
Abstract
The coronavirus disease 2019 (COVID-19) is a respiratory disease caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), but whether the asthmatic patients are at increased risk for severe COVID-19 illness than non-asthmatic patients has remained unclear. This scoping review aimed to assess the available evidence to determine if asthmatic patients are at a higher risk for severe COVID-19 illness. Searching several electronic databases and adhering to the PRISMA guidelines, we conducted a scoping review of 70 articles and using defined inclusion-exclusion criteria, 21 articles were analyzed in-depth and included in this scoping review. The findings of this scoping review point to a lack of relationship between asthma and severe COVID-19 illness. While a limited number of studies (n = 4) identified asthma as a risk factor, most studies (n = 17) found no independent association between asthma and severe COVID-19 illness. We, thus, conclude that asthma may not be a potential risk factor for severe COVID-19 illness. Owing to limited evidence, we recommend large-scale prospective cohort studies with standardized methodologies to decipher potential role of asthma in COVID-19 severity. Further, understanding the impact of specific asthma medications, genetic factors, and other comorbidities on COVID-19 outcomes may help inform clinical practice guidelines for effective patient health management.
Highlights
• The global burden of asthma and COVID-19 is overwhelming.
• If asthmatic patients are at increased risk for severe COVID-19 illness is unknown.
• A scoping review was conducted to assess the link between asthma and COVID-19.
• The findings point to a lack of relationship between asthma and severe COVID-19 illness.
• Future large-scale prospective cohort studies may help decipher potential link between asthma and COVID-19.
Introduction
In December 2019, the appearance of the novel severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) in Wuhan, China, 1 triggered a global pandemic of coronavirus disease 2019 (COVID-19) that has since caused significant morbidity and mortality, contributing to nearly 700 million cases and 7 million deaths, globally (https://www.worldometers.info/coronavirus/). COVID-19 is a viral respiratory illness caused by SARS-CoV-2. 2 The transmission of SARS-CoV-2 occurs primarily through respiratory droplets, including direct contact, droplet transmission, and airborne transmission. 3 Vulnerable populations, particularly the elderly and individuals with underlying medical conditions, have been identified to be at a higher risk for severe COVID-19 illness. 4 The Centers for Disease Control and Prevention (CDC) has highlighted various health conditions, such as cancer, chronic kidney disease, and asthma, that may increase the risk of severe COVID-19. 5 Thus, to mitigate the impact of COVID-19, targeted protection measures and healthcare support for these high-risk groups are crucial.
Asthma is a chronic respiratory condition characterized by airway inflammation and narrowing, affecting a substantial proportion of the global population, particularly children.3,5 The prevalence of asthma is significant, with more than 300 million individuals worldwide living with the disease. 6 Certain environmental factors, including exposure to allergens, pollutants, and workplace hazards, contribute to the development and exacerbation of asthma symptoms. 7 Moreover, disparities in asthma prevalence and outcomes have been observed, with African Americans and Hispanics at a higher risk of developing asthma and experiencing worse health outcomes.6,7
While the impact of asthma on respiratory health is well-documented, its potential influence on the severity of COVID-19 remains relatively less explored. Current evidence regarding the risks of COVID-19 among individuals with asthma is limited, prompting the need for a comprehensive scoping review to gather and evaluate existing literature on the topic. Because previous studies discussed other risk factors, were too broad in scope or were observational studies, and/or did not specifically assess asthma as a risk factor for COVID-19 (see PRISMA diagram, Figure 1; Table 1), this scoping review is novel in that it comprehensively analyzed 21 articles of the 70 articles that were screened for with a focus on addressing a research question, “are asthmatic patients at a higher risk for severe COVID-19 illness,” and identified gaps in knowledge highlighting a lack of substantial evidence to indicate that asthmatic patients are at an appreciable risk for severe COVID-19 illness. Addressing this research question would enable us to improve upon our understanding of the relationship between asthma and COVID-19, potentially identifying asthma as a risk factor for severe illness caused by SARS-CoV-2. The findings of this scoping review will inform clinical decision-making, public health interventions, and future research endeavors aimed at mitigating the impact of COVID-19 on individuals with asthma.

PRISMA flow chart of the studies involved in this review.
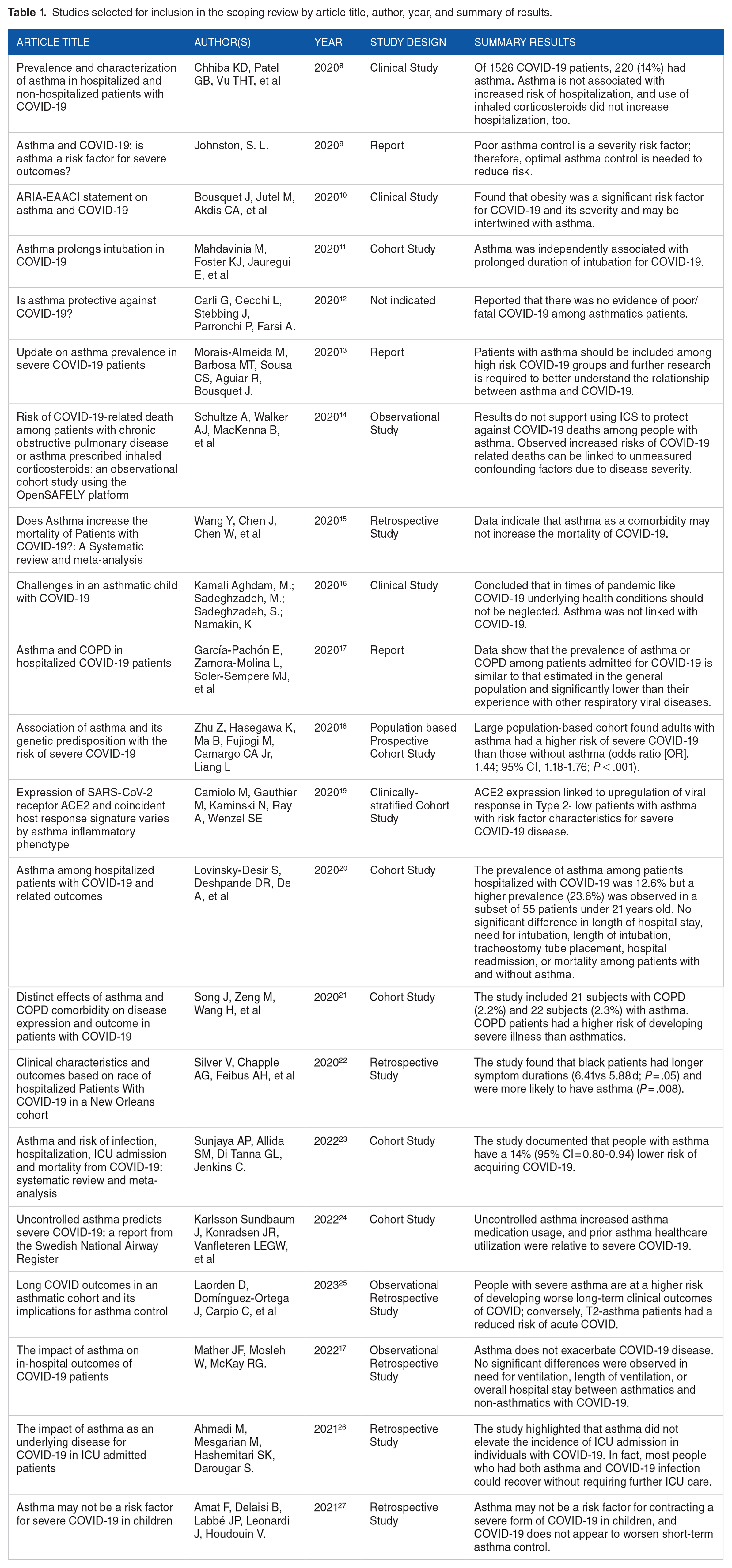
Studies selected for inclusion in the scoping review by article title, author, year, and summary of results.
Methods
Search strategy
A literature review was conducted to gather relevant articles for the scoping review. Several databases and sources were utilized, including PubMed, Google Scholar, IDSA (Infectious Diseases Society of America), American Journal of Respiratory and Critical Care Medicine, and the World Health Organization (WHO) following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines (Figure 1). 28 The search terms used were “SARS-CoV-2,” “COVID-19,” “Coronavirus,” “Asthma,” “Respiratory illness,” and “COVID-19 and Asthmatic patients.”
Inclusion and exclusion criteria
The inclusion criteria included both peer-reviewed and non-peer-reviewed literature, as well as published reports from 2019 to 2023. Articles that were not written in English, articles not available online, articles published before 2019, and articles that did not include reference to SARS-CoV-2, COVID-19, coronavirus, asthma or respiratory illness were excluded from the review.
Study selection procedure
Three reviewers (CU, LP, GK) identified a total of 70 articles from the selected databases and sources. Duplicate articles were removed, resulting in 66 unique articles. The reviewers then screened the titles of these articles, eliminating those that did not meet the inclusion criteria. Four articles were excluded based on the title review, leaving 61 articles for further assessment. The abstracts of these articles were then evaluated, with 28 abstracts not meeting the inclusion criteria and being excluded. The remaining 38 articles underwent full-text review.
Full-text review
During the full-text review, 17 articles were excluded as they discussed other risk factors in addition to asthma, had a broader scope unrelated to asthma and COVID-19, or did not align with the research objective. The final number of articles included in the scoping review was 21.
Data collection and analysis
The literature search covered published articles until April 16, 2023. This ensured the inclusion of the most up-to-date information available at the time of the scoping review. The included articles were thoroughly analyzed and synthesized to extract relevant information related to the research question. Data extraction involved identifying key findings, study designs, sample sizes, methodologies, and conclusions from each article. The extracted data were then organized and synthesized to provide a comprehensive overview of the literature on the relationship between asthma and severe COVID-19 illness. The PRISMA flow diagram depicts the article selection process, highlighting the number of articles identified, screened, and included in the scoping review (Figure 1).
Results
Of the 21 studies included in our scoping review, 6 studies concluded asthmatic patients were at higher risk for developing a severe COVID-19 illness, 10 studies did not identify asthma as a risk factor, and 4 studies had inconclusive findings. Of the 4 inconclusive studies, one study of 744 asthmatic patients diagnosed with COVID-19 illness concluded that the available data on the influence of asthma on the risk of hospitalization, the duration of hospitalization, the requirement of ICU admission, and disease severity are too limited to draw firm conclusions. 15 Three other studies derived similar inconclusive findings, with one study concluding COVID-19 illness in pediatric asthmatic patients may mask other underlying respiratory conditions. 11
Of the studies that implicated asthma as risk factor for severe COVID-19 illness, one study of 935 hospitalized COVID-19 patients found that asthma was independently associated with prolonged intubation. 11 In this cohort, younger asthmatic patients (<65 years) experienced a significantly prolonged intubation time compared to older patients. The study suggested that younger asthmatic individuals may require additional attention due to the increased risk of developing sustained pulmonary failure. A second study, which looked at the association of asthma and its genetic predisposition with the risk of severe COVID-19 illness noted an increased risk for severe illness. 18 The researchers utilized population-based cohort data from the U.K. Bio-Bank of approximately 500 000 individuals. They applied logistic regression modeling to characterize asthma’s association with severe COVID-19 and concluded that adults with asthma had a higher risk of severe COVID-19 disease. The 2 remaining studies that identified asthmatic patients being at higher risk for severe COVID-19 illness concluded that the prescribed choice of asthma relief therapy (inhaled corticosteroids vs short-acting beta-agonists) was the primary driver for risk. In one study, asthmatic individuals with COVID-19 who received high-dose inhaled corticosteroids (ICS) were at increased risk of death compared to those receiving a short-acting beta-agonist (SABA). 14 Another study conducted in the U.K. found a significantly increased risk of severe COVID-19 disease and asthmatic patients’ mortality, particularly in those with recent oral corticosteroid (OCS) use. 13 Asthmatic patients with a recent corticosteroid use also had higher SARS-CoV-2 viral loads. More recently, asthma was implicated in causing severe COVID-19 infection and prolonged maximum respiratory support was required in children admitted to the Children’s National Hospital in Washington, DC, USA. 29
In contrast, 17 studies reviewed concluded that asthma was not an independent risk factor for severe COVID-19 disease. One such study concluded neither asthma nor inhaled corticosteroids were associated with an increased risk of COVID-19 hospitalization. 8 A study by Sunjaya et al 23 documented a 14% lower risk of acquiring COVID-19 in individuals with asthma, which translates to a reduction of 50 cases per 1000 people. However, the risk reduction may be due to down-regulated ACE-2 receptors in people with type 2 (T2)-high severe asthma (characterized by eosinophilic airway infiltrate and TH2-dependent cytokine [IL-4, IL-5, and IL-13] overexpression), 30 which may decrease their susceptibility to SARS-CoV-2 infection.
Asthma is a chronic obstructive airway disease with distinct endotypes or subtypes. The most common type is T2-high inflammation-mediated asthma, characterized by T-helper 2 cell-mediated inflammation driven by cytokines like IL-4, IL-5, and IL-13. This type is associated with eosinophil infiltration, and thus also called eosinophilic asthma. 12 T2-high asthma is diagnosed by elevated eosinophil levels. T2-high inflammation, present in 50% to 70% of asthma patients, involves immune cell activation and the release of cytokines, leading to airway inflammation, exacerbations, and reduced lung function. 12 On the other hand, T2-low or non-T2 asthma lacks a clear definition or biomarker but is characterized by the absence of T2-high inflammation. Non-T2 asthma encompasses different inflammatory and non-inflammatory endotypes, based on sputum cytometry and airway hyperresponsiveness. Non-T2 inflammation can be caused by factors such as structural abnormalities in the airway smooth muscle (ASM) or abnormal neuronal activation.31,32 It’s worth noting that ongoing research aims to further elucidate the distinct subtypes of asthma and their underlying mechanisms, with the goal of developing targeted therapies for each endotype to improve asthma management and patient outcomes.
In a study from one of the U.S. largest healthcare systems (Northwestern Medicine, Chicago) that diagnosed 1526 patients with COVID-19 classified 220 (14%) patients as being asthmatic. 8 Further, the study concluded that asthma as a risk factor was not associated with an increased risk of hospitalization from COVID-19 (relative risk, 0.96; 95% CI, 0.77-1.19). 8 In a study from Italy assessing the risk of severe COVID-19 in a town of 200 000 inhabitants among which about 10 000 were asthmatics found that asthmatic patients were not at a higher risk for severe COVID-19. 33 Only 3 out of 275 COVID-19 positive asthmatics in the town required hospital admission, and only one required ICU admission. 34 This is supported by several retrospective studies, where comorbidity of asthma and COVID-19 did not increase susceptibility to ICU admissions and death.25,35
In a Spanish study that reviewed medical records of 168 consecutive adult patients (aged over 14 years) admitted for COVID-19, only 4 patients (2.4%) were diagnosed with asthma. 35 The authors concluded that the prevalence of asthma in that cohort was similar to that of the general population in Spain (2%-3%) and that these patients did not seem to be at higher risk of hospital admission for COVID-19. 17 In an US study that comprised of 1298 hospitalized patients in New York, researchers aimed to determine whether underlying asthma was associated with poor outcomes among hospitalized patients with severe COVID-19 compared to patients without asthma. 20 Electronic health records review found no significant difference in length of hospital stay, need for intubation, length of intubation, tracheostomy tube placement, hospital readmission, or mortality between patients with and without asthma. 20 These findings led the authors to conclude that asthma diagnosis was not associated with worse outcomes, regardless of age, obesity, or other high-risk comorbidities. 20 Further, a recent pneumopediatric retrospective study conducted in La Guisane, France that studied 51 asthmatic children aged 14.14 ± 2.38 years, who were diagnosed with COVID-19, concluded asthma not a risk factor for a severe COVID-19, and that COVID-19 did not worsen short-term asthma control, in children. 27 The 12 studies identified above shared similar findings, concluding that asthmatic patients are not at an increased risk for poorer outcomes associated with severe COVID-19 disease.9,16 Table 1 summarizes the key findings of the 21 studies included in this scoping review.
Discussion
The findings from the 21 studies included in this scoping review revealed an inconclusive relationship between asthma and severe COVID-19. While a few studies (n = 4) implicated asthma as a risk factor for COVID-19, most of the studies (n = 17) found no significant association between the 2 diseases. This discussion is framed around the potential implications of the findings, the putative mechanisms underlying the observed outcomes, and the limitations of the current science.
The results revealed a mixed picture regarding the risk of severe COVID-19 illness in asthmatic patients. Six studies identified asthma as a risk factor for severe illness, while 10 studies did not find asthma to be an independent risk factor. In some instances, the SARS-CoV-2 infections in children with asthma might have masked other underlying respiratory conditions, making it difficult to isolate the impact of asthma alone. Despite the varying conclusions in the studies, the importance of good asthma management during COVID-19 infection to avoid complications was emphasized across multiple studies.13,14,36,37 Importantly, proper asthma management and strict adherence to medication are essential to mitigate risk of complications should an asthmatic patient presents COVID-19 illness because an uncontrolled asthma may complicate COVID-19 outcome.18,36,37
The studies that identified asthma as risk factor for severe COVID-19 illness pointed to potential mechanisms that may contribute to this association. One study suggested that people with asthma might experience extended intubation times with elevated risk of developing sustained pulmonary failure upon contracting the virus, particularly among younger asthma patients. 38 This finding further highlights the importance of monitoring and providing additional attention to younger asthma patients to manage their respiratory function effectively during COVID-19 infection. Furthermore, another study investigated the association between asthma and genetic predisposition to severe COVID-19 illness. 18 The researchers used a population-based cohort and statistical modeling to conclude that adults with asthma had a higher risk of experiencing severe COVID-19 outcomes. This study suggested for potential genetic factors that might be related to asthma which may contribute to the increased vulnerability to severe COVID-19 infection in the population. 18 Two other studies suggested that the choice of asthma relief therapy could influence the risk of severe coronavirus infection outcomes.14,37 High-dose inhaled corticosteroids (ICS) were associated with higher mortality rates and increased viral load in asthmatic individuals with COVID-19 compared to those receiving SABA. 14 Similarly, recent use of oral corticosteroids (OCS) in asthma patients was linked to a significantly increased risk of severe COVID-19 and higher mortality rates. 37 These findings imply that the type of medication prescribed for asthma may have implications for the severity of COVID-19 infection in these patients. More recently, Salsman et al. 33 reported that people with asthma faced distinct psychological problems during the coronavirus disease pandemic. These psychological difficulties led to increased burnout symptoms and severity of asthma symptoms contributed substantially to vulnerability to emotional exhaustion. Consequently, clinicians should prioritize addressing asthmatic patient’s symptom burdens amidst increased environmental stress and limited healthcare access. 33
On the other hand, several studies found no independent association between asthma and severe COVID-19 illness.8,9,15,30,39 These studies concluded that asthma did not increase the risk of severe outcome related to the coronavirus disease. For example, a study specifically investigated the risk of COVID-19 hospitalization in individuals with asthma and on ICS based therapy. 14 The researchers indicated that neither asthma nor the use of ICS was associated with an increased risk of COVID-19 hospitalization. This suggests that asthma patients using ICS, a common treatment for asthma, were not at a higher risk of severe COVID-19 disease requiring hospitalization. Moreover, another study observed a reduced risk of acquiring COVID-19 in individuals with asthma. 23 The authors suggested a potential protective effect in asthmatic patients, possibly attributed to down-regulated ACE-2 receptors in individuals with T2-high asthma, which may decrease their susceptibility to SARS-CoV-2 infection. Another study reviewed the medical records of 168 adult patients admitted with COVID-19 and found only 2.4% of those admitted were diagnosed with asthma. 35 The authors concluded that the prevalence of asthma in their cohort was similar to that of the general population, and asthmatic patients did not appear to be at a higher risk of hospital admission for severe COVID-19.
Overall, the studies that identified asthma as a risk factor for severe COVID-19 illness provided valuable insights into potential underlying mechanisms. They highlighted the importance of carefully managing asthma patients against the virus, considering individual patient factors, and exploring how genetic predisposition and medication choices may influence disease outcomes. On the other hand, the studies that found no independent association between asthma and severe COVID-19 illness highlight that having asthma does not necessarily increase the risk of experiencing severe outcomes related to COVID-19 infections. Some studies even suggested a potential protective effect or no difference in risk compared to the general population.17,35 Taken together, this scoping review did not find conclusive evidence that asthma is a major risk factor to COVID-19 severity, underscoring the need for more research to fully understand the potential role of asthma in exacerbating COVID-19 outcomes. These findings emphasize the importance of carefully analyzing data from diverse populations and considering other factors that may influence COVID-19 severity among individuals with asthma. It is, thus, paramount to emphasize the need for future research aimed at deciphering the potentially complex relationship between asthma and COVID-19 illness, and the potential confounding effects of high-dose corticosteroid use in severe COVID-19 management among asthmatic individuals as compared to the non-asthmatic populations. Large-scale prospective cohort studies with standardized methodologies are needed to provide more robust evidence on the risk of severe COVID-19 illness among asthmatic patients. Furthermore, understanding the impact of specific asthma medications, genetic factors, and other comorbidities on COVID-19 outcomes may help inform clinical practice guidelines for effective patient health management.
Study limitations
Several limitations are identified of this scoping review. The limited number of studies available for inclusion and the heterogeneity of methodologies and definitions used posed challenges in drawing definitive conclusions. Most of the studies were observational in nature, which inherently carries the risk of biases and confounding factors. Additionally, the dynamic nature of the pandemic means that new evidence may emerge in the future, potentially influencing our understanding of the relationship between asthma and severe COVID-19 illness. Our conclusions were drawn from a limited sample size. However, if methodologies were systematized across studies as one of our inclusion criteria, we would have resulted in fewer than the 21 studies, which would make it difficult to make a meaningful conclusion. The implications of our results must be highlighted as a strength of this scoping review. In the literature currently available on COVID-19 disease, there is no substantial evidence to indicate that asthmatic patients are at an appreciable risk for severe COVID-19.
Conclusion
The findings of this scoping review point to a lack of relationship between asthma and severe COVID-19 illness. While a limited number of studies identified asthma as a risk factor, most studies found no independent association. The current evidence highlights the need for further research to elucidate the mechanisms underlying these observations and to guide clinical decision-making. Clinicians should continue to closely monitor and manage asthma in the context of the COVID-19 severity, considering individual patient characteristics and potential risk factors. Overall, larger comprehensive studies are warranted to understand potential interplay between asthma and COVID-19 outcomes, providing valuable insights for healthcare professionals to mitigate risks and improve care for asthmatics with COVID-19.
Footnotes
Acknowledgements
CSU express gratitude to the senior authors for their assistance in preparing this manuscript.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
CSU, GDK, and LRP designed the study, conducted literature search, and identified relevant articles. CSU performed data extraction and analysis. CSU wrote the first draft. GDK and LRP edited and revised the manuscript. All authors approved the final version.
Data Availability
All data related to this work are presented as table and flow chart and can be made available by the corresponding authors upon reasonable request.