland areas, lowland plains, and valleys. It is part of the Great Rift Valley system, characterized by geological features such as escarpments, volcanic formations, and rift lakes. According to the 2007 Ethiopia Central Statistical Agency, the district has a total population of 142 861, of which 71 883 (50.3%) were male and 70 978 (49.7%) were female. Of the total population, 20 918 (14.6%) were urban residents, while the rest, 121 943 (83.4%), were rural residents. 48 The predicted population by the Ethiopian Central Statistical Agency in 2022 was 211 827 (106 205 males and 105 622 females), with an estimated area of 1274.54 square kilometers and a population density of 193.5/km2. 49
The area is characterized by agricultural and industrial zones, and many state- and private-owned industries operate. As a result, industrial and agricultural operations in the area release chemicals and fertilizers used in floriculture, horticulture, and other activities directly into nearby lakes and the environment. 50 Consequently, excessive application of these chemicals and fertilizers, coupled with the rift systems in the area, deteriorates the quality of surface and groundwater sources and poses a threat to humans in the studied area. In this laboratory-based cross-sectional study, 200 randomly selected participants provided paired human urine and nail samples (Figure 1).

Map of the study area.
Study design and study periods
A community-based analytical cross-sectional study design was used to evaluate the extent of acute and chronic arsenic exposure among the residents in June 02-20, 2022. Human urine and nails were used as biomarkers to assess acute and chronic arsenic exposure levels.
Source and study population
The source population was individuals who resided in the study area, while the study population consisted of individuals residing in the study area during the study period who met the specified inclusion criteria and were selected as the sample for the study.
Inclusion and exclusion criteria
Eligibility criteria: Individuals who had yet to eat fish within the 3 days before the study had sufficient nails at the sampling time. In addition, study participants aged more than 30 years who lived in the study area for at least 10 years and people who volunteered to provide paired urine and nail samples were included in the study.
Exclusion criteria: Individuals who had eaten seafood, such as fish, 3 days before the study and who needed more nails during the study period were excluded from the study. In addition, we excluded study subjects aged less than 30 years and those who refused to provide paired urine and nail samples.
Sample size determination
In this study, the required sample size was determined using the formula provided by Yamane Taro. 51 This formula used a 95% confidence level, a 10% margin of error, and a design effect of 2.0.

Therefore, using the above formula and assumptions, the final calculated sample size for this study was 200. The final calculated sample size was allocated with a population proportion to each selected kebeles. Accordingly, 200 study subjects responded to the interviews and provided paired urine and nail samples.
Sampling procedure
A stratified multistage sampling method was employed for this study to select the study subjects. In the first stage, all kebeles were stratified by residents into urban and rural areas. In the second stage, using ENA software, the PPS cluster sampling method was applied to select clusters or kebeles. Therefore, 16 rural kebeles and 5 urban kebeles (21 kebeles) were randomly chosen for this study via a simple random sampling method. In the third stage, households and study participants within selected kebeles were selected for interviews and to provide paired urine and nail samples via simple random sampling.
Data collection methods
Initially, the data collection tools were prepared in English, then translated into local languages, and finally back-translated into English to ensure their coherence with the original tool. Before the actual data collection, the translated tools were pretested in a similar setting that was not included in the study area. Online mobile application software (Kobo Toolbox) was used to collect sociodemographic, environmental, and exposure history variables. A total of 200 study subjects participated in this study, and 200 paired urine and nail samples were collected from randomly selected respondents to assess the acute and past arsenic exposure status among the study population. Face-to-face interviews using pretested structured questionnaires were conducted among study subjects who provided urine and nail samples to collect sociodemographic, behavioral, lifestyle, and environmental or exposure-related information.
Data collection procedure
After receiving written consent from the study participants, paired urine and nail samples were collected from 1 volunteer respondent per household who fulfilled the inclusion criteria. In the meantime, participants were also interviewed to collect their sociodemographic information, exposure history, and behavioral or lifestyle factor information.
Sample collection procedure and storage
Urine samples
Participants who provided morning urine samples were instructed to avoid consuming fish for 3 days before their scheduled collection appointment. Participants were instructed to self-collect midstream morning urine on their visit and store it carefully until their appointment to minimize potential factors that could influence the results. A tightly sealed 50 ml polyethylene bottle treated with HNO3 was used to collect morning urine samples. Two hundred randomly chosen participants collected urine samples using pre-acid-washed polyethylene bottles. These samples were promptly placed in an ice box set at 4°C and stored at this temperature until they reached the laboratory. 52 The collected samples were transported in an ice box and kept in a deep freezer at −20°C at the Ethiopian Public Health Institute laboratory until analysis.
Nail samples
Apart from urine samples, nail samples were collected from randomly selected study participants who fulfilled the inclusion criteria using stainless-steel clippers. Before collecting the samples, study subjects were instructed not to use or remove existing nail polish from their fingers and toes to avoid any potential influence on the analytical measurements. In addition, prior to sample collection, study participants washed their hands and feet with soap.53 -55 All fingers and toenails from each study participant were clipped to obtain the measurable quantity and placed in polyethylene plastic vials to prevent contamination. We labeled each nail sample with the date of collection and a unique sample code. All the fingers and toes were self-collected and stored in prelabeled polyethylene plastic vials at room temperature until analysis. 52 A total of 200 nail samples were collected from randomly selected respondents to measure the arsenic concentration in nails and determine the chronic arsenic exposure status among the study population.
Sample preparation, processing, and analysis
Urine samples
The frozen urine samples were thawed at ambient temperature for sample preparation. Due to the high matrix of urine, 1 ml of urine sample was diluted 10× with 1% v/v HNO3 (Sigma Aldrich) and 0.5% v/v HCl to minimize the effects of elevated sodium concentrations on signal stability 56 and to minimize the level of TDS in the sample. The sample was shaken gently, and the acidified sample was filtered using a 0.2 μm syringe filter before analysis. The prepared samples were stored at 4°C until analysis. In addition to the real samples, 10 blank samples were made using similar techniques for sample digestion but without the urine sample used for quality control. The instrument was conditioned overnight to create the needed vacuum (1–2 × 10−5) and optimized by adjusting the daily performance using a tuning solution. Potential polyatomic interferences (PPI) with the same mass/charge ratio as As (m/z 75) were eliminated using the helium (He) collision cell method. An Agilent 7900 series inductively coupled plasma mass spectrometry was used to determine the concentration of arsenic in the digested urine samples.
Nail sample
The nail samples were digested using a previously reported protocol. 54 In order to eliminate surface contamination, the samples were physically scratched in the lab using a ceramic knife before being cleaned. The samples were cleaned with tap water after being submerged in nonionic detergent for the entire night. The nail samples were then shaken for 20 minutes in a 0.5% Triton X-100 solution after being cleaned 3 times for 20 minutes in acetone. The samples were then cleaned using deionized water. Lastly, the samples were dried overnight at 60°C in an oven. According to Dessie et al 54 the dried samples were digested. Briefly, 100 g of cleaned and dried nail sample was weighed, transferred to a conical flask, and digested using 6 ml HNO3/HCl (3:1), which resulted in the addition of 5 ml of HNO3 (70%) and 1 ml of HCL (37%). The digesting flasks were maintained at ambient temperature for 30 minutes with a watch glass covering them. The samples were predigested at room temperature, heated to 80°C almost to dryness, and then cooled to ambient temperature. The dried material was then mixed with 2 ml of HNO3 (70% Sigma-Aldrich), and after heating, the residue was dissolved in ultrapure water. Subsequently, the broken-down mixture was filtered through a 0.2 μm syringe filter, diluted to 8 ml using ultrapure water, and kept at 4°C until analysis. A blank sample was also prepared using the same procedures for the digestion of samples but without the nail sample for quality control. Like in urine analysis methods, a calibration curve was prepared for nail analysis. The levels of arsenic in the digested nail samples were analyzed using the Agilent 7900 series ICP-MS at the Ethiopian Food and Drug Authority laboratory.
Chemicals, reagents, and solutions
Analytical grade Ar (99.999%), acetone (99.9%), hydrochloric acid (37%), and nitric acid (70%) from Sigma-Aldrich in the USA, and Triton X-100 (0.5% v/v) were used in the study. We diluted the standards and samples with high-purity deionized water during the analysis. A calibration curve was prepared for arsenic analysis. Accordingly, standard solutions of 1.0, 5.0, 10.0, 20.0, 50.0, and 100 ppb were prepared for the calibration curve (Figures 2 and 3).

Calibration curve for urine samples.

Calibration curve for nail samples.
Study variables
The concentrations of arsenic in the urine and nail samples were considered dependent variables, whereas the independent variables were sociodemographic, environmental, and exposure history. Residence, sex, age, marital and educational status, occupation, and socioeconomic status were considered as sociodemographic variables. Furthermore, we considered time spent at the workplace, years spent in the area, source of water supply, average water consumption per person per day, frequency of taking showers, the practice of water treatment, vegetable gardening, smoking cigarettes, alcohol consumption, and chewing Khat as factors contributing to exposure history and environmental conditions. 57
Statistical analysis
Data analysis was employed using SPSS version 29 statistical software. We used univariate analysis to examine each variable’s distribution and test fundamental assumptions. The descriptive statistics were analyzed, and the results are presented in tables and figures. Bivariate analyses were also conducted to identify the determinant factors or predictor variables. The study included 2 dependent variables and multiple independent variables. Therefore, a multiple linear regression model was applied for this study to examine the relationships between dependent and independent variables. Before running the multiple linear regression model, key assumptions were checked to determine the appropriateness of the model. Therefore, we independently checked the most important assumptions, including linearity, outliers, normality of residuals, homoscedasticity, independence of independent variables (independence of errors), and multicollinearity between the variables.
Cook’s distance was used to check for potential outliers, and the highest Cook’s distance value was less than 1, indicating no influential outliers. To assess homoscedasticity (homogeneity of variance), we utilized a scatterplot of residuals versus predicted values. In contrast, the Kolmogorov-Smirnov and Shapiro-Wilk tests were used to check for the normality of the distributions of urine and nail samples. In addition, the independence of observations was assessed using the Durbin-Watson statistic test, and the result indicates that the data is not autocorrelated and the assumption of independence of errors is met. The standardized scatterplot confirmed the acceptance of the assumption of equal variance. However, the Kolmogorov‒Smirnov and Shapiro‒Wilk tests showed that the data for the urine and nail samples were not normally distributed (P < .05). Since the data were not normally distributed, the normality assumption was violated. As a result, the data were log10 transformed to normalize the data. After the data were transformed, the urine and nail samples were normally distributed, and the assumption of normality was fulfilled. A multicollinearity test was also conducted using the variance inflation factor and tolerance tests. The results of both tests indicate the absence of multicollinearity for all explanatory variables.
Furthermore, Spearman’s rank correlation coefficient (r) was used to assess the degree of association between the arsenic concentration in urine and that in the nail. A P-value of <.05 was set as the level of statistical significance. After fulfilling its key assumptions, we fitted the multiple linear regression model. The F-test was applied to assess the model’s goodness of fit, and the p-value for the F statistic is <.05. Moreover, the results of the F test for overall significance revealed that the model was statistically significant since the P-value was less than .004. Therefore, the overall model summary results suggest that the model is adequate and fits very well. Finally, a multiple linear regression analysis was used to test the relationship between the outcome and predictor variables. The degrees of association between the outcome and predictor variables were assessed using the F test and 95% CI. In the final regression model, a significance level of P < .05 was used to determine statistical significance.
Quality control and assurance
The study teams received a 3-day training. Also, a pretest exercise was done before the actual data collection work, which was not included in the study, to check the accuracy of responses, estimate the time needed, and make some modifications based on the findings. To minimize measurement error, study participants abstained from consuming fish for 3 consecutive days before collecting a urine sample, as consumption of some seafood could alter the measurement of inorganic As exposure. The levels of arsenic in the urine and nail samples were determined using the latest Agilent 7900 series ICP‒MS apparatus with a low detection level, good robustness, high accuracy, and dynamic range. 58 High-purity chemical reagents were used for this study to minimize errors and ensure the sensitivity and accuracy of the instrument. Blank samples were used to monitor background contamination. In addition, adequate sample size, randomization, standard data collection tools, advanced instruments, controlling confounding variables, and advanced statistical analysis were used to minimize chance, bias, and confounding and ensure the reliability and validity of the study’s findings.
Moreover, the laboratory analysis adhered to the manufacturer’s operating protocol. The glassware used in the analysis was immersed in a 10% solution of nitric acid (HNO3) for an extended period, followed by multiple rinses with distilled water to cleanse it thoroughly. After desiccating the bottles, we hermetically sealed them at ambient temperature prior to utilization. We continuously checked the laboratory analysis for analytical correctness and precision. Regular calibration of measurement instruments is also used to ensure accuracy and reliability, minimizing the potential for systematic errors. Analyzing the blank samples in each batch guaranteed the precision of the analytical findings. We evaluated the accuracy and reliability of the ICP-MS by determining the spike recoveries. We used control samples, spiked solutions with a known concentration of arsenic, as standard reference solutions to verify the accuracy of the readings. After every set of 10 samples, we examined a control sample to confirm the precision of the analysis. The recovery rates for urine samples were 86%, while those for nail samples were 115%. The acceptable recovery rate was between 80 and 120%. 59 Thus, the recovery rates of the urine and nail samples tested were within acceptable ranges or satisfactory recoveries, indicating that the method was accurate for determining arsenic concentrations.
Ethical considerations
The study obtained ethical approval from the Addis Ababa University Research Ethics Review Committee. Before signing the written consent form, we informed the participants about the study’s purpose, benefits, and procedures. Accordingly, each study participant signed a written consent form to confirm their willingness before the interview and sample collection. Furthermore, the instruments and procedures did not cause any harm to the study participants or the research team involved in the study.
Results and Discussion
Sociodemographic characteristics of the study participants
A total of 200 study subjects (94 from urban areas and 106 from rural areas) participated in this study. Among the studied population, 91 (45.5%) respondents were male, while the remaining 109 (54.5%) were female. The median age of the respondents was 40 ± 11.2 years, ranging from 30 to 88 years. Regarding the educational background of the participants, 54 (27%) had completed primary education, 30 (15%) had completed secondary education, 29 (14.5%) had a certificate or higher qualification, and 87 (43.5%) had no formal education. In addition, among the studied population, 84 (42%), 22 (11%), and 19 (9.5%) were farmers, merchants/traders, and daily workers, respectively, while the remaining 38 (19%) and 37 (18.5%) were either governmental or private organization employees and unemployed or engaged in other activities, respectively. Furthermore, among the studied population, 96 (48%), 86 (43%), and 18 (9%) of the study participants were classified as having lower, middle, and upper economic status, respectively.
Total arsenic concentration in the urine samples
In this study, arsenic was detected in 90.5% of the urine samples, while the remaining 19 (9.5%) samples were below the analytical limit of detection of 0.01. The As concentration in the urine samples ranged from undetectable (<0.01 μg/L) to 126.13, with an average and median concentration of 16.02 and 13.5 μg/L, respectively. The minimum As concentration in urine samples was 0.31 μg/L, and the maximum was 126.13 μg/L. According to ATSDR 2007, normal arsenic levels in human urine should be less than 50 µg/L, while arsenic levels in urine samples >50 µg/L are considered high and abnormal. 60 In contrast, according to Wongsasuluk et al 61 and the American Conference of Industrial Hygienists, 62 the normal range of arsenic in urine is 35 µg/L. Similarly, Rahman et al 63 reported that the normal range of arsenic in urine samples is 5-40 µg/L, and these findings are consistent with the values reported by Javad et al 64 Since the limit value (cutoff value) for urinary arsenic level has not yet been established in Ethiopia, the normal urinary arsenic level in this study was used as the maximum limit value (<35 μg/L) as a cutoff value recommended by Wongsasuluk et al and the American Conference of Industrial Hygienists.
The study results showed that most of the respondents, 189 (94.5%), had urinary arsenic concentrations lower than 35 μg/L. In comparison, the remaining 11 (5.5%) had urinary arsenic concentrations higher than 35 μg/L at the time of the survey. The study results indicated that the average concentration of As in the urine samples of the study participants was below the recommended cutoff value of 35 μg/L. Thus, the study’s findings revealed that most respondents had urinary arsenic concentrations in the normal category. The mean urine As concentrations in this study were lower than those in other studies from Ghana, 65 Pakistan64 -67 China, 68 Thailand, 69 India, 63 Bangladesh,70,71 and Mexico. 72 However, the mean concentration of As in urine in this study was greater than that in studies from India, 73 Thailand, 61 and South Korea. 74
Research has discovered 2 unique clinical symptoms of acute arsenic poisoning: acute gastrointestinal syndrome and acute paralytic syndrome. 20 Acute gastrointestinal syndrome, which is characterized by burning lips, dry mouth, dysphagia, and severe vomiting, may be followed by hematemesis, while acute paralytic syndrome, which is manifested by cardiovascular collapse, is followed by a depressed central nervous system and death within a few hours. Given the toxic nature of arsenic, residents in the study area are at a higher risk of developing either acute gastrointestinal syndrome or acute paralytic syndrome during their lifetime.
Total arsenic concentration in the nail samples
The present study measured arsenic concentrations in residents’ nail samples using an Agilent 7900 series ICP‒MS apparatus to determine chronic arsenic exposure status among Adami Tulu Jido Kombolicha district residents. Arsenic was detected in 189 (94.5%) of the nail samples, while the remaining 11 (5.5%) samples were below the analytical detection limit of 0.01. The mean and median concentration of As in the nail was 1.01 µg/g, ranging from undetectable (<0.01 μg/g) to 2.54 μg/g. The maximum As concentration in the nail was 2.54 μg/g, and the minimum was 0.17 μg/g. According to Shokoohi et al, 75 the normal level of As in nail samples ranges from 0.02 to 0.5 μg/g, and these findings are consistent with those reported by Javad et al. 64 . Thus, concentrations of total arsenic above 0.5 μg/g are considered high and abnormal. Moreover, previous studies have reported that an arsenic concentration in nails above 1.0 μg/g indicates excessive exposure or toxicity.60,63 The study results showed that 158 (79%) of the respondents had higher than 0.5 μg/g arsenic in their nail samples, while the remaining 42 (21%) had lower than 0.5 μg/g arsenic in their nail samples. Moreover, in this study, the mean concentration of As in the nail samples was 1.01 μg/g, which was higher than the recommended cutoff value and indicated the presence of toxicity and excessive exposure (chronic exposure) among the residents in the study area.
Previous studies have linked chronic exposure to arsenic, even at low concentrations over a long period, to an increased risk of skin, urinary, lung, bladder, liver, kidney, and prostate cancer. In addition to cancer, chronic exposure to As also poses several noncancer risks, including skin lesions (arsenicosis), cardiovascular diseases, hypertension, type 2 diabetes mellitus, liver and kidney disorders, anemia, neurological and mental disorders, respiratory problems, and liver and kidney disorders.14,17,21,23 -25,30,76 Likewise, arsenic is known to cause cytotoxicity and genotoxic effects in humans.20,77,78 Thus, chronic exposure to arsenic in the study area poses a wide range of health risks, including cancer and non-cancer risks. Among those health risks, the residents have a very high likelihood of developing arsenic-induced skin lesions, including melanosis, keratosis, and leucomelanosis, and the findings of this study are consistent with our previous study. 79 Furthermore, the presence of excessive arsenic (chronic exposure) in the studied area may increase the risk of skin, urinary, lung, bladder, liver, kidney, and prostate cancer among the residents. Apart from cancer risks, the residents in the study area are at higher risk of developing cardiovascular diseases, hypertension, type 2 diabetes mellitus, liver and kidney disorders, anemia, neurological and mental disorders, respiratory problems, liver and kidney disorders, and male infertility. Similarly, Demissie et al 46 conducted a recent study in the study area, which found that arsenic exposure through drinking water exceeds acceptable thresholds for both cancer and noncancer risks, 32 and this finding aligns with the current study. Furthermore, chronic exposure to arsenic during pregnancy presents substantial dangers for both mothers and fetuses. 80 Therefore, pregnant mothers in the study area are at higher risk of experiencing miscarriage and stillbirth during their pregnancy. Additionally, children have an increased risk of neurological dysfunction and a higher rate of infant mortality. Therefore, the likelihood of negative health consequences, including morbidity and mortality, among residents will be very high, and it is imperative to prioritize the prevention of further hazards.
The high concentration of As in nail samples among the population studied was attributed to natural and anthropogenic sources such as volcanic deposits and sediments, industrial activities, and groundwater consumption with elevated arsenic concentrations in the study area. 57 Furthermore, the mean concentration of arsenic in nail samples in this study was greater than that in studies conducted in Canada, 81 Slovakia, 82 Thailand, 61 and the USA.83,84 In contrast, these study results are lower than those reported from Pakistan,8 –20,64 Iran, 75 Cambodia, 85 and India. 63
Correlations of arsenic concentrations in urine, nails, and groundwater
This study applied Pearson’s correlation coefficient to measure the association between the log-transformed total As concentrations in urine and nails (Figure 4). Pearson’s correlation coefficient analysis revealed a significant positive correlation between urine and nail arsenic levels (r = 0.432, P < .001). This indicates that when the concentration of As in urine increases, the concentration of As in the nail also increases. A study in Pakistan’s rural community reported a strong positive correlation between the arsenic concentration in urine and nails, with a Pearson’s coefficient of 0.484 (P = 0.036). 86 Additionally, a study from arsenic-contaminated areas in Cambodia reported a positive correlation between arsenic levels in urine and nails, with a correlation of 0.297. 87 Likewise, other studies in the USA found a positive correlation of 0.36 (P = .0012) between arsenic levels measured in urine and those measured in nails. 88 Thus, the results of our study were consistent with those of previous studies.86 -88
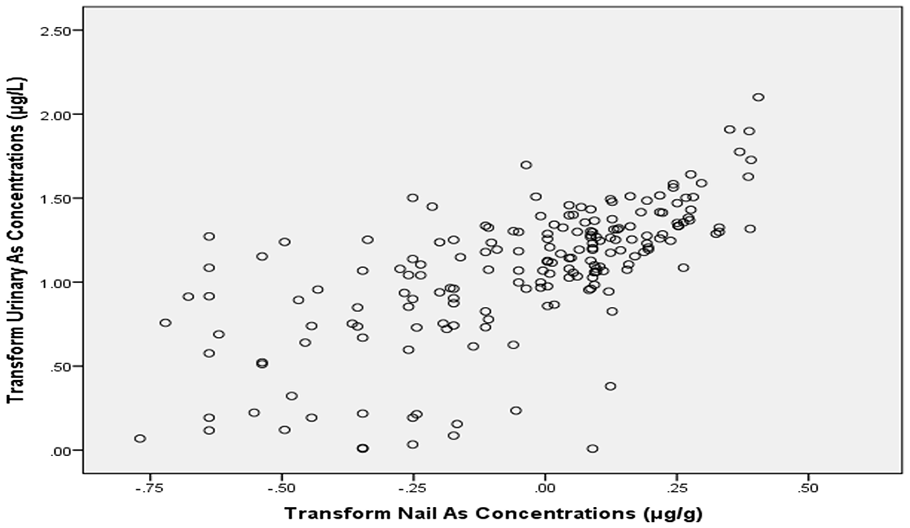
Correlation between arsenic levels in urine and nail samples.
Furthermore, the present study assessed the correlation between log-transformed urinary and nail As concentrations and As concentrations in groundwater with Pearson’s correlation coefficient analysis (Figure 5). In the present study, we found that the concentration of As in groundwater used for drinking purposes was positively correlated with both urine (r = 0.21, P = .007) and nail (r = 0.14, P = .044) arsenic concentrations; however, the observed correlation was a weak positive relationship. The R-square values of 0.21 and 0.14 indicate a 21% and 14% chance of arsenic in urine and arsenic accumulation in nails due to exposure to arsenic in water, respectively, and the relationship was statistically significant (P < .05). The correlation between As concentrations in groundwater and urinary and nail arsenic concentrations indicates that groundwater is a significant determinant of urinary and nail arsenic concentrations and the main source of As exposure. Additionally, the study results suggest that residents in the study area are exposed to As through groundwater consumption, and the potential health risk of As is of great concern among residents. The study’s results were consistent with those of studies reported from Cambodia, Thailand, Vietnam, and the USA.84,85,87,89,90

Correlation between arsenic levels in urine and nail with As concentration in groundwater.
Multiple linear regression analysis (MLR)
Determinants of urinary arsenic concentrations (short-term exposure)
Multiple linear regression analysis revealed that only 2 predictor variables were significantly associated with acute arsenic exposure. The use or consumption of groundwater (shallow or deep wells) sources and smoking cigarettes were significant predictors of acute arsenic exposure among the study population (Table 1). In contrast, sociodemographic variables such as residence, sex, age, marital status, education level, occupation, or socioeconomic status did not significantly relate to the urinary arsenic concentration (acute exposure). Similarly, the urinary arsenic concentration (acute exposure) did not significantly change with time spent at the workplace, duration spent in the study area, source of water supply (spring, piped water, or river), average water consumption per day, the practice of water treatment, vegetable gardening practice, frequency of taking showers, alcohol consumption, and chewing “Chat” or “Khat.”
Sociodemographic characteristics of the study population in Adami Tulu Jido Kombolcha District, June 2022.

This study revealed that groundwater or well water consumption was significantly associated with urinary As (β = 1.81, P = .033). This indicates that the As concentration in urine increased by 1.81 µg/L for each additional microgram per liter of arsenic intake. Thus, this study revealed that the ingestion of arsenic-contaminated water from either shallow or deep wells can increase the concentration of As in urine. Indeed, this is attributed to the fact that the arsenic concentration in drinking water is a significant predictor of acute or short-term exposure, as measured by urinary arsenic concentrations, since approximately 40% to 60% of the ingested dose is eliminated through urine within 1 to 2 days after arsenic intake. 91 Furthermore, urine is the main route of elimination for both pentavalent and trivalent inorganic arsenicals, and the concentration of total As in urine considerably increases. A recent study in the study area found elevated concentrations of As in groundwater, 57 confirming that drinking water is a significant source of arsenic exposure for the general population. Therefore, the study’s findings were coherent with the studies conducted in Italy, Chile, Thailand, and Canada.89,92 -94
The results of this study also showed that smoking cigarettes was significantly associated with urinary As concentration and acute exposure (P < .001). The results indicated that the As concentration in the urine increased with each additional daily cigarette. One study revealed that smoking cigarettes can increase the concentration of As in urine and that cigarette smokers have a significantly greater urinary arsenic concentration. This is attributed to tobacco plants absorbing natural inorganic arsenic, which is naturally present in soils, thus indirectly exposing smokers to carcinogenic metalloids. 95 A study conducted in Bangladesh found that the concentration of As in 5 different brands of cigarettes from local markets ranged between 0.13 and 0.29 μg/g, with a mean of 0.21 μg/g, while the other 3 brands had concentrations ranging from 0.24 to 0.27 μg/g, with a mean concentration of 0.25 μg/g. 96 Another study done in Japan showed that the arsenic concentration in Japanese tobacco plants was estimated to be 1 mg/kg or less in recent years. The mean arsenic level among 10 popular Japanese cigarette brands measured in Japan was 0.19 ppm, and there were no huge differences in the concentrations of arsenic among those brands. 97 The findings of this study were consistent with those of other studies conducted in Taiwan, Australia, the USA, Hungary, Romania, and Slovakia. In contrast, contradictory findings from Korea, Italy, Chile, and Thailand indicate that smoking is not significantly related to urinary arsenic concentration and does not significantly affect the concentration of As in urine.74,92,93,98
Determinants of nail arsenic concentrations (long-term arsenic exposure)
The multiple linear regression analysis showed that only 3 predictor variables were significantly associated with chronic arsenic exposure (Table 2). Using or consuming groundwater sources, smoking cigarettes, and taking a shower or bath were significant predictors of chronic arsenic exposure among the residents in the study area. However, sociodemographic variables such as residence, sex, age, marital status, education level, occupation, or socioeconomic status were not significantly related to the As levels in nails (chronic exposure), similar to those associated with acute arsenic exposure. Additionally, the As levels in the nails (after chronic exposure) did not significantly change concerning the amount of time spent at the workplace, duration of residence in the study area, source of water supply (spring, piped water, and river), average water consumption per day, the practice of water treatment, vegetable gardening practice, alcohol consumption, or chewing “Chat” or “Khat.”
Factors associated with acute arsenic exposure among the study population in Adami Tulu Jido Kombolcha District, June 2022.
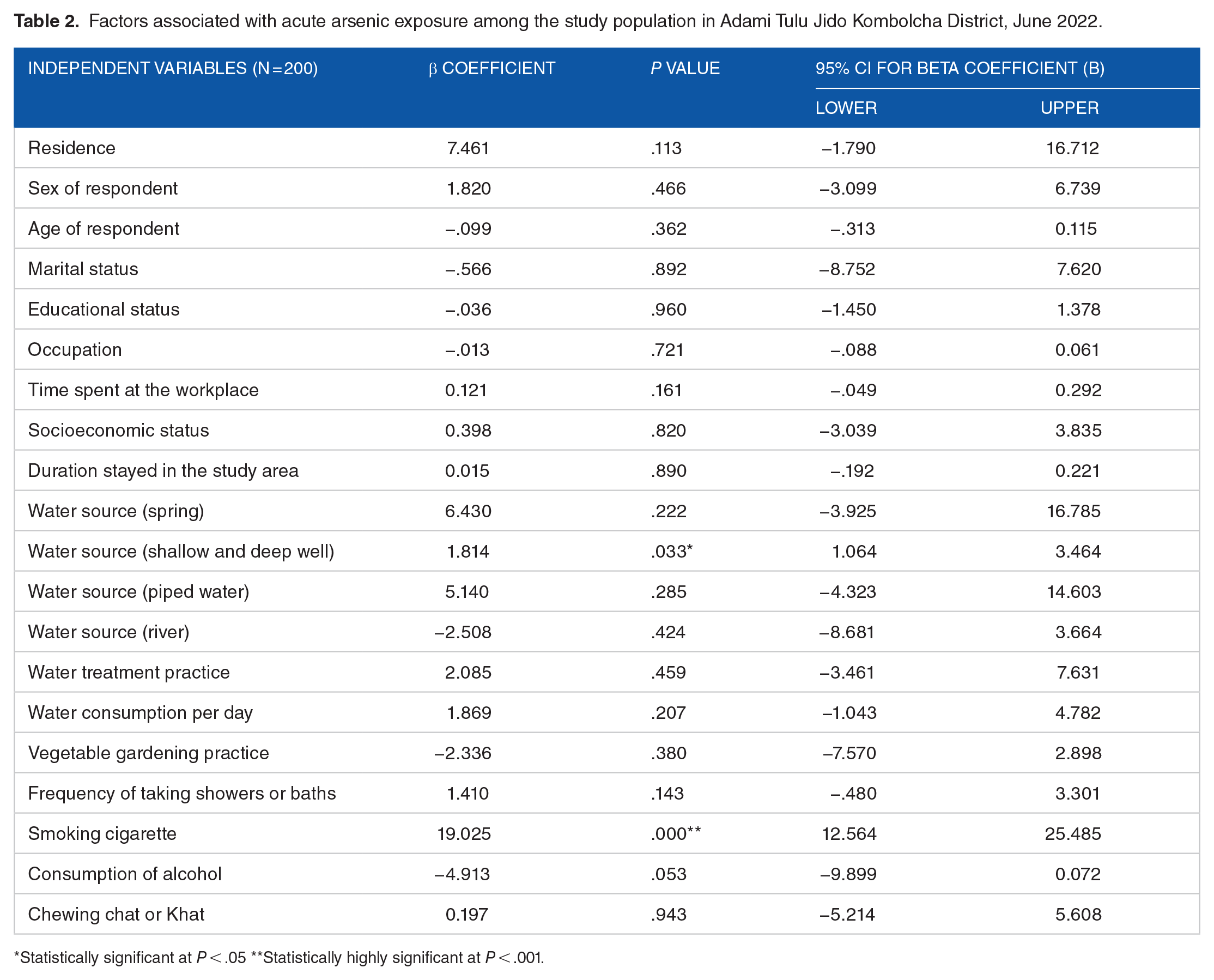
Statistically significant at P < .05 **Statistically highly significant at P < .001.
A multiple linear regression analysis revealed a significant association between the groundwater source and nail arsenic concentration or long-term arsenic exposure (P = .005). The results of this study indicate that the intake of arsenic in drinking water and As in nails also increases, and these findings are consistent with those of studies conducted in Bangladesh, Thailand, and Iran.75,99,100 This suggests that the prolonged consumption of As-contaminated groundwater may have resulted in high As accumulation in the human body. The present study also revealed a statistically significant association between the arsenic concentration in the nail or long-term arsenic exposure and taking a shower or bath (P = .019). The results of this study indicate that with an increased number of showers or baths, the nail arsenic concentration also increases, and these findings are consistent with a study conducted in Thailand. 61 This can be attributed to human exposure to arsenic occurring through skin or dermal absorption while taking showers or baths, but further confirmation is needed. Arsenic exposure through showers or baths is primarily a concern when the water used for bathing is contaminated with arsenic. When bathing or showering with water containing arsenic, there is a potential for exposure through inhalation of steam or aerosolized water droplets, as well as through skin contact. Nevertheless, the level of exposure is contingent upon other circumstances, including the concentration of arsenic in the water, the duration and frequency of contact, and individual factors such as skin condition and bathing habits. 101 The associations between taking a shower or bath and nail arsenic concentration or long-term exposure to As are not well-established in the literature. Additional comparisons with other studies are needed, and further confirmation is needed. Thus, the relationship between the frequency of taking a shower or bath and nail arsenic concentration (long-term exposure) requires further research.
A multiple linear regression analysis also showed that smoking cigarettes was significantly associated with nail arsenic concentration or past exposure (P = .002). The interpretation indicates that the As concentration in the nail increased for each additional daily cigarette. The study revealed that smoking cigarettes can increase the concentration of As in nails and is associated with chronic or long-term arsenic exposure. Therefore, the findings of this study were consistent with a study conducted in Japan. 97 However, the association was not observed in another study conducted in the USA, Iran, and China.44,75,102,103 This is attributed to tobacco or cigarettes containing arsenic, and smokers inhale some arsenic while smoking cigarettes or tobacco and being exposed to As.
According to the WHO, cigarette smokers may also be exposed to the inorganic arsenic found in tobacco, while tobacco plants can absorb arsenic naturally occurring in the soil (WHO, 2022). A previous study reported that smoking cigarettes contain some amount of arsenic, and an estimated 0.25 μg of arsenic is consumed after smoking a single cigarette. 104 Additionally, another study reported that the mean As concentration in tobacco was 0.15 μg/g (range <0.02–2.04 μg/g), while it was 0.11 μg/g in cigarettes (range <0.02–0.71 μg/g). 105 However, to the best of our knowledge, there are no published articles or reports in the literature on the levels of As in Ethiopian tobacco leaves or different brands of commercially available cigarettes. Therefore, smokers may be exposed to As either from smoking cigarettes (tobacco) or from ingesting water contaminated with arsenic, 95 and they may face the double burden of arsenic exposure. Additionally, the risk of lung cancer is increased by smoking cigarettes or tobacco products in addition to being exposed to arsenic from contaminated water. It has also been observed that reducing arsenic exposure lowers the risk of lung cancer in smokers and vice versa. 95 However, the risk of smoking varies from individual to individual according to the duration and frequency of smoking, the type of tobacco or cigarette smoking, the mode of administration, and the ability of the individual to remove carcinogens 106 (Table 3).
Factors associated with chronic arsenic exposure among the study population in Adami Tulu Jido Kombolcha District, June 2022.
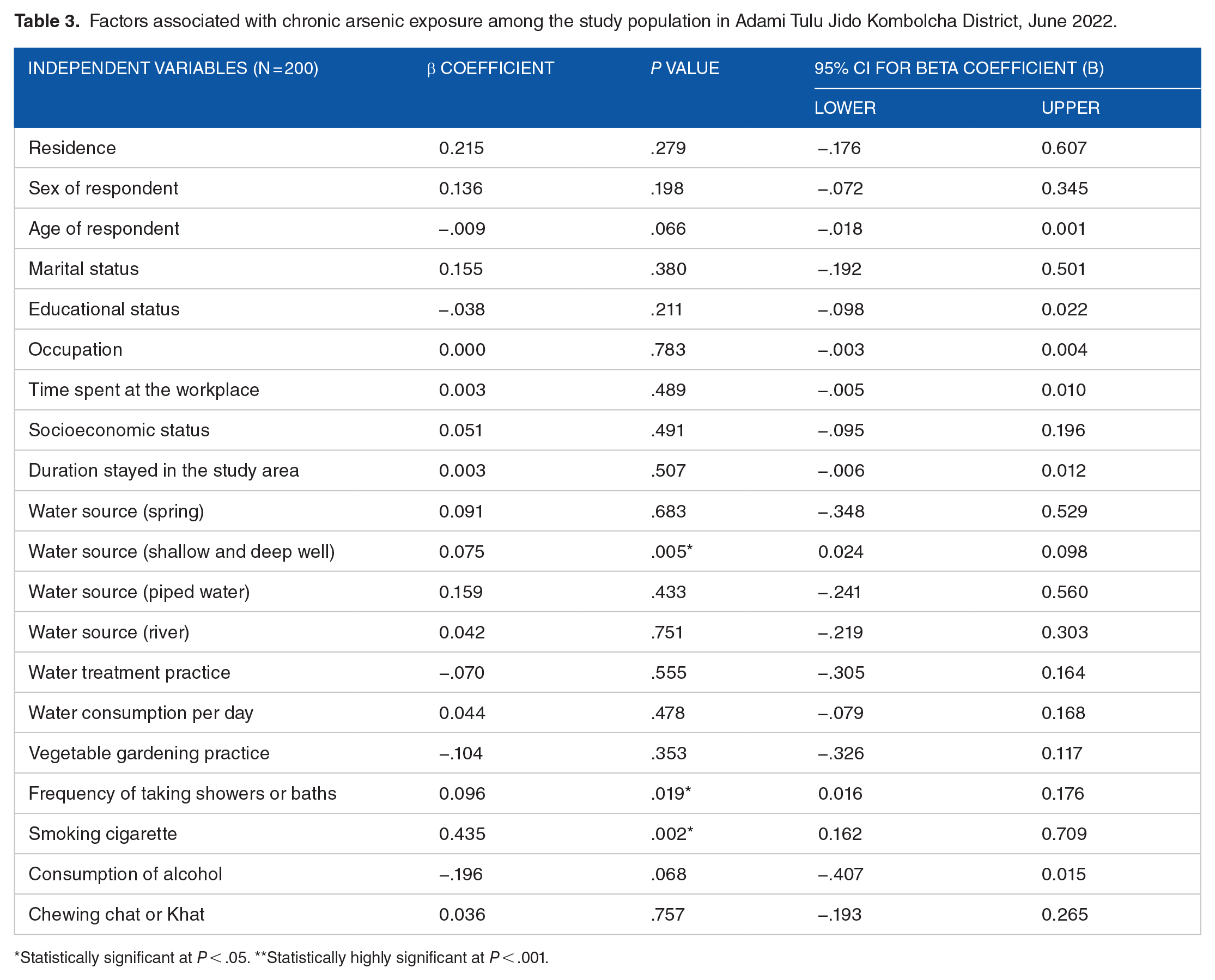
Statistically significant at P < .05. **Statistically highly significant at P < .001.
Strengths and limitations of the study
There are several major strengths in the current study. First, the study assessed acute and past exposure to As using the most preferable and reliable indicators (urine and nail biomarkers) and associated factors. The present study investigated acute and chronic exposure to As among residents in the study area and assessed the relationships between arsenic concentrations in urine and nail samples as biomarkers and between arsenic concentrations in groundwater sources with an adequate sample size. Also, we quantified the levels of arsenic in urine and nail specimens using the ICP-MS, known for its superior sensitivity, durability, precise measurements, and extensive linear range. Additionally, the USEPA classified the ICP-MS instrument among the accepted analytical methods for determining arsenic. Due to the limitations of the present study, we measured only the total arsenic concentration in urine and nail samples, and speciation of As into organic and inorganic forms was not performed; moreover, speciation of arsenic may provide valuable information on the sources of arsenic exposure.
Conclusions and Recommendations
This study assessed acute and chronic exposure to arsenic using urine and nails as body biomarkers and associated factors among the study population in Ethiopia. The study’s results indicated that most participants exhibited measurable levels of arsenic in their urine and nails. This suggests that both acute and chronic exposure to arsenic are prevalent in the study area, highlighting the significance of arsenic toxicity and the need for attention to its potential health impacts. Long-term exposure to arsenic, even at low and moderate concentrations, can increase the risk of cancer and noncancer diseases, which is indicative of the presence of toxicity and may be a good indicator of negative health effects among the residents in the study area. Moreover, excessive and toxic chronic exposure to arsenic may have subclinical effects on the residents in the study area, increasing their risk of both cancer and non-cancer health risks. It is crucial to pay special attention to preventing further risks in this regard. Our study revealed a positive correlation between arsenic concentrations in groundwater and urinary and nail arsenic concentrations. Also, we observed a significant correlation between urinary and nail arsenic concentrations within the study area.
Furthermore, the findings of this study confirmed that drinking water wells, both shallow and deep wells, and smoking cigarettes were significantly associated with urinary arsenic concentrations or acute arsenic exposure. In contrast, drinking water wells, smoking cigarettes, and taking showers were significantly associated with nail arsenic concentrations. These findings emphasize the importance of addressing the sources of arsenic exposure, particularly through groundwater consumption, smoking, and personal hygiene practices, to mitigate the health risks associated with arsenic in the study area. Another interesting finding in the present study was that groundwater sources and smoking cigarettes were determinant risk factors for acute and chronic arsenic exposure. Therefore, it is crucial to prioritize the residents in the study area and make additional efforts to prevent acute and chronic arsenic toxicity. To this end, the findings from this study may provide concrete scientific data or valuable information for governments, nongovernmental organizations, UN agencies, researchers, and policymakers.
Footnotes
Acknowledgements
The authors express their gratitude to the research team, study participants, and Adami Tulu Jido Kombolcha Water and Health Office. In addition, we express our gratitude to Henok Mulugeta, Teklu Gadisa, and Fire Chewaka from the Ethiopian Food and Drug Authority for their unwavering assistance throughout the laboratory work.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
CRediT Authorship Contribution Statement
Ethical Approval
The study received ethical approval from Addis Ababa University (CNCSDO/667/14/2022).
Data Availability Statement
The data will be made available upon request.