
Abstract
Introduction:
Lymphedema is one of the complications of breast cancer treatment. It has no cure yet and can affect the quality of life. This study aimed to identify and investigate informational needs, preferred delivery methods, and time of receiving information about lymphedema for these patients.
Methods:
One hundred participants were recruited through Lymphedema Clinic in Motamed Cancer Institute in Tehran, Iran, through convenience sampling and were asked to complete a self-administered survey. Data collection took place on all opening days between October 2018 and mid-March 2019.
Results:
Most of the participants were above 40 years, have a diploma, homemaker, and the average income of most of the participants (57.2%) was low. The importance of having lymphedema information was very high for them. Most of them wanted detailed information at diagnosis of breast cancer. The preferred information of delivery methods were private sessions and social networks.
Conclusions:
Patients with breast cancer who have lymphedema have high needs as regards concise lymphedema information. Private sessions with physicians and social networks can provide detailed information for them.
Keywords
Background
Breast cancer (BC) is the most frequently diagnosed cancer among women and it is the leading cause of cancer death in most of the countries. 1 Breast cancer ranks first among cancers diagnosed in Iranian women. The 5-year prevalence of BC in Iran is 40 825 in 2018. 2 Studies showed that 3-, 5-, and 10-year survival rates were 0.808, 0.695, and 0.559, respectively. 3
Breast cancer treatments usually include a mix of surgery, chemotherapy, radiotherapy, and hormone therapy and targeted therapy. 4 Curative treatment needs surgery 5 that in many cases is the first treatment option. Not only can surgery remove the tumor, but it can also detect the amount of tumor dissemination and the stage of cancer. 6
Upper limb lymphedema is the most important side effect of BC treatment.7-10 Lymphedema is the accumulation of protein-rich fluid in tissues with inadequate lymphatic drainage. 11 It is accompanied by feelings of heaviness, shoulder dysfunction, psychological issues, and infection. 12 Evidence showed BC survivors with lymphedema reported poorer quality of life compared with those without lymphedema. 13 It is estimated that in the United States, more than 40% of BC survivors are diagnosed with lymphedema. 14
Evidence has shown that more than half of BC survivors, who were not diagnosed with lymphedema, have one or more lymphedema symptoms such as pain, tenderness, and aching and other symptoms. 14
Unfortunately, patients at risk of lymphedema asking for help when there is a visible swelling. Under these conditions, the likelihood of timely treatment is reduced. 14 Early diagnosis is important because the most effective treatment can be accrued in the early stages of lymphedema diagnosis. 15 Also, patient education in the first week after surgery followed by physiotherapy can decrease the risk of breast cancer–related lymphedema (BCRL). 16 The early patient education program can decrease the risk of lymphedema occurrence after BC surgery. 17 On the other side, patients with BC believed that they did not receive sufficient information about secondary lymphedema,18,19 how to detect signs and symptoms, where to look for treatment and find lymphedema professionals, or how to do some preventive behaviors.20,21
Many of these patients do not receive any education about lymphedema 14 and lose the opportunity to receive correct training at the right time. It has been shown that proper education about patients with BC can increase their knowledge and reduces the risk of lymphedema.16,17
On the other side, in scientific literature and clinical practice, symptom management, informational needs, 14 and new methods of accessing information of patients with BC lymphedema 19 are insufficiently investigated. To the best of our knowledge, needs assessment has not been performed for patients with BC who have lymphedema in Iran, so this study aimed to identify and investigate informational needs, preferred delivery methods, and the time of receiving information about lymphedema for these patients.
Methods
This study is a cross-sectional, descriptive study. A total of 120 participants were recruited through Lymphedema Clinic in Motamed Cancer Institute in Tehran, Iran, through convenience sampling. This center is a referral clinic and accepts patients from other provinces of Iran.
Patients were informed about the study by a clinician and those who were interested, were explained the study objectives, and asked to fill the questionnaire. Informed consent was obtained from all participants. Patients were also assured that their responses and data collection would remain confidential. The questionnaire was completed by patients or their caregivers when they were waiting for an appointment. Institutional review board approval was obtained from Shahid Beheshti University of Medical Sciences.
The sampling was done among female patients with BC with a confirmed BCRL diagnosis, between 18 and 90 years of age, and able to read and write Persian proficiently. Data collection took place on all opening days between October 2018 and mid-March 2019.
The questionnaire of our study was inspired by the Supportive Care Needs Survey, 22 which measures the perceived needs of patients with cancer and White’s study 19 that investigated the informational needs of patients with BCRL.
This survey consists of 2 parts: (1) demographics and health information and (2) informational components encountered when someone experiences lymphedema.
The survey was sent to 5 surgeons, lymphedema expert nurses, and health information management professionals to assess the face and content validity for the adapted tool. The pilot group showed minor feedback that was applied to the final version.
The second part includes modified informational questions. The importance of having information was asked in 6 important areas. It has a 5-point response scale: “not important” = 1, “slightly important” = 2, “important” = 3, “fairly important”= 4, or “very important = 5.”
Other questions were design based on patients’ expectations about the level of information they want to know about lymphedema, the best information delivery time, methods and preferences, and the use of new technologies to manage their conditions.
Data analysis
Survey responses were analyzed using SPSS (V.16) with descriptive statistics. The demographic information and clinical characteristics were reported as frequencies and percentages. Mean, median, and frequencies were calculated for informational needs’ questions.
Results
Between October 2018 and mid-March 2019, 120 questionnaires were distributed to eligible participants, of which 100 questionnaires were returned.
All questionnaires were included in the data analysis and comprise the study sample. In our analysis, we found some missing responses, so we reported valid percent.
The demographic characteristics are shown in Table 1. Most of the participants were above the age of 40 (n = 84, 90.4%). Most of them were married (80.8%) and lived in Tehran or the nearby areas (70.4%). Most of the subjects surveyed had a diploma (45%) and 34% had achieved some level of college degree and 21% had a high school level of education.
Patients’ demographic information.

Abbreviation: MT, Million Tomans.
In describing their employment status, 17% of the participants worked, 67% were homemaker, and 15% were retired. The average income of most of the participants (57.2%) was low.
Most of them (n = 43, 45.7%) had no evidence of disease and 29.8% had just finished treatment. Others were undergoing treatment (n = 13) or recurrence diagnosis (n = 10) (Table 2).
Clinical characteristics of the participants.
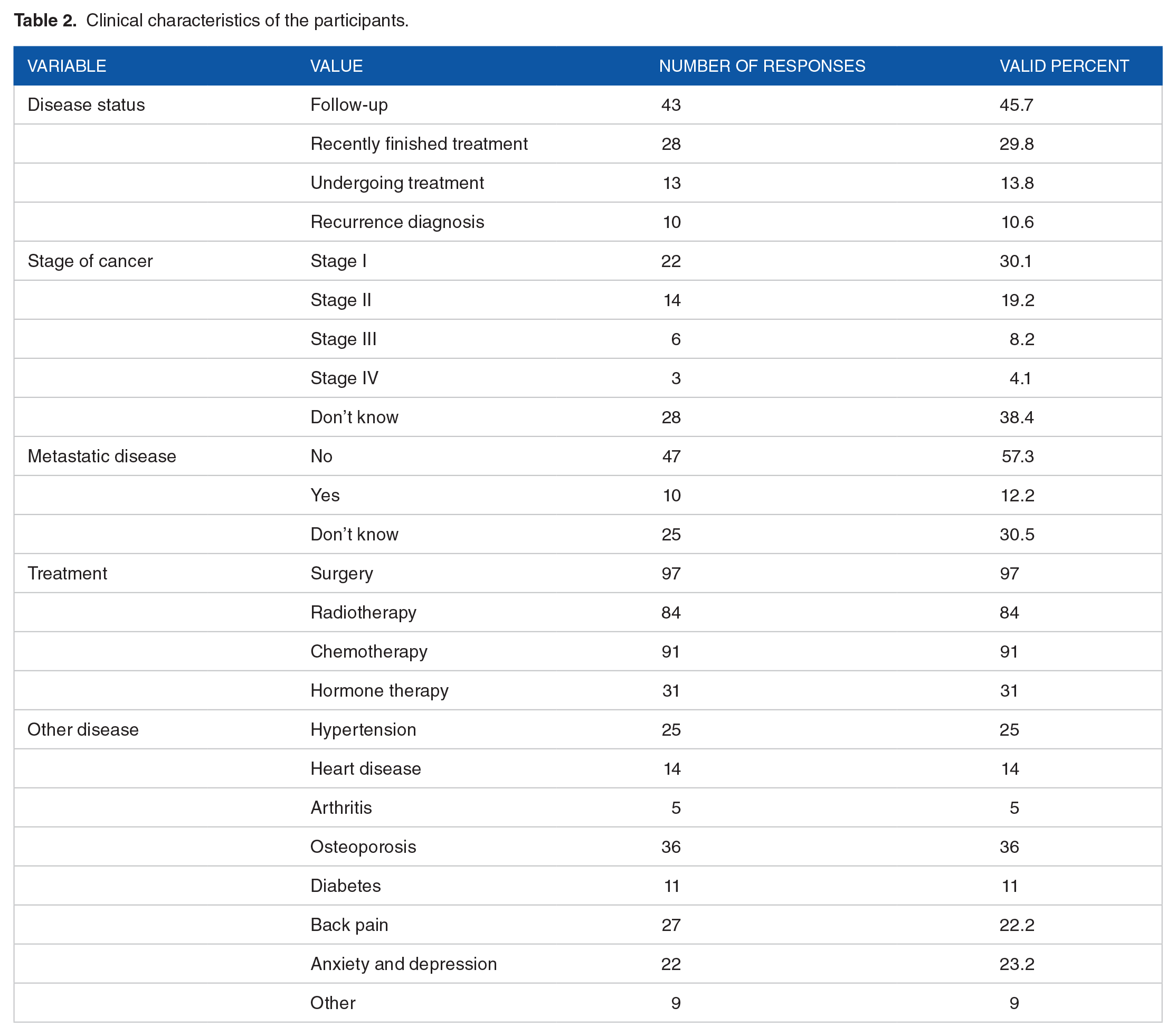
Most of the participants (49.3%) reported having stage I or II and 12.3% reported having stage III or IV. Most of the participants 38.4% (n = 28) did not know their cancer stage.
The frequency of metastatic disease was 12.2% among participants. Most of the respondents had surgery (97%), radiation therapy (84%), and/or chemotherapy (91%), and hormone therapy (31%), to treat cancer.
Participants had other diseases such as osteoporosis (36%) and hypertension (25%).
Participant’s lymphedema characteristics are shown in Table 3. Most of the patients (49%) stated their first lymphedema was diagnosed more than 2 years ago and 15.6% reported being diagnosed 1 to 2 years ago.
Patients’ lymphedema characteristics.

Informational needs questions
We asked the following questions from patients with BCRL to investigate the level of their informational needs:
How important is it for you to have enough information about lymphedema?
How important is it to have information about how to recognize the signs and symptoms of lymphedema?
How important is it to have information about certain self-care behaviors you can do to control and avoid the lymphedema getting worse?
How important is it to have information about how to manage and treat lymphedema?
How important is it to have information about who to contact or where to go if you think you have developed lymphedema?
How important is it to have information about how to cope with fears about developing lymphedema?
Five-point Likert-type scale was used in these questions. It has a 5-point response scale: “not important” = 1, “slightly important” = 2, “important” = 3, “fairly important” = 4, or “very important” = 5.
Median and mode in all questions were 5/5 except question number 2 in median (median = 4). All means were above 4 (4.16-4.35). The level of importance is shown in Figure 1. When we stratified patients by the time of diagnosis, the most frequent selected scale was “very important” in all groups and there was not a difference in the level of the required information.
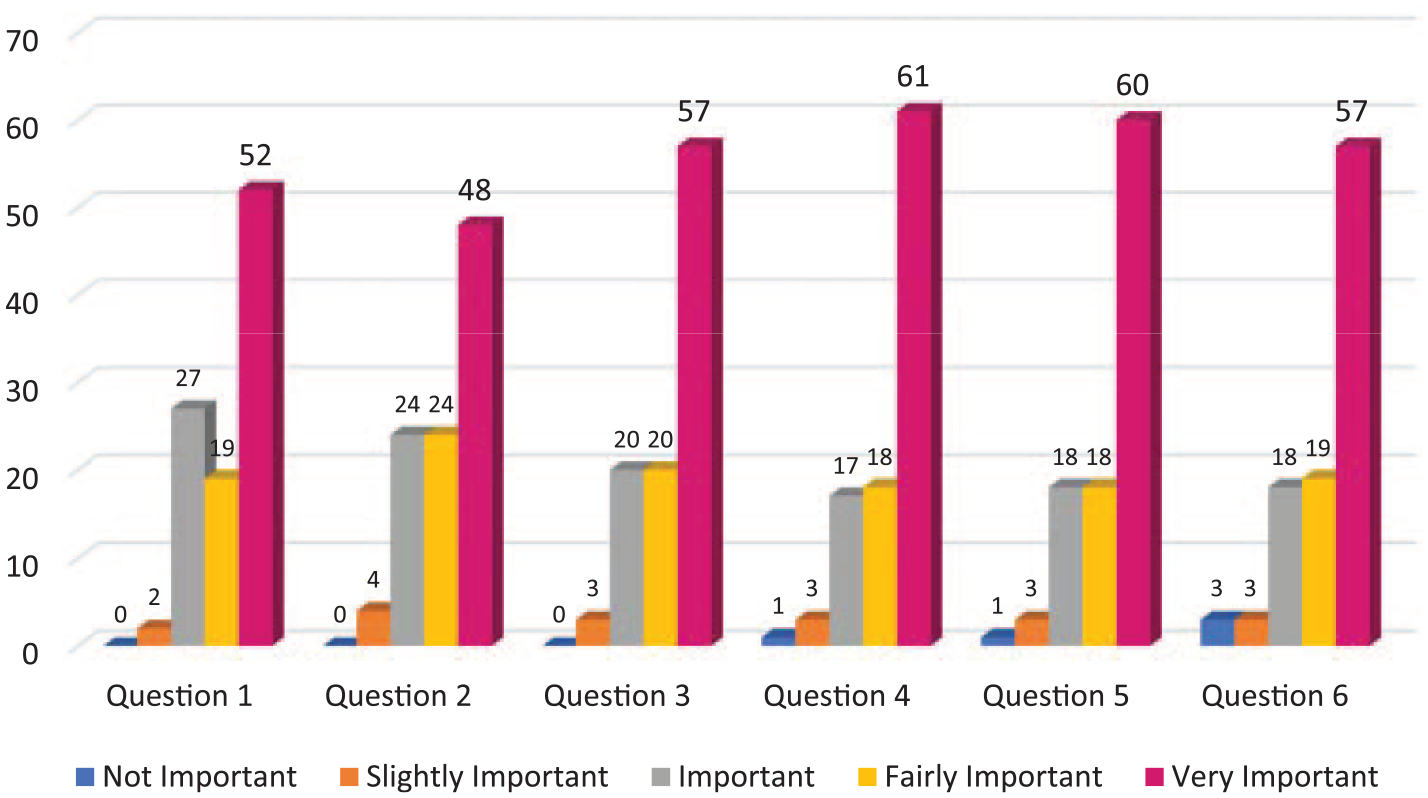
The level of importance of informational needs.
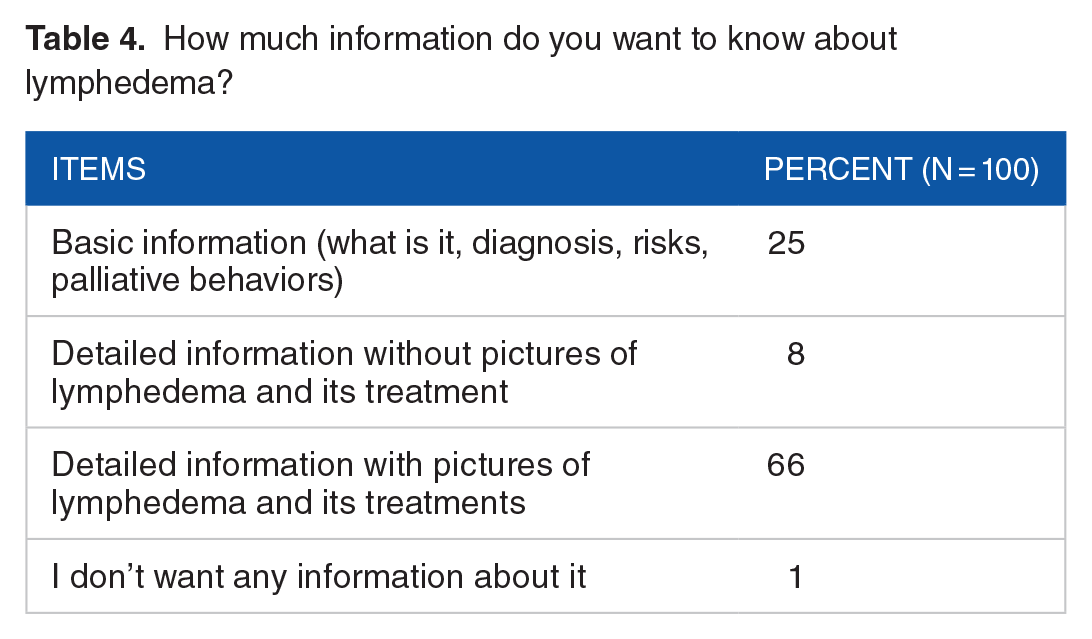
For measuring patients’ expectations about information-level patients want to know, we asked, “What is the level of information you want to know about lymphedema?”
Most of the participants (66%) chose detailed information with pictures of lymphedema and its treatments (Table 4).
How much information do you want to know about lymphedema?
When they were asked “Did you know you may have lymphedema in the future?” more than half of them (67%) said “NO,” 29% of them said “Yes” and 4% did not remember.
The next question was “what is the best time for receiving information about lymphedema”; 34% of patients wanted this information at diagnosis of BC. A slightly lower percentage (26%) wanted this information in the process of treatment, and 26% before starting treatment; 12% wanted this information after the treatment is completed (Table 5).
The best time for receiving information about lymphedema.

What are the preferred methods to deliver the information?
At the end of the survey, the preferred methods of delivering information were asked. The most selected methods were private sessions with doctors (42.9%), then social networks (40.8%), group classes (22.4%), brochures (18.4%), books (14.3%), DVD (13.3%), and websites (8.2%), respectively.
As a new suggestion, we explore patients’ preferences about mobile apps delivering information in this regard. At first, we asked, “Would you like to learn about lymphedema with your smartphone app through the lymphedema self-management program that will be available for you”? More than 90% of participants said they would agree to have this app. But we wanted to know what preferences they might have. So, we asked about the features that this app should have. The most frequently selected features were the special exercise for lymphedema (79.4%), connection with physician (73.2%), and nutrition education and lifestyle (71.1%). Other features are shown in Table 6.
The most frequent mobile app features selected by patients with lymphedema.

Discussion
This study investigated the informational needs, best time and methods of delivering information for patients with who have lymphedema. It shows patients have a high level of needs about lymphedema, signs and symptoms, self-care behaviors, treatments, finding health care services, and coping with fears.
As an important point, we have women with undiagnosed lymphedema or those who are at risk of developing lymphedema whose informational needs are different from women with diagnosed lymphedema. Information collected in this survey about insufficient education about lymphedema diagnosis can be valuable for planning future interventions to provide better education for BC survivors, so we categorize discussion into 2 parts as shown in the following sections.
Information needs for those who have already been diagnosed with lymphedema
There is not enough information about the needs of patients with BC who have lymphedema in Iran. We had no prior assumption about their clear needs and their priorities. Although psychological needs are suggested by the literature, other kinds of needs were unknown. There are limited centers in Iran that provide lymphedema treatment services.
Our findings confirm the previous studies which showed that the level of informational needs in patients with is high.19,23-25 This study showed that patients who were diagnosed with lymphedema, first seek for the treatment. As another need, they search for lymphedema care providers, and then self-care behaviors. In this phase, they have fear of their lymphedema getting worse. For these patients having enough information about lymphedema and recognizing its signs and symptoms have low priority rather than other issues seems normal because they passed this phase before.
Educational plans and recommendations for BC survivors who are at risk of lymphedema
The main solutions for BC survivors who are at risk of lymphedema are providing information and patient education for preventing lymphedema or reducing the risk of developing in severe conditions. 26
Most of our participants (67%) were not aware they may have lymphedema in the future. It showed they did not receive enough information during the treatment process or they forgot information they probably received because of insufficient attention from patients to the received information. 27 However, literature shows that patients with BC were not satisfied with lymphedema education before treatment. 28 Having this information can facilitate recognition of signs and symptoms of lymphedema and can reduce the stress of finding health care providers in the future.
Our study showed most of the participants wanted detailed information about lymphedema with pictures and its treatment. This is an important finding for designing tailored educational content for Iranian patients based on their needs and preferences.
This information should be provided to the patient at an appropriate time and reminded with enough intervals. It would be better to study what times and intervals are better in this regard. In this study, the best time for receiving information from the patient’s perspective was at diagnosis of BC. It is a controversial issue because some clinicians believe providing lymphedema information before treatment can increase patients’ stress and anxiety, but others think differently. 19 However, some researchers believe it is an individual variable that patients should decide about the time of receiving information.29,30
Evidence showed that lymphedema information about prevention and management is not accessible to patients with BC at the right time and it is not considered as an urgent need. 31 It may be the result of underestimating this condition by clinicians.32,33 Literature showed health care professionals also do not have enough information about lymphedema. 34 However, in many cases, referring to other similar specialties that are less encompassed by lymphedema and are outside the treatment team makes the patient’s condition more complicated.
The other point is the medium which is supposed to deliver information to patients. Regarding the age and education of these patients, based on their preferences, different mediums such as brochures, websites, or mobile apps are applicable. Having private sessions with doctors and social networks were the most selected mediums. These patients need to receive the necessary information about lymphedema, especially from their physicians. Physicians who have enough experience in BCRL can play an important role in patient education by providing information about the risk of lymphedema, prevention, detecting early signs and symptoms, and treatments. 35
The most popular method is still private sessions with doctors and then social networks. Interestingly, our patients were willing to receive information from social networks. It is consistent with previous studies.28,36 Finding doctors and health care lymphedema teams and the nearest lymphedema treatment centers is easily accessible via the Internet. About 90% of participants were eager to have an app for lymphedema education and management. The most frequently selected features were special exercises for lymphedema, connection with physicians, nutrition education, and lifestyle, respectively.
Today, the most up-to-date mediums are Internet-based mediums such as websites, mobile apps, and social media. 37 So we propose mobile app software for lymphedema patient education be designed and implemented in our clinic based on updated evidence. In this study, most of the participants were above 40 years, have a diploma, and were homemakers who are eager to use technology for managing their conditions which is probably an efficient method when an appropriate design is available.
This study can create a base for other research in this area. In the future study, we want to investigate the effect of self-management app for patients with BC who have lymphedema based on desired features we found in this study.
One of the strongest points of this study is the good sample of participants that allowed us to generalize our findings in our clinic and even our town with high validity. However, this survey was conducted in one setting and was not multicentered. It is because of the lack of clinics for treating lymphedema in Tehran and Iran. We have many patients from other provinces that compensate for multicenter limitations.
Conclusions
This study has shown high informational needs in patients with BC who have lymphedema. These findings can provide evidence for designing and developing educational programs through different mediums, especially social media and smartphone applications in both domains of prevention and management of lymphedema.
Footnotes
Acknowledgements
This study is related to the project no. 1396/64678 from Student Research Committee, Shahid Beheshti University of Medical Sciences, Tehran, Iran. We also appreciate the Student Research Committee and Research & Technology Chancellor in Shahid Beheshti University of Medical Sciences for their financial support of this study. The authors thank the patients who participated in this study and Motamed Cancer Institute for their cooperation.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is financially supported by Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SD performed data collection, analysis, and interpretation in collaboration with FA. AO and FA contributed to the interpretation of data and revised the manuscript critically. SD drafted the manuscript and FA approved the final version of the submitted manuscript.
Ethical Approval
Institutional Review Board approval was obtained from Shahid Beheshti University of Medical Sciences (IR.SBMU.RETECH.REC.1396.1186) and informed consent was obtained from all participants.