
Abstract
Breast cancer (BC) is the most prevalent malignancy in women. The emergence of targeted therapies and advancements in comprehensive treatment protocols have significantly improved survival outcomes for patients with early-stage BC. However, individuals with refractory BC, particularly those who have received multiple lines of therapy or presented with distant metastases at diagnosis, continue to face challenges due to the limitations of conventional antibodies and cytotoxic agents in meeting therapeutic needs. Thus, the development of novel and effective treatments for BC, along with strategies to prevent recurrence, remains an urgent priority. Research has shown that nanodrug delivery systems can modify the pharmacokinetic profiles of traditional chemotherapeutic agents, thereby markedly reducing adverse drug reactions. Furthermore, studies have demonstrated that innovative approaches, such as hyaluronic acid-based systems, ultrasound-mediated microbubbles, and antibody-drug conjugates (ADCs), enable targeted and controlled drug release, offering advantages including high drug efficacy, reduced toxicity, and significant antitumor effects. Among these, ADCs have gained increasing attention in BC therapy over recent years. This article provides a comprehensive review of the development and progress of various drug delivery systems in BC treatment, offering an in-depth analysis of their potential applications in clinical practice.
Plain Language Summary
Breast cancer (BC) represents the most prevalent form of cancer affecting women. The advent of targeted therapies and the enhancement of comprehensive treatment protocols for BC have significantly improved survival outcomes for individuals with early-stage BC. Nevertheless, patients with refractory BC, particularly those who have undergone multiple lines of treatment or initially presented with distant metastases, face challenges as conventional antibodies or cytotoxic drugs fail to meet therapeutic needs. Therefore, the development of novel and effective medications for BC treatment and the prevention of recurrence is an urgent priority. Research indicates that nanodrug delivery systems modify the pharmacokinetic properties of traditional chemotherapeutics, thereby substantially mitigating adverse drug reactions. Additional studies have demonstrated that innovative approaches, such as hyaluronic acid, ultrasound microbubbles, and antibody-drug conjugates (ADCs), enable targeted controlled drug release, offering benefits such as high drug release rates, reduced adverse reactions, and significant antitumor effects. Among these, ADCs have gained increasing prominence in BC therapy in recent years. Now this article presents a comprehensive examination of the present developments and advancements of these different drug delivery carriers in BC therapy.
Introduction
Breast cancer (BC) is not only the most prevalent malignancy in women but also a leading cause of cancer-related mortality. Breast cancer is classified into 4 subtypes based on the expression of estrogen receptor (ER), progesterone receptor (PR), HER-2, and Ki-67: Luminal A (LA), Luminal B (LB), HER-2-overexpressing, and triple-negative breast cancer (TNBC). Standard treatment modalities include endocrine therapy for HR+/ER+ patients, HER-2-targeted therapy for HER2+ patients, chemotherapy and immunotherapy for TNBC patients, and PARP inhibitor therapy for BRCA-mutated TNBC patients. Triple-negative breast cancer is characterized by rapid recurrence, a high incidence of brain metastasis, and a 5-year survival rate below 80%, often exhibiting resistance to broad-spectrum anticancer agents.1,2 Encouragingly, substantial progress has been achieved in the management of localized BC, with a 5-year survival rate approaching 90%. However, despite the use of chemotherapy, radiotherapy, or estrogen blockers, effective treatment strategies for advanced metastatic BC remain limited.3,4 In view of the rising prevalence of long-term diseases and the accelerating process of population aging, there is an urgent need to develop more efficient and less toxic therapies. Consequently, novel drug delivery systems have attracted significant attention and are undergoing vigorous development.
In this context, the research and development of novel drug delivery systems have gained significant attention, with the aim of enhancing drug bioavailability, reducing adverse effects, and achieving precise tumor targeting. 5 Specifically, these systems include various forms such as nanoparticles, hyaluronic acid (HA), ultrasound (US) microbubbles, and antibody-drug conjugates (ADCs), which can protect drugs from degradation in vivo, prolong their circulation time, and deliver them directly to tumor tissues via specific targeting mechanisms, thereby improving therapeutic efficacy while minimizing damage to normal tissues.6 -8 Moreover, novel drug delivery systems can enable intelligent drug release in response to changes in the tumor microenvironment, allowing dynamic adjustment of drug concentrations and further optimizing treatment outcomes. These systems demonstrate promising applications in BC therapy, with the potential to improve patient prognosis. 9 This article systematically reviews the advantages, disadvantages, prospects, and future developments of 4 types of drug delivery systems—nanoparticles, HA, US microbubbles, and ADCs—providing a reference for comprehensive BC treatment strategies (Figure 1).

Application of various drug delivery systems in breast tumors.
Nano-Drug Delivery Systems
The mechanisms of nanomaterials in targeted therapy can be classified into passive targeting, active targeting, and physicochemical targeting. The advantages of applying nanotechnology in the medical field include reversing drug resistance in tumor chemotherapy, reducing dosing frequency while prolonging drug residence time to achieve sustained-release and controlled-release effects, and enabling surface modification of nanomaterials for the development of multifunctional drug delivery systems, thereby enhancing therapeutic efficacy and minimizing adverse effects. In addition, nanomaterials with unique optical or magnetic properties can be utilized in minimally invasive tumor treatments.10,11 Jiang et al 12 developed a multifunctional nanotherapeutic platform (PEG-PEI-AuAg@HCT, PPAPH) specifically targeting HER2-positive BC. This platform employs gold-silver hollow nanoshells (AuAg HNS) as carriers to achieve synergistic chemotherapy and photothermal therapy. With dual-stimuli-responsive drug release characteristics, it exhibits superior photothermal conversion efficiency under 808 nm laser irradiation, effectively inhibiting tumor growth and reducing tumor size while exerting minimal effects on healthy tissues. The Yang Piaoping team 13 designed Cu-doped BiOCl nanosheets with surface oxygen vacancies (SV-CBOC NSs) for synergistic anticancer therapy (Figure 2). The seamless integration of photodynamic therapy (PDT), sonodynamic therapy (SDT), and chemodynamic therapy (CDT) enhances the cytotoxic effect on tumor cells, offering a novel approach and reference for US-mediated multimodal tumor treatment.

Schematic diagram of the preparation of SV-CBOC NSs and the proposed synergistic therapeutic mechanism.
Nanomaterials for targeted BC therapy primarily encompass organic and inorganic nanomaterials. Organic nanomaterials include solid liposomes, liposomes, and polymers.14 -18 Among these, cyclodextrins, cyclic macromolecules approved by the Food and Drug Administration (FDA), have been demonstrated to function as molecular valves that regulate conformational changes in supramolecular systems, thereby facilitating the controlled release of therapeutic payloads. 19 Kaduri et al 20 developed a novel therapeutic strategy targeting tumors via nerve cells. This approach involves the intravenous injection of lipid nanoparticles loaded with the anesthetic bupivacaine. These nanoparticles circulate through the bloodstream to the tumor site, accumulate around nerve cells in BC tissue, and induce paralysis of local nerves as well as disrupt communication between nerve cells and cancer cells. Consequently, this significantly suppresses breast tumor formation and metastasis to the lungs, brain, and bone marrow. Ren et al 21 prepared a liposomal nanomedicine co-delivering doxycycline hydrochloride (Doxy), an antibiotic, and chlorin e6 (Ce6), a photosensitizer. By integrating Ce6-mediated PDT with Doxy-induced autophagy suppression and mitochondrial dysfunction, they achieved efficient photodynamic/immunotherapy for “cold tumor” BC. Zhen et al 22 reported an afterglow/photothermal dual-functional conjugated polymeric nanomaterial (Figure 3), composed of an amphiphilic long afterglow conjugated polymer containing tumor-targeting groups (PPV-PEG-cRGD), a long afterglow initiator (NCBS), and a near-infrared II (NIR-II) photothermal conjugated polymer with high photothermal conversion efficiency (PBBTOT). The afterglow imaging capability of this nanomaterial enables precise localization of minute residual tumor foci following breast-conserving surgery in mice. Subsequently, the NIR-II photothermal imaging function facilitates the precise ablation of localized residual tumor foci, minimizing ionizing radiation side effects while effectively inhibiting the in situ recurrence of BC.
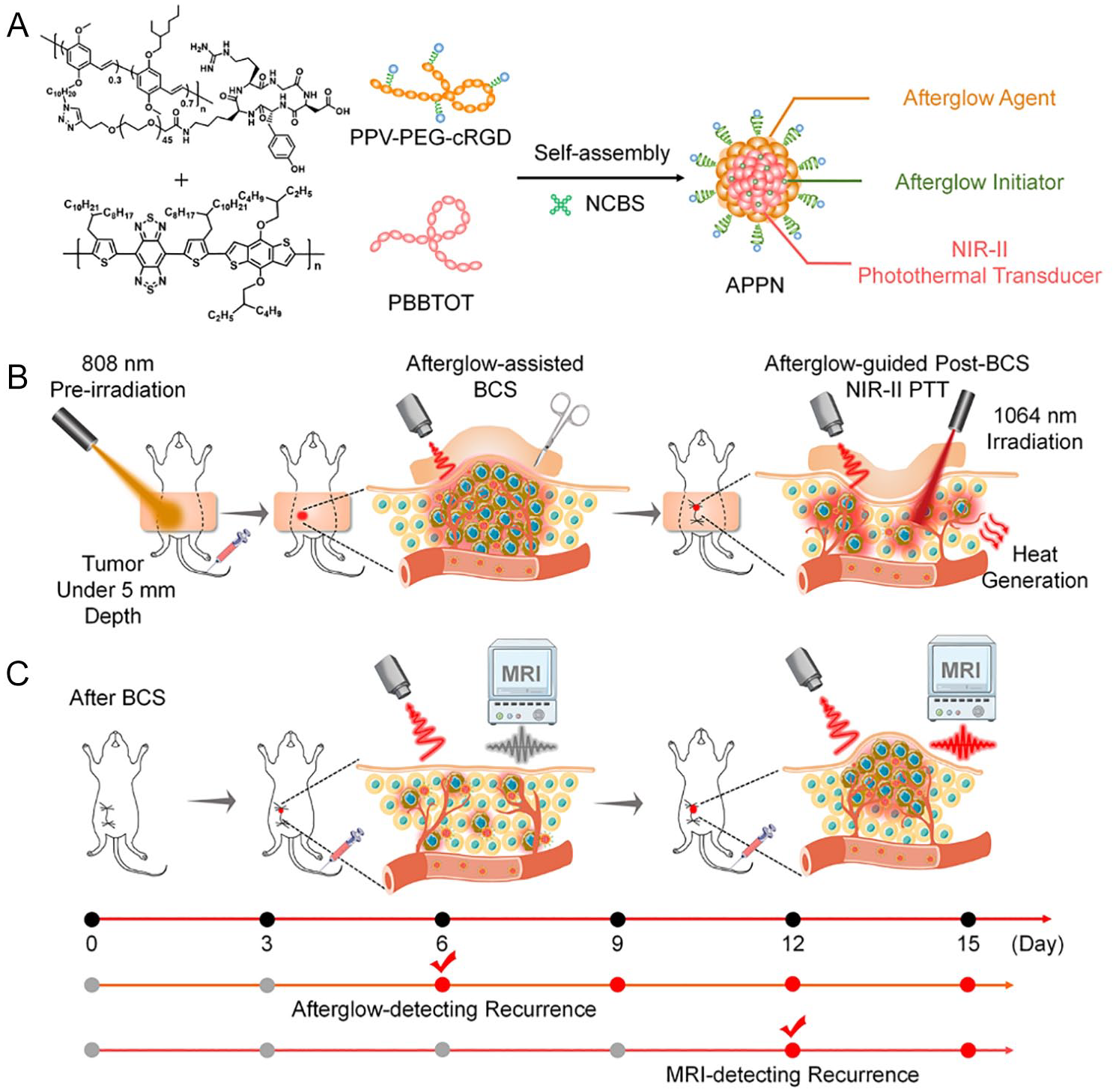
Schematic diagram of APPN for postoperative imaging-guided adjuvant therapy and early recurrence diagnosis and treatment after BCS. APPN, afterglow/photothermal polymeric nanoparticles; BCS, breast-conserving surgery. A. APPN is composed of an amphiphilic long-persistent luminescence conjugated polymer (PPV-PEG-cRGD) containing tumor-targeting groups, a long-persistent luminescence initiator (NCBS), and a near-infrared material with high photothermal conversion efficienciency. B. The afterglow imaging function of APPN enables precise localization of small residual tumor foci in mice after surgery, reducing the side effects of ionizing radiation while effectively inhibiting the recurrence of breast cancer in situ. C. APPN’s long-lasting luminescence imaging function can sensitively detect recurrent tumor cells that have not yet formed microscopic solid tumors in vivo, with a detection sensitivity superior to that of traditional magnetic resonance imaging.
Inorganic nanomaterials encompass quantum dots (QDs), 23 silica-based nanomaterials (MSNs), 24 metallic nanomaterials, 25 and carbon-based nanomaterials. 26 Liang et al 27 reported a mitochondrial oxidative stress amplifier, MitoCAT-g, consisting of atomically dispersed gold particles (CAT-g) supported on carbon dots and further surface-modified with triphenylphosphine and cinnamaldehyde. Their study demonstrated that MitoCAT-g particles specifically target mitochondria, consuming mitochondrial glutathione in an atom-economical manner to amplify reactive oxygen species (ROS) damage induced by cinnamaldehyde, ultimately leading to cancer cell apoptosis [Figure 4].
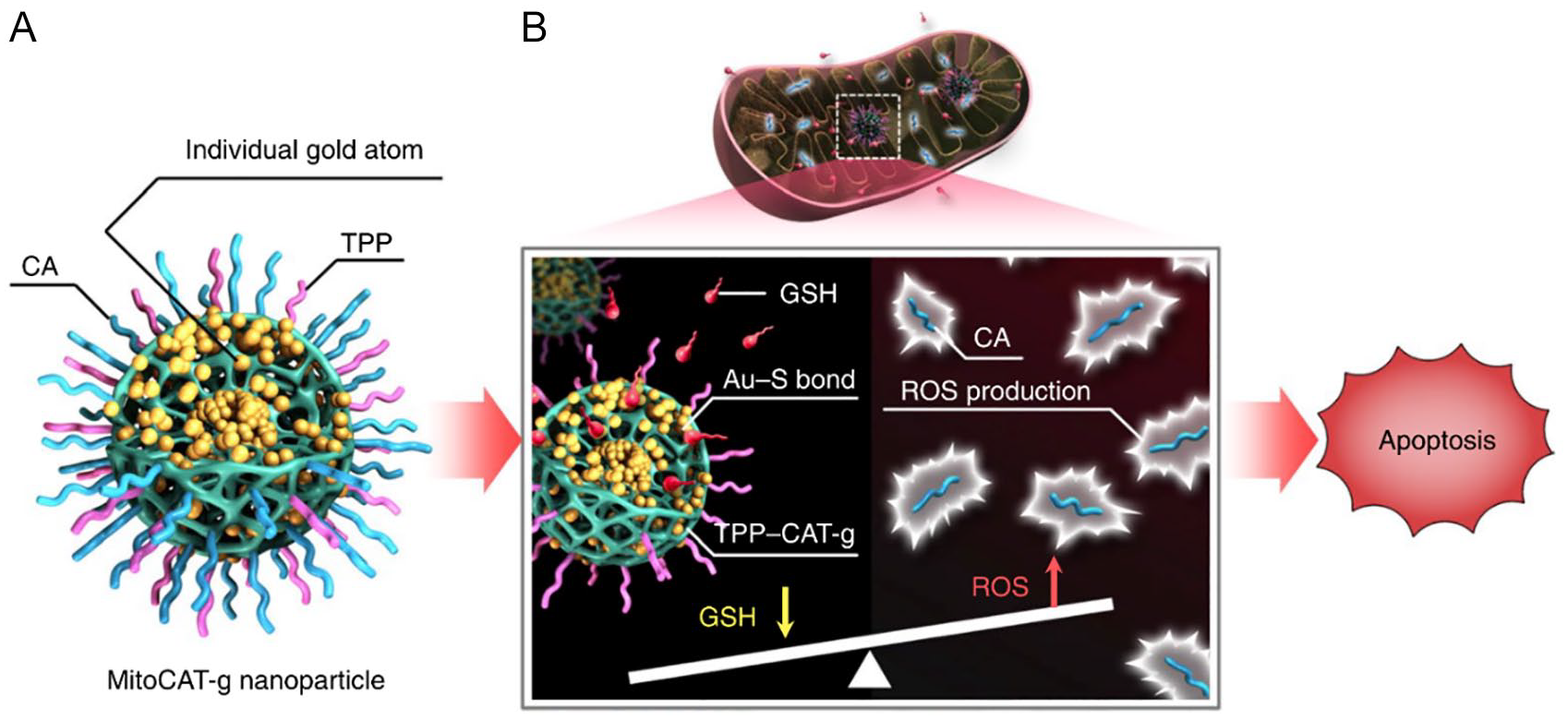
Fabrication of HM-NPs@G. Schematic of MitoCAT-g nanoparticle structure (A) and its mechanism: targeting mitochondria, reacting with GSH via AU-S bonds to deplete GSH, trigger ROS production, and induce apoptosis (B). HM-NPs@G: hybrid membrane-camouflaged reactive oxygen species (ROS)-responsive nanoparticles loaded with Gboxin. 27
Shi et al 28 developed cancer cell-mitochondrial hybrid membrane-camouflaged, ROS-responsive nanoparticles loaded with Gboxin, enabling noninvasive targeted delivery of Gboxin to glioblastoma multiforme (GBM) mitochondria. The hybrid membrane-encapsulated biomimetic nanoparticles significantly prolonged the circulation half-life by evading immune clearance, thereby overcoming the limitations of Gboxin therapy. This innovative nanoplatform can effectively penetrate the blood-brain barrier and selectively deliver Gboxin to GBM mitochondrial targets, thus inhibiting GBM tumor cell proliferation (Table 1).
Nano drug delivery system in breast tumor.
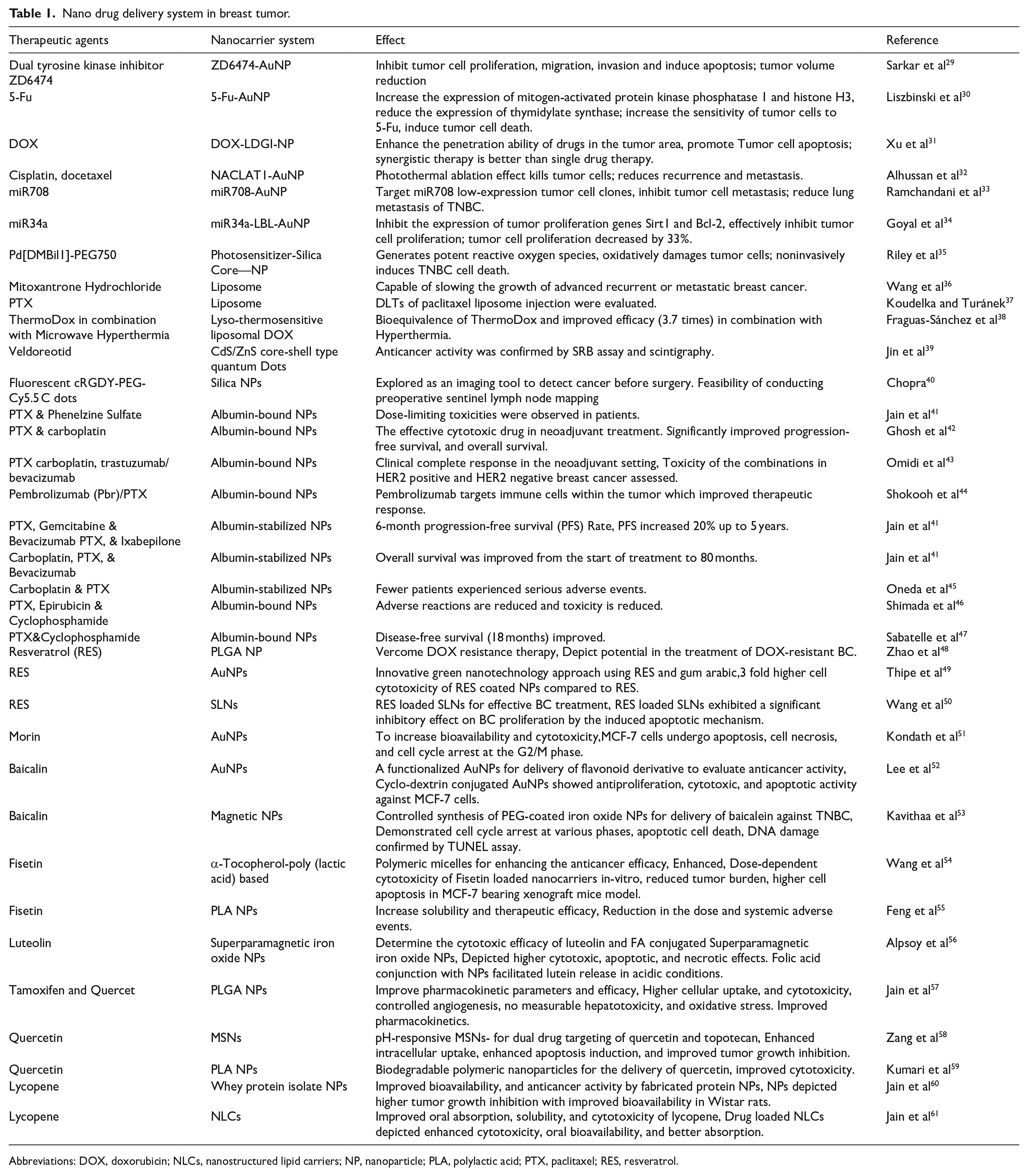
Abbreviations: DOX, doxorubicin; NLCs, nanostructured lipid carriers; NP, nanoparticle; PLA, polylactic acid; PTX, paclitaxel; RES, resveratrol.
Nanodelivery systems not only demonstrate remarkable potential in BC vaccine development but also leverage unique physical and chemical properties. These properties include enhancing drug bioavailability, improving targeting specificity, minimizing side effects, and protecting drugs from degradation within the body. 62 In BC vaccine research, nanodelivery systems can augment immune responses via multiple mechanisms, such as promoting antigen uptake by antigen-presenting cells, stabilizing antigens and prolonging their retention in the body, as well as activating specific immune signaling pathways. 63 Nanodelivery systems can enhance vaccine targeting through both passive and active strategies. Passive targeting primarily depends on nanoparticle size and surface modification to facilitate accumulation in tumor tissues. Active targeting involves modifying nanoparticles with specific ligands, such as antibodies or peptides, to recognize and bind to receptors on tumor cell surfaces. Notably, nanodelivery systems can shield vaccine antigens from enzymatic and other forms of degradation, extending their circulation time, which is critical for improving vaccine stability and efficacy. 64 Furthermore, nanoparticles can function as adjuvants, enhancing immune responses by activating specific receptors on immune cells, such as Toll-like receptors (TLRs). 65
Of course, during the circulation of BC nanomedicines in the body, they inevitably interact with the immune system. These interactions significantly influence the efficacy and safety of nanomedicines. For example, BC nanomedicines can activate macrophages, promoting their polarization toward the antitumor M1 phenotype, thereby enhancing their antitumor activity. 66 In addition, macrophages can phagocytose nanomedicines, affecting their distribution and metabolism in the body. Furthermore, BC nanomedicines can modulate the maturation and function of dendritic cells (DCs), promoting their capture and presentation of tumor antigens and thus activating T-cell-mediated immune responses. Therefore, to improve the efficacy and safety of BC nanomedicines, it is essential to rationally regulate their interactions with the immune system. 67 By modifying the surface of nanomedicines with highly biocompatible polymers, antibodies, peptides, and so on, nonspecific interactions with immune cells can be minimized, thereby improving their targeting and biocompatibility. Combining BC nanomedicines with immunotherapeutic agents (such as immune checkpoint inhibitors, cytokines, etc.) can further enhance immune responses and improve therapeutic efficacy.68,69 The interaction between BC nanomedicines and the immune system is a complex process involving multiple immune cells and signaling pathways. In-depth research into these interactions and their underlying mechanisms can aid in the development of safer and more effective BC nanomedicines, offering new treatment options for BC patients.
Hyaluronic acid Delivery Carriers
Hyaluronic acid is a naturally occurring linear polysaccharide with excellent biocompatibility and biodegradability. It targets tumors via the cell surface receptor cluster of differentiation 44 (CD44).70,71 CD44, a receptor exhibiting high affinity for HA, serves as a tumor marker or targeted receptor due to its overexpression and specificity in tumor cells. When conjugated with nanomedicine carriers, CD44 ligands can enhance the affinity of nanocarriers for tumor cells. 72 Hyaluronic acid is recognized for its efficient tumor-targeting capability, which is attributed to the presence of CD44 ligands within its structure.
Moreover, the presence of various functional groups within the HA structure enables further structural modification and functionalization, making it a promising carrier material for tumor-targeted delivery. 73 Hyaluronic acid serves as an ideal polymeric carrier for systemic drug administration and has been extensively applied in the delivery of diverse therapeutic agents. 74 Zhang et al 75 co-encapsulated the chemotherapeutic drug cisplatin (Cis) and chloroquine (CQ) into hyaluronan-based nanogels, markedly enhancing the intracellular delivery efficiency of Cis and achieving efficient, targeted therapy for TNBC. Compared with the free drug combination (Cis + CQ), this HA/Cis/CQ nanogel formulation maintains robust antitumor efficacy while significantly reducing nephrotoxicity-associated adverse effects (Table 2).
HA-anticancer drug conjugates.

Characterisation of HA
Hyaluronic acid enhances drug uptake in cells with high expression of its receptors, thereby potentiating therapeutic efficacy. Cluster of differentiation 44, the primary receptor for HA, is a transmembrane glycoprotein that exhibits elevated expression in various tumors. The CD44 receptor undergoes alternative exon splicing and posttranscriptional modifications in gene expression, resulting in multiple isoforms. 80 Anttila et al 81 demonstrated that stromal HA accumulation correlates with tumor progression by evaluating HA levels and CD44 expression; however, they argued that HA accumulation is not associated with CD44 expression on the surface of human ovarian cancer cells. Zhao et al 82 found that CD44 promotes cell proliferation in lung cancer cells through activation of mitogen-activated protein kinase (MAPK) signaling, whereas deletion of the CD44 gene inhibits Kras-mediated lung adenocarcinoma proliferation in mice. Furthermore, the interaction between HA and CD44 facilitates ankyrin binding to MDR-1, leading to the efflux of chemotherapeutic drugs and chemotherapy resistance in tumor cells. 83
Targeted therapy with HA
Hyaluronic acid demonstrates excellent biocompatibility and exhibits no immunogenicity. 84 HA can bind to the overexpressed cluster of differentiation protein 44 (CD44) receptors on cancer cell membranes, thereby conferring tumor-targeting properties. Notably, CD44 receptors are upregulated in various BC subtypes, with significant overexpression observed in TNBC. Li et al 85 synthesized targeted micelles with an average diameter of 120 nm using an HA-deoxycholic acid (DOCA) copolymer loaded with paclitaxel (Taxol), achieving a drug loading content of 34%. MTT assays were performed to analyze and compare the cytotoxicity of this formulation with clinically used paclitaxel in MDA-MB-231 BC cells and normal human embryonic lung fibroblasts (HELF). The results indicated that paclitaxel-loaded HA micelles exhibited enhanced cytotoxicity against CD44-positive tumor cells compared with paclitaxel alone, while demonstrating reduced toxicity toward HELF cells at equivalent concentrations. Studies have highlighted that breast tumor cells contain high levels of hyaluronidase (HAase), which can rapidly degrade HA-based drug carriers, releasing the drug and targeting tumor cells.86,87 Stenzel 88 developed a pH-responsive HA micellar system by conjugating thiolated HA (HA-SH) with the lateral unsaturated bonds of phosphatidylcholine via click chemistry methodology. The resultant copolymer spontaneously formed doxorubicin-encapsulated micelles, achieving a 10% drug loading efficiency. The release kinetics were evaluated at pH 7.4 and 5.0, revealing approximately 2-fold higher doxorubicin release in an acidic environment (pH 5.0) compared with physiological conditions (pH 7.4) over a 48-h period. Wang et al 89 developed HA-modified liposomes loaded with cisplatin (CDDP) and hesperidin (Hes), enhancing the efficacy of chemotherapy in TNBC. Hyaluronic acid modification promotes the uptake and retention of nanoparticles in BC cell lines. These nanoparticles mitigate inflammation by inhibiting the PI3K/Akt/mTOR pathway and improve chemosensitivity by inhibiting epithelial-mesenchymal transition, effectively suppressing the invasion and metastasis of TNBC while exhibiting reduced side effects on normal tissues.
Hydrogen sulfide (H2S) has been recognized as the third gasotransmitter implicated in various physiological and pathological processes. Endogenous H2S or moderate exogenous H2S levels promote tumor cell survival, whereas increased expression of H2S-generating enzymes or exposure to high concentrations of H2S-releasing compounds may exhibit antitumor effects.90,91 ADT-OH, a commonly used H2S-releasing agent, contains the ~3H-1,2-dithiol-3-thione moiety within its molecular structure. 92 The synthesis of HA-ADT is achieved through the chemical conjugation of HA with ADT-OH. Dong et al 93 investigated the effects of HA-ADT on human BC cell progression. The findings revealed that HA-ADT released higher levels of H2S compared with NaHS and GYY4137. Hyaluronic acid-ADT exhibited superior inhibitory effects on the proliferation and viability of human BC cells relative to NaHS and GYY4137, while also reducing their migratory and invasive capabilities. These results suggest that HA-ADT may play a pivotal role in suppressing the growth, migration, and invasion of human BC cells. The integration of these in vitro findings supports the development of a promising formulation with enhanced tumor-targeting efficacy and improved safety for normal cells, highlighting the potential benefits of active tumor targeting. 94
As evident from the above, both in vitro and in vivo studies robustly support the concept that conjugating HA to the outer surface of micelles enhances the targeting of tumor cells. When combined with passive targeting, this active targeting strategy offers a promising approach for delivering chemotherapeutics to tumors that overexpress CD44. 95 As depicted in Figure 5, HA-based nanomicelles exhibit excellent biological safety and possess notable capabilities for drug release, blood compatibility, and systemic tumor targeting, thus presenting a favorable prospect for clinical oncology treatment.96,97

Structure and function of hyaluronic acid (HA).
Ultrasound Microbubble Delivery Vehicle
Ultrasound imaging technology is a real-time imaging modality in which contrast agent microbubbles preferentially accumulate within the rich microvasculature of tumors for tumor visualization.98,99 Traditional intravenous drug administration methods are limited by low tumor-targeting concentrations, short drug circulation times, and significant adverse reactions, such as nephrotoxicity and bone marrow suppression. In recent years, studies have confirmed that microbubbles can serve as carriers for chemotherapeutic agents (e.g., paclitaxel). Ultrasound-targeted microbubble destruction (UTMD), as a drug and gene delivery system, enables targeted and controlled drug release, offering advantages such as high drug release efficiency, uniform distribution, prolonged circulation time, reduced adverse effects, and enhanced antitumor efficacy, thereby demonstrating substantial potential.
Characteristics of US microbubble for drug delivery
The efficacy of chemotherapy for tumors depends on the effective concentration and duration of chemotherapeutic drugs at the tumor site. Chemotherapeutic agents can prolong survival in BC patients; however, adverse reactions remain the primary issue limiting their clinical application. Paclitaxel, a lipophilic drug, is widely used as a chemotherapeutic agent for BC but often induces numerous adverse reactions during chemotherapy. Encapsulating paclitaxel within microbubbles can reduce drug toxicity and side effects while enhancing local drug concentration within the tumor. Tang et al 100 investigated the effects of UTMD-mediated suppressor of cytokine signaling 3 (SOCS3) gene therapy on the biological characteristics and epithelial-mesenchymal transition of BC stem cells by establishing an in vivo BC model and culturing BC stem cells in vitro. The results indicated that UTMD-mediated SOCS3 gene therapy exhibited superior therapeutic effects. Takabatake et al 101 studied the inhibitory impact of gefitinib and taxane microbubble complexes on BC cell lines MDA-MB-231 (EGFR-positive) and MCF7/ADR (EGFR and HER2-positive). These findings suggested that gefitinib and taxane microbubble complexes could overcome drug resistance in these cancer cells, thereby enhancing the effect of taxanes on MCF7/ADR cells.
Researchers have also prepared dual-modified lipid CLR8LP (DOX + VER) microbubbles co-loaded with doxorubicin (DOX) and verapamil (VER) to investigate their inhibitory effects on the proliferation of human BC MCF7 cells. The results showed that co-encapsulating DOX and VER within co-modified liposomes significantly increased the cytotoxic efficacy against MCF7 cells. Overexpression of P-glycoprotein (Pgp) on tumor cell membranes is one of the primary mechanisms of drug resistance.102 -104 A commonly used strategy is to combine Pgp inhibitors with chemotherapeutic drugs. Verapamil, as a Pgp inhibitor, and dual-modified liposomes (CLR8LP) with excellent tumor-targeting delivery capabilities were used as carriers for chemotherapeutic drugs and Pgp inhibitors to create microbubble complexes. This enables chemotherapeutic drugs, with the synergistic effect of Pgp inhibitors, to effectively accumulate within cells, inhibiting and killing tumor cells. Ultrasound microbubbles carrying drugs not only reduce drug toxicity and side effects but also increase local drug concentration within tumors, enhancing the cytotoxic effect on tumor tissues.
Targeting of US microbubble in therapy
Ultrasonic microbubbles, as carriers, can not only reduce drug side effects in systemic circulation while enhancing drug concentration in pathological regions but also protect drugs and gene fragments from degradation by nucleases and clearance by the reticuloendothelial system. Gene therapy involves the use of gene engineering techniques to introduce exogenous genes into target cells for correcting functional defects or providing new functions. 105 Ultrasonic targeted microbubble destruction technology represents a targeted and efficient gene delivery method that minimizes injury, as supported by the excellent cavitation effect of microbubbles. 106 Some researchers 107 combined targeted ultrasonic microbubbles with CD/TK bicistronic suicide gene plasmids and prodrugs to transfect BC MCF7 cells expressing the KDR promoter, followed by US irradiation. The results demonstrated that the KDR promoter could drive the targeted expression of CD/TK bicistronic suicide genes in MCF7 cells, and the KDRP-CD/TK gene exhibited a targeted cytotoxic effect on MCF7 cells in vitro. Survivin, a member of the inhibitor of apoptosis protein family, promotes tumor proliferation. By inhibiting survivin gene expression and interfering with survivin Thr34 phosphorylation, cancer cells undergoing mitosis can be induced to undergo apoptosis, thereby enhancing the apoptosis-inducing effects of chemotherapeutic drugs on cancer cells. 108 Researchers have constructed an siRNA eukaryotic expression vector to silence the human survivin gene 109 and prepared lipid microbubbles loaded with this vector using the reverse-phase evaporation method with mechanical agitation. In vitro experiments showed that gene-loaded targeted microbubbles could specifically bind to BC cells with high HER-2 expression and induce apoptosis. The safety, efficacy, and stability of microbubbles as gene carriers have been confirmed in numerous experiments conducted by scholars worldwide; however, their clinical application still faces many challenges. Some scholars 110 noted as early as the 2015 Annual Meeting of the American Association for Cancer Research (AACR) that MPDL3280A exhibited durable efficacy in advanced TNBC. Programmed death 1/PDL1 immunotherapy is currently a hot topic in antitumor therapy, but no studies have been reported on conjugating anti-PD1 monoclonal antibodies to microbubbles for BC treatment.
This indicates that ultrasonic microbubbles can enhance the permeability of tumor cell membranes, induce mechanical damage to vascular endothelium and adjacent tumor tissues, and enlarge endothelial gaps. Ultrasonic microbubbles are capable of delivering chemotherapeutic agents such as paclitaxel in a targeted manner, thereby reducing drug toxicity and side effects, increasing local drug concentration in tumors, and potentiating the cytotoxic effects of chemotherapeutics on tumor cells. Ultrasonic microbubbles can facilitate the introduction of exogenous genes into BC cells to correct functional defects in target cells and promote apoptosis. Furthermore, they can deliver monoclonal antibody carriers for targeted immunotherapy, activating the immune system, enhancing immune responses, and inhibiting tumor initiation and progression. Currently, there are limited reports on microbubbles carrying drugs and genes targeting tumor parenchymal cells. Therefore, future research should focus on identifying safe and efficient targets for tumor parenchymal cells to improve the precision of ultrasonic microbubble-mediated targeted therapy.
Application of ADCs
Antibody-drug conjugates represent a novel strategy in cancer therapy. By exploiting the high specificity of monoclonal antibodies for binding to antigens on the surface of cancer cells, ADCs deliver potent cytotoxic agents directly to tumor cells. This approach integrates the targeted precision of antibodies with the robust antitumor efficacy of cytotoxic drugs, achieving high potency and reduced systemic toxicity. 111 To date, T-DM1 remains the sole ADC approved for the treatment of advanced HER-2-positive BC, and its success has catalyzed the development of next-generation ADCs.
The mechanism of action of ADCs
The design of ADCs comprises 3 critical components: the antibody, the cytotoxic drug, and the linker. 112 Antibody-drug conjugates combine the highly specific targeting capability of antibodies with potent small-molecule cytotoxic agents, maintaining stability in the circulatory system. As depicted in Figure 6, upon binding to antigens expressed on the surface of tumor cells, ADCs undergo intracellular degradation and release their payload within the cell, achieving a high local drug concentration that effectively and precisely eliminates tumor cells. By integrating the targeting properties of monoclonal antibodies with the cytotoxicity of chemotherapeutic agents, ADCs represent a significant advancement over traditional chemotherapy and targeted therapy. 113 When specific antigens on the surface of tumor cells are kinase receptors or molecules involved in signaling pathways associated with tumor growth, differentiation, and proliferation, the antibody component of ADCs binds to these antigens, thereby blocking downstream signaling pathways and inhibiting tumor cell proliferation. 114 In addition, ADCs can induce apoptosis via antibody-dependent cellular cytotoxicity (ADCC) and complement-dependent cytotoxicity (CDC). 115

Hyaluronic acid-decorated nanomicelle-mediated active and passive targeting.
Trastuzumab emtansine (T-DM1) is a novel ADC that demonstrates biological activity analogous to trastuzumab. It selectively targets and delivers the potent antimicrotubule agent DM-1 to HER-2-positive tumor cells, effectively and specifically eliminating them. The initial success of T-DM1 in BC treatment has expedited advancements in this field, with over 60 new ADCs currently in development.116 -118 Nevertheless, ADC development continues to encounter substantial challenges, including complex drug structures, targeting efficiency, and adverse effects, which have contributed to suboptimal outcomes in clinical trials. 119 Of particular significance is the balance between lower-than-expected efficacy and higher-than-expected toxicity, highlighting the necessity for further innovation in designing next-generation ADCs. 120 In summary, ADCs provide novel opportunities to enhance the prognosis of BC patients. Through ongoing optimization of drug molecule design and target selection, improved treatment options for BC can be anticipated in the future. 121
Clinical application of ADCs
Antibody-drug conjugates selectively deliver cytotoxic agents or radioisotopes to malignant cells through targeted monoclonal antibodies. 122 In the TNBC field, ADCs that have entered clinical trials include DS-8201a, sacituzumab govitecan, ladiratuzumab vedotin (SGN-LIV1A), CAB-ROR2-ADC, anti-CA6-DM4 immunoconjugate (SAR566658), AVID100, and U3-1402. 123 Although atezolizumab and albumin-bound paclitaxel have been approved, their combination is currently limited to PD-L1-positive TNBC patients, highlighting ADCs as a promising targeted therapeutic option for the remaining 60% of PD-L1-negative patients.
DS-8201, also known as T-DXd, is an ADC comprising trastuzumab, a peptide-based cleavable linker, and a topoisomerase I inhibitor payload. 124 The amino acid sequence of its antibody component is identical to that of trastuzumab, and it is conjugated to the cytotoxic agent DXd via a protease-cleavable tetrapeptide linker, achieving a drug-to-antibody ratio (DAR) of 8. The phase III DESTINY-Breast03 trial demonstrated that T-DXd significantly reduced the risk of mortality by 36% in patients with HER2-positive BC, with a median progression-free survival (PFS) more than 4 times longer compared with the T-DM1 arm (28.8 months vs. 6.8 months, HR = 0.33, P < 0.0001). In addition, 79% of participants achieved an objective response, including 21% who attained a complete response. 125 These findings indicate that, compared with T-DM1, T-DXd provides clinically and statistically significant improvements in survival and sustained PFS benefits for patients with pretreated HER2-positive metastatic BC. Furthermore, T-DXd has shown manageable and tolerable safety profiles even with prolonged treatment exposure. Recently, results from a phase I dose-escalation study (NCT02564900) were published to evaluate the safety and tolerability of DS-8201 in HER2-positive BC patients who progressed after prior T-DM1 therapy. 126 The dosing regimens were 5.4 mg/kg or 6.4 mg/kg every 3 weeks, and common grade 3 or higher adverse events included anemia (17%), neutropenia (14%), leukopenia (9%), and thrombocytopenia (8%). The trial confirmed controllable safety for DS-8201. Moreover, an ongoing phase III clinical trial (NCT03529110) is enrolling 500 patients with HER2-positive, unresectable, and/or metastatic BC who have received prior trastuzumab or taxane-based chemotherapy. This trial compares DS-8201 to T-DM1, with PFS as the primary endpoint and overall survival (OS) and objective response rate (ORR) as secondary endpoints.
Trophoblast cell surface antigen 2 (Trop-2), a glycoprotein widely expressed in various tumor types, is also referred to as tumor-associated calcium signal transducer 2 (TACSTD2), membrane component 1 surface marker 1 (M1 S1), gastrointestinal antigen 733-1 (GA733-1), and epithelial glycoprotein 1 (EGP-1). First identified in a human choriocarcinoma cell line in 1981, it belongs to the category of cell surface receptors. Trop-2 serves as a critical signaling molecule regulating tumor growth. 127 It is overexpressed in malignant tumors such as BC, gastric cancer, colorectal cancer, and nonsmall cell lung cancer. Through mediation of multiple signaling pathways, Trop-2 regulates cell proliferation and apoptosis, thereby participating in tumor development. 128 Particularly in TNBC cells, this characteristic makes Trop-2 an ideal target for ADCs. 129 Sacituzumab govitecan (SG), a Trop-2-targeted ADC, exerts antitumor activity by conjugating an anti-Trop-2 antibody with the cytotoxic agent SN-38 (7-ethyl-10-hydroxycamptothecin). 130 The final results of the phase III ASCENT study demonstrated that SG significantly prolonged median PFS (5.6 months vs. 1.7 months, HR = 0.39, P < 0.001) and overall survival (OS) (12.1 months vs. 6.7 months, HR = 0.48, P < 0.001) compared with single-agent chemotherapy in patients with unresectable, recurrent, or refractory locally advanced/metastatic TNBC who had received ⩾ 2 prior lines of standard chemotherapy. The most common grade 3/4 treatment-related adverse events were neutropenia and diarrhea, which could be managed with symptomatic support. Furthermore, the final analysis of the phase III TROPiCS-02 study indicated that SG was superior to physician’s choice of chemotherapy in patients with endocrine therapy-resistant metastatic hormone receptor (HR)-positive/HER2-negative BC who had previously received taxanes, endocrine therapy, CDK4/6 inhibitors, and 2-4 lines of chemotherapy, with median OS of 14.4 months versus 11.2 months, respectively (HR = 0.79, P = 0.02). 131 A single-arm, multicenter, phase II clinical trial evaluated the efficacy and safety of sacituzumab govitecan in patients with recurrent/refractory metastatic TNBC. 132 Results showed an objective response rate (ORR) of 30%, including 2 complete responses and 19 partial responses, with a median PFS of 6 months and median OS of 16.6 months. Immunohistochemical analysis revealed moderate to strong Trop-2 expression in 88% of patients. The most common grade ⩾ 3 adverse events included neutropenia (39%), leukopenia (16%), anemia (14%), and diarrhea (13%), with a febrile neutropenia incidence rate of approximately 7%. The trial confirmed the favorable efficacy and tolerability of sacituzumab govitecan in metastatic TNBC. Another ongoing multicenter, randomized, open-label, phase III clinical trial (NCT02574455) is enrolling patients with refractory/metastatic TNBC or recurrence after at least 2 prior lines of chemotherapy. This trial compares sacituzumab govitecan to the physician’s choice of chemotherapy (capecitabine, eribulin, gemcitabine, and vinorelbine), with PFS as the primary endpoint and OS, ORR, and other indicators as secondary endpoints.
SGN-LIV1A represents an additional ADC therapeutic, comprising a monoclonal antibody targeting LIV1 conjugated to the microtubule inhibitor monomethyl auristatin E (MMAE). 133 LIV1 is a transmembrane protein with zinc transporter and metalloproteinase activities, exhibiting high expression in over 90% of breast tumors but limited expression in normal tissues. 134 An ongoing open-label, dose-escalation Phase I clinical trial (NCT01969643) is evaluating the safety and tolerability of SGN-LIV1A in patients with metastatic BC. The interventional strategies in this study include the administration of SGN-LIV1A as a single agent or in combination with trastuzumab. The primary endpoint is the incidence of adverse events, while secondary endpoints include blood concentrations of SGN-LIV1A and its metabolites, overall response rate (ORR), and other indicators. Currently, multiple clinical studies for this drug are underway, with results anticipated within the next 2 years. Other ADCs under investigation include CAB-ROR2-ADC, SAR566658, AVID100, and U3-1402. CAB-ROR2-ADC integrates conditionally active biologics (utilizing BioAtla’s proprietary CAB technology) with an antibody targeting ROR2, and its tolerability, safety, and antitumor activity are being assessed in patients with solid tumors. The anti-CA6-DM4 immunoconjugate (SAR566658) is an ADC consisting of a ds6 antibody targeting carbonic anhydrase 6 (CA6) coupled with the microtubule inhibitor DM4. 135 AVID100 is the first epidermal growth factor receptor (EGFR)-targeted ADC to achieve clinical progress. AVID100 was evaluated in a multicenter, dose-escalation Phase IIa clinical trial in TNBC patients, initially demonstrating promising results, 136 but recent updates indicate the trial was terminated due to insufficient efficacy. U3-1402 is an ADC where the HER3 monoclonal antibody patritumab is conjugated to the topoisomerase I inhibitor deruxtecan (Dxd) via a tetrapeptide linker. 137 Previous data indicate that HER3 is expressed in approximately 50% to 70% of BC patients, yet few therapies specifically target HER3. 138 At the 2022 ASCO meeting, the novel HER3-targeted ADC patritumab deruxtecan demonstrated efficacy in treating HER3-expressing metastatic BC. The U31402-A-J101 study enrolled 182 patients with HER3-expressing metastatic BC, including 113 HR +/HER2-, 53 TNBC, and 14 HER2+ patients. Following treatment with patritumab deruxtecan, overall survival (OS) was 14.6, 14.6, and 19.5 months, respectively, while PFS was 5.5, 7.4, and 11.0 months across the 3 subtypes. The study demonstrated the efficacy of patritumab deruxtecan irrespective of HER3 expression levels, with favorable safety, as only 10% of patients discontinued treatment due to intolerance. Researchers believe that HER3 will emerge as a critical target for treating diseases such as BC.
In summary, the application of ADCs in BC treatment has demonstrated significant progress and evolution in recent years. By leveraging the targeting specificity of antibodies to deliver cytotoxic agents to designated lesions, ADCs exert enhanced antitumor efficacy. Despite over 2 decades of investigation in oncology, ADC development has been relatively slow due to challenges in target selection, conjugation technology, antibody optimization, and drug release. However, advancements in fourth-generation ADC technology have established a promising contemporary landscape. In TNBC, SGN-LIV1A underwent a series of clinical trials, leading to the full FDA approval of the targeted anticancer agent Trodelvy, expanding its indication to adult patients who have received at least 2 prior systemic therapies, including 1 for metastatic or unresectable locally advanced TNBC. In addition, as depicted in Figure 7, ADCs such as ladiratuzumab vedotin, SAR566658, CAB-ROR2-ADC, and U3-1402 are currently under clinical evaluation (Figures 8, 9). 139

Schematic of the microbubble-based, ultrasound-assisted photodynamic therapy (PDT) strategy. 90 PDT, photodynamic therapy; PGL, porphyrin-grafted lipid; MB, microbubbles; LFUS, low-frequency ultrasound; CEUS, contrast-enhanced ultrasound.

Schematic representation of ADC drug structure and its mechanism of action.
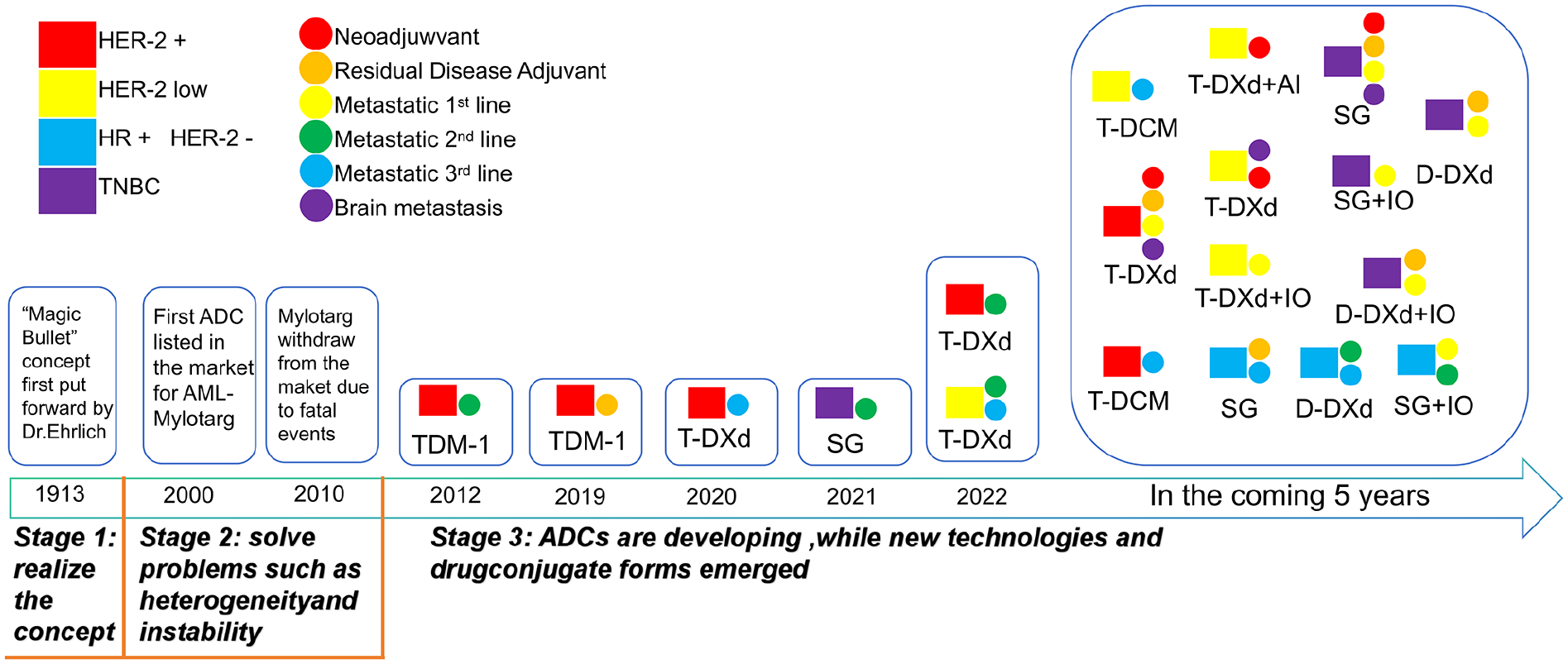
Timeline of current and future ADC development in BC.
Conclusions
In brief, within the current treatment landscape, BC patients face significant challenges related to drug resistance or nonresponsiveness, highlighting the necessity for developing novel anticancer agents as a promising strategy to further improve patient outcomes. The 4 aforementioned technologies each exhibit distinct advantages. Given the diverse mechanisms of action employed by these drugs, it is crucial to select or customize therapies based on individual patient characteristics. For example, antiangiogenic compounds may achieve optimal efficacy when targeted to the interstitial space rather than intracellularly, whereas chemotherapeutic agents function most effectively upon intracellular delivery. Furthermore, the heterogeneity of the BC cell population emphasizes the importance of targeting multiple cell types expressing varied surface markers to effectively reduce tumor burden and eliminate cancer cells. An effective multitargeted approach may also require the incorporation of several distinct targeting ligands, representing a current and future research focus in anticancer drug development. In conclusion, the optimal pharmacotherapeutic strategy aims to maximize therapeutic efficacy, overcome drug resistance, and minimize adverse effects. Advancing research on these drug delivery systems and developing safer, more effective targeted therapies for BC may offer new treatment opportunities for patients.
Footnotes
Acknowledgements
Not applicable.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the National Natural Science Foundation of China (grant no. 82460495), Jiangxi Provincial Natural Science Foundation (grant nos. 20242BAB216064 and 20242BAB25353), Jiangxi Provincial Health Commission Science and Technology Plan Project (grant no. SKJP220225453) and Ganzhou City, Jiangxi Province “Science and Technology + health care” Joint Program Project (grant no. 2023LNS36669).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
Not applicable.