
Abstract
Background:
Knowledge about community awareness and practices related to a disease, among other things, helps to plan relevant control strategies. This study assessed the knowledge, attitude, and practices (KAPs) of the community in Abobo district of Gambella Regional State in Southwestern Ethiopia about urogenital schistosomiasis (UGS), which is endemic to the region.
Methods:
A community-based cross-sectional study was conducted in 2022. A pretested structured questionnaire was administered. Multivariable logistic regression was used to examine factors associated with KAPs variables.
Results:
Most study participants (90.6%) responded they have previously heard of UGS. Over 95% of the participants knew at least 1 symptom of UGS and 30% knew the transmission cycle. About 15.9% and 26.8% knew keeping environmental hygiene and refraining from using cercariae infested water, as preventive methods, respectively. Over half of the participants (50.1%) disagreed or did not know that urinating close to the river/dam water contributes to transmission, and almost all participants had contact with the dam/river water in one way or another. Education status and history of having the infection were the key significant correlates of most KAPs variables.
Conclusion:
Most of the community members had poor knowledge and attitudes about the mode of transmission and preventive measures of UGS. Thus, besides school-based mass drug administration (MDA), UGS control efforts in the region should incorporate health education in conjunction with safe water supplies, and provision of sanitary facilities to effectively reduce the transmission of the disease.
Introduction
Schistosomiasis is one of the neglected tropical diseases (NTDs) caused by blood flukes of the genus Schistosoma. There are 6 main species of Schistosoma that can infect humans, namely Schistosoma haematobium, S. mansoni, S. japonicum, S. mekongi, S. intercalatum, and S. guineensis. Schistosomiasis is estimated to affect over 220 million people globally, with an annual mortality rate of approximately 11 792. 1 Sub-Saharan Africa bears the highest burden of the disease, with 90.6% of individuals requiring treatment.2,3
The World Health Organization (WHO) has targeted schistosomiasis for elimination as a public health problem by 2030. 4 To achieve this goal, the WHO strategies include preventive chemotherapy of at-risk groups, increasing access to safe drinking water, and improved sanitation, hygiene education, environmental improvement and intermediate host control.2,3
Schistosomiasis is one of the NTDs that the Ethiopian Federal Ministry of Health has designated as a priority for control and elimination. 5 According to a national survey of the country, 6 265 districts are endemic for schistosomiasis, and 14 million school-age children need regular deworming through mass drug administration (MDA) campaigns. Intestinal schistosomiasis caused by S. mansoni is widely distributed in Ethiopia, including Addis Ababa,6,7 whereas UGS caused by S. haematobium has been known to occur in lower areas below 800 m above sea level in Afar (Amibara district), Gambella (Abobo district ), Somalia (Afder Gode zone) and Benishangul Gumuz (Kurmuk district) regions.6-11 However, despite the high burden of UGS in Ethiopia, there is limited information on the community’s KAPs regarding the disease and its prevention and control mechanisms.
MDA in Ethiopia was launched in 2015 to control helminths infection-associated morbidity by reducing moderate-to-heavy intensity infections. In addition, the NTD sector, which focuses on preventive treatment, and the Water Sanitation and Hygiene (WASH) sector have been established to break parasite transmission and reach elimination.6,12 Although these interventions have been implemented in several endemic areas, their coverage, effectiveness and sustainability are still uncertain and need to be evaluated. Similar to other schistosomiasis endemic areas in Ethiopia, Gambella is one of the Ethiopian regions where MDA is applied. It is essential to assess the community’s awareness, practices, and perceptions of the disease in order to evaluate the effectiveness of the control measures and to design complementary prevention and control methods. No previous study has investigated KAPs of UGS at the community level in Abobo. Therefore, this study aimed to investigate KAPs of the community on schistosomiasis in the Abobo district, Gambella, Ethiopia.
Methods
Study area and population
The study was carried out among the Abobo community in Gambella Regional State, Southwestern Ethiopia. Abobo is located at 7°51′0″ North, 34°33′0″ East, and approximately 822 km southwest of Addis Ababa (Figure 1). Its altitude ranges from 650 to 1337 m above sea level. According to 2022 regional office demographic data, the population of the Abobo was 28 661, of whom 14 043 were males and 14 618 were females. The major economic activities of the community are agriculture and fishing. The Alwero River traverses Abobo Town and is used for washing clothes, bathing, occupational and recreational purposes.

Map of Gambella, showing the study area.
As per the health authorities of Abobo, the implementation of school-based (MDA) for bilharzia, along with soil-transmitted helminths, has been carried out annually since 2016, except for the first year of the COVID-19 pandemic.
Study design and sample size
A community-based cross-sectional study was conducted in August 2022 in the Abobo district, Gambella, Ethiopia. The sample size was determined using the formula n = (zα½)2 p(1 − p)/d2, 13 assuming a 95% confidence interval, marginal error (d) = 5%, and a proportion of 50%, was used since no similar study conducted in the community and 5% non-respondent. Accordingly, a total of 403 samples were taken.
Sampling procedure
Based on the endemicity to S. haematobium infection11,14 and their reliance on the Alwero dam reservoir, Villages 5 and 6 and Abobo town were chosen for the study. A random sampling technique with proportional allocation was used to select the households. House heads were interviewed in each house, and in the absence of the household head, an individual whose age was at least 12 years old was interviewed.
Data collection methods
Data were collected using a structured pretested self-administered questionnaire. The questionnaire addressed demographic characteristics, the level of awareness, knowledge (symptoms, mode of transmission, prevention, and control), attitude, and practices toward schistosomiasis. Questionnaires were mainly structured questions with single or multiple responses, incorporating “I don’t know” and “other” options to reduce guessing and also supported by an open-ended question to capture participants’ perspectives regarding the prevention and treatment of schistosomiasis. The questionnaire was developed in English, later translated into Amharic, and administered in Amharic and the local language, “Anuak language,” using trained persons who speak the local language. In the course of the assessment, direct observations were made concerning the open-water contact behavior of the inhabitants, the presence of Bulinus snails and human wastes by the dam side.
Data processing
A correct answer to a question was given one point and a wrong answer or a “do not know” response was given zero point. All correct points were then added up to get the total score, amounting to 24, 2, 2, and 5 points for knowledge, attitudes, treatment-seeking practice, and risky practice (open water contact practice and urinating in an open field/bush/by open water), respectively.
Data analysis
The collected data were entered in Excel and analyzed using IBM SPSS version 23. Descriptive statistics was used to summarize the data. A multivariable logistic regression was used to examine the associations of demographic factors and past infection with KAP variables. Odds ratios (OR) at 95% confidence intervals (CI) were computed. A P-value of less than .05 was considered statistically significant.
Ethical considerations
The study protocol was approved by the Institutional Review Board (IRB) of the Aklilu Lemma Institute of Pathobiology, Addis Ababa University (ALIPB IRB/13/2019/20). Permissions were also obtained from the Gambella Zone Health Bureau and the district authority. Participants in the study received detailed information about the research objectives, potential benefits and risks, and procedures. To ensure their understanding and willingness to participate, written and verbal informed consent were obtained from participants. For participants under age 18, informed consent was also obtained from their parents/guardians.
Results
Socio-demographic characteristics of the study participants
Among the 403 participants, 308 (76.4%) were males and 95 (23.6%) were females. The survey involved conducting interviews with individuals present in the house during the research. It was noted that household heads, mostly men, were considered as the representatives, leading to a higher level of male participation in comparison to females. The participants ages ranged from 12 to 90 years, with a mean (SD) of 35.107 (11.88) and a median of 32.0. Of the 403 participants, 178 (44.2%) were farmers, while 136 (33.7%) were government or private employees. Additionally, 239 (59.3%) attended school either at the primary (57/23.8%), secondary (68/28.5%), or college/university (144/60.3%) levels (Table 1).
Socio-demographic characteristics of the study participants in Abobo district, Gambella, Ethiopia.
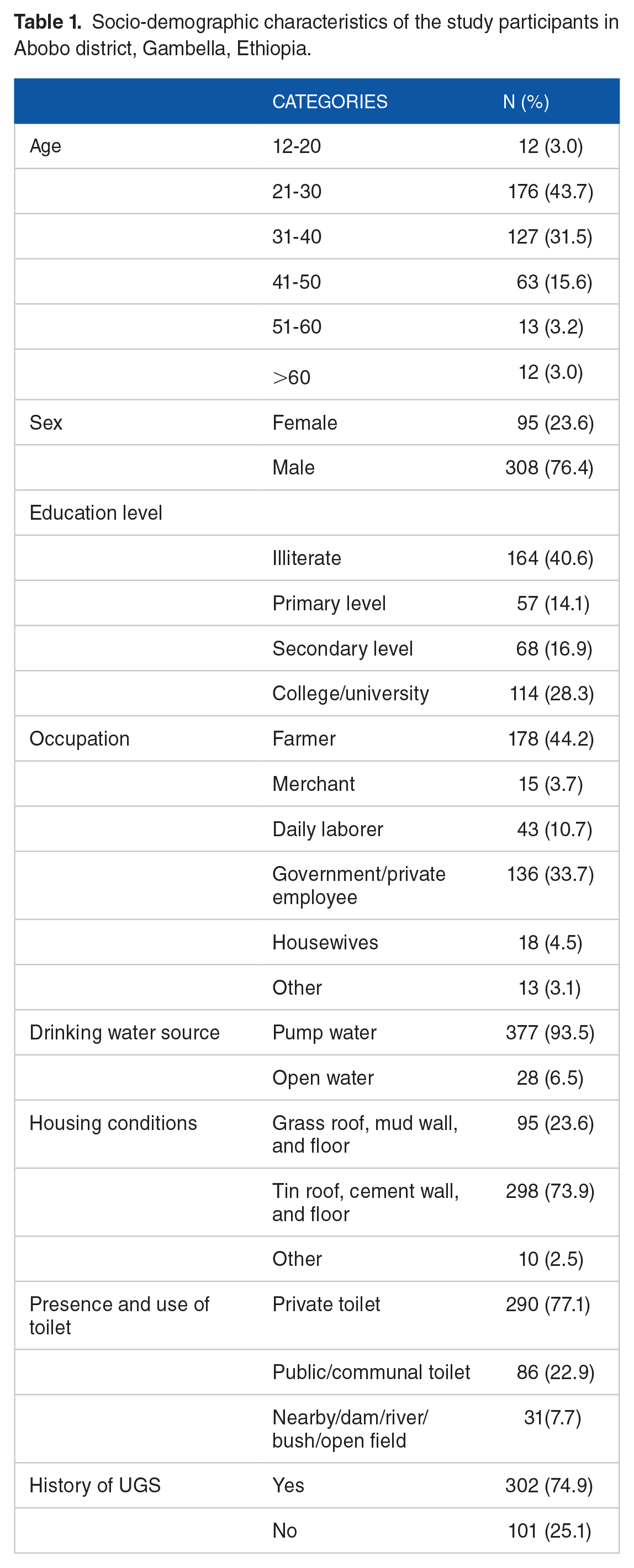
Out of 298 residential houses visited, most (73.9%) were made of tin roofs, cement walls, and floors, while a smaller percentage (23.6%) had thatched roofs, mud walls, and floors. Around 376 participants (93.3%) had access to toilets, with 290 (77.1%) having toilets in their own homes and 86 (22.9%) using public toilets. About 377 (93.5%) used public hand pumps for drinking water, while the remaining 6.5% relied on open water sources. More than 50% of households have a history of schistosomiasis affecting at least one of its household members (Table 1).
Urogenital schistosomiasis and mass drug administration (MDA) awareness
It was found that, out of 403 participants, 90.6% (365/403) were aware of schistosomiasis and for half of the participants (52.1%) a health institution was the main source of information. Over 81% of the participants were aware of the MDA program and 66.5% admitted that children in their families had taken drugs from this program (Table 2).
Knowledge of participants on symptoms, transmission, prevention, and control mechanisms of Schistosomiasis, Abobo district, Gambella region, Ethiopia.

Othera Ingesting spoiled food, contaminated soil and unhygienic hand.
Otherb Drinking dam/river water and nothing.
More than one answer is possible.
Knowledge of symptoms and mode of transmission of schistosomiasis
Most participants (96%) who had heard about schistosomiasis were able to mention at least one symptom of UGS. The major symptom mentioned by the participants is bloody urine (81.9%), followed by a burning sensation during urination (13.4%). Regarding the transmission pathways, only 107(28.7%) of the respondents knew skin penetration as a means of infection and only 71(19.5%) knew of snails role in the transmission. Over half of the participants (54.0%) responded that they didn’t know the involvement of the vector in the infectious process and 59.6% of respondents pointed out drinking unclean water as a way of getting an infection. Most participants recognize at least one way of open water contact activity leads to contracting the disease. However, only 0.3% of participants knew that all forms of infested water contact practice as a source of infection (Table 2).
Knowledge about prevention and control measures against schistosomiasis
Among those who stated that UGS is preventable (92.6%), the most frequently mentioned correct prevention or control measure was getting treatment (32.9%), followed by avoiding any open water contact behavior (26.8%), while 5.2% of respondents misconceived the prevention mechanisms. On the other hand, modern medicine (going to a health facility and getting treatment) was the most noted cure option mentioned by the participants (84.2%). Only 2 participants mentioned treatment to all people (MDA), as a prevention strategy (Table 2).
Attitude and practices of participants toward schistosomiasis
Among the participants who were aware of schistosomiasis, nearly two-thirds (236/365), perceived UGS as a deadly disease, and half of the respondents only agreed urinating on exposed water as the origin of the infection (Table 3).
Attitude, risky and treatment-seeking practice of participants toward schistosomiasis, Abobo district, Gambella region, Ethiopia.

Abbreviation: N, number of respondents.
More than one answer is possible.
Regarding the risky behavior, out of the total of 403 participants, it was found that 347 (89%) respondents had swimming/playing habits in open water, 357 (88.6%) respondents used dam water for domestic purposes (washing clothes or bathing) and 31 (7.7%) respondents, used outdoor places, including by open water, as frequently means of urination and excretion.
The majority of respondents (86.1%) sought modern treatment at the time of infection (Table 3).
Level of knowledge, attitude and risky practice
The mean score for knowledge was 8.19 out of 24 points, or 34.1% level of knowledge, with a minimum score of 4 and a maximum score of 15. The most frequent score (mode) was 9. The attitude mean score was 1.04 out of 2 points. The mean score on risky practice was 1.97 out of 5 points. Of the 403 individuals, 324 (80.4%) were involved in at least 2 risky practices (ie, mode = 2).
Association of participant’s knowledge, attitudes and practices about schistosomiasis with their sex and age
Compared to female participants, male participants exhibited a higher likelihood of being informed about schistosomiasis (P = .046) and a lower tendency to engage in indiscriminate urination or defecation (COR: 0.5, CI: 0.2-0.9). However, male respondents demonstrated a proclivity for swimming or playing in open water (COR: 2.4, CI: 1.3-4.4) and were less inclined to acknowledge that all forms of open water contact, including washing, swimming, bathing, and crossing the river barefoot, can lead to contracting the disease (COR: 0.2, CI: 0.1-0.8).
Participants with an age greater than 40 years were more likely to know snail as an intermediate host (COR: 2.5, CI: 1.4-4.4) but less likely to perceive UGS as a fatal disease (COR: 0.5, CI: 0.3-0.9), compared to study population less than or equal to 40 years of age.
Multiple logistic regression analyses showed that individuals over the age of 40 were found to be key predictors for knowing the snail as an intermediate host and for exhibiting less agreement about the fatality of the UGS; on the other hand, being male (sex) continued to be the primary indicator for lack of understanding about the risks associated with unsafe freshwater contact as a means of contracting the parasite (P < .05) (Table 4).
Multivariable analysis of participants knowledge, attitude and practice about schistosomiasis with respect to sex and age.

Abbreviation: AOR, adjusted for occupation status, education status, and history of schistosomiasis.
Association of participant’s knowledge, attitude and practices about schistosomiasis with their education and occupation status
Compared to non-educated participants, educated participants had a higher likelihood of recognizing painful urination (COR: 3.8, CI: 1.7-8.3) as a symptom of UGS, as well as identifying swimming or playing in open water as an exposure factor (COR: 2.1, CI: 1.3-3.4), getting treatment (COR: 1.7, CI: 1.1-2.6), and valuing health education (COR: 3.1, CI: 1.3-7.7) as a prevention measure.
Respondents with formal education are more likely to perceive urinating in an open field, by bush, or near open water as a source of transmission (COR: 2.7, CI: 1.6-4.6) and they are also less likely to use dam water to wash clothes (COR: 0.6, CI: 0.4-0.9) compared to non-educated ones.
On the other hand, working participants were 3 times more informed about MDA (COR: 3.0, CI:1.2-7.2) and schistosomiasis (COR: 3.8, CI:1.4-10.4), and know hematuria as a symptom (COR: 2.8, CI:1.2-6.5). Additionally, working individuals are less likely to engage in open defecation or urination (COR: 0.2, CI: 0.1-0.4) compared to non-working respondents. In terms of attitudes, working people also perceive UGS as a potentially fatal disease (P < .05) in contrast to non-working people.
Multiple logistic regression analyses showed that formal education was a significant predictor for all associated factors (P < .05). Additionally, employment status remained a significant factor for perceptions of UGS as a fatal disease and a reduced likelihood of engaging in unselective urination or defecation (P < .05) (Table 5).
Multivariate analysis of participants knowledge, attitude and practice about schistosomiasis with respect to education and occupation status.

Abbreviation: AOR, adjusted for age, sex, history of schistosomiasis.
Working group: farmers, merchants,employees and daily laborer.
Association of participants knowledge, attitude and practices about schistosomiasis with a history of schistosomiasis
Participants with a history of UGS were found to have a higher likelihood of being aware of schistosomiasis (COR: 5.5, CI: 2.7-11.6) and MDA (COR: 3.6, CI: 2.1-6.0) compared to those without a history of UGS. Additionally, they exhibited better knowledge regarding hematuria (COR: 2.4, CI: 1.5-3.8), snails (COR: 2.2, CI: 1.2-4.1), and the importance of avoiding unsafe water (COR: 1.6, CI: 1.0-2.6). On the other hand, individuals who had been infected with UGS were less likely to agree that indiscriminate urination in open water contributes to the spread of schistosomiasis. Furthermore, they were more likely to swim or play in open water (COR: 6.3, CI: 3.4-11.7) than their counterparts.
In Multiple logistic regression analyses, past infection history continued to be significantly predictive for all factors, as it was in one-to-one analysis (P < .05) (Table 6) (Additional File.1). Participants who had a history of schistosomiasis showed higher odds of hearing about schistosomiasis (AOR: 3.6, CI: 1.6-8.0) and MDA (AOR: 2.4, CI: 1.4-4.2); knowing about hematuria as a symptom (AOR: 1.8, CI: 1.0-3.0) and avoiding unsafe water (AOR: 1.9, CI: 1.0-3.3) as prevention mechanisms, in comparison to those without any previous infection history.
Discussion
A detailed understanding of the factors affecting community members’ knowledge, perceptions, and preventative and control practices is crucial for effective and long-term disease control. 15 Community-based research is essential in developing a strong foundation for successful interventions against schistosomiasis. 2 Therefore, we looked at the specific knowledge or needs of the community in relation to UGS. Our study offers important insights into the KAPs of the community in Abobo, one of the UGS endemic areas in Ethiopia, with prevalence ranging from 22.2% to 35.9%.11,14 Our study revealed that the community had a high level of awareness but a low level of knowledge, attitude and practices regarding UGS.
The level of prior knowledge pertaining to schistosomiasis among community members was found to be high (90.6%). The awareness level of schistosomiasis in our study area was higher than in some other regions of Ethiopia, such as Benishangul Gumuz, 16 where the disease is prevalent but not recognized by the community. This finding aligns with other studies conducted in Africa,17-22 which have also examined community-level knowledge regarding schistosomiasis. Furthermore, a significant proportion of the study participants (81.1%) demonstrated the ability to recognize hematuria as a primary symptom of UGS. The observed high level of prior awareness and familiarity with bloody urine in this study might be explained by past infection history, as it was found to be a significant contributor (P < .05) to hearing and knowing the symptoms of UGS.
On the other hand, the participants’ level of knowledge regarding S.haematobium transmission was inadequate. They were unaware of how the parasite enters the body, the role of snails in the disease’s lifecycle, and how unsafe contact and unhygienic activities in freshwater can lead to the disease. These knowledge gaps were also identified in previous studies, such as in Gabon, 18 where the mode of transmission was not identified despite high awareness and recognition of hematuria as a symptom. Similarly, in South Africa, Sacolo-Gwebu et al 20 reported that respondents had the least recognition of the transmission cycle, despite a higher level of awareness and knowledge of the symptoms of schistosomiasis. The lack of knowledge regarding the transmission pathways of UGS could potentially increase exposure and transmission of the parasite, leading to higher infection and morbidity rates within the community.
It was also noted that there was insufficient knowledge and attitude toward the prevention methods of UGS. This included inadequate awareness about maintaining environmental hygiene (15.9%), avoiding open water contact (26.8%), and failure to recognize open-air urination as a potential source of water contamination (49.6%). Other studies on KAPs related to schistosomiasis also identified this lack of comprehension despite a high level of awareness.19,22-24 It is crucial to address this issue as without comprehensive knowledge, the infection will persist and hinder effective control of schistosomiasis. 20 To improve the knowledge level of prevention and control measures against UGS, it is essential to provide more health education and promotion activities, such as community meetings, radio programs, posters, and leaflets, that emphasize the role of skin penetration, snail vector, and MDA in the transmission and prevention of the disease.
Furthermore, as seen in other studies,18,20,24-28 drinking contaminated water is misunderstood as a mode of transmission, and avoiding it is thought to be a means of prevention. Some participants also believed that removing stagnant water, avoiding sunlight exposure, and minimizing contact with infected individuals could effectively prevent the spread of the disease. These misconceptions and inadequate understanding of the prevention and transmission cycle of the disease highlight a lack of health education and promotion of preventive measures in the research area.
Even though our data showed the community’s primary drinking water sources are public hand pumps, for other essential activities such as washing, bathing and recreational purposes such as swimming and playing, the community relies on dam/river water, as previously reported. 29 Additionally, a considerable number of participants frequently practice open-air urination and defecation, which could lead to the persistence of schistosomiasis in the area. Hence, it is imperative to develop integrated control strategies to break the transmission cycle effectively. 3
Interestingly, the study participants had appreciable health-seeking practices, as more than 81% sought out medical treatment at the time of infection. Similar trends were reported in Yemen 25 and Gabon 18 , as 81.1% and 78.2% of participants sought medical care in health institutes, respectively. Our analysis of respondents attitudes about the disease also revealed that 65% of them thought UGS to be a fatal disease, which likely contributes to their inclination to seek treatment in healthcare facilities. This practice and attitude are highly beneficial and should be encouraged to interrupt transmission and prevent the occurrence of complications. 24
Moreover, the present study showed a significant level of public awareness regarding school-based MDA, as 81.1% of participants exhibited familiarity with the initiative. This surpasses the awareness reported by Assefa et al 16 in the Benishangul Gumuz region of Ethiopia. Additionally, two-thirds of the study participants acknowledged that their families had received drugs through this program, which is also higher than the reported rates of praziquantel drug distribution in Mozambique (9%) 17 and Gabon (10%). 18 This observation may show a more effective advocacy of the program in the area and/or could be attributed to consistent MDA campaigns conducted over the years.
In relation to factors associated with KAP variables, persons who were formally educated demonstrated greater awareness of symptoms (such as dysuria), prevention methods (such as receiving treatment and health education), and risky behaviors (such as swimming or playing in exposed waters). Additionally, they also acknowledged that urinating or defecating near water sources could contribute to the transmission of the disease. This highlights the importance of education in equipping communities with the necessary knowledge and attitudes toward the disease. 27 This is consistent with findings from a study conducted in Yemen, 25 where respondents’ knowledge of various KAP variables was strongly correlated with their educational attainment. Similarly, in Nigeria, 28 individuals with formal education exhibited greater awareness of contaminated water as a source of schistosomiasis and deworming as a preventative measure. Additionally, Koffi et al 24 found that participants with higher levels of education were more knowledgeable about burning urination as a symptom and the risks of swimming in rivers. On the other hand, gender was only associated with having less knowledge about open water contact as a means of contracting the disease, as male respondents were less knowledgeable than female respondents (P < .05). This may also explain why males engage more in swimming or playing habits in freshwater than female participants, as knowledge is the foundation and a key factor influencing people’s attitudes and practices. 30 Similarly, a previous study conducted near Alwero Dam reported that males tended to have more frequent contact with freshwater than females. 29 Age, occupation, and infection history were also factors that influenced participants knowledge, perception, and risky or safe practices in the research region, consistent with previous studies.23,28
Understanding the dynamic interaction of diverse factors in varying contexts is a complex task, 15 nevertheless, this study enabled us to identify both protective and risk factors associated with KAPs regarding UGS. This understanding of the health behavior of the target population holds the potential for informing the development of future interventions, particularly the creation of appropriate educational messages tailored to the community.
Study limitations
Given that the study was conducted as a cross-sectional analysis, causal inferences could not be made from the results reported.
Conclusion
Despite the fact that most study participants had heard of schistosomiasis, knowledge among participants regarding the disease’s transmission mechanisms and methods of prevention and control were inadequate, and the majority of participants also engaged in risky practices that would expose them to the infection and contribute to the spread of UGS in the district. The lack of wells-equipped pumps in every household and alternative water sources for their domestic uses, certainly forced the community to be exposed to snail-infested water. Therefore, to effectively limit the unsafe practices, availing an additional water source and improving sanitation and hygiene (WASH) should be a priority and strengthen in the region. In addition, health education and community dialog should be organized in the region to dispel misconceptions about the prevention and control measures of UGS. Therefore, besides MDA, multifaceted approaches addressing both infrastructure, health education and community engagement will be essential to reduce ongoing UGS transmission in this population.
Supplemental Material
sj-docx-1-ehi-10.1177_11786302241234731 – Supplemental material for Assessment of Urogenital Schistosomiasis Knowledge, Attitudes and Practices Among Abobo Communities in Gambella Regional State, Southwestern Ethiopia
Supplemental material, sj-docx-1-ehi-10.1177_11786302241234731 for Assessment of Urogenital Schistosomiasis Knowledge, Attitudes and Practices Among Abobo Communities in Gambella Regional State, Southwestern Ethiopia by Tigist Mohammed, Abraham Degarege, Mulugeta Aemero, Abebe Animut, Yohannes Negash and Berhanu Erko in Environmental Health Insights
Footnotes
Acknowledgements
We are grateful to the Abobo district administrations for providing the required information. We also want to express our gratitude to Mr. Bekegna Samson and Mrs. Zenebech Alname for facilitating the data collection, as well as to all of the study communities’ residents for their cooperation and involvement.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported as a side issue with funds from the College of Public Health at the University of Nebraska Medical Center through the Innovation Fund.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
TM and BE conceived the study. TM analyzed the data and wrote the first draft, BE, YN, AD, AM, and MA reviewed the manuscript and all authors approved the final version of the manuscript.
Availability of Data and Materials
The corresponding author will provide the dataset used in the current study upon reasonable request
Ethical Approval and Consent to Participate
The study protocol was approved by the Institutional Review Board (IRB) of the Aklilu Lemma Institute of Pathobiology, Addis Ababa University (ALIPB IRB/13/2019/20). Permission was obtained from the Gambella Zone Health Bureau and the respective district authority. Participants were informed about the objective of the study and written and verbal informed consent was obtained from the participants. For participants under the age of 18 informed consent was obtained from a parent and/or legal guardian.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.